Route and Type of Formulation Administered Influences the Absorption and Disposition of Vitamin B12 Levels in Serum

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Subjects/Samples/Formulations Administered
- (i)
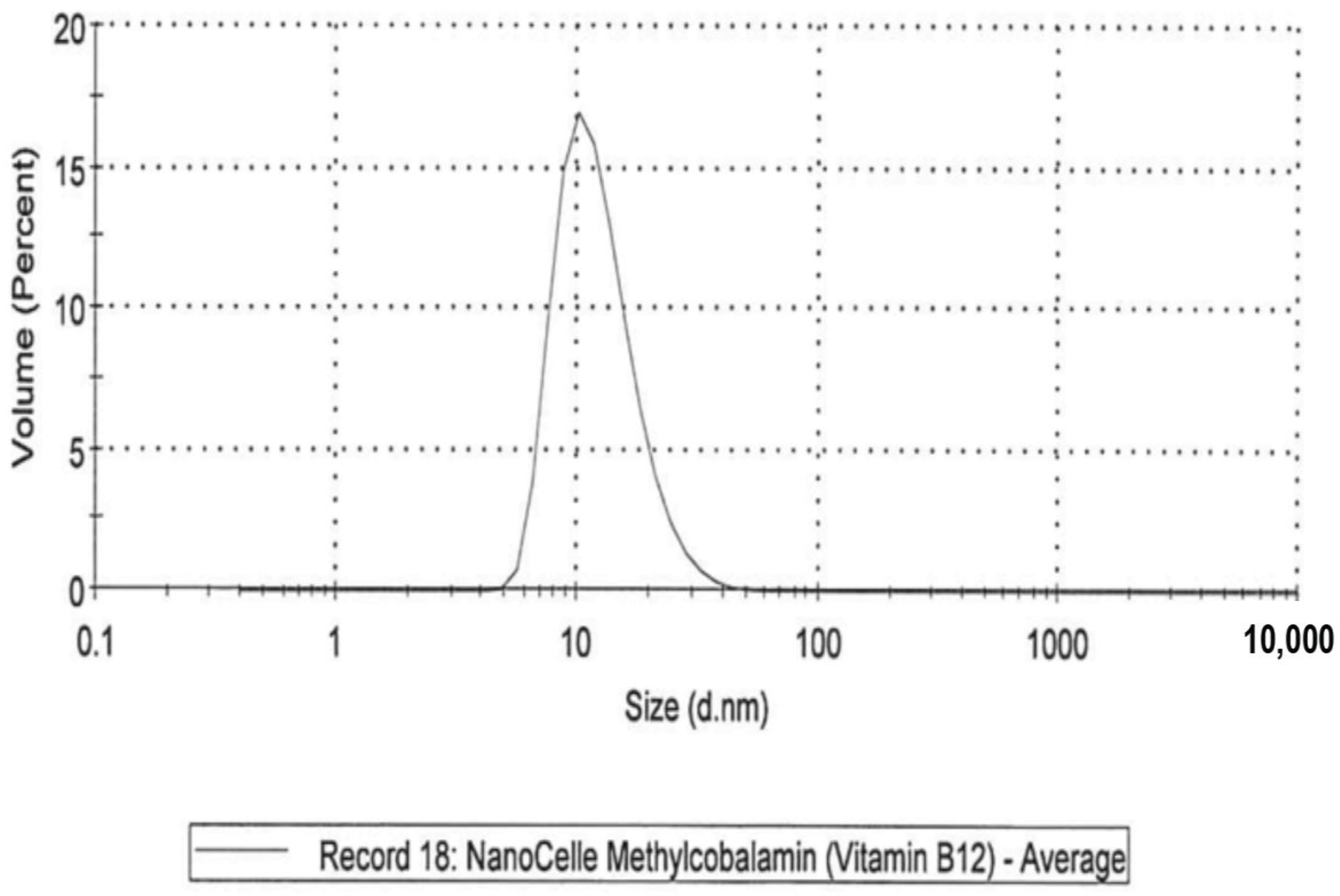
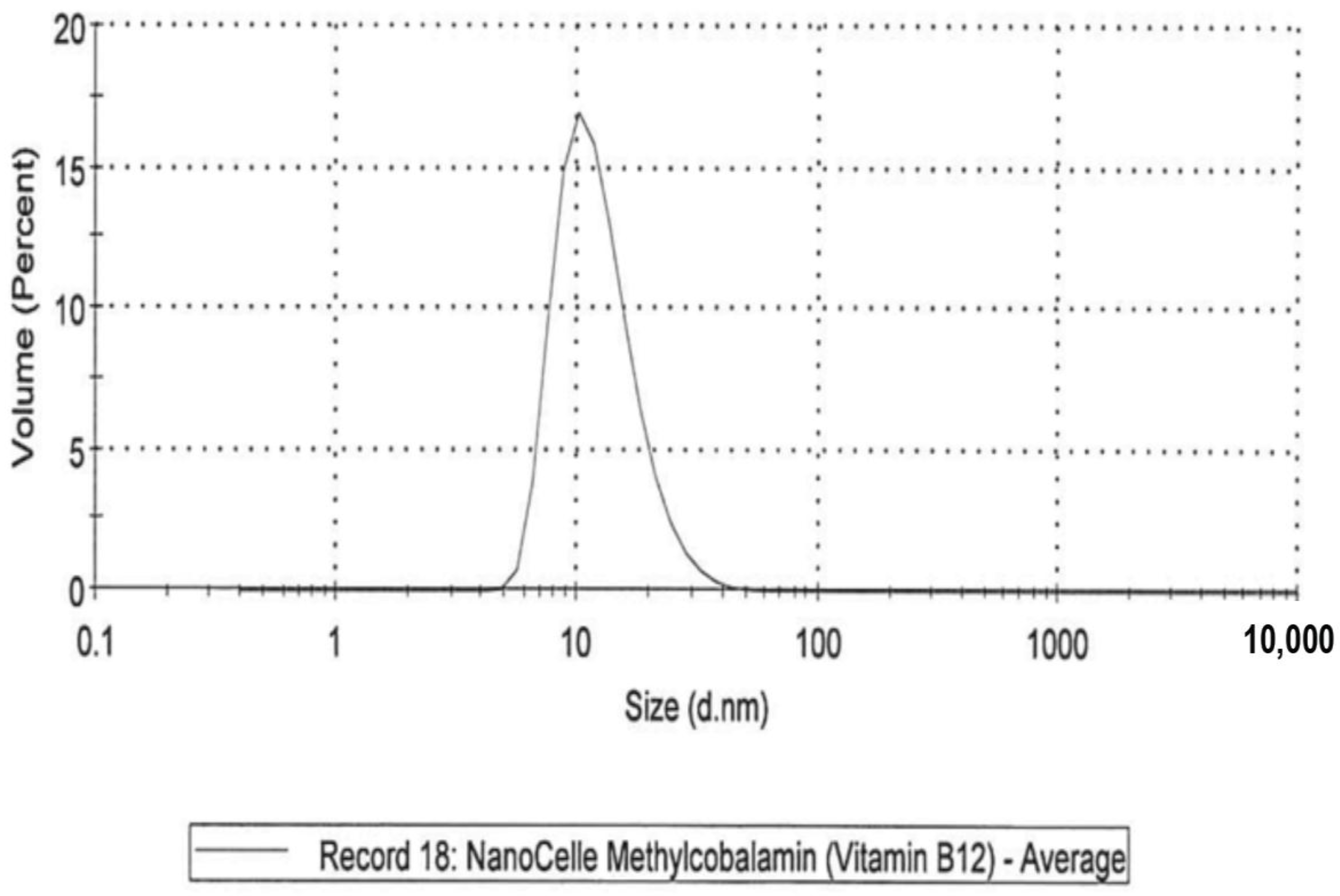
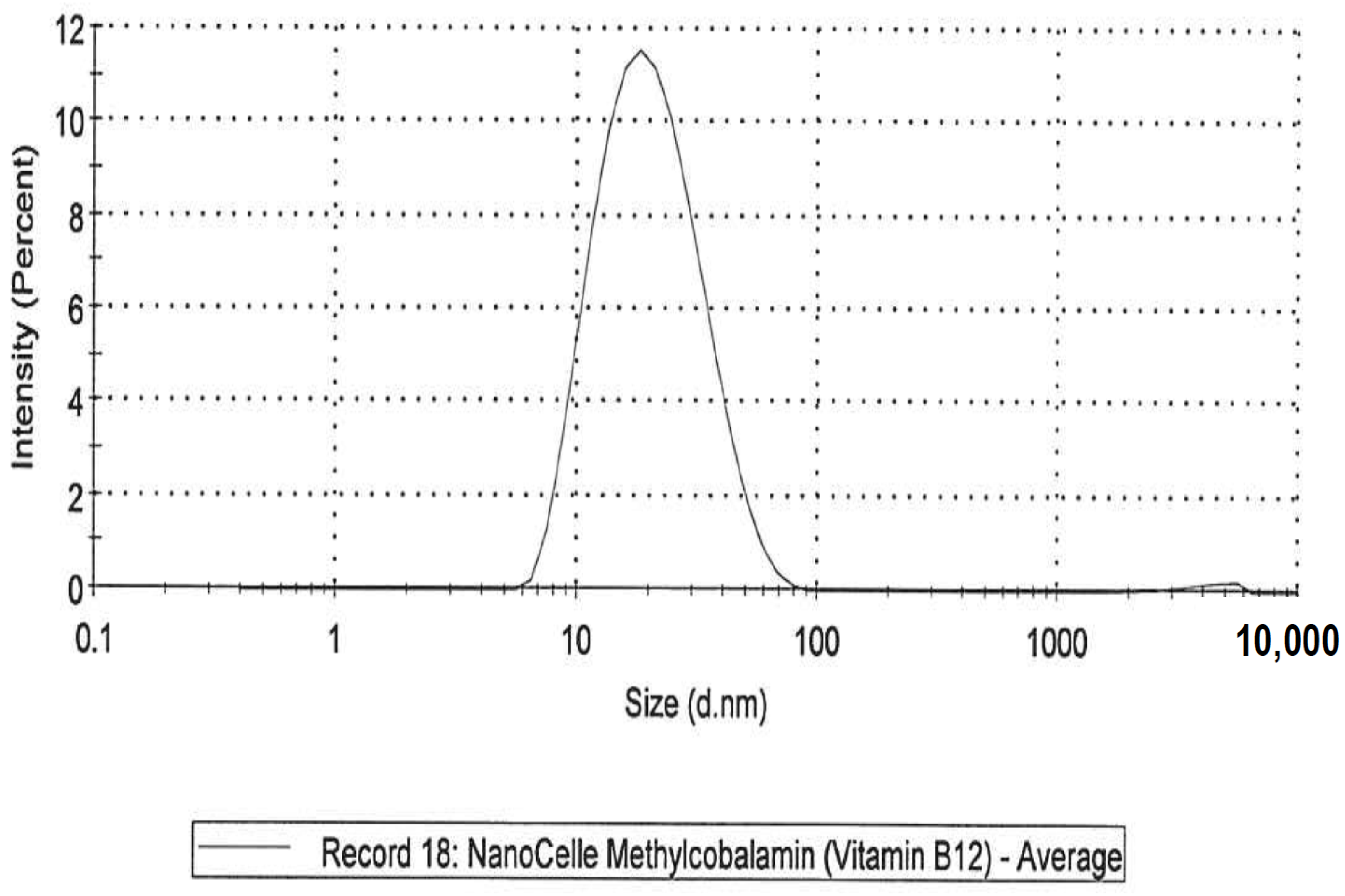
- A NanoCelle (nanoparticle) formulation of B12 comprised an oral-buccal spray (Patent: WO2016141069 [21]). This formulation encompasses nano-sized methylcobalamin B12 particles (two actuations of the pump delivering 1000 µg/300 µL/dose). The particles consist of an inner hydrophobic core and an outer hydrophilic shell, and has an average particle size of about 20 nm (Figure 1 and Figure 2). Particle analysis was carried out by Malvern Zetasizer from Particle Technology Labs (Chicago, IL, USA).
- (ii)
- An emulsion formulation of B12 as cyanocobalamin (two actuations of the pump delivering 1000 µg/340 µL/dose). This formulation was postulated as absorbed through the sublingual mucosa located underneath the tongue by passive diffusion across the membranes.
- (iii)
- A standard tablet formulation of B12 as cyanocobalamin (1000 µg/10 tablets/dose) that is absorbed through the gastrointestinal tract.
- (iv)
- A dissolvable (chewable) tablet of B12 as methylcobalamin (5000 µg/tablet/dose) that is absorbed through the sublingual mucosa via passive diffusion.
- (v)
- A liposome oral spray formulation of B12 as methylcobalamin (two actuations of the pump delivering 1000 µg/300 µL/dose). This formulation provides B12 in vesicles constructed of a phospholipid bi-layer, with particle sizes of approximately 100 nm. This nano-sized liposome preparation is posited to assist with the absorption of B12 across mucosal membranes.
2.2. Serum Vitamin B12 Assay
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Zhang, C.; Rodriguez, E.; Bi, C.; Zheng, X.; Suresh, D.; Suh, K.; Li, Z.; Elsebaei, F.; Hage, D.S. High performance affinity chromatography and related separation methods for the analysis of biological and pharmaceutical agents. Analyst 2018, 143, 374–391. [Google Scholar] [CrossRef] [PubMed]
- Mopuri, R.; Islam, M.S. Medicinal plants and phytochemicals with anti-obesogenic potentials: A review. Biomed. Pharmacother. 2017, 89, 1442–1452. [Google Scholar] [CrossRef] [PubMed]
- Sun, N.N.; Wu, T.Y.; Chau, C.F. Natural dietary and herbal products in anti-obesity treatment. Molecules 2016, 21. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.F.; Zhu, L.L.; Chen, M.; Xu, H.M.; Wang, H.F.; Feng, X.Q.; Zhu, X.P.; Zhou, Q. The optimal choice of medication administration route regarding intravenous, intramuscular, and subcutaneous injection. Patient Preference Adherence 2015, 9, 923–942. [Google Scholar] [PubMed]
- Kwan, K.C. Oral bioavailability and first-pass effects. Drug Metab. Dispos. 1997, 25, 1329–1336. [Google Scholar] [PubMed]
- Rosenthal, M.D.; Carrott, P.W.; Patel, J.; Kiraly, L.; Martindale, R.G. Parenteral or enteral arginine supplementation safety and efficacy. J. Nutr. 2016, 146, 2594s–2600s. [Google Scholar] [CrossRef] [PubMed]
- Van Den Abeele, J.; Rubbens, J.; Brouwers, J.; Augustijns, P. The dynamic gastric environment and its impact on drug and formulation behaviour. Eur. J. Pharm. Sci. 2017, 96, 207–231. [Google Scholar] [CrossRef] [PubMed]
- Morales, J.O.; Fathe, K.R.; Brunaugh, A.; Ferrati, S.; Li, S.; Montenegro-Nicolini, M.; Mousavikhamene, Z.; McConville, J.T.; Prausnitz, M.R.; Smyth, H.D.C. Challenges and future prospects for the delivery of biologics: Oral mucosal, pulmonary, and transdermal routes. AAPS J. 2017, 19, 652–668. [Google Scholar] [CrossRef] [PubMed]
- Hofmann-Amtenbrink, M.; Grainger, D.W.; Hofmann, H. Nanoparticles in medicine: Current challenges facing inorganic nanoparticle toxicity assessments and standardizations. Nanomed. Nanotechnol. Biol. Med. 2015, 11, 1689–1694. [Google Scholar] [CrossRef] [PubMed]
- Chan, V.S. Nanomedicine: An unresolved regulatory issue. Regul. Toxicol. Pharmacol. 2006, 46, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Ali Khan, A.; Mudassir, J.; Mohtar, N.; Darwis, Y. Advanced drug delivery to the lymphatic system: Lipid-based nanoformulations. Int. J. Nanomed. 2013, 8, 2733–2744. [Google Scholar]
- Kesharwani, P.; Gorain, B.; Yeng Low, S.; Ann Tan, S.; Chai Siaw Ling, E.; Khai Lim, Y.; Ming Chin, C.; Yee Lee, P.; Mey Lee, C.; Haw Ooi, C.; et al. Nanotechnology based approaches for anti-diabetic drugs delivery. Diabetes Res. Clin. Pract. 2017, 136, 52–77. [Google Scholar] [CrossRef] [PubMed]
- Shoji, Y.; Nakashima, H. Nutraceutics and delivery systems. J. Drug Target. 2004, 12, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Stern, S.T.; McNeil, S.E. Nanotechnology safety concerns revisited. Toxicol. Sci. 2008, 101, 4–21. [Google Scholar] [CrossRef] [PubMed]
- Szebeni, J.; Storm, G. Complement activation as a bioequivalence issue relevant to the development of generic liposomes and other nanoparticulate drugs. Biochem. Biophys. Res. Commun. 2015, 468, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Grimaldi, N.; Andrade, F.; Segovia, N.; Ferrer-Tasies, L.; Sala, S.; Veciana, J.; Ventosa, N. Lipid-based nanovesicles for nanomedicine. Chem. Soc. Rev. 2016, 45, 6520–6545. [Google Scholar] [CrossRef] [PubMed]
- Ranganathan, R.; Madanmohan, S.; Kesavan, A.; Baskar, G.; Krishnamoorthy, Y.R.; Santosham, R.; Ponraju, D.; Rayala, S.K.; Venkatraman, G. Nanomedicine: Towards development of patient-friendly drug-delivery systems for oncological applications. Int. J. Nanomed. 2012, 7, 1043–1060. [Google Scholar]
- Watanabe, F. Vitamin b12 sources and bioavailability. Exp. Biol. Med. 2007, 232, 1266–1274. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, F.; Samman, S. Vitamin b12 in health and disease. Nutrients 2010, 2, 299–316. [Google Scholar] [CrossRef] [PubMed]
- Masucci, L.; Goeree, R. Vitamin b12 intramuscular injections versus oral supplements: A budget impact analysis. Ont. Health Technol. Assess. Ser. 2013, 13, 1–24. [Google Scholar] [PubMed]
- Hall, S.M.; Vitetta, L.; Zhou, Y.; Rutolo, D.A., Jr.; Coulson, S.M. Transmucosal and Transdermal Delivery Systems. International Patent Application No. PCT/US2016/020468, 9 September 2016. [Google Scholar]
- Ispir, E.; Serdar, M.A.; Ozgurtas, T.; Gulbahar, O.; Akin, K.O.; Yesildal, F.; Kurt, I. Comparison of four automated serum vitamin b12 assays. Clin. Chem. Lab. Med. 2015, 53, 1205–1213. [Google Scholar] [CrossRef] [PubMed]
- Martinez, M.N.; Amidon, G.L. A mechanistic approach to understanding the factors affecting drug absorption: A review of fundamentals. J. Clin. Pharmacol. 2002, 42, 620–643. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, M.; Rutkowski, B.; Debska-Slizien, A. Vitamins and microelement bioavailability in different stages of chronic kidney disease. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, A.G.; Gornati, R.; Sabbioni, E.; Chiriva-Internati, M.; Cobos, E.; Jenkins, M.R.; Bernardini, G. Nanotechnology and human health: Risks and benefits. J. Appl. Toxicol. 2010, 30, 730–744. [Google Scholar] [CrossRef] [PubMed]
- Szebeni, J.; Moghimi, S.M. Liposome triggering of innate immune responses: A perspective on benefits and adverse reactions. J. Liposome Res. 2009, 19, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Szebeni, J.; Baranyi, L.; Savay, S.; Milosevits, J.; Bodo, M.; Bunger, R.; Alving, C.R. The interaction of liposomes with the complement system: In vitro and in vivo assays. Methods Enzymol. 2003, 373, 136–154. [Google Scholar] [PubMed]
- Moein Moghimi, S.; Hamad, I.; Bunger, R.; Andresen, T.L.; Jorgensen, K.; Hunter, A.C.; Baranji, L.; Rosivall, L.; Szebeni, J. Activation of the human complement system by cholesterol-rich and pegylated liposomes-modulation of cholesterol-rich liposome-mediated complement activation by elevated serum ldl and hdl levels. J. Liposome Res. 2006, 16, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Moghimi, S.M.; Hamad, I. Liposome-mediated triggering of complement cascade. J. Liposome Res. 2008, 18, 195–209. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Demographic Variable | Males (9) | Females (7) |
|---|---|---|
| Age (years) mean (SD) | 37 (11.8) | 31.4 (5.9) |
| BMI (Kg/m2) | 27.9 (4.6) | 23.6 (2.1) |
| Systolic BP (mmHg) | 132.3 (15.3) | 119.3 (4.2) |
| Diastolic BP (mmHg) | 84.8 (8.9) | 85.3 (7.6) |
| Allergies | – | – |
| Yes | 2 | 2 |
| No | 7 | 5 |
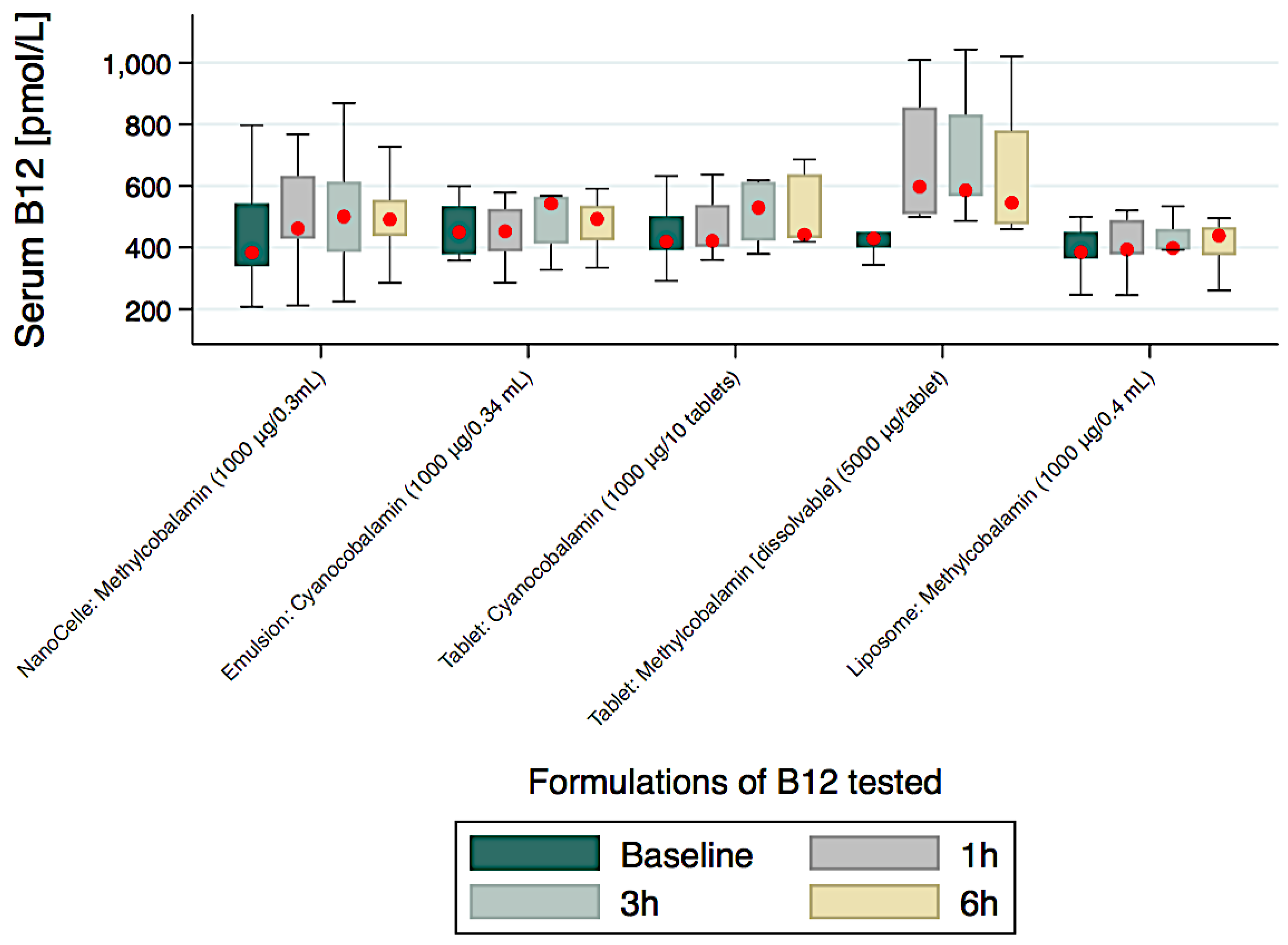
| Collection Times | Formulations | ||||
|---|---|---|---|---|---|
| Nanocelle Ω 1000 µg/0.3 mL | Emulsion 1000 µg/0.3 mL | Tablet 1000 µg/Tablet | Chewable 5000 µg/Tablet ⊥ | Liposome 1000 µg/0.3 mL | |
| Serum B12 Reported as Median (IQR) pmoles/L | |||||
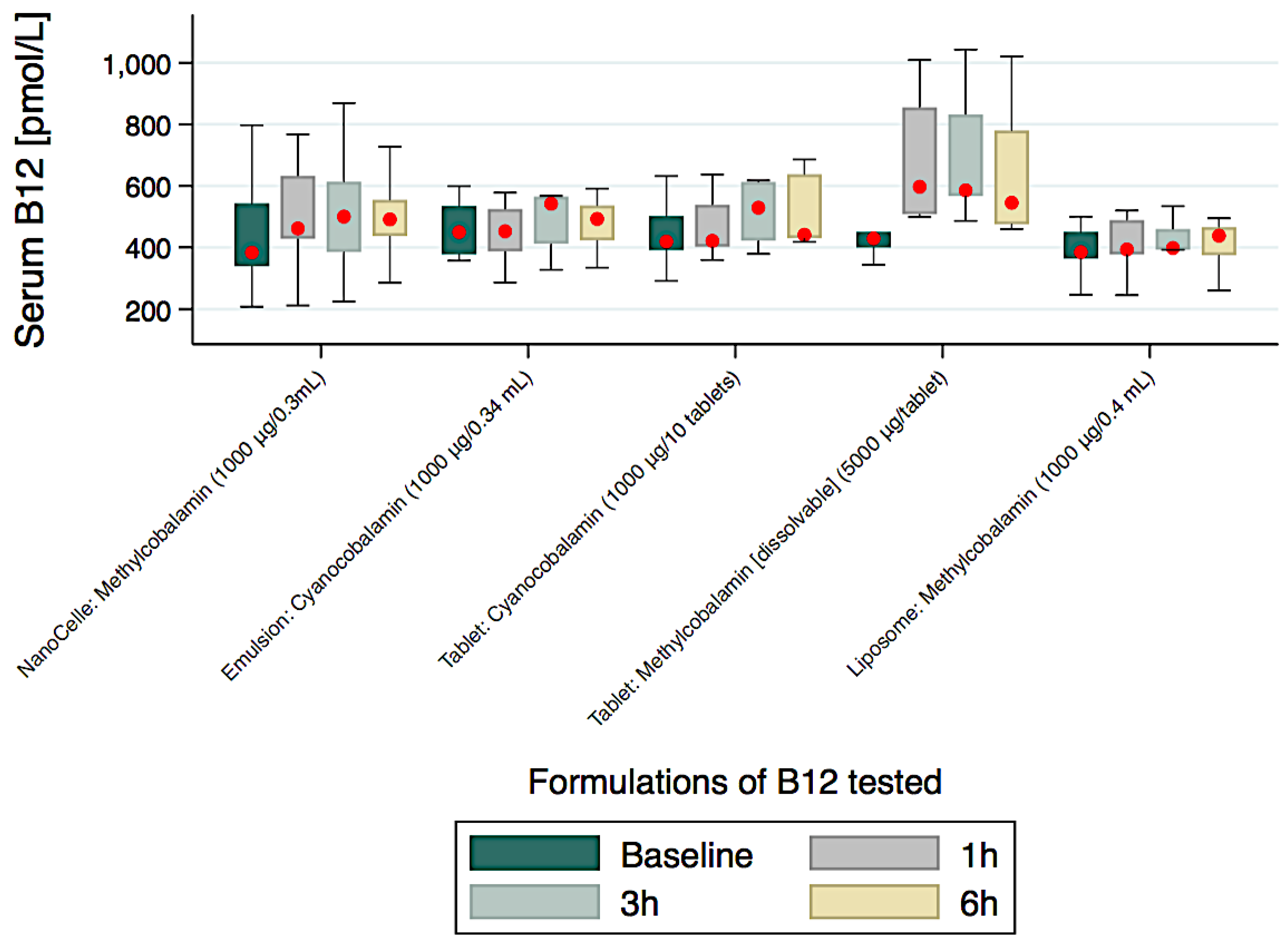
| Baseline | 383 (204) | 450 (157) | 419 (110) | 429 (50) | 385 (86) |
| 1 h | 462 (205) * | 453 (138) | 421 (137) | 597 (327) * | 393 (112) |
| %↑baseline-to-1 h | 21% (p < 0.05) | 1% | 0.5% | 39% | 2% |
| 3 h | 500 (229) * | 542 (154) | 529 (191) | 586 (265) * | 398 (67) |
| 6 h | 491 (118) * | 493 (114) | 441 (208) * | 545 (305) * | 438 (92) * |
| %↑baseline-to-6 h | 28% (p < 0.05) | 10% | 5% | 27% | 14% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitetta, L.; Zhou, J.; Manuel, R.; Dal Forno, S.; Hall, S.; Rutolo, D. Route and Type of Formulation Administered Influences the Absorption and Disposition of Vitamin B12 Levels in Serum. J. Funct. Biomater. 2018, 9, 12. https://doi.org/10.3390/jfb9010012
Vitetta L, Zhou J, Manuel R, Dal Forno S, Hall S, Rutolo D. Route and Type of Formulation Administered Influences the Absorption and Disposition of Vitamin B12 Levels in Serum. Journal of Functional Biomaterials. 2018; 9(1):12. https://doi.org/10.3390/jfb9010012
Chicago/Turabian StyleVitetta, Luis, Joyce Zhou, Rachel Manuel, Serena Dal Forno, Sean Hall, and David Rutolo. 2018. "Route and Type of Formulation Administered Influences the Absorption and Disposition of Vitamin B12 Levels in Serum" Journal of Functional Biomaterials 9, no. 1: 12. https://doi.org/10.3390/jfb9010012