
Biomechanical Analysis of Titanium Dental Implants in the All-on-4 Treatment with Different Implant–Abutment Connections: A Three-Dimensional Finite Element Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
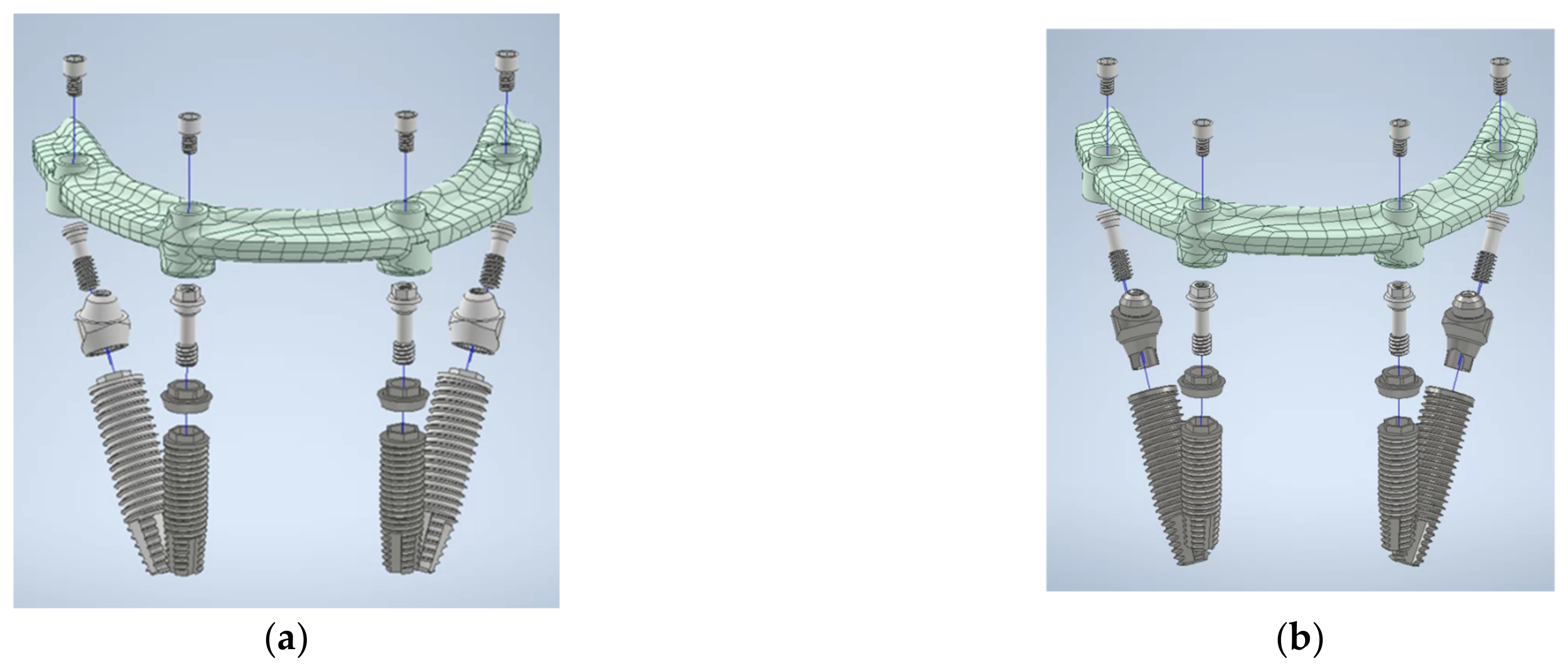
2.1. 3D Finite Element Modeling
2.2. Finite Element Model Analysis
3. Results
3.1. Von Mises Stress Values in the EHC and IHC Groups
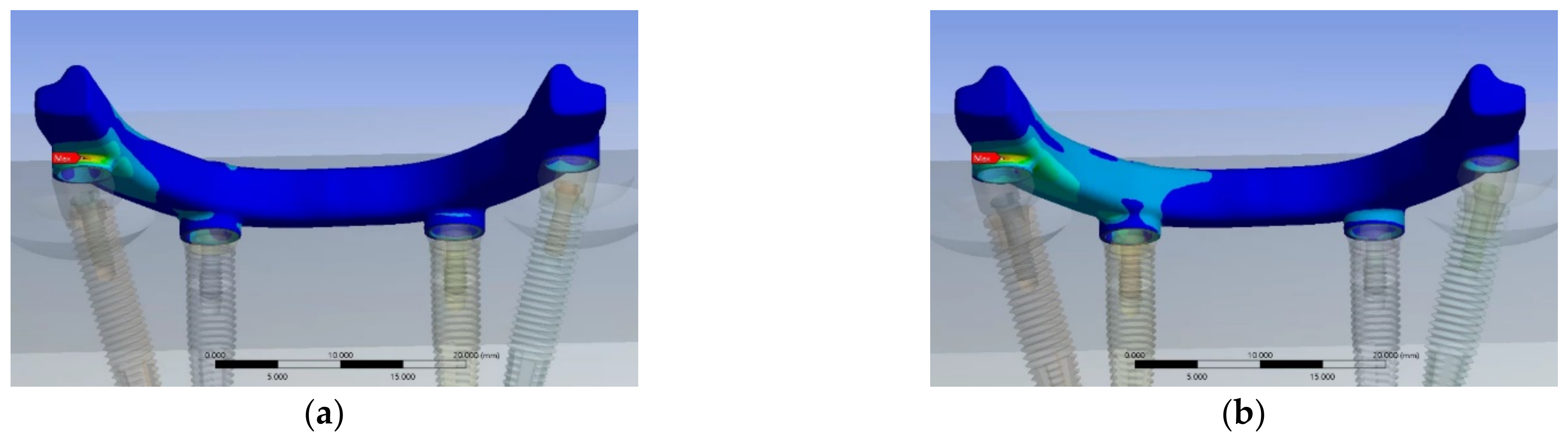
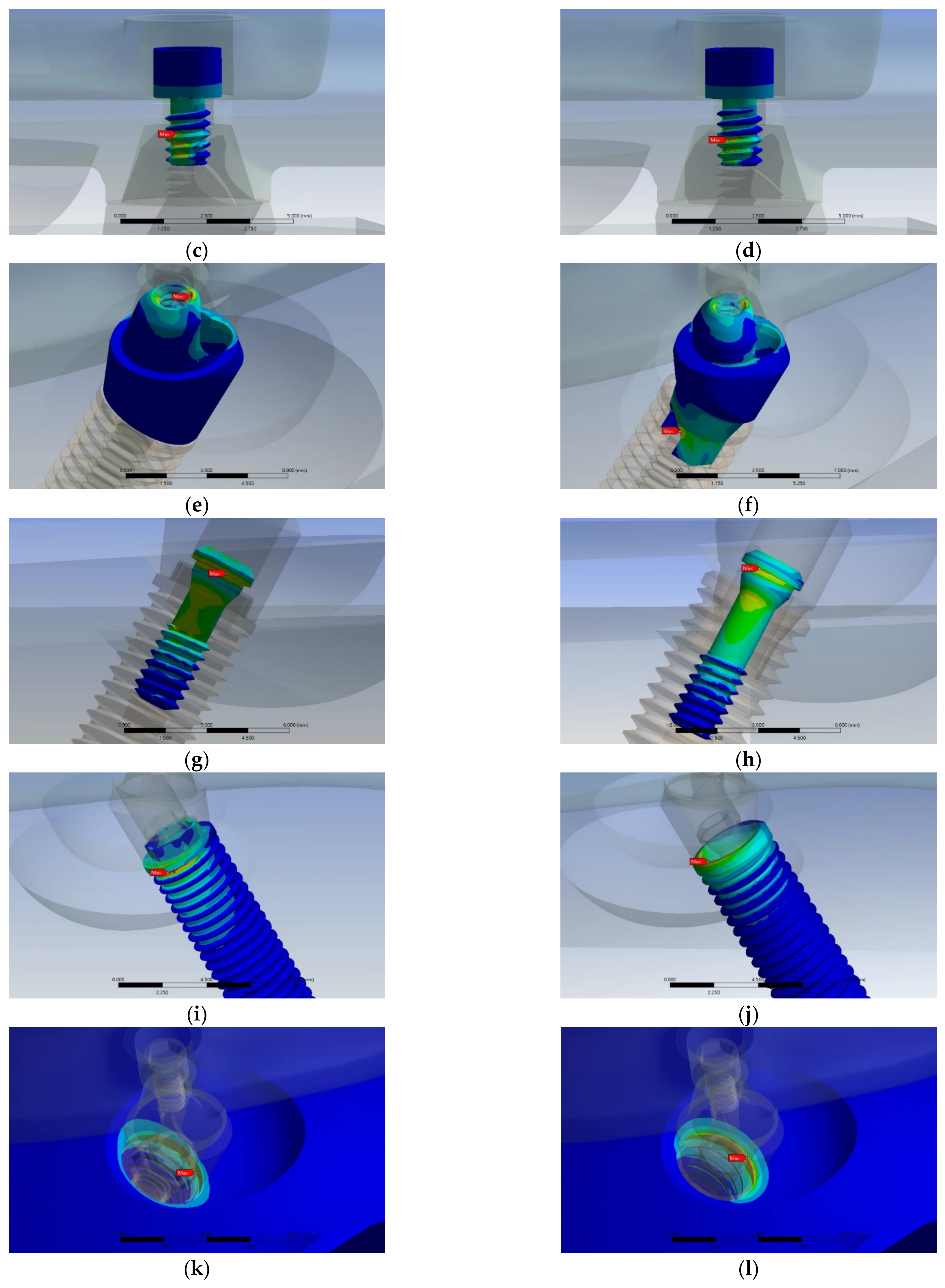
3.2. Stress Distribution Pattern in Each Component of the EHC and IHC Groups
4. Discussion
5. Conclusions
- Both EHCs and IHCs are clinically durable under the tested loading conditions.
- The most stressed region in the EHC and IHC groups was the prosthetic screw, followed by the MUAs, which indicates these components can be the weakest points on the posterior implant within the all-on-4 assembly.
- The peak stress value of the implant screw and implant fixture in the EHC group were 37.75% and 33.03% lower than the IHC group, respectively.
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministry of Health and Welfare of Taiwan. Available online: https://dep.mohw.gov.tw/DOOH/lp-6553-124.html (accessed on 17 January 2018).
- Centers for Disease Control and Prevention. Available online: https://stacks.cdc.gov/view/cdc/82756/cdc_82756_DS1.pdf (accessed on 25 September 2023).
- Soboleva, U.; Rogovska, I. Edentulous Patient Satisfaction with Conventional Complete Dentures. Medicina 2022, 58, 344. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Hu, K. Optimum selection of the dental implant diameter and length in the posterior mandible with poor bone quality—A 3D finite element analysis. Appl. Math. Model. 2011, 35, 446–456. [Google Scholar] [CrossRef]
- Malo, P.; Rangert, B.; Nobre, M. “All-on-Four” immediate-function concept with Brånemark system implants for completely edentulous mandibles retrospective clinical study. Clin. Implant Dent. Relat. Res. 2003, 5, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Maló, P.; de Araújo Nobre, M.; Lopes, A.; Ferro, A.; Botto, J. The All-on-4 treatment concept for the rehabilitation of the completely edentulous mandible: A longitudinal study with 10 to 18 years of follow-up. Clin. Implant Dent. Relat. Res. 2019, 21, 565–577. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.H.; Holmes, C. Contemporary, ‘All-on-4’ Concept. Dent. Clin. N. Am. 2015, 59, 421–470. [Google Scholar] [CrossRef] [PubMed]
- Soto-Penaloza, D.; Zaragozí-Alonso, R.; Penarrocha-Diago, M.; Penarrocha-Diago, M. The all-on-four treatment concept: Systematic review. J. Clin. Exp. Dent. 2017, 9, e474–e488. [Google Scholar] [CrossRef] [PubMed]
- Stoichkov, B.; Kirov, D. Analysis of the causes of dental implant fracture: A retrospective clinical study. Quintessence Int. 2018, 49, 279–286. [Google Scholar] [PubMed]
- Coelho Goiato, M.; Pesqueira, A.A.; Falcón-Antenucci, R.M.; Dos Santos, D.M.; Haddad, M.F.; Bannwart, L.C.; Moreno, A. Stress distribution in implant-supported prosthesis with external and internal implant-abutment connections. Acta Odontol. Scand. 2013, 71, 283–288. [Google Scholar] [CrossRef]
- Geng, J.P.; Tan, K.B.; Liu, G.R. Application of finite element analysis in implant dentistry: A review of the literature. J. Prosthet. Dent. 2001, 85, 585–598. [Google Scholar] [CrossRef]
- Abuhussein, H.; Pagni, G.; Rebaudi, A.; Wang, H.L. The effect of thread pattern upon implant osseointegration. Clin. Oral Implants Res. 2010, 21, 129–136. [Google Scholar] [CrossRef]
- Bozkaya, D.; Muftu, S.; Muftu, A. Evaluation of load transfer characteristics of five different implants in compact bone at different load levels by finite elements analysis. J. Prosthet. Dent. 2004, 92, 523–550. [Google Scholar] [CrossRef] [PubMed]
- Tallarico, M.; Meloni, S.M.; Park, C.-J.; Zadrożny, Ł.; Scrascia, R.; Cicciù, M. Implant Fracture: A Narrative Literature Review. Prosthesis 2021, 3, 267–279. [Google Scholar] [CrossRef]
- Fernández-Asián, I.; Martínez-González, Á.; Torres-Lagares, D.; Serrera-Figallo, M.-Á.; Gutiérrez-Pérez, J.-L. External Connection versus Internal Connection in Dental Implantology. A Mechanical in vitro Study. Metals 2019, 9, 1106. [Google Scholar] [CrossRef]
- De Medeiros, R.A.; Pellizzer, E.P.; Filho, A.J.V.; dos Santos, D.M.; Freitas da Silva, E.V.; Goiato, M.C. Evaluation of marginal bone loss of dental implants with internal or external connections and its association with other variables: A systematic review. J. Prosthet. Dent. 2016, 116, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Steinebrunner, L.; Wolfart, S.; Bossmann, K.; Kern, M. In vitro evaluation of bacterial leakage along the implant-abutment interface of different implant systems. Int. J. Oral Maxillofac. Implants 2005, 20, 875–881. [Google Scholar] [PubMed]
- Pessoa, R.S.; Muraru, L.; Júnior, E.M.; Vaz, L.G.; Sloten, J.V.; Duyck, J.; Jaecques, S.V. Influence of implant connection type on the biomechanical environment of immediately placed implants—CT-based nonlinear, three-dimensional finite element analysis. Clin. Implant Dent. Relat. Res. 2010, 12, 219–234. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.K.; Chowdhary, R.; Kumari, S. Microleakage at the different implant abutment interface: A systematic review. J. Clin. Diagn. Res. 2017, 11, ZE10–ZE15. [Google Scholar] [CrossRef] [PubMed]
- Gracis, S.; Michalakis, K.; Vigolo, P.; Vult von Steyern, P.; Zwahlen, M.; Sailer, I. Internal vs. external connections for abutments/reconstructions: A systematic review. Clin. Oral Implants Res. 2012, 23, 202–216. [Google Scholar] [CrossRef]
- Pera, F.; Menini, M.; Bagnasco, F.; Mussano, F.; Ambrogio, G.; Pesce, P. Evaluation of internal and external hexagon connections in immediately loaded full-arch rehabilitations: A within-person randomized split-mouth controlled trial with a 3-year follow-up. Clin. Implant Dent. Relat. Res. 2021, 23, 562–567. [Google Scholar] [CrossRef]
- Hansson, S. The implant neck: Smooth or provided with retention elements: A biomechanical approach. Clin. Oral Implants Res. 1999, 10, 394–405. [Google Scholar] [CrossRef]
- Wang, Q.; Zhang, Z.Z.; Bai, S.Z.; Zhang, S.F. Biomechanical analysis of stress around the tilted implants with different cantilever lengths in all-on-4 concept. BMC Oral Health 2022, 22, 469. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.L.; Tsai, H.L.; Wu, Y.L.; Hsu, J.T.; Wu, A.Y. Biomechanical Evaluation of Bone Atrophy and Implant Length in Four Implants Supporting Mandibular Full-Arch-Fixed Dentures. Materials 2022, 15, 3295. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.Y.-J.; Hsu, J.-T.; Fuh, L.-J.; Huang, H.-L. Effects of Positions and Angulations of Titanium Dental Implants in Biomechanical Performances in the All-on-Four Treatment: 3D Numerical and Strain Gauge Methods. Metals 2020, 10, 280. [Google Scholar] [CrossRef]
- Saleh Saber, F.; Ghasemi, S.; Koodaryan, R.; Babaloo, A.; Abolfazli, N. The Comparison of Stress Distribution with Different Implant Numbers and Inclination Angles in All-on-four and Conventional Methods in Maxilla: A Finite Element Analysis. J. Dent. Res. Dent. Clin. Dent. Prospect. 2015, 9, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Akca, K.; Iplikcioglu, H. Finite element stress analysis of the influence of staggered versus straight placement of dental implants. Int. J. Oral Maxillofac. Implants 2001, 16, 722–730. [Google Scholar] [PubMed]
- Teixeira, E.R.; Sato, Y.; Akagawa, Y.; Shindoi, N. A comparative evaluation of mandibular finite element models with different lengths and elements for implant biomechanics. J. Oral Rehabil. 1998, 25, 299–303. [Google Scholar] [CrossRef]
- Pierrisnard, L.; Hure, G.; Barquins, M.; Chappard, D. Two dental implants designed for immediate loading: A finite element analysis. Int. J. Oral Maxillofac. Implants 2002, 17, 353–362. [Google Scholar] [PubMed]
- Alkan, I.; Sertgöz, A.; Ekici, B. Influence of occlusal forces on stress distribution in preloaded dental implant screws. J. Prosthet. Dent. 2004, 91, 319–325. [Google Scholar] [CrossRef]
- Lee, S.H.; Hong, M.; Lee, K. Finite Element Analysis of Screw-Tightening Torque Applied to Custom and Conventional Abutment. Glob. J. Health Sci. 2017, 9, 165. [Google Scholar] [CrossRef]
- Pessoa, R.S.; Sousa, R.M.; Pereira, L.M.; Neves, F.D.; Bezerra, F.J.; Jaecques, S.V.; Sloten, J.V.; Quirynen, M.; Teughels, W.; Spin-Neto, R. Bone Remodeling Around Implants with External Hexagon and Morse-Taper Connections: A Randomized, Controlled, Split-Mouth, Clinical Trial. Clin. Implant Dent. Relat. Res. 2017, 19, 97–110. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Reasons for failures of oral implants. J. Oral Rehabil. 2014, 41, 443–476. [Google Scholar] [CrossRef] [PubMed]
- Zembic, A.; Kim, S.; Zwahlen, M.; Kelly, J.R. Systematic review of the survival rate and incidence of biologic, technical, and esthetic complications of single implant abutments supporting fixed prostheses. Int. J. Oral Maxillofac. Implants 2014, 29, 99–116. [Google Scholar] [CrossRef] [PubMed]
- Özdemir Doğan, D.; Polat, N.T.; Polat, S.; Şeker, E.; Gul, E.B. Evaluation of “all-on-four” concept and alternative designs with 3D finite element analysis method. Clin. Implant Dent. Relat. Res. 2014, 16, 501–510. [Google Scholar] [CrossRef]
- Santiago Junior, J.F.; Verri, F.R.; Almeida, D.A.; de Souza Batista, V.E.; Lemos, C.A.; Pellizzer, E.P. Finite element analysis on influence of implant surface treatments, connection and bone types. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 63, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Lemos, C.A.A.; Verri, F.R.; Bonfante, E.A.; Santiago Júnior, J.F.; Pellizzer, E.P. Comparison of external and internal implant-abutment connections for implant supported prostheses. A systematic review and meta-analysis. J. Dent. 2018, 70, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Chun, H.J.; Shin, H.S.; Han, C.H.; Lee, S.H. Influence of implant abutment type on stress distribution in bone under various loading conditions using finite element analysis. Int. J. Oral Maxillofac. Implants 2006, 21, 195–202. [Google Scholar] [PubMed]
- Astrand, P.; Engquist, B.; Dahlgren, S.; Gröndahl, K.; Engquist, E.; Feldmann, H. Astra Tech and Brånemark system implants: A 5-year prospective study of marginal bone reactions. Clin. Oral Implants Res. 2004, 15, 413–420. [Google Scholar] [CrossRef]
- Maeda, Y.; Satoh, T.; Sogo, M. In vitro differences of stress concentrations for internal and external hex implant-abutment connections: A short communication. J. Oral Rehabil. 2006, 33, 75–78. [Google Scholar] [CrossRef]
- Tribst JP, M.; Dal Piva AM, O.; Anami, L.C.; Borges AL, S.; Bottino, M.A. Influence of implant connection on the stress distribution in restorations performed with hybrid abutments. J. Osseointegr. 2019, 11, 507–512. [Google Scholar]
- Chang, H.S.; Chen, Y.C.; Hsieh, Y.D.; Hsu, M.L. Stress distribution of two commercial dental implant systems: A three-dimensional finite element analysis. J. Dent. Sci. 2013, 8, 261–271. [Google Scholar] [CrossRef]
- Quaresma, S.E.; Cury, P.R.; Sendyk, W.R.; Sendyk, C. A finite element analysis of two different dental implants: Stress distribution in the prosthesis, abutment, implant, and supporting bone. J. Oral Implantol. 2008, 34, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Cicciù, M.; Cervino, G.; Terranova, A.; Risitano, G.; Raffaele, M.; Cucinotta, F.; Santonocito, D.; Fiorillo, L. Prosthetic and Mechanical Parameters of the Facial Bone under the Load of Different Dental Implant Shapes: A Parametric Study. Prosthesis 2019, 1, 41–53. [Google Scholar] [CrossRef]
- Gibbs, C.H.; Mahan, P.E.; Lundeen, H.C.; Brehnan, K.; Walsh, E.K.; Sinkewiz, S.L.; Ginsberg, S.B. Occlusal forces during chewing—Influences of biting strength and food consistency. J. Prosthet. Dent. 1981, 46, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Apostolov, N.; Chakalov, I.; Drajev, T. Measurement of the Maximum Bite Force in the Natural Dentition with a Gnathodynamometer. MedInform J. Med. Dent. Pract. 2014, 1, 70–75. [Google Scholar] [CrossRef]
- Eerikainen, E.; Kononen, M. Forces required by complete dentures for penetrating food in simulated function. J. Oral Rehabil. 1987, 14, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Taheri, R.A.; Jarrahi, A.; Farnoosh, G.; Karimi, A. A comparative finite element simulation of stress in dental implant–bone interface using isotropic and orthotropic material models in three mastication cycles. J. Braz. Soc. Mech. Sci. Eng. 2018, 40, 489. [Google Scholar] [CrossRef]
- Dhatrak, P.; Girme, V.; Shirsat, U.; Sumanth, S.; Deshmukh, V. Significance of Orthotropic Material Models to Predict Stress Around Bone-Implant Interface Using Numerical Simulation. BioNanoScience 2019, 9, 652–659. [Google Scholar] [CrossRef]
- Pietroń, K.; Mazurkiewicz, Ł.; Sybilski, K.; Małachowski, J. Correlation of Bone Material Model Using Voxel Mesh and Parametric Optimization. Materials 2022, 15, 5163. [Google Scholar] [CrossRef]
- Van der Bilt, A. Assessment of mastication with implications for oral rehabilitation: A review. J. Oral Rehabil. 2011, 38, 754–780. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Young’s Modulus (GPa) | Poisson’s Ratio | Yield Strength/MPa |
|---|---|---|---|
| Cortical bone | 13.4 [27] | 0.30 | - |
| Cancellous bone | 1.37 [27] | 0.30 | - |
| Pure Titanium (Implant fixture) | 115 [28] | 0.35 | 680 |
| Ti-6Al-4V alloy (Implant bar, Implant screw, Prosthetic screw, Screws, Abutments) | 110 [29] | 0.33 | 795 |
| Component | Max. Stress/MPa of the EHC Group | Max. Stress/MPa of the IHC Group |
|---|---|---|
| Implant bar | 340.29 | 312.81 |
| Prosthetic screw | 689.00 | 680.52 |
| MUA | 657.39 | 624.37 |
| Implant screw | 326.89 | 525.13 |
| Implant fixture | 350.66 | 523.63 |
| Bone | 98.91 | 93.17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, P.-S.; Tsai, M.-H.; Wu, Y.-L.; Chen, H.-S.; Lei, Y.-N.; Wu, A.Y.-J. Biomechanical Analysis of Titanium Dental Implants in the All-on-4 Treatment with Different Implant–Abutment Connections: A Three-Dimensional Finite Element Study. J. Funct. Biomater. 2023, 14, 515. https://doi.org/10.3390/jfb14100515
Wang P-S, Tsai M-H, Wu Y-L, Chen H-S, Lei Y-N, Wu AY-J. Biomechanical Analysis of Titanium Dental Implants in the All-on-4 Treatment with Different Implant–Abutment Connections: A Three-Dimensional Finite Element Study. Journal of Functional Biomaterials. 2023; 14(10):515. https://doi.org/10.3390/jfb14100515
Chicago/Turabian StyleWang, Pei-Shuang, Ming-Hsu Tsai, Yu-Ling Wu, Hung-Shyong Chen, Yao-Ning Lei, and Aaron Yu-Jen Wu. 2023. "Biomechanical Analysis of Titanium Dental Implants in the All-on-4 Treatment with Different Implant–Abutment Connections: A Three-Dimensional Finite Element Study" Journal of Functional Biomaterials 14, no. 10: 515. https://doi.org/10.3390/jfb14100515