Effects of the Oxygen-Carrying Solution OxyVita C on the Cerebral Microcirculation and Systemic Blood Pressures in Healthy Rats

Abstract
:1. Introduction
2. Results and Discussion
2.1. General Observations
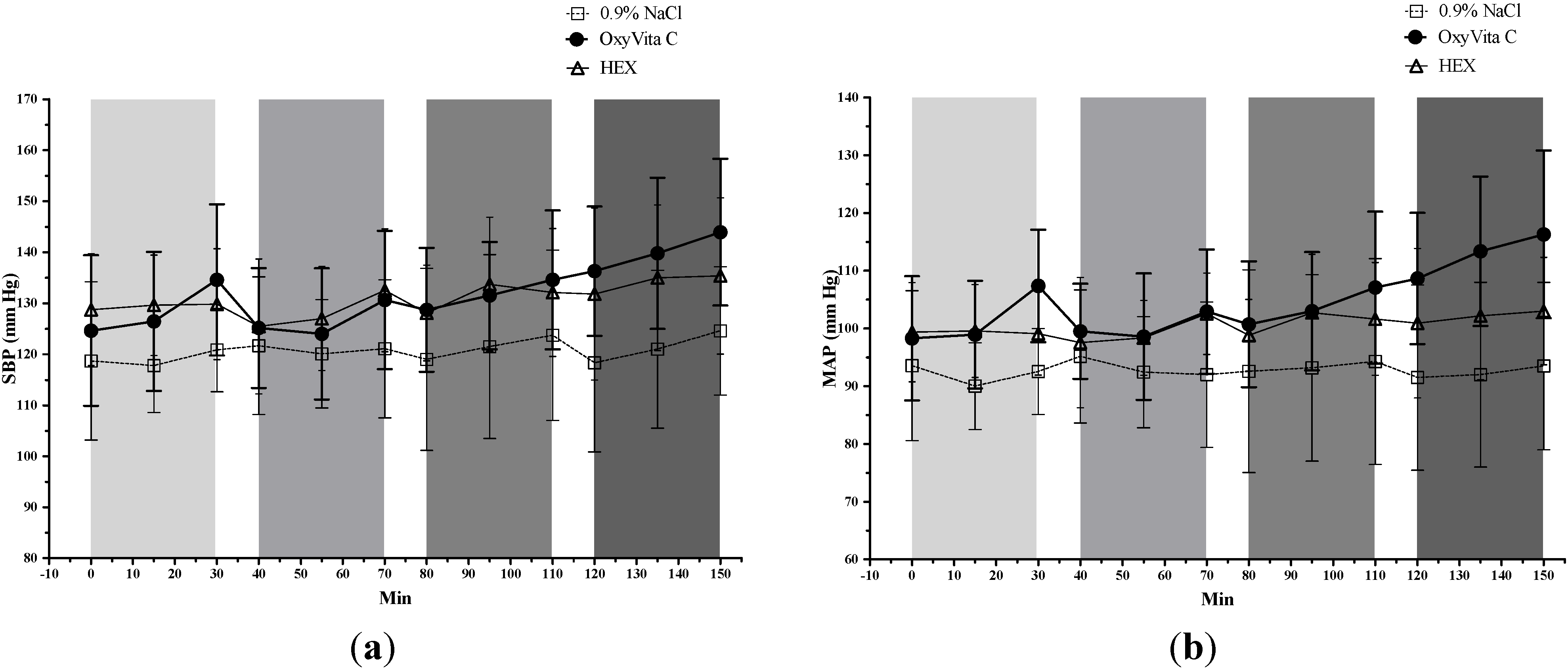
2.2. Systemic Blood Pressures

{kind=link}
{kind=link}
{kind=link}
| Time | Treatment | SBP (mm Hg) | MAP (mm Hg) | DBP (mm Hg) | HR (beats/min) |
|---|---|---|---|---|---|
| T0 (Pre-treatment) | OxyVita C | 124.6 ± 14.8 | 98.3 ± 10.7 | 82.3 ± 9.6 | 385.8 ± 76.3 a |
| 0.9% NaCl | 118.7 ± 15.5 | 93.5 ± 13.0 | 78.5 ± 11.8 | 304.5 ± 61.3 a,b | |
| HEX | 128.7 ± 11.0 | 99.4 ± 8.6 | 81.7 ± 9.9 | 391.6 ± 73.8 b | |
| T30 (After infusion 1) | OxyVita C | 134.6 ± 14.8 #,a | 107.4 ± 9.7 #,a,b | 90.4 ±7.9 | 392.9 ± 72.8 a |
| 0.9% NaCl | 120.9 ± 8.2 a | 92.5 ± 7.4 a | 76.5 ± 7.6 | 308.3 ± 41.9 a,b | |
| HEX | 129.8 ± 10.9 | 99.1 ± 7.2 b | 80.7 ± 8.6 | 367.0 ± 79.2 b | |
| T40 (Before infusion 2) | OxyVita C | 125.1 ± 11.7 | 99.5 ± 8.2 | 84.1 ± 8.2 | 388.5 ± 90.0 |
| 0.9% NaCl | 121.7 ± 13.5 | 95.2 ± 11.5 | 79.0 ± 11.1 | 338.0 ± 35.8 | |
| HEX | 125.5 ± 13.2 | 97.5 ± 11.3 | 79.7 ± 12.5 | 349.8 ± 89.4 | |
| T70 (After infusion 2) | OxyVita C | 130.6 ± 13.6 # | 102.9 ± 10.8 | 84.8 ± 10.3 | 383.5 ± 78.9 |
| 0.9% NaCl | 121.1 ± 13.6 | 92.0 ± 12.6 | 76.7 ± 12.0 | 318.1 ± 43.7 | |
| HEX | 132.5 ± 12.0 | 102.5 ± 7.0 | 85.0 ± 4.8 | 363.6 ± 79.4 | |
| T80 (Before infusion 3) | OxyVita C | 128.7 ± 12.1 | 100.7± 10.9 a | 83.9 ± 10.2 | 387.3 ± 97.1 |
| 0.9% NaCl | 119.0 ± 17.8 | 92.6 ± 17.5 a,b | 76.8 ± 16.5 | 335.8 ± 65.4 | |
| HEX | 128.1 ± 9.4 | 98.8 ± 6.2 b | 81.4 ± 5.9 | 377.7 ± 72.5 | |
| T110 (After infusion 3) | OxyVita C | 134.6 ± 13.6 # | 107.1 ± 13.2 #,a | 90.1 ± 13.5 | 388.1 ± 98.9 |
| 0.9% NaCl | 123.7 ± 16.7 | 94.3 ± 17.8 a | 78.8 ± 17.3 | 331.0 ± 44.6 * | |
| HEX | 132.1 ± 12.5 | 101.6 ± 9.8 | 83.5 ± 7.3 | 387.7 ± 76.6 | |
| T120 (Before infusion 4) | OxyVita C | 136.3 ± 12.7 | 108.6 ± 11.4 | 91.6 ± 11.1 | 382.1 ± 87.2 |
| 0.9% NaCl | 118.3 ± 17.5 | 91.5 ± 16.0 | 75.3 ± 15.6 | 351.2 ± 47.9 | |
| HEX | 131.8 ± 16.9 | 100.9 ± 12.9 | 83.3 ± 10.8 | 370.7 ± 73.8 | |
| T150 (After infusion 4) | OxyVita C | 143.9 ± 14.4 #,*,a | 116.3 ± 14.5 #,*,a,b | 98.9 ± 14.4 | 386.3 ± 84.8 |
| 0.9% NaCl | 124.6 ± 12.6 a | 93.5 ± 14.5 a | 77.1 ± 14.3 | 324.7 ± 56.5 | |
| HEX | 135.4 ± 15.3 | 103.0 ± 9.3 b | 84.8 ± 7.0 | 363.5 ± 68.3 |

2.3. Cerebral Pial Arteriolar Diameters


2.4. Laboratory Analyses
| Time | Group | Hb (g/dL) | pH | PaCO2 (mm Hg) | PaO2 (mm Hg) | Lactate (mmol/L) |
|---|---|---|---|---|---|---|
| T0 (Pre-treatment) | OxyVita C | 12.6 ± 1.0 | 7.389 ± 0.05 | 39 ± 8 | 132 ± 107 | 0.8 ± 0.7 |
| 0.9% NaCl | 12.5 ± 0.9 | 7.349 ± 0.08 | 47 ± 12 | 110 ± 41 | 0.6 ± 0.3 | |
| T30 (After infusion 1) | OxyVita C | 12.3 ± 0.8 | 7.385 ± 0.07 | 37 ± 9 | 130 ± 110 | 0.8 ± 0.6 |
| 0.9% NaCl | 12.4 ± 0.9 | 7.352 ± 0.07 | 46 ± 10 | 116 ± 34 | 0.7 ± 0.3 | |
| T70 (After infusion 2) | OxyVita C | 12.6 ± 0.6 a | 7.359 ± 0.05 § | 40 ± 7 | 146 ± 125 | 0.8 ± 0.5 |
| 0.9% NaCl | 12.3 ± 1.3 b | 7.354 ± 0.06 | 42 ± 9 | 118 ± 29 | 0.7 ± 0.3 | |
| T110 (After infusion 3) | OxyVita C | 12.6 ± 1.1 a | 7.349 ± 0.05 § | 38 ± 6 | 133 ± 99 | 1.1 ± 0.4 a |
| 0.9% NaCl | 12.1 ± 1.1 b | 7.340 ± 0.06 | 43 ± 9 | 111 ± 31 | 0.7 ± 0.2 a | |
| T150 (After infusion 4) | OxyVita C | 13.4 ± 1.2 § a | 7.361 ± 0.06 | 39 ± 10 a,b | 155 ± 129 | 1.2 ± 0.4 a |
| 0.9% NaCl | 12.6 ± 1.1 b | 7.323 ± 0.05 § | 47 ± 8 a | 106 ± 29 | 0.7 ± 0.2 a |
3. Experimental Section
3.1. Animal Preparation and Surgical Procedures
3.2. Test Solutions
3.3. Experimental Protocol
3.4. Statistical Analyses
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Nemoto, M.; Mito, T.; Brinigar, W.S.; Fronticelli, C.; Koehler, R.C. Salvage of focal cerebral ischemic damage by transfusion of high O2-affinity recombinant hemoglobin polymers in mouse. J. Appl. Physiol. 2006, 100, 1688–1691. [Google Scholar] [PubMed]
- Mito, T.; Nemoto, M.; Kwansa, H.; Sampei, K.; Habeeb, M.; Murphy, S.J.; Bucci, E.; Koehler, R.C. Decreased damage from transient focal cerebral ischemia by transfusion of zero-link hemoglobin polymers in mouse. Stroke 2009, 40, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Cao, S.; Kwansa, H.; Crafa, D.; Kibler, K.K.; Koehler, R.C. Transfusion of hemoglobin-based oxygen carriers in the carboxy state is beneficial during transient focal cerebral ischemia. J. Appl. Physiol. 2012, 113, 1709–1717. [Google Scholar] [CrossRef]
- Bouma, G.J.; Muizelaar, J.P.; Choi, S.C.; Newlon, P.G.; Young, H.F. Cerebral circulation and metabolism after severe traumatic brain injury: The elusive role of ischemia. J. Neurosurg. 1991, 75, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Natanson, C.; Kern, S.J.; Lurie, P.; Banks, S.M.; Wolfe, S.M. Cell-free hemoglobin-based blood substitutes and risk of myocardial infarction and death: A meta-analysis. JAMA 2008, 299, 2304–2312. [Google Scholar] [CrossRef] [PubMed]
- Doherty, D.H.; Doyle, M.P.; Curry, S.R.; Vali, R.J.; Fattor, T.J.; Olson, J.S.; Lemon, D.D. Rate of reaction with nitric oxide determines the hypertensive effect of cell-free hemoglobin. Nat. Biotech. 1998, 16, 672–676. [Google Scholar] [CrossRef]
- Olson, J.S.; Foley, E.W.; Rogge, C.; Tsai, A.-L.; Doyle, M.P.; Lemon, D.D. No scavenging and the hypertensive effect of hemoglobin-based blood substitutes. Free Radic. Biol. Med. 2004, 36, 685–697. [Google Scholar] [CrossRef] [PubMed]
- Urbaitis, B.K.; Razynska, A.; Corteza, Q.; Fronticelli, C.; Bucci, E. Intravascular retention and renal handling of purified natural and intramolecularly cross-linked hemoglobins. J. Lab. Clin. Med. 1991, 117, 115–121. [Google Scholar] [PubMed]
- Alayash, A.I. Oxygen therapeutics: Can we tame haemoglobin? Nat. Rev. Drug Discov. 2004, 3, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Acharya, S.A.; Friedman, J.M.; Manjula, B.N.; Intaglietta, M.; Tsai, A.G.; Winslow, R.M.; Malavalli, A.; Vandegriff, K.; Smith, P.K. Enhanced molecular volume of conservatively pegylated hb: (SP-PEG5K)6-Hba is non-hypertensive. Artif. Cells Blood Substit. Immobil. Biotechnol. 2005, 33, 239–255. [Google Scholar] [CrossRef] [PubMed]
- Alayash, A.I.; D’Agnillo, F.; Buehler, P.W. First-generation blood substitutes: What have we learned? Biochemical and physiological perspectives. Expert Opin. Biol. Ther. 2007, 7, 665–675. [Google Scholar] [CrossRef] [PubMed]
- Harrington, J.P.; Wollocko, H. Molecular design properties of OxyVita hemoglobin, a new generation therapeutic oxygen carrier: A review. J. Funct. Biomater. 2011, 2, 414–424. [Google Scholar] [CrossRef] [PubMed]
- Bucci, E.; Razynska, A.; Kwansa, H.; Matheson-Urbaitis, B.; O’Hearne, M.; Ulatowski, J.A.; Koehler, R.C. Production and characteristics of an infusible oxygen-carrying fluid based on hemoglobin intramolecularly cross-linked with sebacic acid. J. Lab. Clin. Med. 1996, 128, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Harrington, J.P.; Wollocko, J.; Kostecki, E.; Wollocko, H. Physicochemical characteristics of oxyvita hemoglobin, a zero-linked polymer: Liquid and powder preparations. Artif. Cells Blood Substit. Biotechnol. 2011, 39, 12–18. [Google Scholar] [CrossRef]
- Matheson, B.; Kwansa, H.E.; Bucci, E.; Rebel, A.; Koehler, R.C. Vascular response to infusions of a nonextravasating hemoglobin polymer. J. Appl. Physiol. 2002, 93, 1479–1486. [Google Scholar] [PubMed]
- Harrington, J.; Wollocko, H. Pre-clinical studies using oxyvita hemoglobin, a zero-linked polymeric hemoglobin: A review. J. Artif. Organs 2010, 13, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Song, B.K.; Nugent, W.H.; Moon-Massat, P.F.; Auker, C.R.; McCarron, R.; Pittman, R.N. Effects of top-loading a zero-link bovine hemoglobin, oxyvita, on systemic and microcirculatory variables. Mil. Med. 2013, 178, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Abutarboush, R.; Scultetus, A.; Arnaud, F.; Auker, C.; McCarron, R.; Moon-Massat, P.F. Effects of N-acetyl-L-cysteine and hyaluronic acid on HBOC-201-induced systemic and cerebral vasoconstriction in the rat. Curr. Drug Discov. Technol. 2013, 10, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Povlishock, J.T.; Kontos, H.A.; DeWitt, D.S.; Wei, E.P. Effects of mechanical brain injury and acute hypertension upon the cerebral vasculature: Morphophysiological considerations of those factors involved in the genesis of cerbrovascular dysfunction. In Cerebral Microcirculation and Metabolism; Cervos-Navarro, J., Fritschka, E., Eds.; Raven Press: New York, NY, USA, 1981; pp. 67–74. [Google Scholar]
- Linninger, A.A.; Gould, I.G.; Marinnan, T.; Hsu, C.Y.; Chojecki, M.; Alaraj, A. Cerebral microcirculation and oxygen tension in the human secondary cortex. Ann. Biomed. Eng. 2013, 41, 2264–2284. [Google Scholar] [CrossRef] [PubMed]
- Holt, D.C.; Fedinec, A.L.; Vaughn, A.N.; Leffler, C.W. A brief communication: Age and species dependence of pial arteriolar responses to topical carbon monoxide in vivo. Exp. Biol. Med. 2007, 232, 1465–1469. [Google Scholar] [CrossRef]
- Levasseur, J.E.; Wei, E.P.; Raper, A.J.; Kontos, H.A.; Patterson, J.L. Detailed description of a cranial window technique for acute and chronic experiments. Stroke 1975, 6, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Rosenblum, W.; Zweifach, B. Cerebral microcirculation in the mouse brain: Spontaneous and drug-induced changes in flow and vascular diameter. Arch. Neurol. 1963, 9, 414–423. [Google Scholar] [CrossRef] [PubMed]
- Drabkin, D.L.; Austin, J.H. Spectrophotometric studies: II. Preparations from washed blood cells; nitric oxide hemoglobin and sulfhemoglobin. J. Biol. Chem. 1935, 112, 51–65. [Google Scholar]
- Evelyn, K.A.; Malloy, H.T. Micro determination of oxyhemoglobin, methemoglobin sulfhemoglobin in a singlesample of blood. J. Biol. Chem. 1938, 126, 655–662. [Google Scholar]
- Vandegriff, K.D.; Young, M.A.; Lohman, J.; Bellelli, A.; Samaja, M.; Malavalli, A.; Winslow, R.M. CO-MP4, a polyethylene glycol-conjugated haemoglobin derivative and carbon monoxide carrier that reduces myocardial infarct size in rats. Br. J. Pharmacol. 2008, 154, 1649–1661. [Google Scholar] [CrossRef] [PubMed]
- Rebel, A.; Cao, S.; Kwansa, H.; Doré, S.; Bucci, E.; Koehler, R.C. Dependence of acetylcholine and ADP dilation of pial arterioles on heme oxygenase after transfusion of cell-free polymeric hemoglobin. Am. J. Physiol. Heart Circ. Physiol. 2006, 290, H1027–H1037. [Google Scholar] [CrossRef] [PubMed]
- Rebel, A.; Ulatowski, J.A.; Kwansa, H.; Bucci, E.; Koehler, R.C. Cerebrovascular response to decreased hematocrit: Effect of cell-free hemoglobin, plasma viscosity, and CO2. Am. J. Physiol. Heart Circ. Physiol. 2003, 285, H1600–H1608. [Google Scholar] [PubMed]
- Rosenblum, W.I. Pial arteriolar responses in mouse-brain revisited. Stroke 1976, 7, 283–287. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abutarboush, R.; Aligbe, C.; Pappas, G.; Saha, B.; Arnaud, F.; Haque, A.; Auker, C.; McCarron, R.; Scultetus, A.; Moon-Massat, P. Effects of the Oxygen-Carrying Solution OxyVita C on the Cerebral Microcirculation and Systemic Blood Pressures in Healthy Rats. J. Funct. Biomater. 2014, 5, 246-258. https://doi.org/10.3390/jfb5040246
Abutarboush R, Aligbe C, Pappas G, Saha B, Arnaud F, Haque A, Auker C, McCarron R, Scultetus A, Moon-Massat P. Effects of the Oxygen-Carrying Solution OxyVita C on the Cerebral Microcirculation and Systemic Blood Pressures in Healthy Rats. Journal of Functional Biomaterials. 2014; 5(4):246-258. https://doi.org/10.3390/jfb5040246
Chicago/Turabian StyleAbutarboush, Rania, Chioma Aligbe, Georgina Pappas, Biswajit Saha, Francoise Arnaud, Ashraful Haque, Charles Auker, Richard McCarron, Anke Scultetus, and Paula Moon-Massat. 2014. "Effects of the Oxygen-Carrying Solution OxyVita C on the Cerebral Microcirculation and Systemic Blood Pressures in Healthy Rats" Journal of Functional Biomaterials 5, no. 4: 246-258. https://doi.org/10.3390/jfb5040246
APA StyleAbutarboush, R., Aligbe, C., Pappas, G., Saha, B., Arnaud, F., Haque, A., Auker, C., McCarron, R., Scultetus, A., & Moon-Massat, P. (2014). Effects of the Oxygen-Carrying Solution OxyVita C on the Cerebral Microcirculation and Systemic Blood Pressures in Healthy Rats. Journal of Functional Biomaterials, 5(4), 246-258. https://doi.org/10.3390/jfb5040246