The Effects of Uniquely-Processed Titanium on Balance and Walking Performance in Healthy Older Adults



 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
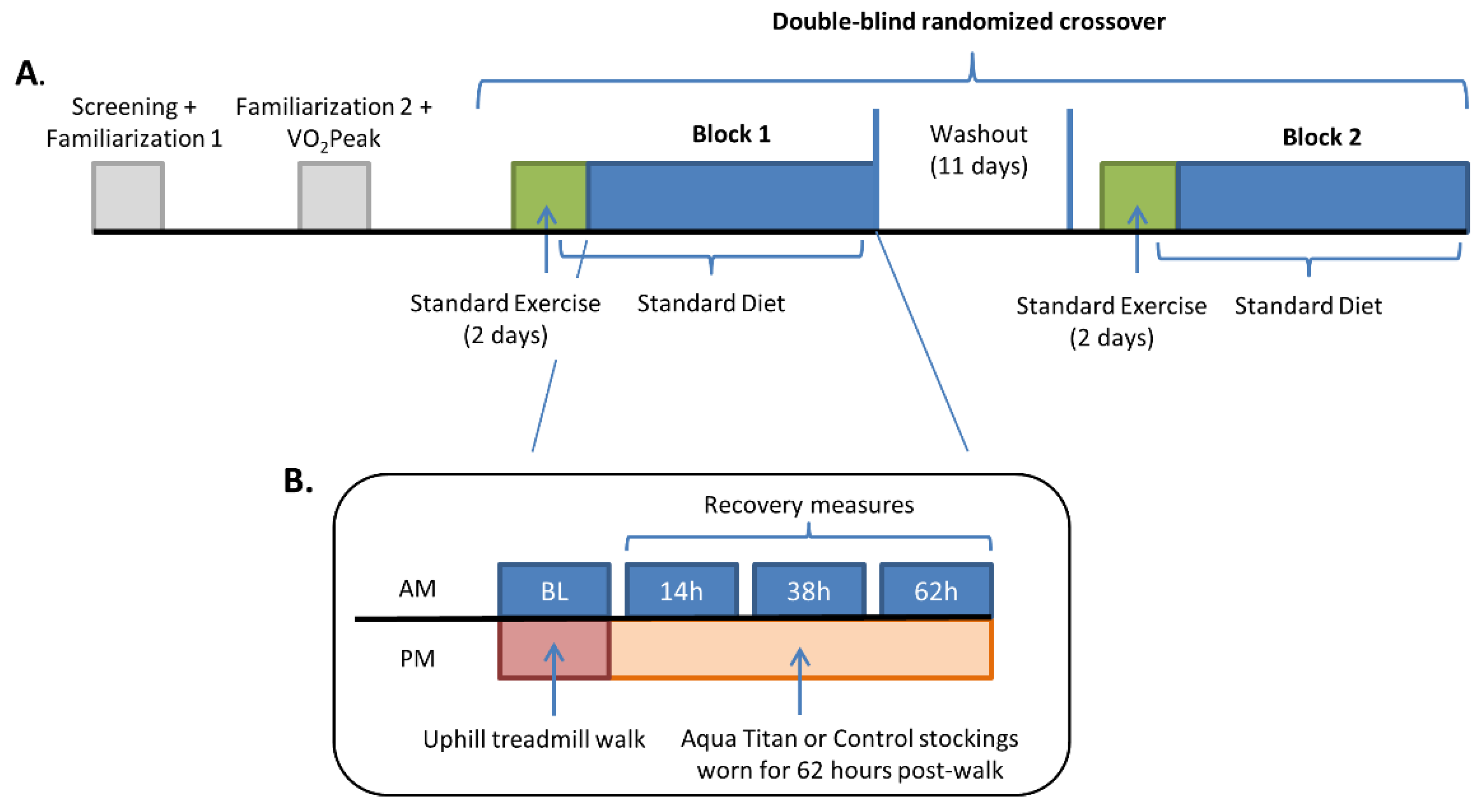
2.2. Experimental Design
2.3. Preliminary Sessions
2.4. Main Trial Procedures
2.4.1. Ankle Range of Motion
2.4.2. Balance
2.4.3. Triceps Surae Short Latency Stretch Reflex Response
2.4.4. Muscle Microvascular Perfusion, Blood Flow and Oxygen Consumption
2.4.5. Submaximal Oxygen Consumption and Walking Performance
2.5. Statistical Analysis
3. Results
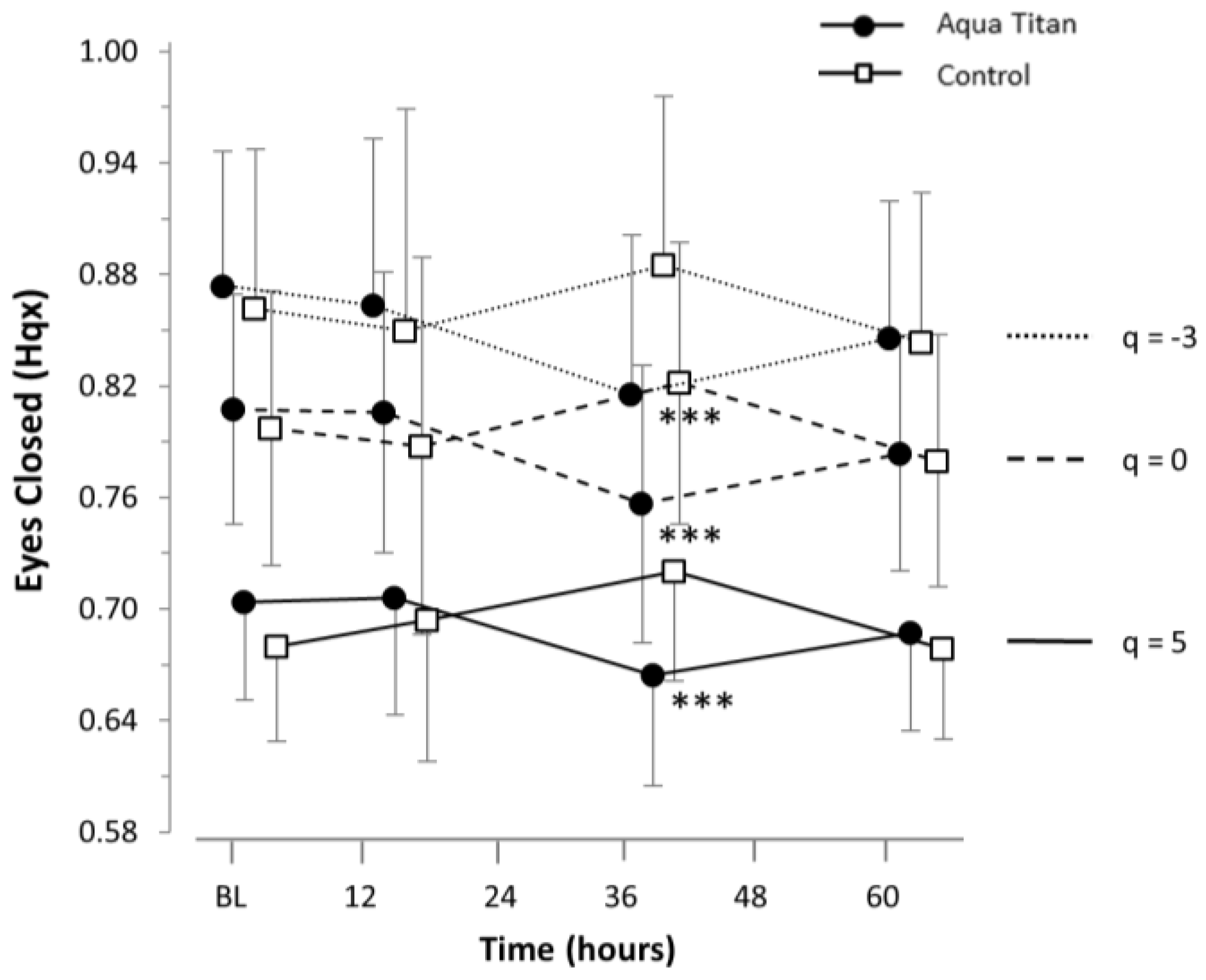
3.1. Effects of Aqua Titan-Treated Stockings on Balance
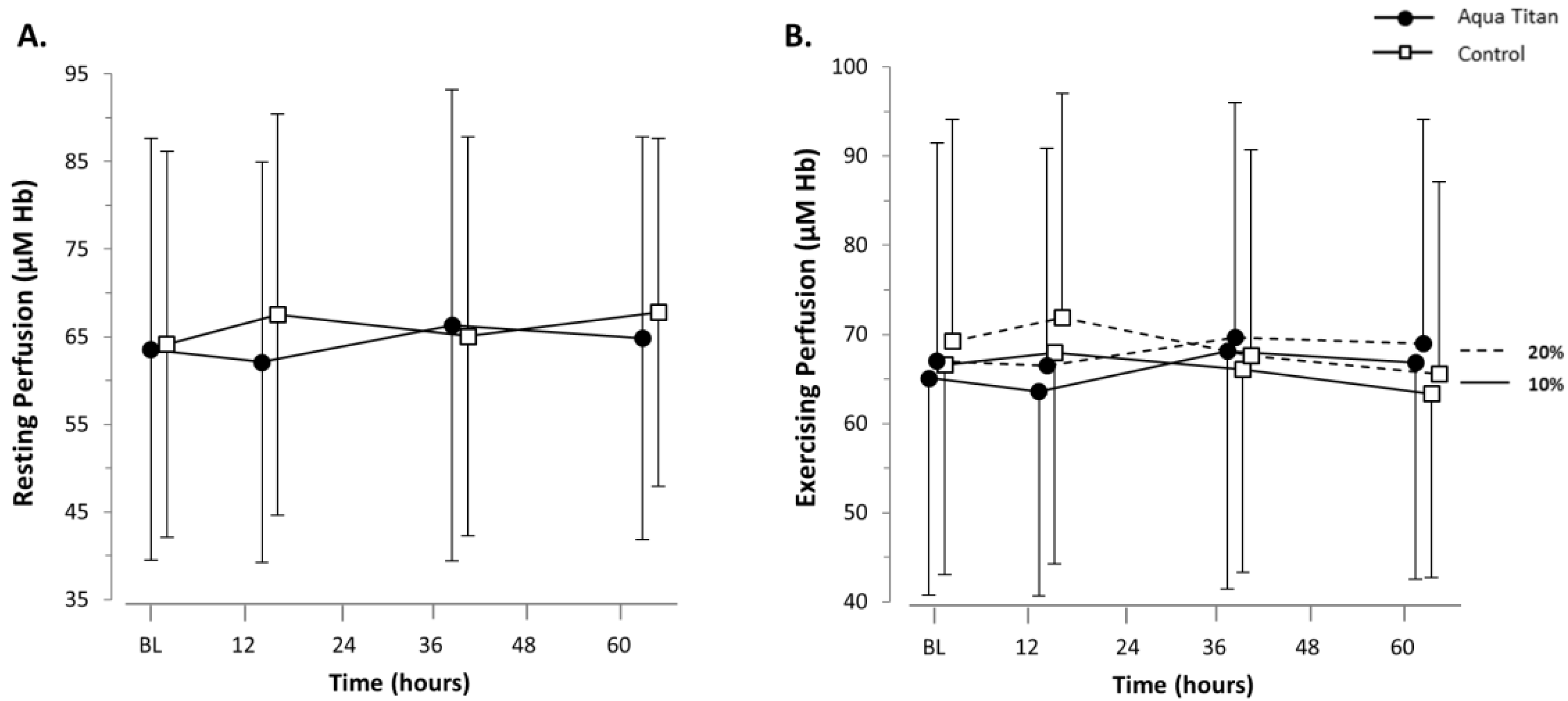
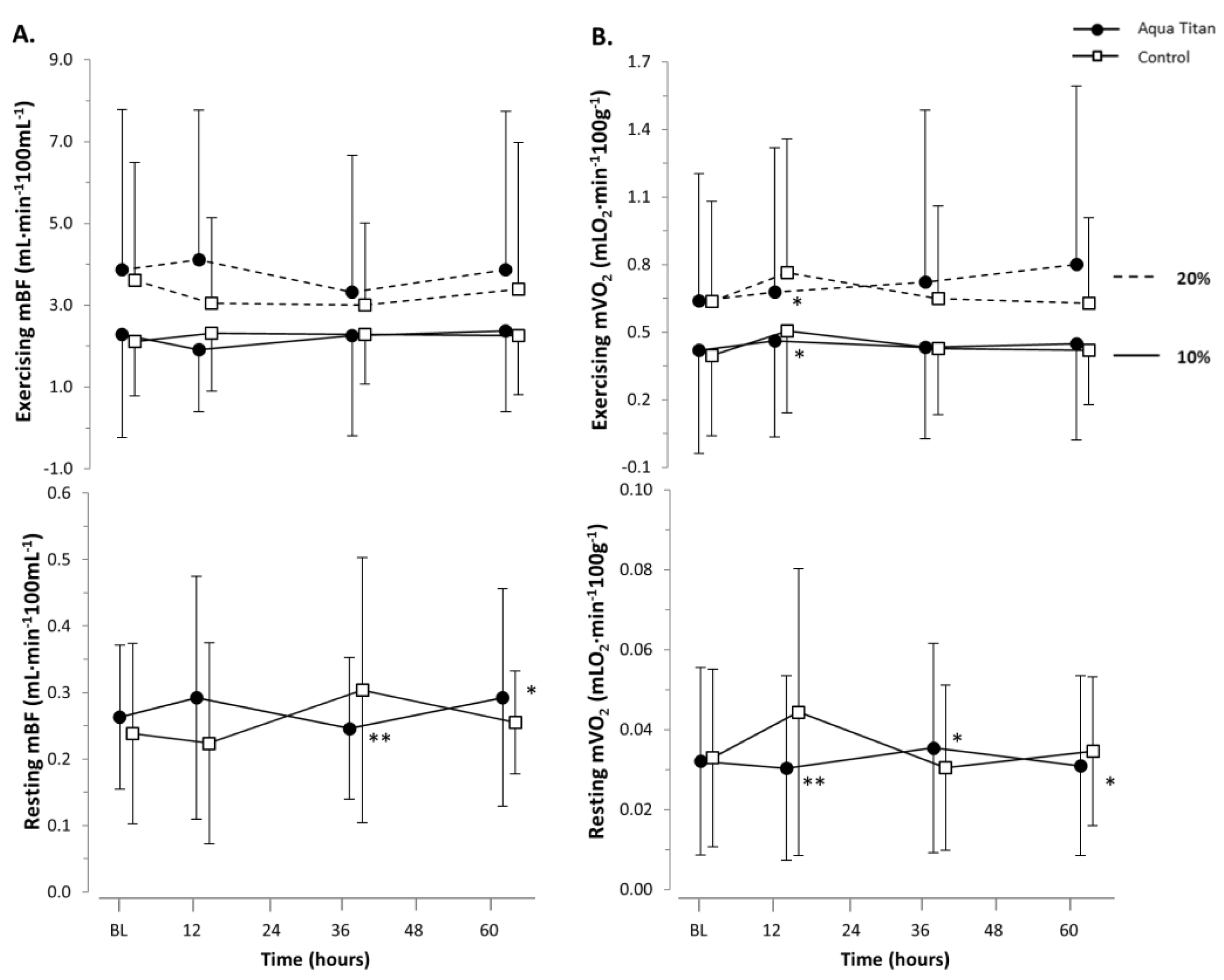
3.2. Effects of Aqua Titan-Treated Stockings on Muscle Microvascular Perfusion, Blood Flow and Oxygen Consumption
3.3. Effects of Aqua Titan-Treated Stockings on Ankle Range of Motion
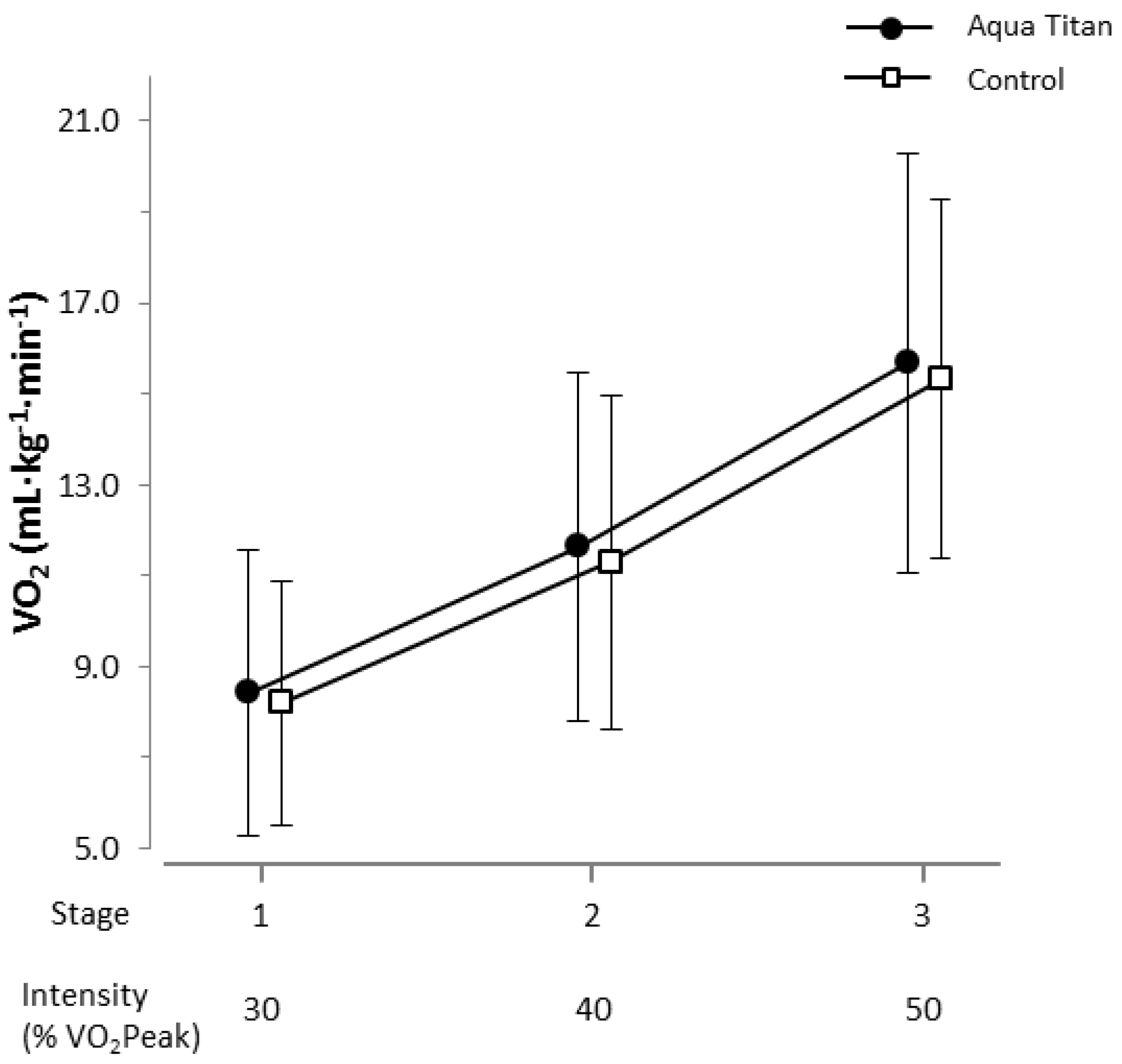
3.4. Effects of Aqua Titan-Treated Stockings on Submaximal Whole Body Oxygen Consumption and Maximal Walking Performance
4. Discussion
4.1. Aqua Titan-Treated Stockings Improved Balance, But Had No Effect on Walking Performance or Economy
4.2. Aqua Titan-Treated Stockings Had No Clear Effects on Muscle Microvascular Blood Flow, Perfusion or Oxygen Consumption
4.3. Aqua Titan-Treated Stockings Increased Ankle Joint Range of Motion
4.4. Considerations and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Near-Infrared Spectroscopy
Appendix A.2. Muscle Microvascular Perfusion
Appendix A.3. Muscle Microvascular Blood Flow
Appendix A.4. Muscle Oxygen Consumption

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Contrast a | Change (Hq) | Lower CI | Upper CI | p-Value | Likelihood (%) Decrease/Trivial/Increase | Qualitative b |
|---|---|---|---|---|---|---|
| Hq COPx (q = −3) | ||||||
| 14 h–BL AqT–Control | −0.0003 | −0.0527 | 0.0521 | 0.990 | 27.6/45.7/26.7 | Unclear |
| 38 h–BL AqT–Control | −0.0703 | −0.124 | −0.017 | 0.013 | 98.7/1.30/0.03 | Very likely decrease |
| 62 h–BL AqT–Control | 0.0040 | −0.0462 | 0.0543 | 0.865 | 21.1/46.5/32.3 | Unclear |
| Hq COPx (q = 0) | ||||||
| 14 h–BL AqT–Control | 0.0078 | −0.0331 | 0.0487 | 0.686 | 14.0/46.3/39.7 | Unclear |
| 38 h–BL AqT–Control | −0.0635 | −0.109 | −0.0184 | 0.009 | 99.2/0.82/0.02 | Very likely decrease |
| 62 h–BL AqT–Control | 0.0054 | −0.0417 | 0.0525 | 0.810 | 20.5/42.6/36.8 | Unclear |
| Hq COPx (q = 5) | ||||||
| 14 h–BL AqT–Control | −0.0097 | −0.0439 | 0.0245 | 0.548 | 51.6/36.7/11.7 | Unclear |
| 38 h–BL AqT–Control | −0.0456 | −0.0816 | −0.0093 | 0.017 | 98.5/1.5/0.06 | Very likely decrease |
| 62 h–BL AqT–Control | 0.0114 | −0.0271 | 0.0498 | 0.550 | 13.7/31.7/54.6 | Unclear |
| Contrast a | Change (°) | Lower CI | Upper CI | p-Value | Likelihood (%) Decrease/Trivial/Increase | Qualitative b |
|---|---|---|---|---|---|---|
| Dorsiflexion ROM (°) | ||||||
| 14 h–BL AqT–Control | 0.657 | −0.0607 | 1.38 | 0.070 | 0.00/81.6/14.4 | Likely trivial |
| 38 h–BL AqT–Control | 1.09 | −0.0783 | 1.03 | 0.065 | 0.01/44.6/55.4 | Possible increase |
| 62 h–BL AqT–Control | 1.24 | −0.226 | 2.70 | 0.091 | 0.08/37.2/62.8 | Possible increase |
| Plantar Flexion ROM (°) | ||||||
| 14 h–BL AqT–Control | 0.630 | −1.69 | 2.94 | 0.540 | 5.62/57.7/36.6 | Possibly trivial |
| 38 h–BL AqT–Control | 1.26 | 0.326 | 2.21 | 0.013 | 0.00/28.8/71.2 | Possible increase |
| 62 h–BL AqT–Control | 1.44 | 0.30 | 2.58 | 0.017 | 0.00/21.5/78.5 | Likely increase |
| Total ROM (°) | ||||||
| 14 h–BL AqT–Control | 0.823 | −0.833 | 2.48 | 0.302 | 0.46/70.8/28.8 | Possibly trivial |
| 38 h–BL AqT–Control | 2.37 | 0.614 | 4.13 | 0.012 | 0.00/10.0/90.0 | Likely increase |
| 62 h–BL AqT–Control | 2.70 | 0.974 | 4.42 | 0.005 | 0.00/4.54/95.5 | Very likely increase |
References
- Lord, S.R.; Sherrington, C.; Menz, H.B.; Close, J.C. Falls in Older People: Risk Factors and Strategies for Prevention; Cambridge University Press: Cambridge, UK, 2007. [Google Scholar]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35, ii37–ii41. [Google Scholar] [CrossRef] [PubMed]
- Lautenschlager, E.P.; Monaghan, P. Titanium and titanium alloys as dental materials. Int. Dent. J. 1993, 43, 245–253. [Google Scholar] [PubMed]
- Albrektsson, T.; Brånemark, P.-I.; Hansson, H.-A.; Lindström, J. Osseointegrated titanium implants: Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Buettner, K.M.; Valentine, A.M. Bioinorganic chemistry of titanium. Chem. Rev. 2011, 112, 1863–1881. [Google Scholar] [CrossRef] [PubMed]
- Hirata, Y.; Ueda, Y.; Takase, H.; Suzuki, K. High Functional Water Containing Titanium and Method and Apparatus for Producing the Same. U.S. Patent 7,144,589, 5 December 2006. [Google Scholar]
- Korte, M. Influence of aquatitan tape on nerve cells of the central nervous system. J. Clin. Biochem. Nutr. 2008, 43, 44–47. [Google Scholar]
- Aoi, W.; Takanami, Y.; Kawai, Y.; Otsuki, T.; Kawake, T.; Naito, Y.; Yoshikawa, T. Relaxant effect of microtitan via regulation of autonomic nerve activity in mice. Life Sci. 2009, 85, 408–411. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.D.; Fink, P.W.; Graham, D.F.; Rowlands, D.S. Effect of microtitanium impregnated tape on the recovery of triceps surae musculotendinous function following strenuous running. SpringerPlus 2013, 2, 653. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, D.S.; Graham, D.F.; Fink, P.W.; Wadsworth, D.P.; Hughes, J.D. Effect of whole-body microtitanium-treated garments on metabolic cost of exercise following strenuous hill running. J. Sci. Med. Sport 2014, 17, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Wadsworth, D.P.; Walmsley, A.; Rowlands, D.S. Aquatitan garments extend joint range of motion without effect on run performance. Med. Sci. Sports Exerc. 2010, 42, 2273–2281. [Google Scholar] [CrossRef] [PubMed]
- Northridge, D.B.; Grant, S.; Ford, I.; Christie, J.; McLenachan, J.; Connelly, D.; McMurray, J.; Ray, S.; Henderson, E.; Dargie, H. Novel exercise protocol suitable for use on a treadmill or a bicycle ergometer. Heart 1990, 64, 313–316. [Google Scholar] [CrossRef]
- Ihlen, E.A.F.E. Introduction to multifractal detrended fluctuation analysis in matlab. Front. Physiol. 2012, 3, 141. [Google Scholar] [CrossRef] [PubMed]
- Okin, P.M.; Ameisen, O.; Kligfield, P. A modified treadmill exercise protocol for computer-assisted analysis of the st segment/heart rate slope: Methods and reproducibility. J. Electrocardiol. 1986, 19, 311–318. [Google Scholar] [CrossRef]
- Kenward, M.G.; Roger, J.H. The use of baseline covariates in crossover studies. Biostatistics 2010, 11, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Gaffney, K.A.; Lucero, A.; Stoner, L.; Faulkner, J.; Whitfield, P.; Krebs, J.; Rowlands, D.S. Nil whey protein effect on glycemic control after intense mixed-mode training in type 2 diabetes. Med. Sci. Sports Exerc. 2018, 50, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G.; Batterham, A.M. Error rates, decisive outcomes and publication bias with several inferential methods. Sports Med. 2016, 46, 1563–1573. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.; Marshall, S.; Batterham, A.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3. [Google Scholar] [CrossRef] [PubMed]
- Dorfman, L.J.; Bosley, T.M. Age-related changes in peripheral and central nerve conduction in man. Neurology 1979, 29, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Mendonca, G.V.; Pezarat-Correia, P.; Vaz, J.R.; Silva, L.; Heffernan, K.S. Impact of aging on endurance and neuromuscular physical performance: The role of vascular senescence. Sports Med. 2017, 47, 583–598. [Google Scholar] [CrossRef] [PubMed]
- Skinner, H.B.; Barrack, R.L.; Cook, S.D. Age-related decline in proprioception. Clin. Orthop. Relat. Res. 1984, 208–211. [Google Scholar] [CrossRef]
- Woollacott, M.H.; Shumway-Cook, A.; Nashner, L.M. Aging and posture control: Changes in sensory organization and muscular coordination. Int. J. Aging Hum. Dev. 1986, 23, 97–114. [Google Scholar] [CrossRef] [PubMed]
- Hultborn, H.; Meunier, S.; Pierrot-Deseilligny, E.; Shindo, M. Changes in presynaptic inhibition of Ia fibres at the onset of voluntary contraction in man. J. Physiol. 1987, 389, 757–772. [Google Scholar] [CrossRef] [PubMed]
- Katz, B. Depolarization of sensory terminals and the initiation of impulses in the muscle spindle. J. Physiol. 1950, 111, 261–282. [Google Scholar] [CrossRef] [PubMed]
- Milne, J.; Williamson, J. The ankle jerk in older people. Gerontol. Clin. 1972, 14, 86–88. [Google Scholar] [CrossRef]
- Levy, W.B.; Baxter, R.A. Energy efficient neural codes. Neural Comput. 1996, 8, 531–543. [Google Scholar] [CrossRef] [PubMed]
- Niven, J.E.; Laughlin, S.B. Energy limitation as a selective pressure on the evolution of sensory systems. J. Exp. Biol. 2008, 211, 1792–1804. [Google Scholar] [CrossRef] [PubMed]
- Pyne, D.B. Exercise-induced muscle damage and inflammation: A review. Aust. J. Sci. Med. Sport 1994, 26, 49–58. [Google Scholar] [PubMed]
- Rowlands, D.S.; Shultz, S.P.; Ogawa, T.; Aoi, W.; Korte, M. The effects of uniquely-processed titanium on biological systems: Implications for human health and performance. J. Funct. Biomater. 2014, 5, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Hutton, R. Neuromuscular basis of stretching exercises. In Strength and Power in Sport; Komi, P.V., Ed.; Blackwell Scientific Oxford: Oxford, UK, 1992; pp. 29–38. [Google Scholar]
- Taylor, D.C.; Dalton, J.D., Jr.; Seaber, A.V.; Garrett, W.E., Jr. Viscoelastic properties of muscle-tendon units: The biomechanical effects of stretching. Am. J. Sports Med. 1990, 18, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Weppler, C.H.; Magnusson, S.P. Increasing muscle extensibility: A matter of increasing length or modifying sensation? Phys. Ther. 2010, 90, 438–449. [Google Scholar] [CrossRef] [PubMed]
- Sandkühler, J. Learning and memory in pain pathways. Pain 2000, 88, 113–118. [Google Scholar] [CrossRef]
- Fantini, S.; Franceschinifantini, M.; Maier, J.; Walker, S.; Barbieri, B.; Gratton, E. Frequency-domain multichannel optical-detector for noninvasive tissue spectroscopy and oximetry. Opt. Eng. 1995, 34, 32–43. [Google Scholar] [CrossRef]
- Paunescu, L.A.; Casavola, C.; Franceschini, M.A.; Fantini, S.; Winter, L.; Kim, J.; Wood, D.; Gratton, E. Calf muscle blood flow and oxygen consumption measured with near-infrared spectroscopy during venous occlusion. In Proceedings of the Optical Tomography and Spectroscopy of Tissue III, San Jose, CA, USA, 23–29 January 1999. [Google Scholar] [CrossRef]
- Cross, T.J.; Sabapathy, S. The impact of venous occlusion per se on forearm muscle blood flow: Implications for the near-infrared spectroscopy venous occlusion technique. Clin. Physiol. Funct. Imaging 2017, 37, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Ryan, T.E.; Erickson, M.L.; Brizendine, J.T.; Young, H.-J.; McCully, K.K. Noninvasive evaluation of skeletal muscle mitochondrial capacity with near-infrared spectroscopy: Correcting for blood volume changes. J. Appl. Physiol. 2012, 113, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Van Beekvelt, M.C.; Colier, W.N.; Wevers, R.A.; Van Engelen, B.G. Performance of near-infrared spectroscopy in measuring local O2 consumption and blood flow in skeletal muscle. J. Appl. Physiol. 2001, 90, 511–519. [Google Scholar] [CrossRef] [PubMed]






| Characteristic | n = 16 |
|---|---|
| Age (year) | 67.9 ± 4.2 |
| Gender (male, female) | 8, 8 |
| Height (m) | 1.68 ± 0.11 |
| Weight (kg) | 70.1 ± 12.8 |
| Body mass index (kg/m2) | 24.8 ± 3.1 |
| Adipose tissue thickness at NIRS site (mm) | 4.7 ± 1.7 |
| Peak oxygen uptake (mL·kg−1·min−1) | 35.0 ± 10.4 |
| All values are the mean ± SD |
| Contrast a | Change | Lower CI | Upper CI | p-Value | Likelihood (%) Decrease/Trivial/Increase | Qualitative b |
|---|---|---|---|---|---|---|
| µM Hb | Resting Perfusion (µM Hb) | |||||
| 14 h–BL AqT–Control | −3.11 | −7.44 | 1.22 | 0.141 | 28.6/71.4/0.03 | Possibly trivial |
| 38 h–BL AqT–Control | 1.70 | −2.06 | 5.47 | 0.337 | 0.08/91.2/8.75 | Likely trivial |
| 62 h–BL AqT–Control | 0.722 | −1.66 | 3.10 | 0.515 | 0.01/99.5/0.51 | Very likely trivial |
| 10% Exercise Perfusion (µM Hb) | ||||||
| 14 h–BL AqT–Control | −2.02 | −6.93 | 2.89 | 0.377 | 14.5/85.2/0.30 | Likely trivial |
| 38 h–BL AqT–Control | 3.54 | 0.140 | 6.94 | 0.042 | 0.00/71.7/28.3 | Possibly trivial |
| 62 h–BL AqT–Control | 3.07 | −3.14 | 9.28 | 0.158 | 0.02/63.3/36.7 | Possibly trivial |
| 20% Exercise Perfusion (µM Hb) | ||||||
| 14 h–BL AqT–Control | −1.83 | −8.87 | 5.21 | 0.578 | 18.7/79.0/2.36 | Likely trivial |
| 38 h–BL AqT–Control | 3.05 | −0.668 | 6.77 | 0.097 | 0.00/81.0/19.0 | Likely trivial |
| 62 h–BL AqT–Control | 3.88 | −1.57 | 9.33 | 0.137 | 0.05/62.8/37.1 | Possibly trivial |
| Contrast a | Change | Lower CI | Upper CI | p-Value | Likelihood (%) Decrease/Trivial/Increase | Qualitative b |
|---|---|---|---|---|---|---|
| mBF (mL·min−1·100 mL−1) | Resting mBF (mL·min−1·100 mL−1) | |||||
| 14 h–BL AqT–Control | 0.0715 | −0.0918 | 0.235 | 0.368 | 10.0/18.5/71.5 | Unclear |
| 38 h–BL AqT–Control | −0.0629 | −0.171 | 0.0455 | 0.225 | 76.6/20.1/3.3 | Likely decrease |
| 62 h–BL AqT–Control | 0.0413 | −0.0372 | 0.120 | 0.269 | 2.75/32.1/65.2 | Possible increase |
| 10% Exercise mBF (mL·min−1·100 mL−1) | ||||||
| 14 h–BL AqT–Control | −0.141 | −0.536 | 0.253 | 0.436 | 35.0/62.5/2.5 | Possibly trivial |
| 38 h–BL AqT–Control | −0.154 | −0.839 | 0.531 | 0.628 | 42.6/45.4/12.0 | Unclear |
| 62 h–BL AqT–Control | 0.174 | −0.529 | 0.876 | 0.593 | 11.3/43.5/45.2 | Unclear |
| 20% Exercise mBF (mL·min−1·100 mL−1) | ||||||
| 14 h–BL AqT–Control | 0.752 | −1.24 | 2.75 | 0.407 | 6.52/34.9/58.6 | Unclear |
| 38 h–BL AqT–Control | 0.104 | −0.736 | 0.944 | 0.788 | 4.54/83.3/12.2 | Likely trivial |
| 62 h–BL AqT–Control | 0.443 | −0.703 | 1.59 | 0.409 | 2.81/56.5/40.7 | Possibly trivial |
| mVO2 (mLO2·min−1·100g−1) | Resting mVO2 (mLO2·min−1·100 g−1) | |||||
| 14 h–BL AqT–Control | −0.0155 | −0.0382 | 0.0072 | 0.154 | 86.6/11.1/2.24 | Likely decrease |
| 38 h–BL AqT–Control | 0.0052 | −0.0030 | 0.0134 | 0.188 | 0.55/42.2/57.3 | Possible increase |
| 62 h–BL AqT–Control | −0.0051 | −0.0135 | 0.0034 | 0.212 | 55.8/43.5/0.74 | Possible decrease |
| 10% Exercise mVO2 (mLO2·min−1·100 g−1) | ||||||
| 14 h–BL AqT–Control | −0.0852 | −0.238 | 0.0677 | 0.236 | 60.5/38.1/1.33 | Possible decrease |
| 38 h–BL AqT–Control | −0.0033 | −0.104 | 0.0970 | 0.943 | 8.89/84.3/6.84 | Unclear |
| 62 h–BL AqT–Control | 0.0310 | −0.149 | 0.211 | 0.707 | 11.6/55.5/32.9 | Unclear |
| 20% Exercise mVO2 (mLO2·min−1·100 g−1) | ||||||
| 14 h–BL AqT–Control | −0.0973 | −0.291 | 0.0960 | 0.284 | 54.6/43.6/1.77 | Possible decrease |
| 38 h–BL AqT–Control | 0.0508 | −0.215 | 0.317 | 0.680 | 12.7/49.3/38.1 | Unclear |
| 62 h–BL AqT–Control | 0.144 | −0.229 | 0.516 | 0.411 | 8.5/28.4/63.0 | Unclear |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Black, M.J.; Lucero, A.A.; Fink, P.W.; Stoner, L.; Shultz, S.P.; Lark, S.D.; Rowlands, D.S. The Effects of Uniquely-Processed Titanium on Balance and Walking Performance in Healthy Older Adults. J. Funct. Biomater. 2018, 9, 39. https://doi.org/10.3390/jfb9020039
Black MJ, Lucero AA, Fink PW, Stoner L, Shultz SP, Lark SD, Rowlands DS. The Effects of Uniquely-Processed Titanium on Balance and Walking Performance in Healthy Older Adults. Journal of Functional Biomaterials. 2018; 9(2):39. https://doi.org/10.3390/jfb9020039
Chicago/Turabian StyleBlack, Melissa J., Adam A. Lucero, Philip W. Fink, Lee Stoner, Sarah P. Shultz, Sally D. Lark, and David S. Rowlands. 2018. "The Effects of Uniquely-Processed Titanium on Balance and Walking Performance in Healthy Older Adults" Journal of Functional Biomaterials 9, no. 2: 39. https://doi.org/10.3390/jfb9020039
APA StyleBlack, M. J., Lucero, A. A., Fink, P. W., Stoner, L., Shultz, S. P., Lark, S. D., & Rowlands, D. S. (2018). The Effects of Uniquely-Processed Titanium on Balance and Walking Performance in Healthy Older Adults. Journal of Functional Biomaterials, 9(2), 39. https://doi.org/10.3390/jfb9020039