
Pharmacodynamics of Ceftibuten: An Assessment of an Oral Cephalosporin against Enterobacterales in a Neutropenic Murine Thigh Model


Abstract
:1. Introduction
2. Results
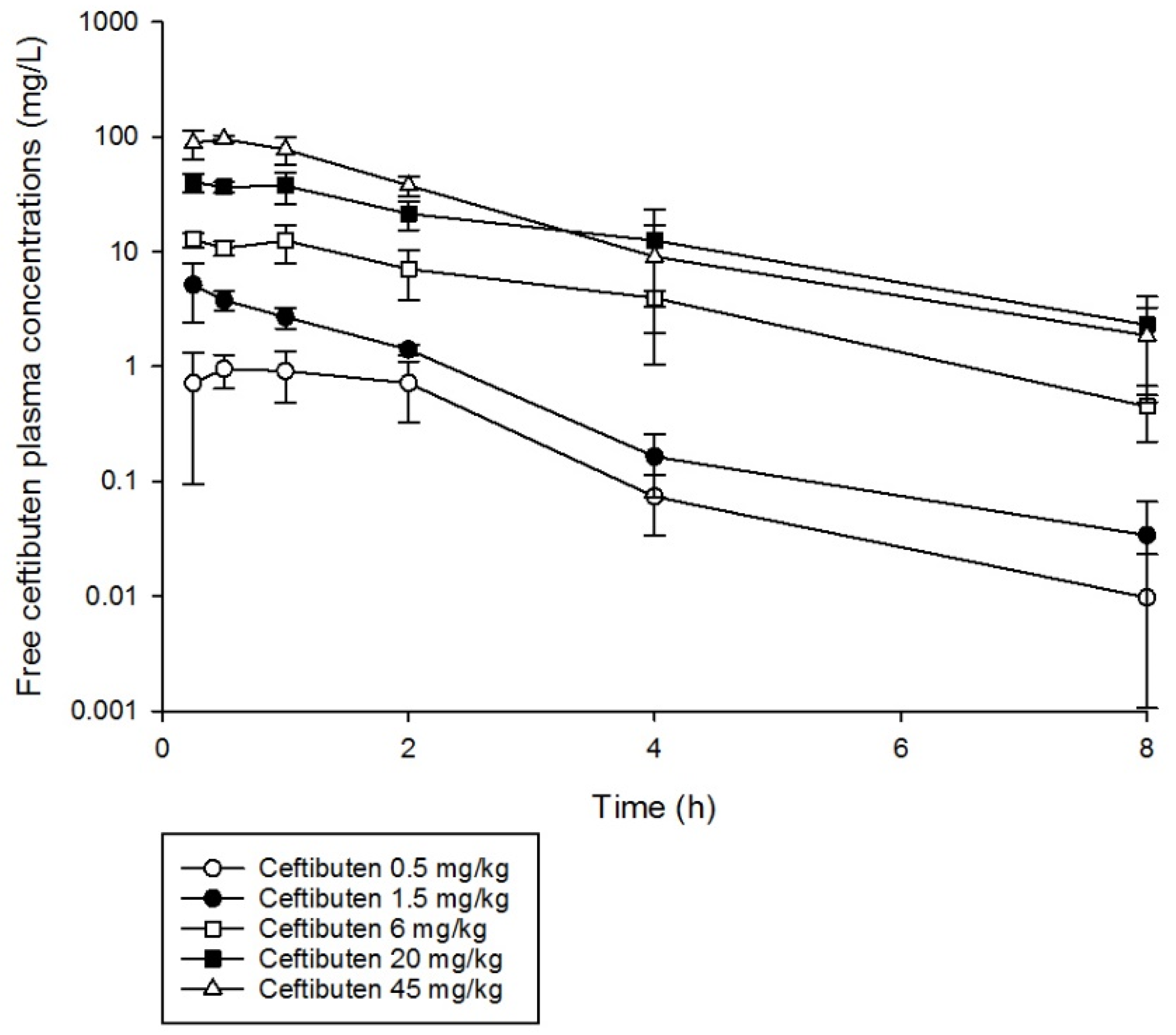
2.1. Murine Pharmacokinetic Studies
2.2. Pharmacodynamic Studies
3. Discussion
4. Materials and Methods
4.1. Antimicrobial Test Agents
4.2. Isolates
4.3. Animals
4.4. Neutropenic Thigh Infection Model
4.5. Murine Pharmacokinetic Studies
4.6. Pharmacodynamic Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bush, K.; Bradford, P.A. Epidemiology of β-Lactamase-Producing Pathogens. Clin. Microbiol. Rev. 2020, 33. [Google Scholar] [CrossRef] [PubMed]
- Guh, A.Y.; Bulens, S.N.; Mu, Y.; Jacob, J.T.; Reno, J.; Scott, J.; Wilson, L.E.; Vaeth, E.; Lynfield, R.; Shaw, K.M.; et al. Epidemiology of Carbapenem-Resistant Enterobacteriaceae in 7 US Communities, 2012–2013. JAMA 2015, 314, 1479–1487. [Google Scholar] [CrossRef] [PubMed]
- McDanel, J.; Schweizer, M.; Crabb, V.; Nelson, R.; Samore, M.; Khader, K.; Blevins, A.E.; Diekema, D.; Chiang, H.-Y.; Nair, R.; et al. Incidence of Extended-Spectrum β-Lactamase (ESBL)-Producing Escherichia coli and Klebsiella Infections in the United States: A Systematic Literature Review. Infect. Control Hosp. Epidemiol. 2017, 38, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Meije, Y.; Pigrau, C.; Fernández-Hidalgo, N.; Clemente, M.; Ortega, L.; Sanz, X.; Loureiro-Amigo, J.; Sierra, M.; Ayestarán, A.; Morales-Cartagena, A.; et al. Non-intravenous carbapenem-sparing antibiotics for definitive treatment of bacteraemia due to Enterobacteriaceae producing extended-spectrum β-lactamase (ESBL) or AmpC β-lactamase: A propensity score study. Int. J. Antimicrob. Agents 2019, 54, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Harrington, S.; Dihmess, A.; Woo, B.; Masoud, R.; Martis, P. Clinical epidemiology of carbapenem-intermediate or -resistant Enterobacteriaceae. J. Antimicrob. Chemother. 2011, 66, 1600–1608. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Kotapati, S.; Kuti, J.L.; Nightingale, C.H.; Nicolau, D.P. Impact of extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella species on clinical outcomes and hospital costs: A matched cohort study. Infect. Control Hosp. Epidemiol. 2006, 27, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Papp-Wallace, K.M. The latest advances in β-lactam/β-lactamase inhibitor combinations for the treatment of Gram-negative bacterial infections. Expert Opin. Pharmacother. 2019, 20, 2169–2184. [Google Scholar] [CrossRef] [PubMed]
- Owens, R.C., Jr.; Nightingale, C.H.; Nicolau, D.P. Ceftibuten: An overview. Pharmacotherapy 1997, 17, 707–720. [Google Scholar] [PubMed]
- Stewart, A.G.; Harris, P.N.A.; Henderson, A.; Schembri, M.A.; Paterson, D.L. Oral cephalosporin and β-lactamase inhibitor combinations for ESBL-producing Enterobacteriaceae urinary tract infections. J. Antimicrob. Chemother. 2020, 75, 2384–2393. [Google Scholar] [CrossRef] [PubMed]
- European Society of Clincial Microbiology and Infectious Diseases. Why Do EUCAST Have No Systemic Breakpoints for Enterobacterales with Oral Cephalosporins? Version 2. EUCAST. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Guidance_documents/Oral_ceph_breakpoints_v2_20200710.pdf (accessed on 20 December 2020).
- Auckenthaler, R. Pharmacokinetics and pharmacodynamics of oral beta-lactam antibiotics as a two-dimensional approach to their efficacy. J. Antimicrob. Chemother. 2002, 50 (Suppl. 1), 13–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuti, J.L. Optimizing antimicrobial pharmacodynamics: A guide for your stewardship program. Rev. Med. Clin. Condes 2016, 27, 615–624. [Google Scholar] [CrossRef] [Green Version]
- Abdelraouf, K.; Stainton, S.M.; Nicolau, D.P. In Vivo Pharmacodynamic Profile of Ceftibuten-Clavulanate Combination against Extended-Spectrum-β-Lactamase-Producing Enterobacteriaceae in the Murine Thigh Infection Model. Antimicrob. Agents Chemother. 2019, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lomovskaya, O.; Tsivkovski, R.; Nelson, K.; Rubio-Aparicio, D.; Sun, D.; Totrov, M.; Dudley, M.N. Spectrum of Beta-Lactamase Inhibition by the Cyclic Boronate QPX7728, an Ultrabroad-Spectrum Beta-Lactamase Inhibitor of Serine and Metallo-Beta-Lactamases: Enhancement of Activity of Multiple Antibiotics against Isogenic Strains Expressing Single Beta-Lactamases. Antimicrob. Agents Chemother. 2020, 64. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.; Lim, J.; Radwanski, E.; Marco, A.; Affrime, M. Pharmacokinetics and dose proportionality of ceftibuten in men. Antimicrob. Agents Chemother. 1995, 39, 359–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Target Product Profiles for Oral Therapy of Urinary Tract Infections; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Grayson, M.L.; Crowe, S.M.; McCarthy, J.S.; Mills, J.; Mouton, J.W.; Norrby, S.R.; Paterson, D.; Pfaller, M.A. Kucers’ the Use of Antibiotics Sixth Edition: A Clinical Review of Antibacterial, Antifungal and Antiviral Drugs; CRC Press: Boca Raton, FL, USA, 2010. [Google Scholar]
- Jernigan, J.A.; Hatfield, K.M.; Wolford, H.; Nelson, R.E.; Olubajo, B.; Reddy, S.C.; McCarthy, N.; Paul, P.; McDonald, L.C.; Kallen, A.; et al. Multidrug-Resistant Bacterial Infections in U.S. Hospitalized Patients, 2012–2017. N. Engl. J. Med. 2020, 382, 1309–1319. [Google Scholar] [CrossRef] [PubMed]
- Andes, D.; Craig, W.A. Treatment of infections with ESBL-producing organisms: Pharmacokinetic and pharmacodynamic considerations. Clin. Microbiol. Infect. 2005, 11, 10–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolau, D.P.; Onyeji, C.O.; Zhong, M.; Tessier, P.R.; Banevicius, M.A.; Nightingale, C.H. Pharmacodynamic assessment of cefprozil against Streptococcus pneumoniae: Implications for breakpoint determinations. Antimicrob. Agents Chemother. 2000, 44, 1291–1295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avery, L.M.; Abdelraouf, K.A.; Nicolau, D.P. Assesment of the In Vivo Pharmacodynamic Profile of Ceftibuten/VNRX-7145 Combination against Serine-Beta-Lactamase-Producing Enterobacteriaceae in the Neutropeneic Murine Thigh Infection Model. Presented at ASM Microbe, San Fransisco, CA, USA, 20–24 June 2019. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Single Dose Regimen | λ1/2 (h) | fCmax | fAUC0–8 | R2 |
|---|---|---|---|---|
| 0.5 mg/kg | 1.0 | 1.0 | 2.3 | 0.90 |
| 1.5 mg/kg | 1.2 | 5.1 | 6.8 | 0.92 |
| 6 mg/kg | 1.5 | 12.8 | 37.0 | 0.98 |
| 20 mg/kg | 1.8 | 40.4 | 119.3 | 0.99 |
| 45 mg/kg | 1.4 | 95.6 | 191.0 | 0.97 |
| Dosing Regimen | %fT > MIC (mg/L) | fAUC0–24 | Cmax | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0.03 | 0.06 | 0.125 | 0.25 | 0.5 | 1 | 2 | 4 | |||
| CTB 300 mg q8 h (human) [15] | 100% | 100% | 100% | 100% | 100% | 91% | 59% | 0% | 56.2 | 3.75 |
| CTB 300 mg q8 h HSR (murine) | 100% | 100% | 100% | 100% | 100% | 91% | 50% | 0% | 50.1 | 3.6 |
| 0.5 mg/kg single dose | 24% | 22% | 17% | 12% | 7% | 0% | 0% | 0% | 2.1 | 0.97 |
| 3 mg/kg single dose | 37% | 35% | 30% | 25% | 20% | 15% | 10% | 4% | 12.8 | 5.8 |
| 0.5 mg/kg q8 h | 71% | 66% | 51% | 36% | 21% | 0% | 0% | 0% | 6.4 | 0.98 |
| 1 mg/kg q6 h | 100% | 100% | 90% | 70% | 48% | 28% | 1% | 0% | 16.89 | 2.02 |
| 6 mg/kg q8 h | 100% | 100% | 100% | 91% | 76% | 61% | 45% | 30% | 76.4 | 11.8 |
| 20 mg/kg q6 h | 100% | 100% | 100% | 100% | 100% | 100% | 96% | 76% | 337.8 | 40.3 |
| 20 mg/kg q4 h | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 500.7 | 43.8 |
| 45 mg/kg q3 h | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 1487.6 | 108.7 |
| Isolate (MIC (mg/L)) | Ceftibuten %fT > MIC Required to Achieve | R2 | |
|---|---|---|---|
| Stasis | 1-log Reduction | ||
| KP 956 (0.03) | 46 | 68 | 0.90 |
| EC 756 (0.125) | 17 | 35 | 0.72 |
| KP 957 (0.125) | NA | NA | 0.74 |
| EC 551 (0.25) | 35 | NA | 0.85 |
| KP 958 (0.25) | 40 | 59 | 0.92 |
| EC 25922 (0.5) | 26 | 56 | 0.78 |
| EC 761 (1) | 17 | 31 | 0.9 |
| KP 700603 (1) | 44 | NA | 0.89 |
| EC 643 (4) | 11 | 69 | 0.39 |
| Median 1 | 31 | 58 | - |
| IQR 1 | 17–41 | 40–66 | 0.74–0.9 |
| Organism | CAIRD ID | Strain | Known Resistance Mechanism(s) | Ceftibuten MIC (mg/L) |
|---|---|---|---|---|
| Klebsiella pneumoniae | 956 | ARLG 1112 | SHV | 0.03 |
| Escherichia coli | 756 | ARLG 1023 | None | 0.12 |
| Klebsiella pneumoniae | 957 | ARLG 1118 | None | 0.12 |
| Escherichia coli | 551 | CDC 0077 | None | 0.25 |
| Klebsiella pneumoniae | 958 | ARLG 1120 | None | 0.25 |
| Escherichia coli | 25922 | ATCC 25922 | None | 0.5 |
| Escherichia coli | 761 | ARLG 1050 | None | 1 |
| Klebsiella pneumoniae | 700603 * | ATCC 700603 | SHV-18, OXA-2, OKP-B-6 | 1 |
| Escherichia coli | 643 * | SI-LP377 | CTX-M2 | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lasko, M.J.; Asempa, T.E.; Nicolau, D.P. Pharmacodynamics of Ceftibuten: An Assessment of an Oral Cephalosporin against Enterobacterales in a Neutropenic Murine Thigh Model. Antibiotics 2021, 10, 201. https://doi.org/10.3390/antibiotics10020201
Lasko MJ, Asempa TE, Nicolau DP. Pharmacodynamics of Ceftibuten: An Assessment of an Oral Cephalosporin against Enterobacterales in a Neutropenic Murine Thigh Model. Antibiotics. 2021; 10(2):201. https://doi.org/10.3390/antibiotics10020201
Chicago/Turabian StyleLasko, Maxwell J., Tomefa E. Asempa, and David P. Nicolau. 2021. "Pharmacodynamics of Ceftibuten: An Assessment of an Oral Cephalosporin against Enterobacterales in a Neutropenic Murine Thigh Model" Antibiotics 10, no. 2: 201. https://doi.org/10.3390/antibiotics10020201