
Shifting Behaviors and Attitudes of Socially Stigmatizing Illnesses to Improve Wellbeing: A Conceptual Framework for Epilepsy

1
Department of Psychology, Faculty of Health Science, University of Venda, University Road, Thohoyandou 0950, South Africa
2
Department of Public Health, Faculty of Health Science, University of Venda, University Road, Thohoyandou 0950, South Africa
*
Author to whom correspondence should be addressed.
Challenges 2024, 15(1), 2; https://doi.org/10.3390/challe15010002
Submission received: 17 August 2023
/
Revised: 12 December 2023
/
Accepted: 19 December 2023
/
Published: 21 December 2023
{kind=link}
{kind=link}
Abstract
:The attitudes and behaviors towards people living with neurological conditions, such as epilepsy, have major implications for the quality of life of affected individuals and for human progress more broadly. Epilepsy is a common neurological disorder often associated with misconceptions leading to discrimination, stigma, and burden for people living with epilepsy (PLWE) and their families. Addressing these negative factors and improving the quality of life has become a crucial area of research. This conceptual framework paper explores the potential of attitude and behavior change to enhance the quality of life for PLWE and their families. The study was conducted in rural Limpopo and Mpumalanga provinces (South Africa), employing an explanatory sequential mixed method approach. Participants included were PLWE (n = 163), their family members and caregivers (n = 519), healthcare practitioners (n = 102), and community members (n = 4290). The findings revealed significant knowledge, awareness, and behavior disparities among participants, with PLWE showing better consistency. Furthermore, the study highlighted the impact of consistency and balance in knowledge, awareness, and behavior on the overall quality of life for PLWE and their families. It is important to have intentional epilepsy education and accurate information sharing to influence attitudes, positive behavior, and improved quality of life for PLWE and their families. While the primary emphasis of this study lies in epilepsy, its implications may extend to other stigmatized and discrimination-prone illnesses, especially those affecting the brain. This highlights the significance of addressing societal attitudes toward such conditions as a measure of social progress.
1. Introduction
Societal attitudes towards people with illness, particularly those with mental or neurological conditions, have major implications for both individual wellbeing and social progress. While there has been considerable social progress since people with conditions such as epilepsy were viewed as witches or possessed by demons and tortured or put to death, the long shadows of stigma are still residual today [1]. This paper focuses on the ongoing issue of misunderstanding, stigma, discrimination, and reduced opportunities in education, employment, and social interactions that contribute to isolation, emotional distress, and overall low quality of life (QL) for people living with epilepsy (PLWE) and their family members [2,3,4,5,6,7,8]. ‘The history of epilepsy can be summarized as 4000 years of ignorance, superstition, and stigma followed by 100 years of knowledge, superstition, and stigma’ [9].
While our focus is on epilepsy, as a chronic seizure disorder [10,11,12] of major global public health concern [13], we believe that this current study also has implications for other neurological and psychiatric conditions, as well as social attitudes to illness more broadly. A better community understanding of conditions affecting the brain, including appreciation for the potentially modifiable wider factors in the physical and social environments that may be exacerbating them, is important for progress. For example, factors such as negative attitudes [14,15], minimal awareness [16,17], unsatisfactory to low knowledge toward epilepsy [18,19,20], and poor practices towards epileptic patients [21,22] contribute to low QL for PLWE and their families. Wider social environments, including community awareness, support systems, and societal attitudes towards epilepsy, significantly influence the psychological wellbeing and social interactions of PLWE [23,24,25]. Finally, environmental factors such as air quality, noise pollution, and urban vs. rural living conditions have been shown to affect the health of PLWE [26,27,28].
For these reasons, it is important to explore behavior patterns and attitudes (held by community members, health practitioners, PLWE themselves, and their families) and how these might be altered to reduce epilepsy’s psychosocial impacts and improve overall QL for these individuals.
This is demonstrated in a study by Eze et al. [29] on schoolteachers in Nigeria, who investigated knowledge and attitudes toward epilepsy and showed how these can be positively influenced with tailored intervention. Other intervention studies reported increased QL post-intervention [30,31,32]. For instance, in a study conducted in Norway, a nurse program intervention aimed at improving QL was employed [30]. In the United States of America, a cognitive behavioral intervention was initiated for patients with improved QL [31]. In Iran, a self-management intervention was developed and tested on PLWE for increased QL [32]. A systematic review conducted by Musekwa et al. [33] showed a low number of basic epilepsy research in South Africa, which may slow the possibilities for applied research to impact epilepsy knowledge and behavior change positively. However, a recent study by Makhado et al. [34] reported an epilepsy knowledge and behavior intervention tailored to advance epilepsy life skills for primary teachers and learners. Most studies primarily focus on epilepsy perceptions, management, knowledge, and attitudes toward epilepsy [35,36,37,38,39,40,41,42,43]. Still, there needs to be more research exploring the influence of environmental and social factors on these aspects.
However, no known studies have been conducted to explore attitudes and behavior changes of individuals toward epilepsy to improve QL. Moreover, research often does not look into the knowledge, awareness, learning, and behavior of community members, health care providers (HCPs), PLWE, and FMCs residing in rural areas such as MP and LP, which can profoundly influence individuals’ experiences and behavior towards epileptics. Addressing these is important to crafting a comprehensive framework that caters to the diverse needs of those affected by epilepsy and perhaps illustrates how lasting change of attitude and behavior can be achieved. The framework could provide a basis for modulating behavior patterns and attitudes to encourage positive behaviors, practices and perhaps overall QL for PLWE and their families. The complexities of epilepsy demand a systematic and holistic approach to understanding underlying factors that influence QL.
As previously alluded, more work needs to be carried out on behavior and attitude changes in South Africa. This study attempts to answer the question of what can be done to change the behavior and attitudes of individuals to improve the QL of PLWE and their families. With a framework guided by the study findings and theory, the literature gap on ‘how attitude and behavior can be changed’ may be bridged. It consolidates existing knowledge on attitude and behavior change (as demonstrated in the theories of attitude change) and the study findings on knowledge, attitudes, and behaviors. In addition, the framework can lead to a more comprehensive understanding of epilepsy interventions based on the contextualized needs of participants. The framework’s emphasis is on how knowledge influences attitudes, and behaviors can enhance the overall QL for patients and their families.
2. Methodology
An explanatory sequential mixed method was employed for the empirical phase of the study. This paper shows the integration of the two stages guided by a theoretical framework that the study was embedded in. This particular framework is a meta-inference of empirical studies’ quantitative and qualitative findings. It does not present new findings but combines them to create a scientific trace to attitude, behavior change, and improved QL. The study was conducted in rural Limpopo and Mpumalanga provinces. These two provinces were purposefully selected as they host a mix of cultures in South Africa and were rurally situated. The study included four groups of participants (PLWE, family members and caregivers, community members, and HCP). The purposeful selection of these groups was guided by the study’s theoretical foundation concepts (attitude, behavior, learning and knowledge). Two concepts (learning and knowledge) emphasize that for attitude and behavior to be held and changed, an individual needs to learn through stimulus (PLWE experiencing epileptic seizures and receiving how they are treated), observation (community members observe epileptic seizures, PLWE and their families), or conditioning (family members and caregivers, and HCPs are trained into epilepsy knowledge and care for patients).
From the first stage of data collection, questionnaires were used to collect data physically and analyzed using a statistical package for the social sciences. From these, the researcher sought to investigate levels of knowledge (a key concept of knowledge), awareness (a key concept of learning), attitudes (a key concept of attitude), and practices (a key concept of behavior) toward epilepsy. A total of 5074 respondents completed the questionnaires: PLWE (n = 163), their family members and caregivers (n = 519), HCP (n = 102), and community members (n = 4290). Community members were randomly selected, a total population sampling of HCPs from selected clinics was included, and snowballing was used to select PLWE and their FMC.
On the other hand, stage two of data collection and analysis employed a case study method for the participant groups. In this stage, 45 participants were purposefully and conveniently sampled from the first sampled pool and included in the study. The findings in the quantitative study guided the type of questions asked in the qualitative stage of the study. The questions asked included questions on epilepsy knowledge, epilepsy support and education, epilepsy practices and participants’ ideas on how epilepsy knowledge and attitudes can be positively influenced.
Data were collected face-to-face (all quantitative and qualitative data in Mpumalanga) and telephonically (Limpopo qualitative data). Due to depleted funds, researchers could not travel to conduct interviews; however, these were carried out for 30–45 min each, like face-to-face interviews. The researcher coded the collected raw data, co-coded by an independent expert, and the six-step thematic analysis was applied to analyze the findings, as explained by Braun and Clarke [43]. This study was designed on the foundation of theories of attitude change by Simonson and Maushak [44], especially the population selection and data collection tools. This aided in interpreting the findings according to the framework of the theories. This paper consists of a deductive and inductive theoretical framework (for the deductive aspect of the study) and a conceptual framework developed from the findings (inductive).
3. Theoretical Context
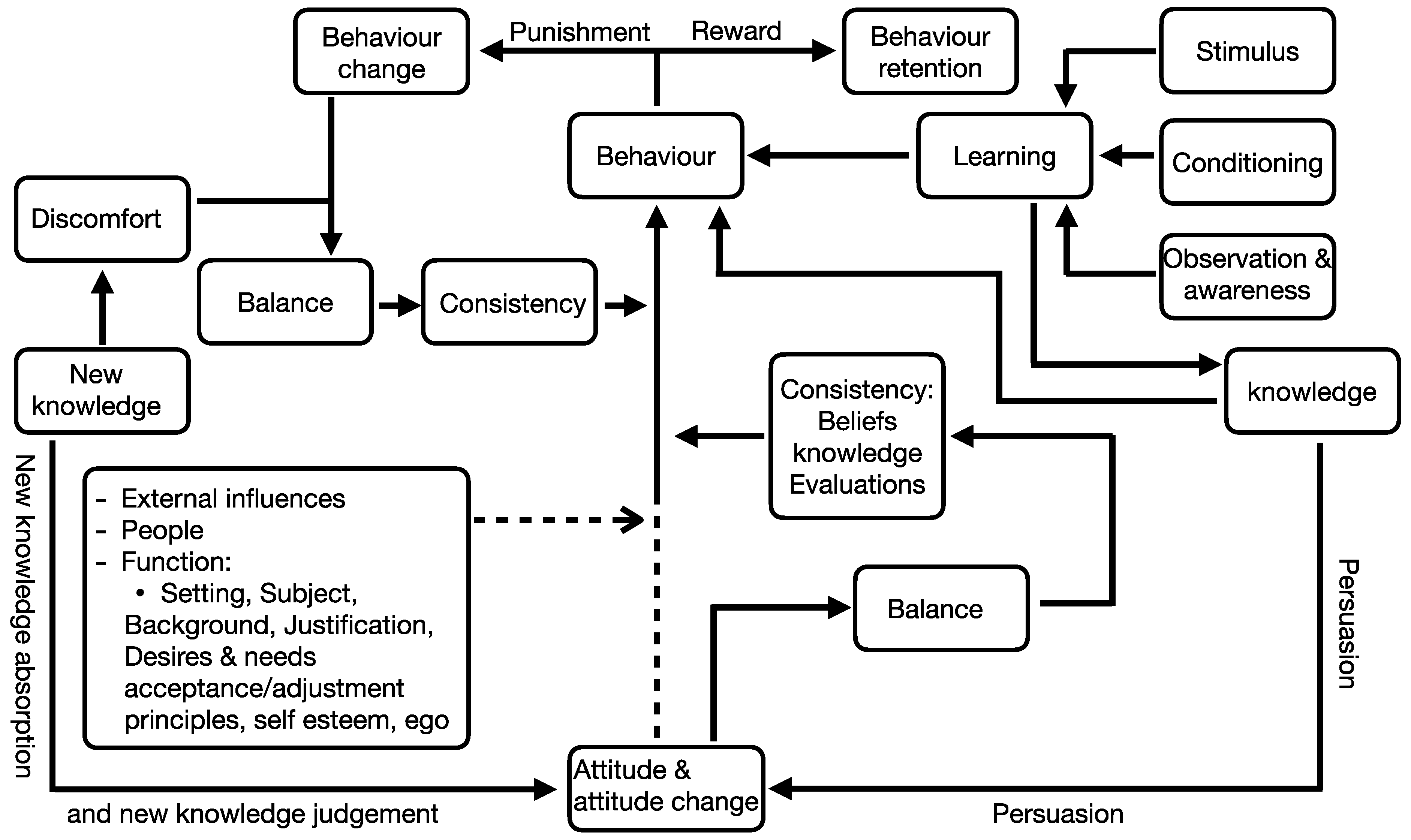
Simonson and Maushak [44] explained how embedded and new knowledge relate. New knowledge is either integrated or rejected by existing knowledge, resulting in attitude, behavior change, or retention. This theoretical foundation encompasses four different theories of attitude change within it. These include consistency theories, learning theories, social judgment theories, and functional theories. Together, these theories have a better chance of influencing and changing behavior than if they were applied singlehandedly (see the outlined framework in Figure 1).
3.1. Learning Theories
Learning theories primarily reflected behavior creation and modification within behavioral psychology. Simonson and Maushak [44] state that what connects learning theories is the emphasis on the characteristics of a stimulus in communication. According to these theories, attitudes and behaviors are established and changed through learning, and learning occurs through observation and conditioning [45]. In addition, whether or not a punishment or reward is associated with certain learned behaviors and motivates change or behavior retention. This means that attitudes and behaviors are created, sustained, or inspired for change if punishment or a reward exists. In connection to social constructivism, learning theories in this study stand on the philosophical position that individuals are not blank slates concerning aspects of the world; they have pre-existing knowledge, attitudes, and varied cognitive resources [46]. For this reason, it was important for researchers to explore existing knowledge, attitudes, awareness, and practices toward epilepsy. From this theory, the following concepts emerged: behavior (behavior retention and behavior change via punishment or reward), communication, learning, observation (awareness), and conditioning. Learning theories explain how behaviors are created, changed, or retained.
3.2. Social Judgement Theories
Our attitudes are set almost like a standard to judge new information gained and retained information [44]. According to the theory, the already available knowledge determines the attitude and awareness toward epilepsy and filters new data or information. In this case, old data/knowledge serves as a referral. Social judgment theories additionally investigate how people absorb information and generate opinions on new communications considering their pre-existing views [47]. This would mean that what an individual already knows is considered necessary, and any new information given is to influence the knowledge/attitude anchor present. Social judgment theories have to do with how one’s ideas, feelings, thoughts, and behaviors are influenced by others [45]. This theory emphasizes the interaction between knowledge and attitudes amongst other concepts, such as knowledge judgment and absorption. In addition, external factors can influence our attitudes and behaviors.
3.3. Functional Theories
In their essence, functional theories focus on answering what function or purpose a particular attitude/s has. Attitudes may have different functions for people or the same person in other settings. It makes it necessary to distinguish who carries the attitude, why they carry it, and in what background that may influence the attitude [44]. This aspect of the learning theories assumes that not all strategies and measures of persuasion uniformly affect attitudes the same way [48]. This is because different attitudes serve different functions/purposes to different people. For example, an individual can have a negative attitude toward epilepsy linked to guilt (stimulates certain behaviors) or fear (which stimulates its behaviors), but both have negative attitudes. Carpenter et al. [48] highlight that there are five types of functions within the theory, these include:
- Utilitarian function: Attitudes whose function serves personal desires and needs.
- Social-adjustive function: Attitudes functions to facilitate acceptance/adjustment to interact with a particular desired social group.
- Value-Expressive function: Attitudes whose function is cantered by consistency with one’s principles, one can express and live by their set value system.
- Ego defensive function: In attitudes that protect one’s self-esteem and ego, one can ignore unpleasant ideas about the self and the world.
- Knowledge function: The function here is to learn about the world inspired by a simple need to know.
Functional theories state that attitudes are persuaded to change based on their function. It theorizes concepts that enforce attitude change, such as people, external forces and function: setting, subject (who carries the attitude), background, attitude reasoning, desires and needs, acceptance/adjustment, principles, self-esteem, and ego. According to the theory, these factors determine whether an attitude changes/is retained.
3.4. Consistency Theories
Consistency theories generally emphasize the need for consistency between attitudes and behavior and between attitudes and behaviors [44,49]. An individual’s attitude towards a phenomenon should be consistent and non-circumstantial; this is the same for behavior. To achieve consistency, there must be a balance, and the lack of balance creates discomfort. To achieve this balance, one must either alter their attitude or behavior or justify the discrepancy [49]. In addition, Khushboo [49] explains that this theory looks into inconsistencies that may exist or develop between our beliefs, knowledge, and evaluations about an issue. Consistency theories alternatively become the panicle of attitude change theories because, through these, new knowledge upsets the existing equilibrium that may alternatively change and advocate for new behavior and attitude retention. From this theory, these concepts emerged: consistency, balance, discomfort, attitude change, behavior change, and evaluation.
According to the theories of attitude change, four key concepts drive attitude and behavior acquisition and change (learning, knowledge, attitudes and behaviors). What we learn constitutes what we know; it could be what we learn through observation, which speaks to our awareness, learning through stimulus communication or conditioning. In addition, what we learn influences our behavior in the same way that what we know impacts our behavior, which can be affected by factors other than our knowledge and learning. Retaining the punishment or reward agent can influence our behavior towards change. However, attitudes can influence our behaviors depending on specific external influences, people/instigators for change, and function. If these are satisfied, attitudes may change and influence our behavior. However, there is a need for balance and consistency between our attitudes and behaviors for there to be retained behavior.
When new knowledge is introduced, it is understood as a persuasion toward attitude change. In addition, new knowledge is absorbed and judged before it changes attitudes. The perception of new knowledge creates discomfort, and for this discomfort to be resolved, there needs to be consistency, which can only be established by obtaining balance, attitude, and behavior change.
4. Operational Key Concepts Definition and Explanations
Attitude: Attitudes are an acquired inclination to look at and assess things/a phenomenon in a certain way [50]. They can also be described as a feeling which can be felt automatically or post-premeditation. These can either be negative or positive.
Awareness: Is explained as being conscious, alert, and informed. It speaks to being conscious about something without essentially applying understanding [51] and having perceptions about an element or phenomenon, comprehension of their meaning and future status. For this study, observation and awareness will be considered the same concepts explained as a consciousness of a phenomenon concerning its nature, impact, and practices.
Behavior: Although the true definition of behavior is uncertain, Henriques et al. [52] states that this is any observable action exhibited. In this study, the behavior will incorporate practices underpinning habitual behaviors individuals exhibit.
Knowledge: defined as the acquisition of information through learning [53]. In this study, we will also consider knowledge as having a collective/thorough understanding of a phenomenon through information held about it.
5. Results
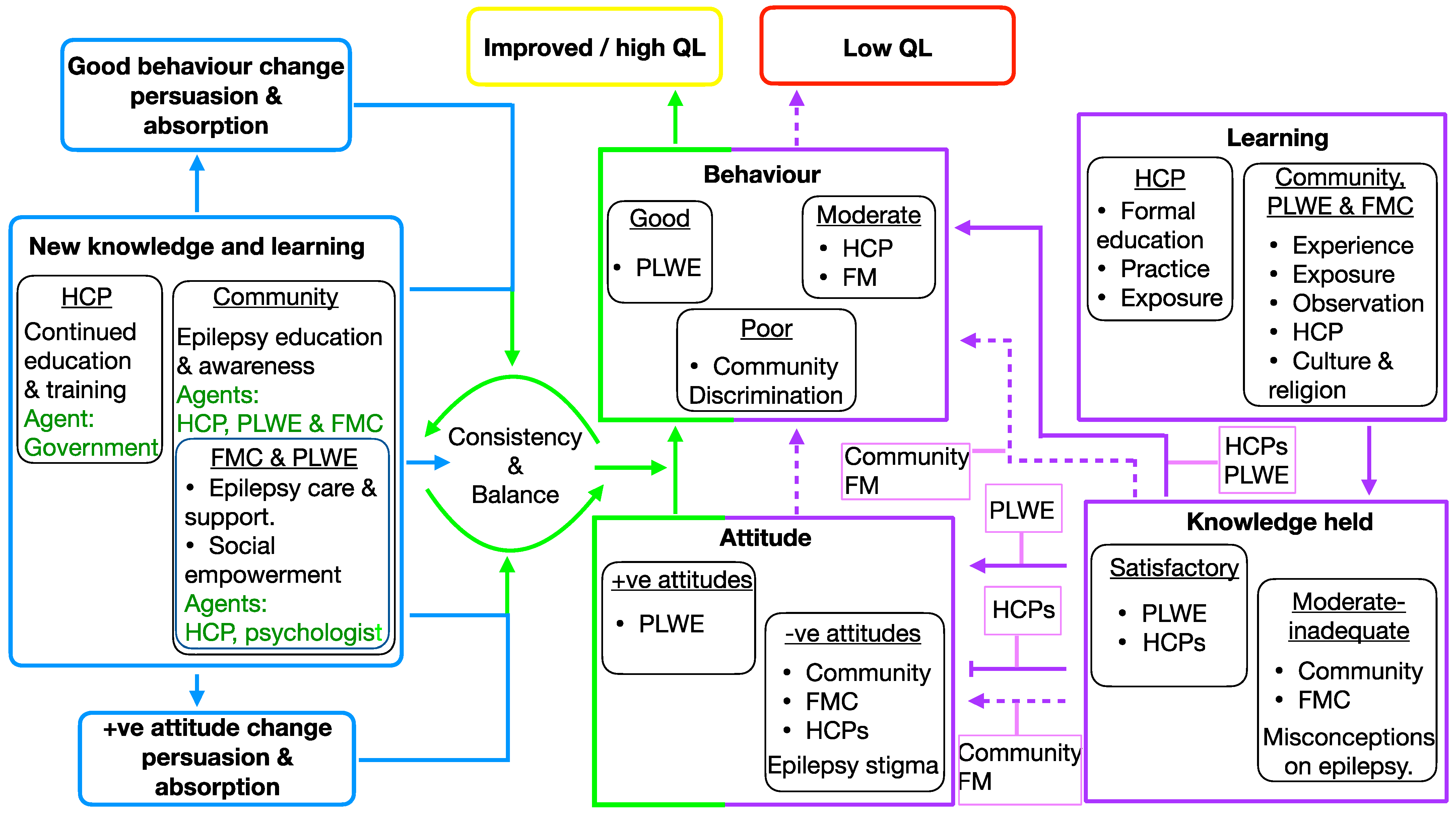
This conceptual framework includes four central concepts covered in the theoretical framework (attitudes, behavior (practices), knowledge, and learning); see Figure 2 below for concept integration as supported by the study findings. Aspects within the purple lines represent the quantitative and qualitative study findings, and blue lines cover study recommendations to mend findings in the purple. Green was adapted from the theoretical framework, though consistency was one of the recommendations from the study.
5.1. Awareness
Amongst the research participants, the researchers found that only community members may not know about epilepsy. During data collection, they were asked if they were aware of epilepsy as a disorder; 59% in Limpopo and 35% in Mpumalanga province reported that they were unaware [36]. This revealed that some participants do not know about epilepsy or have an existing attitude because they are oblivious to it. Concerning learning, we found that awareness was the most significant marker for learned attitudes. Because awareness of something denotes acknowledgement of existence, participants generally appeared aware of epilepsy as a disorder. To those who acknowledged awareness (PLWE, FMCS, HCPs, and some community members), most seem to have learned about epilepsy through exposure and observation, experience, formal education, practice, and HCPs. Specifically, PLWE and their family members (often primary caregivers) learn about epilepsy from HCPs. However, they expressed a need for consistent training and support for these groups. HCPs expressed the need for support and consistent training post-formal education to capacitate and support FMCs properly. Environmental factors, including social and healthcare infrastructure in rural areas, might have implicitly influenced these awareness levels and the subsequent learning process.
5.2. Attitudes
The study found mixed attitudes towards epilepsy. While a slightly above-average number of community members in both Limpopo and Mpumalanga had positive attitudes toward epilepsy [36], negative attitudes were prevalent among family members and caregivers [35]. However, PLWE had a good attitude towards epilepsy. In addition, healthcare providers had negative attitude towards epilepsy. On the other hand, community members and HCPs had negative attitudes towards epilepsy but a somewhat moderate knowledge of epilepsy. FMC scored 63.2% in Limpopo and 51.4% in Mpumalanga on knowledge but had negative attitudes [35]. These attitudes reflect individual perceptions and are shaped by the broader social environment, including prevailing stigmas and cultural beliefs in rural communities. Despite moderate knowledge, the social environment’s influence is evident in the sustained stigma and discrimination against PLWE.
5.3. Knowledge
From the participant groups, most participants (PLWE, HCPs, FM, and some community members) generally knew about epilepsy as a medical condition. However, there was a lack of comprehensive understanding of epilepsy’s impact and appropriate first-aid practices. Community members showed a positive correlation between their knowledge levels and education, suggesting that educational exposure significantly shapes epilepsy knowledge [36]. There was a positive correlation between community members’ knowledge and education level, suggesting that the source of knowledge may be through education and exposure [37]. However, misconceptions and negative attitudes about epilepsy were maintained. These results are different among FMCs and HCPs. HCPs generally had a high knowledge score and negative attitudes. This argues that formal education does not account for “knowledge for the sake of knowing”. Moreover, FMCs scored moderately on knowledge levels [35]. These variations in knowledge can be attributed to environmental factors such as the availability of educational resources and the quality of health information dissemination in rural areas.
5.4. Practices (Behavior)
We found that although HCPs stated that they receive epilepsy training (84.3%) and give counselling to PLWE and their family members. This may prove insufficient as participants (PLWE and FMC) expressed inadequate counselling and information sharing from HCPs who explained that they do not receive consistent training. This further emphasizes the need for epilepsy education and support. As mentioned, individuals who were aware and learned about epilepsy (except professional HCPs) showed poor practices regarding PLWE and epilepsy care. Home-based-carers (within the HCPs cluster) and FMC had inconsistencies regarding care and first aid routines. In addition, most family members had poor practices regarding epileptic seizure first aid [35]. For instance, most reported putting an object in their mouth or praying for the seizure to stop. In addition, they stated that they often feel unprepared to handle a seizure. However, regarding treatment (Western medicine as preferred), FMC ensured good PLWE treatment adherence for PLWE by collecting or buying medication timeously. Issues such as stigma and discrimination against PLWE and their family members persist. Poor practices may be sustained because individuals do not receive intentional knowledge sharing and training on epilepsy. It is arguable that some first aid methods were learned from general community members and passed on through generations as they have not been formally disproven. This explains why ‘spoon in the mouth’ is a consistently known epileptic seizure method. Moreover, family members said they sometimes pray or apply anointing oil to stop the seizure. As stated before, individuals who do not experience punishment (physical, emotional- stress, pain, or psychological–emotional distress) for their behaviors change their practices. Environmental limitations may perpetuate such practices, including the lack of access to current medical information and training in these rural communities.
The results indicate that environmental and social factors significantly impact awareness, attitudes, knowledge, and practices regarding epilepsy in rural South African provinces. Future strategies and interventions must consider these environmental and social dynamics to effectively address PLWE’s challenges and improve their overall quality of life.
6. Implementation
On the one hand, it is clear from the study’s findings that the only participating group that may not be experiencing an imbalance and lack of consistency between attitudes held and behaviors exhibited is PLWE. This is shown by the inconsistencies between knowledge, attitudes, and behaviors held by community members, FMCs, and HCPs. The attitudes and behaviors of HCPs and community members result in PLWE and their FMCs experiencing a low quality of life (QL). This manifests itself in high school dropout, caregiver burden, and psychosocial challenges that they experience.
It is crucial to incorporate environmental and social considerations into the intervention strategies to address these issues. Such an approach would involve the following:
Community-Based Initiatives: Developing community-based programs that integrate human and environmental health considerations is essential. These initiatives could include awareness campaigns, support groups, and educational workshops that not only inform about epilepsy but also address the social and environmental factors contributing to stigma and discrimination. We can foster a more supportive and inclusive environment by engaging community members, PLWE, and FMCs in these initiatives.
Policy Changes: Advocating for policy changes that recognize the intersection of human health and environmental factors is critical. Policies should aim to improve access to quality healthcare in rural areas, enhance educational resources about epilepsy, and support environmental modifications that can aid PLWE’s quality of life. This might include improving healthcare infrastructure in rural areas or providing resources for better community-based and in-home care.
Education and Information Sharing: Enhancing QL for PLWE requires intentional education and information sharing among all relevant stakeholders. Misconceptions about epilepsy can be reduced through structured and strategic dissemination of information. HCPs, due to their pivotal role, should be at the forefront of educating the community, PLWE, and their families. Continuous support and updated training for HCPs, particularly home-based caregivers and community health workers, are essential to ensure this education is effective and current.
Ongoing Training for Healthcare Practitioners: There is a clear need for further education, training, and workshops on epilepsy, as expressed by HCPs. The health department should take responsibility for providing such training, focusing on the specific needs of PLWE and their caregivers. This training should not only cover medical aspects of epilepsy care but also include modules on how to handle the social and environmental aspects that affect PLWE.
Maintaining Consistency in Epilepsy Communication: To ensure a lasting impact, it is imperative to maintain consistency in epilepsy-related communication. This means regularly updating training materials, holding workshops, and engaging with medical professionals and the community.
By implementing these strategies, we aim not only to improve the quality of life for individuals with epilepsy but also to foster a more informed, supportive, and empathetic community. This holistic approach, which considers the medical and socio-environmental aspects of epilepsy, can be adapted to address a range of health psychology diseases that are similarly impacted by stigma, discrimination, and environmental factors. This was demonstrated by the route to improved QL, which requires new knowledge and learning about a health condition to be consistently shared by appropriate agents to persuade the audience to absorb new messages and establish balance and consistency between what is known and exhibited behaviors.
7. Conclusions and Limitations
The study’s findings, encapsulated within the Attitude and Behavior Change Conceptual Framework and visually represented in Figure 2, highlight significant discrepancies in attitudes and behaviors among various participant groups. This figure effectively illustrates the complex dynamics between attitudes, behaviors, knowledge, and learning and their impact on the quality of life (QL) of PLWE and their family members and caregivers (FMCs). PLWE demonstrates a more consistent alignment between attitudes and behaviors than community members, FMCs, and healthcare practitioners (HCPs). Figure 2 is pivotal in understanding these dynamics, showcasing the interconnections between the theoretical concepts and the study’s empirical findings. It visually underscores the potential for enhanced QL through targeted education and information sharing. As the diagram suggests, incorporating environmental and social health perspectives into this framework could significantly deepen our understanding of epilepsy. It highlights the importance of contextual factors such as living conditions, community infrastructure, cultural beliefs, and societal support systems.
In conclusion, the integration of the diagram strengthens the study by providing a clear visual representation of the conceptual framework. It highlights the need for a holistic approach to epilepsy management, encompassing medical, environmental, and social aspects. Future research should expand upon this framework and diagram, exploring how these relationships play out in different environmental and social contexts, to develop more universally applicable strategies for improving the quality of life for PLWE and their families.
While the study and its accompanying diagram offer valuable insights into epilepsy, they are limited in fully capturing the intricate environmental and social nuances influencing the condition. Conducted in rural South Africa, the generalizability of the results and framework to other contexts, especially urban or culturally distinct areas, may need to be revised. This limitation underscores the need for cautious application of these findings in diverse settings beyond the specific study area. Finally, although the focus of this work is on epilepsy, we believe that this is of relevance to relationships between wider social attitudes and knowledge of the disease, especially for stigmatizing conditions affecting mental and neurological health. This again emphasizes the importance of wider health educational programs for attitudinal shifts.
Author Contributions
O.P.M. conceptualized and drafted the manuscript, L.M. supervised the study, did the formal analysis, edited, and proofread. All authors have read and agreed to the published version of the manuscript.
Funding
This study is funded by the GladAfrica Foundation Trust and NIHSS-SAHUDA doctoral scholarship (project number: SDS20/1189). The work reported herein was made possible through funding by the South African Medical Research Council through its Division of Research Capacity Development under the SAMRC Re-searcher Development Award from funding received from the South African National Treasury (SAMRC/RCD/RDA23/24). The content hereof is the sole responsibility of the authors and do not necessarily represent the official views of the SAMRC or the funders.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Human and Clinical Trial Research Ethics Committee of the University of Venda (SHS/20/PSYCH/12/2710, approved 30 October 2020).
Informed Consent Statement
Written informed consent has been obtained from the patients of this study to publish this paper.
Data Availability Statement
Data are contained within the article.
Acknowledgments
The authors acknowledge all participants who agreed to participate in the study, traditional authorities who allowed us to conduct the study in their villages, and A. Maphula for supervision.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the study’s design, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
References
- Sapolsksky, R.M. Determined: A Science of Life without Free Will; Penguin Press: New York, NY, USA, 2023. [Google Scholar]
- Kwon, C.S.; Jacoby, A.; Ali, A.; Austin, J.; Birbeck, G.L.; Braga, P.; Cross, J.H.; de Boer, H.; Dua, T.; Fernandes, P.T.; et al. A systematic review of frequency of felt and enacted stigma in epilepsy and determining factors and attitudes toward persons living with epilepsy—Report from the International League Against Epilepsy Task Force on Stigma in Epilepsy. Epilepsia 2022, 63, 573–597. [Google Scholar] [CrossRef] [PubMed]
- Braga, P.; Hosny, H.; Kakooza-Mwesige, A.; Rider, F.; Tripathi, M.; Guekht, A. How to understand and address the cultural aspects and consequences of diagnosis of epilepsy, including stigma. Epileptic Disord. 2020, 22, 531–547. [Google Scholar] [CrossRef] [PubMed]
- Sabo, U.A.; Buttner, P.; Scher, G. Impact of caregiver burden on health-related quality of life and family functioning of carers of children with epilepsy at the Charlotte Maxeke Johannesburg Academic Hospital, South Africa. S. Afr. J. Child Health 2020, 14, 66–70. [Google Scholar] [CrossRef]
- Pandey, D.K.; Dasgupta, R.; Levy, J.; Wang, H.; Serafini, A.; Habibi, M.; Song, W.; Shafer, P.O.; Loeb, J.A. Enhancing epilepsy self-management and quality of life for adults with epilepsy with varying social and educational backgrounds using PAUSE to Learn Your Epilepsy. Epilepsy Behav. 2020, 111, 107228. [Google Scholar] [CrossRef] [PubMed]
- Gutter, T.; Callenbach, P.M.; Brouwer, O.F.; de Weerd, A.W. Prevalence of sleep disturbances in people with epilepsy and the impact on quality of life: A survey in secondary care. Seizure 2019, 69, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Tombini, M.; Assenza, G.; Quintiliani, L.; Ricci, L.; Lanzone, J.; Di Lazzaro, V. Epilepsy and quality of life: What does really matter? Neurol. Sci. 2021, 42, 3757–3765. [Google Scholar] [CrossRef] [PubMed]
- Riechmann, J.; Willems, L.M.; Boor, R.; Kieslich, M.; Knake, S.; Langner, C.; Neubauer, B.A.; Oberman, B.; Philippi, H.; Reese, J.P.; et al. Quality of life and correlating factors in children, adolescents with Epilepsy, and their caregivers: A cross-sectional multicenter study from Germany. Seizure 2019, 69, 92–98. [Google Scholar] [CrossRef]
- Kale, R. Bringing epilepsy out of the shadows: Wide treatment gap needs to be reduced. BMJ 1997, 315, 2–3. [Google Scholar] [CrossRef]
- Yuan, Y.; Xun, G.; Jia, K.; Zhang, A. A multi-context learning approach for EEG epileptic seizure detection. BMC Syst. Biol. 2018, 12, 47–57. [Google Scholar] [CrossRef]
- World Health Organisation. Epilepsy Fact Sheet. 9 February 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/epilepsy (accessed on 24 October 2023).
- National Institute of Neurological Disorders and Stroke. Epilepsy and Seizures. 15 August 2023. Available online: https://www.ninds.nih.gov/health-information/disorders/epilepsy-and-seizures (accessed on 24 October 2023).
- Muhigwa, A.; Preux, P.M.; Gérard, D.; Marin, B.; Boumediene, F.; Ntamwira, C.; Tsai, C.H. Comorbidities of epilepsy in low and middle-income countries: Systematic review and meta-analysis. Sci. Rep. 2020, 10, 9015. [Google Scholar] [CrossRef]
- Kaddumukasa, M.; Nalubwama, H.; Kaddumukasa, M.N.; Lhatoo, S.; Sewankambo, N.; Katabira, E.; Sajatovic, M.; Blixen, C. Barriers to epilepsy care in Central Uganda, a qualitative interview and focus group study involving PLWE and their caregivers. BMC Neurol. 2019, 19, 161. [Google Scholar] [CrossRef] [PubMed]
- Kolahi, A.A.; Abbasi-Kangevari, M.; Bakhshaei, P.; Mahvelati-Shamsabadi, F.; Tonekaboni, S.H.; Farsar, A.R. Knowledge, attitudes, and practices among mothers of children with epilepsy: A study in a teaching hospital. Epilepsy Behav. 2017, 69, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Kabel, A.M.; Algethami, S.A.; Algethami, B.S.; Alzahrani, A.S.; Almutairi, S.K.; Almutairi, A.S. Knowledge, perceptions, and attitudes of students of health-related science colleges towards Epilepsy in Taif, Saudi Arabia. J. Fam. Med. Prim. Care 2020, 9, 2394. [Google Scholar] [CrossRef] [PubMed]
- Altowayan, R.; Aloqaily, H.; Almutairi, A.; Almassri, R.; Alharbi, B.; Alsallum, G.; Alhabib, R.; Alkharaz, G.; Alateyah, A.; Alharbi, Y.; et al. Level of awareness and attitudes toward epilepsy in Qassim, Saudi Arabia: A cross-sectional study. Epilepsy Behav. 2019, 90, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Shawahna, R.; Jaber, M. Assessing knowledge and attitudes of Palestinian undergraduate nursing students toward epilepsy and patients with epilepsy: A cross-sectional study. Epilepsy Behav. 2020, 102, 106811. [Google Scholar] [CrossRef] [PubMed]
- Unsar, S.; Özdemir, Ö.; Erol, Ö.; Bıkmaz, Z.; Bulut, E.Y. Evaluation of nursing students’ epilepsy-related knowledge and attitudes. Epilepsy Behav. 2020, 111, 107167. [Google Scholar] [CrossRef] [PubMed]
- Henok, A.; Lamaro, T. Knowledge about and attitude towards epilepsy among Menit Community, Southwest Ethiopia. Ethiop. J. Health Sci. 2017, 27, 47–58. [Google Scholar] [CrossRef]
- Elsakka, E.E.; El Said, H.G.; Aly, S.M.; Ibrahim, E.A.; Abd Elmaksoud, M.S. Knowledge, skills, and attitudes towards children with epilepsy among egyptian parents: A comparative cross-sectional study. Epilepsy Res. 2021, 172, 106573. [Google Scholar] [CrossRef]
- Asare, R.O. Knowledge, attitude and practice regarding epilepsy among nurses in asutifi north district. 2019. Available online: http://www.udsspace.uds.edu.gh/bitstream/123456789/2277/1/KNOWLEDGE%2c%20ATTITUDE%20AND%20PRACTICE%20REGARDING%20EPILEPSY%20AMONG%20NURSES%20IN%20ASUTIFI%20NORTH%20DISTRICT.pdf (accessed on 17 June 2023).
- Tjimuine, K. Demographic and socio-economic factors influencing medical care-seeking behaviour among people who experienced mental health issues in Namibia. Doctoral Dissertation, University of Namibia, Windhoek, Namibia, 2023. [Google Scholar]
- Mamman, R.; Grewal, J.; Garrone, J.N.; Schmidt, J. Biopsychosocial factors of quality of life in individuals with moderate to severe traumatic brain injury: A scoping review. Qual. Life Res. 2023, 1–25. Available online: https://pubmed.ncbi.nlm.nih.gov/37925675/ (accessed on 13 December 2023). [CrossRef]
- Alemu, A.; Dendir, G.; Gonfa, A.; Sisay, Y.; Tadesse, T.; Abebe, A. Health-related quality of life and associated factors among adult patients with epilepsy in public hospitals of Wolaita zone, southern Ethiopia. An embedded mixed method study. Epilepsy Behav. 2023, 145, 109316. [Google Scholar] [CrossRef]
- Dada, O.T.; Tongo, S.O.; Uzzi, F.O.; Faniran, G.B.; Afon, A.O. Seasonal Cycles in Environmental Quality of Peri-Urban Areas and their Variability in Nigeria: Some Preliminary Findings. KIU J. Soc. Sci. 2023, 9, 147–157. [Google Scholar]
- Yesmin, M.F.; Chowdhury, M.R.; Bornee, F.A.; Kader, M.; Mondal, M.N.; Hossain, M.; Rashid, M. Urban–rural difference in factors associated with childhood functional difficulty in Bangladesh: A cross-sectional study. Front. Public Health 2023, 11, 1270853. [Google Scholar] [CrossRef] [PubMed]
- Rabipour, S. Air chemical particles and pollution quality association with mental health: A case for depression and anxiety among Iranian university students in Iranian cities with lower air quality. Chem. Rev. Lett. 2023, 6, 66–78. [Google Scholar]
- Eze, C.N.; Ebuehi, O.M.; Brigo, F.; Otte, W.M.; Igwe, S.C. Effect of health education on trainee teachers’ knowledge, attitudes, and first aid management of epilepsy: An interventional study. Seizure 2015, 33, 46–53. [Google Scholar] [CrossRef]
- Helde, G.; Bovim, G.; Bråthen, G.; Brodtkorb, E. A structured, nurse-led intervention program improves quality of life in patients with epilepsy: A randomized, controlled trial. Epilepsy Behav. 2005, 7, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Caller, T.A.; Ferguson, R.J.; Roth, R.M.; Secore, K.L.; Alexandre, F.P.; Zhao, W.; Tosteson, T.D.; Henegan, P.L.; Birney, K.; Jobst, B.C. A cognitive behavioral intervention (HOBSCOTCH) improves quality of life and attention in epilepsy. Epilepsy Behav. 2016, 57, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Yadegary, M.A.; Maemodan, F.G.; Nayeri, N.D.; Ghanjekhanlo, A. The effect of self-management training on health-related quality of life in patients with epilepsy. Epilepsy Behav. 2015, 50, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Musekwa, O.P.; Makhado, L.; Maphula, A.; Mabunda, J.T. How much do we know? Assessing public knowledge, awareness, impact, and awareness guidelines for epilepsy: A systematic review. Open Public Health J. 2020, 13, 794–807. [Google Scholar] [CrossRef]
- Makhado, T.G.; Lebese, R.T.; Maputle, M.S. Development and Validation of Epilepsy Life Skills Guidelines for Primary School Learners and Teachers in Limpopo and Mpumalanga Provinces. Children 2023, 10, 1194. [Google Scholar] [CrossRef]
- Musekwa, O.P.; Makhado, L.; Maphula, A. Caregivers’ and Family Members’ Knowledge Attitudes and Practices (KAP) towards Epilepsy in Rural Limpopo and Mpumalanga, South Africa. Int. J. Environ. Res. Public Health 2023, 20, 5222. [Google Scholar] [CrossRef]
- Musekwa, O.P.; Makhado, L.; Maphula, A. Public Perception of Epilepsy in Rural Limpopo and Mpumalanga Provinces: A Quantitative Study on Knowledge, Awareness, and Attitudes. Challenges 2022, 13, 65. [Google Scholar] [CrossRef]
- Mangena-Netshikweta, M.L. Perceptions about epilepsy in the Limpopo Province of the Republic of South Africa. Curationis 2003, 26, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Eastman, R. Epilepsy in South Africa. Acta Neurol. Scand. 2005, 112, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Muchada, I.F.; Wilmshurst, J.M.; Laing, N.; Davies, E.H.; Fieggen, K. A qualitative study exploring caregivers’ experiences, perspectives, and expectations for precision medicine in epilepsy in South Africa. Epilepsy Behav. 2021, 117, 107873. [Google Scholar] [CrossRef]
- Gilani, Z.A.; Naidoo, K.; Ross, A. A review of “medical” knowledge of epilepsy amongst isiZulu-speaking patients at a regional hospital in KwaZulu-Natal. Afr. J. Prim. Health Care Fam. Med. 2015, 7, 789. [Google Scholar] [CrossRef]
- Egenasi, C.K.; Moodley, A.A.; Steinberg, W.J.; Joubert, G. The perceptions and attitudes of patients with epilepsy to the use of a seizure diary, South Africa. S. Afr. Fam. Pract. 2023, 65, 5503. [Google Scholar] [CrossRef]
- Munyadziwa, M. Knowledge, Attitude, and Awareness of Community Members Regarding Epilepsy in Selected Villages of Limpopo and Mpumalanga Provinces, South Africa; University of Venda: cvccvvLimpopo, South Africa, 2022. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Simonson, M.R.; Maushak, N. Instructional technology and attitude change. In Handbook of Research on IEducational Communications and Technology; Scholastic: New York, NY, USA, 1996. [Google Scholar]
- Olufemi, T.D. Theories of attitudes. Psychol. Attitudes. 2012. Available online: https://www.researchgate.net/profile/Temitayo-Adewuyi-2/publication/370124518_In_Psychology_of_Attitudes_THEORIES_OF_ATTITUDES/links/6440296539aa471a524ca414/In-Psychology-of-Attitudes-THEORIES-OF-ATTITUDES.pdf (accessed on 13 May 2023).
- Leyva, R.; Beckett, C. Testing and unpacking the effects of digital fake news: On presidential candidate evaluations and voter support. AI Soc. 2020, 35, 969–980. [Google Scholar] [CrossRef]
- Rajpaul, V. Towards a Dynamic Social Judgement Theory—An experiment Using Fake News. Ph.D. Thesis, University of Pretoria, Pretoria, South Africa, 2022. [Google Scholar]
- Carpenter, C.; Boster, F.J.; Andrews, K.R. Functional attitude theory. In The SAGE Handbook of Persuasion: Developments in Theory and Practice; SAGE Publications: New York, NY, USA, 2013; pp. 104–119. [Google Scholar]
- Khushboo, S. Top Three Theories of Attitude Change. N.d. Available online: https://www.yourarticlelibrary.com/organization/attitude/top-3-theories-of-attitude-with-diagram/63835 (accessed on 15 May 2023).
- Cherry, K. Attitudes and behavior in psychology. Verywell Mind. 2019. Available online: https://d1wqtxts1xzle7.cloudfront.net/58765604/attitudes-how-they-form-change-shape-behavior-279589720190401-68603-x2xhp3-libre.pdf?1554140563=&response-content-disposition=inline%3B+filename%3DAttitudes_and_Behavior_in_Psychology.pdf&Expires=1703080703&Signature=BeSOHCiuRC6zbBs2zKOd~m0f8OCWkvndcIUPjCFdJDfYcshhb0chnaodmsjdJ~w4EkVKjhtcUcAxANa7igk403H2KnEftrHiZf2gZspGlFSzevi9JkIqoqp3DiNSsO2U0o9917gojcIrZ~4JsRYIMpZz8zJlWeK~yTiq9efI5WVGzt12EdLlQGRTfbAEd7iAocBY~Kc3ICXSrxmsIWWZMJirPUQdzDdRXLMrKnbbppFxG6cF0St170JF2yBv2EV8i8wyEktzLZiOhDQNMiNRglPezcpW~s6d41gNLadqyS9A2GquttKT8gBE981Kbq8w1ats~6luzvjJY0yi~GbanA__&Key-Pair-Id=APKAJLOHF5GGSLRBV4ZA (accessed on 13 May 2023).
- Gafoor, K.A. Considerations in the Measurement of Awareness. 2012. Available online: https://eric.ed.gov/?id=ED545374 (accessed on 5 June 2023).
- Henriques, G.; Michalski, J. Defining Behavior and its Relationship to the Science of Psychology. Integr. Psychol. Behav. Sci. 2020, 54, 328–353. [Google Scholar] [CrossRef]
- Oeberst, A.; Kimmerle, J.; Cress, U. What is knowledge? Who creates it? Who possesses it? The need for novel answers to old questions. In Mass Collaboration and Education; Springer: Cham, Switzerland, 2016; pp. 105–124. [Google Scholar]
Figure 1.
Conceptual framework according to theories of attitude change.

Figure 2.
Attitude and behavior change conceptual framework. Explanatory-sequential mixed methods was employed on PLWE, FMCs, HCPs, and community members. Dark purple lines (![Challenges 15 00002 i001]() ) represent the interaction and relationship between concepts (learning, knowledge held, attitudes, and behavior) as represented by the findings of the study. Solid dark purple lines with arrow end point (
) represent the interaction and relationship between concepts (learning, knowledge held, attitudes, and behavior) as represented by the findings of the study. Solid dark purple lines with arrow end point (![Challenges 15 00002 i002]() ) show the direction of the relationship, light purple lines (
) show the direction of the relationship, light purple lines (![Challenges 15 00002 i003]() ) show which participants are aligned to which direction. Dotted lines with arrow end point (
) show which participants are aligned to which direction. Dotted lines with arrow end point (![Challenges 15 00002 i004]() ) show that there may be a causal relationship but it is not conclusively strong enough. Solid lines with vertical end point (
) show that there may be a causal relationship but it is not conclusively strong enough. Solid lines with vertical end point (![Challenges 15 00002 i005]() ) show that there was no relationship found. Blue solid lines with arrow end point (
) show that there was no relationship found. Blue solid lines with arrow end point (![Challenges 15 00002 i006]() ) represent study recommendations and interventions highlighted by the participants which will potentially lead to behavior and attitude change. However, the green solid lines with arrow end point (
) represent study recommendations and interventions highlighted by the participants which will potentially lead to behavior and attitude change. However, the green solid lines with arrow end point (![Challenges 15 00002 i007]() ) indicate acceptance and application of interventions and recommendations which may lead to increased QL if successful.
) indicate acceptance and application of interventions and recommendations which may lead to increased QL if successful.
 ) represent the interaction and relationship between concepts (learning, knowledge held, attitudes, and behavior) as represented by the findings of the study. Solid dark purple lines with arrow end point (
) represent the interaction and relationship between concepts (learning, knowledge held, attitudes, and behavior) as represented by the findings of the study. Solid dark purple lines with arrow end point ( ) show the direction of the relationship, light purple lines (
) show the direction of the relationship, light purple lines ( ) show which participants are aligned to which direction. Dotted lines with arrow end point (
) show which participants are aligned to which direction. Dotted lines with arrow end point ( ) show that there may be a causal relationship but it is not conclusively strong enough. Solid lines with vertical end point (
) show that there may be a causal relationship but it is not conclusively strong enough. Solid lines with vertical end point ( ) show that there was no relationship found. Blue solid lines with arrow end point (
) show that there was no relationship found. Blue solid lines with arrow end point ( ) represent study recommendations and interventions highlighted by the participants which will potentially lead to behavior and attitude change. However, the green solid lines with arrow end point (
) represent study recommendations and interventions highlighted by the participants which will potentially lead to behavior and attitude change. However, the green solid lines with arrow end point ( ) indicate acceptance and application of interventions and recommendations which may lead to increased QL if successful.
) indicate acceptance and application of interventions and recommendations which may lead to increased QL if successful.
Figure 2.
Attitude and behavior change conceptual framework. Explanatory-sequential mixed methods was employed on PLWE, FMCs, HCPs, and community members. Dark purple lines (![Challenges 15 00002 i001]() ) represent the interaction and relationship between concepts (learning, knowledge held, attitudes, and behavior) as represented by the findings of the study. Solid dark purple lines with arrow end point (
) represent the interaction and relationship between concepts (learning, knowledge held, attitudes, and behavior) as represented by the findings of the study. Solid dark purple lines with arrow end point (![Challenges 15 00002 i002]() ) show the direction of the relationship, light purple lines (
) show the direction of the relationship, light purple lines (![Challenges 15 00002 i003]() ) show which participants are aligned to which direction. Dotted lines with arrow end point (
) show which participants are aligned to which direction. Dotted lines with arrow end point (![Challenges 15 00002 i004]() ) show that there may be a causal relationship but it is not conclusively strong enough. Solid lines with vertical end point (
) show that there may be a causal relationship but it is not conclusively strong enough. Solid lines with vertical end point (![Challenges 15 00002 i005]() ) show that there was no relationship found. Blue solid lines with arrow end point (
) show that there was no relationship found. Blue solid lines with arrow end point (![Challenges 15 00002 i006]() ) represent study recommendations and interventions highlighted by the participants which will potentially lead to behavior and attitude change. However, the green solid lines with arrow end point (
) represent study recommendations and interventions highlighted by the participants which will potentially lead to behavior and attitude change. However, the green solid lines with arrow end point (![Challenges 15 00002 i007]() ) indicate acceptance and application of interventions and recommendations which may lead to increased QL if successful.
) indicate acceptance and application of interventions and recommendations which may lead to increased QL if successful.
) represent the interaction and relationship between concepts (learning, knowledge held, attitudes, and behavior) as represented by the findings of the study. Solid dark purple lines with arrow end point () show the direction of the relationship, light purple lines () show which participants are aligned to which direction. Dotted lines with arrow end point () show that there may be a causal relationship but it is not conclusively strong enough. Solid lines with vertical end point () show that there was no relationship found. Blue solid lines with arrow end point () represent study recommendations and interventions highlighted by the participants which will potentially lead to behavior and attitude change. However, the green solid lines with arrow end point () indicate acceptance and application of interventions and recommendations which may lead to increased QL if successful.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Musekwa, O.P.; Makhado, L. Shifting Behaviors and Attitudes of Socially Stigmatizing Illnesses to Improve Wellbeing: A Conceptual Framework for Epilepsy. Challenges 2024, 15, 2. https://doi.org/10.3390/challe15010002
AMA Style
Musekwa OP, Makhado L. Shifting Behaviors and Attitudes of Socially Stigmatizing Illnesses to Improve Wellbeing: A Conceptual Framework for Epilepsy. Challenges. 2024; 15(1):2. https://doi.org/10.3390/challe15010002
Chicago/Turabian StyleMusekwa, Ofhani Prudance, and Lufuno Makhado. 2024. "Shifting Behaviors and Attitudes of Socially Stigmatizing Illnesses to Improve Wellbeing: A Conceptual Framework for Epilepsy" Challenges 15, no. 1: 2. https://doi.org/10.3390/challe15010002
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.