
Ceftazidime/Avibactam and Meropenem/Vaborbactam for the Management of Enterobacterales Infections: A Narrative Review, Clinical Considerations, and Expert Opinion

 , , , , , , ,
, , , , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Chemical Structure, Pharmacological Properties, and Resistance Mechanisms
2.1. Ceftazidime–Avibactam
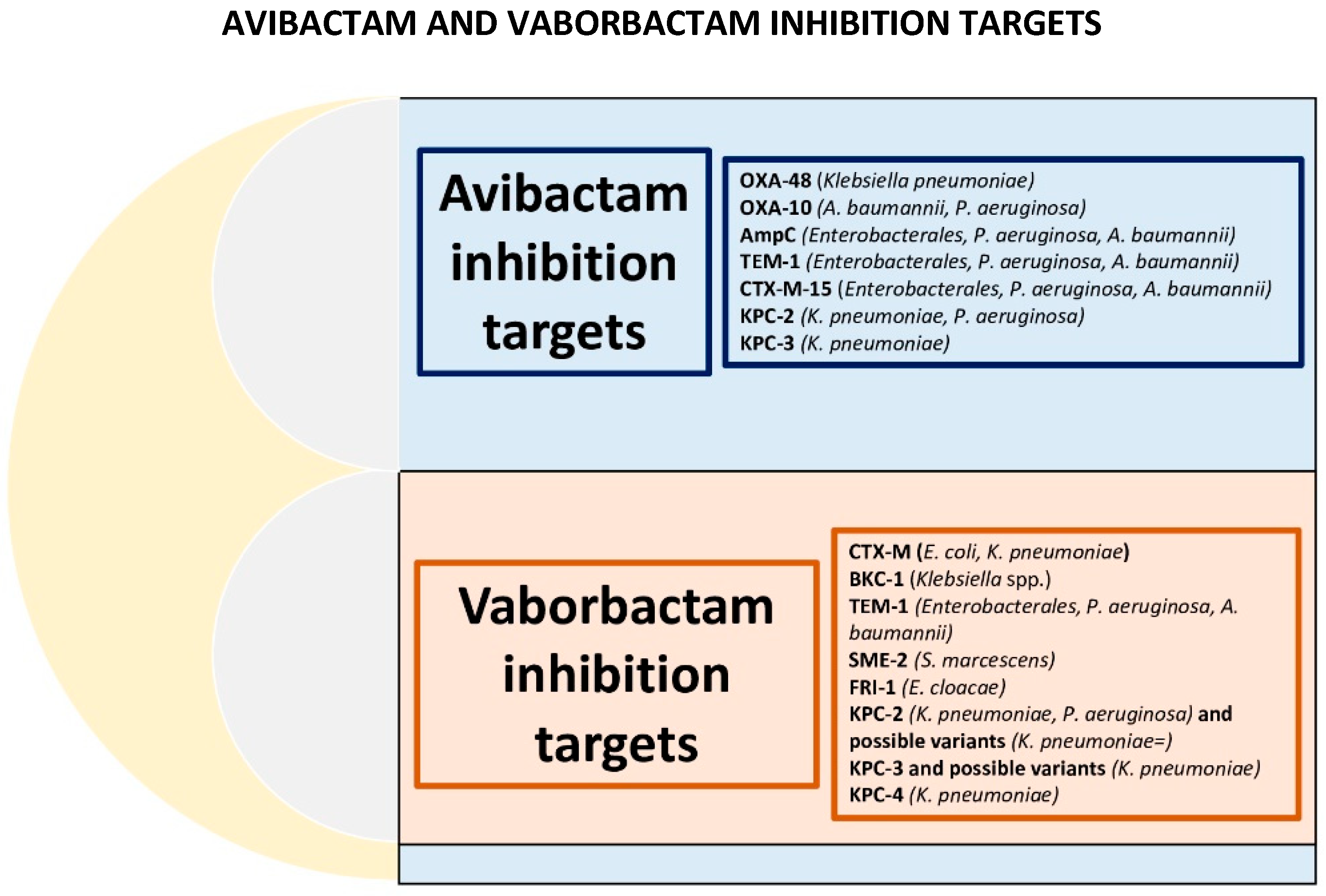
2.1.1. Chemical Structures and Activity Spectrum
2.1.2. Pharmacological Properties
2.1.3. Resistance Mechanisms
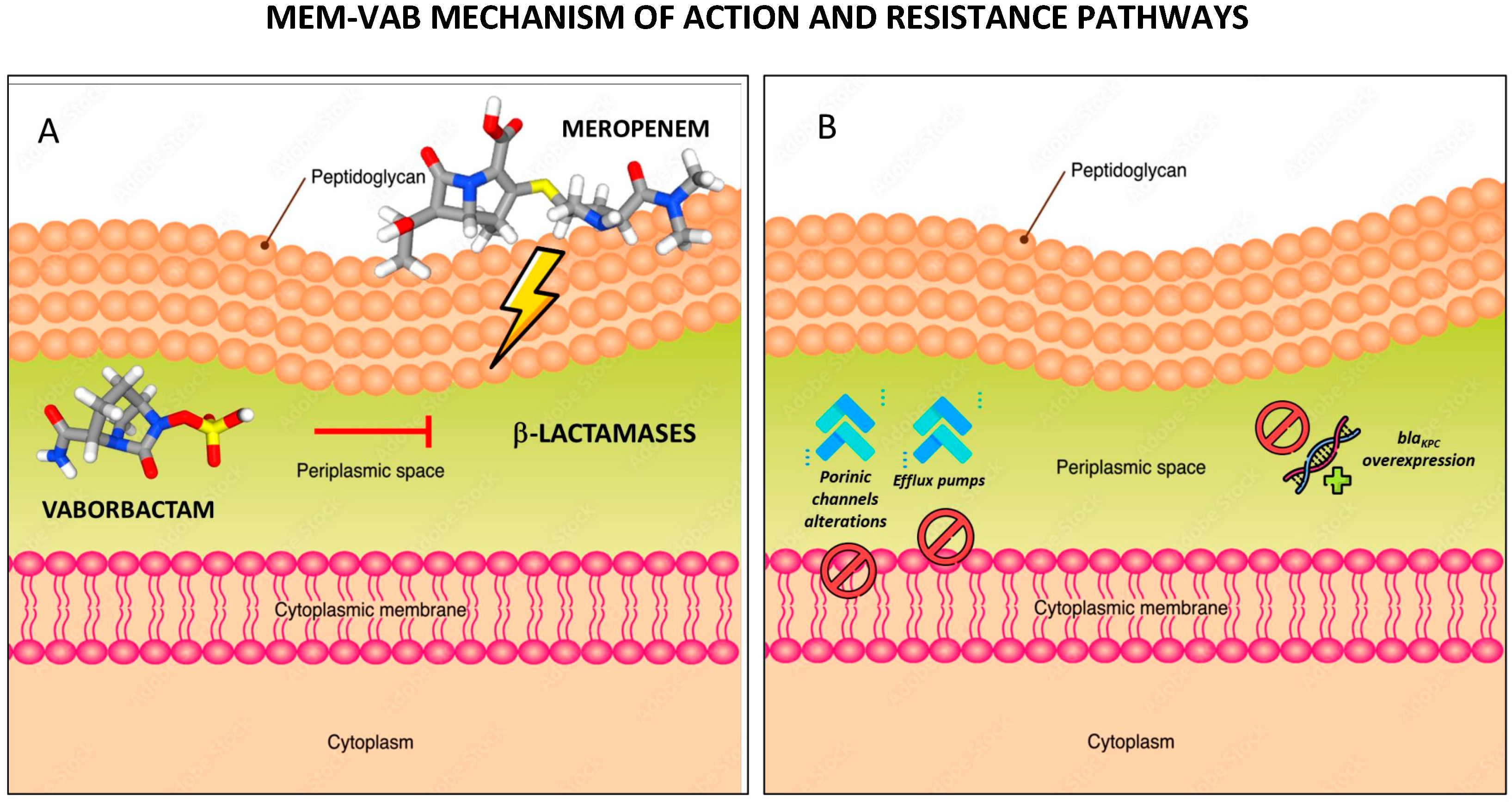
2.2. Meropenem–Vaborbactam
2.2.1. Chemical Structures and Activity Spectrum
2.2.2. Pharmacological Properties
2.2.3. Resistance Mechanisms
3. Susceptibility Testing
4. Clinical Data and Considerations
4.1. CAZ-AVI
4.2. MEM-VAB
4.3. CAZ-AVI vs. MEM-VAB
5. Expert Opinions
5.1. The Microbiological Point of View
5.2. The Clinical Point of View
6. Key Messages
- I.
- The optimal treatment for KPC-producing Enterobacterales infections is not well defined due to a lack of well-conducted RCTs, making treatment decisions primarily reliant on clinical experience.
- II.
- CAZ-AVI has demonstrated effectiveness in treating severe infections caused by KPC- or OXA-48-like-producing Enterobacterales, with high clinical success rates.
- III.
- CAZ-AVI’s efficacy varies by infection type: pneumonia and mechanical ventilation may increase the risk of treatment failure due to penetration issues. Optimal dosing for pneumonia patients, especially those on ventilation, requires further studies.
- IV.
- Concerns exist regarding CAZ-AVI’s effectiveness against KPC enzyme subtypes and KPC overexpression. Resistance to CAZ-AVI may develop after prolonged drug exposure, posing a challenge in the treatment of recurrent infections.
- V.
- MEM-VAB shows promise in treating CRE infections thanks to its microbiological potency and PK characteristics.
- VI.
- MEM-VAB is highly effective against KPC-producing strains, being active even against KPC subtypes. It has no effect against OXA-48 producing isolates.
- VII.
- Resistance development appears less common with MEM-VAB compared to CAZ-AVI, but further research is needed to understand long-term resistance patterns.
- VIII.
- There is no clear evidence of one drug being superior to the other in treating Enterobacterales infections. The choice should be tailored to the specific clinical scenario and local epidemiology.
- IX.
- Microbiology laboratories play a crucial role in supporting treatment decisions by providing susceptibility profiles, and clinicians should consider local resistance patterns when choosing between CAZ-AVI and MEM-VAB.
- X.
- Both CAZ-AVI and MEM-VAB are essential in managing KPC-producing Enterobacterales infections, and further research is needed to optimize treatment strategies in this challenging context.
7. Materials and Methods
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Centre for Disease Prevention and Control Antimicrobial Resistance in the EU/EEA (EARS-Net)—Annual Epidemiological Report. 2020. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe-2021 (accessed on 2 March 2023).
- Kalil, A.C.; Klompas, M. Ceftazidime-avibactam versus meropenem for the treatment of nosocomial pneumonia. Lancet Infect. Dis. 2018, 18, 229–231. [Google Scholar] [CrossRef] [PubMed]
- Falcone, M.; Tiseo, G.; Carbonara, S.; Marino, A.; Di Caprio, G.; Carretta, A.; Mularoni, A.; Mariani, M.F.; Maraolo, A.E.; Scotto, R.; et al. Mortality Attributable to Bloodstream Infections Caused by Different Carbapenem-Resistant Gram-Negative Bacilli: Results from a Nationwide Study in Italy (ALARICO Network). Clin. Infect. Dis. 2023, 76, 2059–2069. [Google Scholar] [CrossRef]
- Naimi, T.; Ringwald, P.; Besser, R.; Thompson, S.; Bell, D. Antimicrobial Resistance. Available online: https://www.who.int/health-topics/antimicrobial-resistance (accessed on 2 March 2023).
- Gaibani, P.; Giani, T.; Bovo, F.; Lombardo, D.; Amadesi, S.; Lazzarotto, T.; Coppi, M.; Rossolini, G.M.; Ambretti, S. Resistance to Ceftazidime/Avibactam, Meropenem/Vaborbactam and Imipenem/Relebactam in Gram-Negative MDR Bacilli: Molecular Mechanisms and Susceptibility Testing. Antibiotics 2022, 11, 628. [Google Scholar] [CrossRef] [PubMed]
- Tehrani, K.H.M.E.; Martin, N.I. Β-Lactam/Β-Lactamase Inhibitor Combinations: An Update. Medchemcomm 2018, 9, 1439–1456. [Google Scholar] [CrossRef] [PubMed]
- Salmon-Rousseau, A.; Martins, C.; Blot, M.; Buisson, M.; Mahy, S.; Chavanet, P.; Piroth, L. Comparative review of imipenem/cilastatin versus meropenem. Med. Mal. Infect. 2020, 50, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S.; Hujer, A.M.; Rojas, L.J.; Papp-Wallace, K.M.; Humphries, R.M.; Spellberg, B.; Hujer, K.M.; Marshall, E.K.; Rudin, S.D.; Perez, F.; et al. Can ceftazidime-avibactam and aztreonam overcome β-lactam resistance conferred by metallo-β-lactamases in Enterobacteriaceae? Antimicrob. Agents Chemother. 2017, 61, e02243-16. [Google Scholar] [CrossRef] [PubMed]
- Tuon, F.F.; Rocha, J.L.; Formigoni-Pinto, M.R. Pharmacological aspects and spectrum of action of ceftazidime–avibactam: A systematic review. Infection 2018, 46, 165–181. [Google Scholar] [CrossRef]
- Zhanel, G.G.; Lawson, C.D.; Adam, H.; Schweizer, F.; Zelenitsky, S.; Lagacé-Wiens, P.R.S.; Denisuik, A.; Rubinstein, E.; Gin, A.S.; Hoban, D.J.; et al. Ceftazidime-avibactam: A novel cephalosporin/β-lactamase inhibitor combination. Drugs 2013, 73, 159–177. [Google Scholar] [CrossRef]
- Xu, T.; Guo, Y.; Ji, Y.; Wang, B.; Zhou, K. Epidemiology and Mechanisms of Ceftazidime–Avibactam Resistance in Gram-Negative Bacteria. Engineering 2022, 11, 138–145. [Google Scholar] [CrossRef]
- Singh, S.D.S.; Ranjini, R.; Aswathi, G. A review on clinical insights of the novel ceftazidime-avibactam in gram negative infections. World J. Pharm. Pharm. Sci. 2021, 10, 1037–1050. [Google Scholar]
- González-Bello, C.; Rodríguez, D.; Pernas, M.; Rodríguez, Á.; Colchón, E. β-Lactamase Inhibitors to Restore the Efficacy of Antibiotics against Superbugs. J. Med. Chem. 2020, 63, 1859–1881. [Google Scholar] [CrossRef] [PubMed]
- Novelli, A.; Del Giacomo, P.; Rossolini, G.M.; Tumbarello, M. Meropenem/vaborbactam: A next generation β-lactam β-lactamase inhibitor combination. Expert Rev. Anti Infect. Ther. 2020, 18, 643–655. [Google Scholar] [CrossRef] [PubMed]
- Giri, P.; Patel, H.; Srinivas, N.R. Review of Clinical Pharmacokinetics of Avibactam, A Newly Approved non-β lactam β-lactamase Inhibitor Drug, in Combination Use with Ceftazidime. Drug Res. 2019, 69, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Sy, S.K.B.; Zhuang, L.; Sy, S.; Derendorf, H. Clinical Pharmacokinetics and Pharmacodynamics of Ceftazidime–Avibactam Combination: A Model-Informed Strategy for its Clinical Development. Clin. Pharmacokinet. 2019, 58, 545–564. [Google Scholar] [CrossRef] [PubMed]
- Dimelow, R.; Wright, J.G.; MacPherson, M.; Newell, P.; Das, S. Population Pharmacokinetic Modelling of Ceftazidime and Avibactam in the Plasma and Epithelial Lining Fluid of Healthy Volunteers. Drugs RD 2018, 18, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Drwiega, E.N.; Rodvold, K.A. Penetration of Antibacterial Agents into Pulmonary Epithelial Lining Fluid: An Update. Clin. Pharmacokinet. 2022, 61, 17–46. [Google Scholar] [CrossRef]
- Zhanel, G.G.; Lawrence, C.K.; Adam, H.; Schweizer, F.; Zelenitsky, S.; Zhanel, M.; Lagacé-Wiens, P.R.S.; Walkty, A.; Denisuik, A.; Golden, A.; et al. Imipenem–Relebactam and Meropenem–Vaborbactam: Two Novel Carbapenem-β-Lactamase Inhibitor Combinations. Drugs 2018, 78, 65–98. [Google Scholar] [CrossRef]
- Armstrong, T.; Fenn, S.J.; Hardie, K.R. JMM Profile: Carbapenems: A broad-spectrum antibiotic. J. Med. Microbiol. 2021, 70, 001462. [Google Scholar] [CrossRef]
- Cho, J.C.; Zmarlicka, M.T.; Shaeer, K.M.; Pardo, J. Meropenem/Vaborbactam, the First Carbapenem/β-Lactamase Inhibitor Combination. Ann. Pharmacother. 2018, 52, 769–779. [Google Scholar] [CrossRef]
- Shoulders, B.R.; Casapao, A.M.; Venugopalan, V. An Update on Existing and Emerging Data for Meropenem-Vaborbactam. Clin. Ther. 2020, 42, 692–702. [Google Scholar] [CrossRef]
- Griffith, D.C.; Sabet, M.; Tarazi, Z.; Lomovskaya, O.; Dudley, M.N. Pharmacokinetics/pharmacodynamics of vaborbactam, a novel beta-lactamase inhibitor, in combination with meropenem. Antimicrob. Agents Chemother. 2019, 63, e01659-18. [Google Scholar] [CrossRef] [PubMed]
- Finazzi, S.; Luci, G.; Olivieri, C.; Langer, M.; Mandelli, G.; Corona, A.; Viaggi, B.; Di Paolo, A. Tissue Penetration of Antimicrobials in Intensive Care Unit Patients: A Systematic Review—Part I. Antibiotics 2022, 11, 1164. [Google Scholar] [CrossRef] [PubMed]
- Lomovskaya, O.; Sun, D.; Rubio-Aparicio, D.; Nelson, K.; Tsivkovski, R.; Griffith, D.C.; Dudley, M.N. Vaborbactam: Spectrum of beta-lactamase inhibition and impact of resistance mechanisms on activity in enterobacteriaceae. Antimicrob. Agents Chemother. 2017, 61, e01443-17. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Rubio-Aparicio, D.; Nelson, K.; Dudley, M.N.; Lomovskaya, O. Meropenem-vaborbactam resistance selection, resistance prevention, and molecular mechanisms in mutants of KPC-producing Klebsiella pneumoniae. Antimicrob. Agents Chemother. 2017, 61, e01694-17. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Yang, Q.; Lomovskaya, O.; Sun, D.; Kudinha, T.; Xu, Z.; Zhang, G.; Chen, X.; Xu, Y. In vitro activity of meropenem combined with vaborbactam against KPC-producing Enterobacteriaceae in China. J. Antimicrob. Chemother. 2018, 73, 2789–2796. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing (EUCAST) EUCAST: Clinical Breakpoints and Dosing of Antibiotics. Available online: https://www.eucast.org/clinical_breakpoints/ (accessed on 28 September 2023).
- Papadomanolaki, A.; Siopi, M.; Karakosta, P.; Vourli, S.; Pournaras, S. Comparative Evaluation of Vitek 2 and Etest versus Broth Microdilution for Ceftazidime/Avibactam and Ceftolozane/Tazobactam Susceptibility Testing of Enterobacterales and Pseudomonas aeruginosa. Antibiotics 2022, 11, 865. [Google Scholar] [CrossRef] [PubMed]
- Jean, S.; Garrett, S.; Anglade, C.; Bridon, L.; Davies, L.; Garner, O.B.; Richards, J.; Wallace, M.; Wootton, M.; Burnhama, C.A.D. Multicenter clinical evaluation of etest meropenem-vaborbactam (bioMérieux) for Susceptibility testing of Enterobacterales (Enterobacteriaceae) and Pseudomonas aeruginosa. J. Clin. Microbiol. 2020, 58, e01205-19. [Google Scholar] [CrossRef] [PubMed]
- Humphries, R.; Campeau, S.; Davis, T.E.; Nagaro, K.J.; LaBombardi, V.J.; Franklin, S.; Heimbach, L.; Dwivedi, H.P. Multicenter evaluation of ceftazidime-avibactam susceptibility testing of enterobacterales and pseudomonas aeruginosa on the vitek 2 system. J. Clin. Microbiol. 2021, 59, e01870-20. [Google Scholar] [CrossRef]
- Dwivedi, H.P.; Franklin, S.; Chandrasekaran, S.; Garner, O.; Traczewski, M.M.; Beasley, D.; Procop, G.W.; Tuohy, M.; Wilson, D.; Bala, Y.; et al. Multicenter Clinical Evaluation of Vitek 2 Meropenem-Vaborbactam for Susceptibility Testing of Enterobacterales and Pseudomonas aeruginosa. J. Clin. Microbiol. 2022, 60, e0161021. [Google Scholar] [CrossRef]
- Wilson, G.M.; Fitzpatrick, M.; Walding, K.; Gonzalez, B.; Schweizer, M.L.; Suda, K.J.; Evans, C.T. Meta-analysis of Clinical Outcomes Using Ceftazidime/Avibactam, Ceftolozane/Tazobactam, and Meropenem/Vaborbactam for the Treatment of Multidrug-Resistant Gram-Negative Infections. Open Forum Infect. Dis. 2021, 8, ofaa651. [Google Scholar] [CrossRef]
- Shields, R.K.; Nguyen, M.H.; Chen, L.; Press, E.G.; Potoski, B.A.; Marini, R.V.; Doi, Y.; Kreiswirth, B.N.; Clancy, C.J. Ceftazidime-avibactam is superior to other treatment regimens against carbapenem-resistant Klebsiella pneumoniae bacteremia. Antimicrob. Agents Chemother. 2017, 61, e00883-17. [Google Scholar] [CrossRef] [PubMed]
- Tumbarello, M.; Trecarichi, E.M.; Corona, A.; De Rosa, F.G.; Bassetti, M.; Mussini, C.; Menichetti, F.; Viscoli, C.; Campoli, C.; Venditti, M.; et al. Efficacy of Ceftazidime-Avibactam Salvage Therapy in Patients with Infections Caused by Klebsiella pneumoniae Carbapenemase-producing K. pneumoniae. Clin. Infect. Dis. 2019, 68, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Marino, A.; Pulvirenti, S.; Campanella, E.; Stracquadanio, S.; Ceccarelli, M.; Micali, C.; Tina, L.G.; Di Dio, G.; Stefani, S.; Cacopardo, B.; et al. Ceftazidime-Avibactam Treatment for Klebsiella pneumoniae Bacteremia in Preterm Infants in NICU: A Clinical Experience. Antibiotics 2023, 12, 1169. [Google Scholar] [CrossRef] [PubMed]
- Castón, J.J.; Cano, A.; Pérez-Camacho, I.; Aguado, J.M.; Carratalá, J.; Ramasco, F.; Soriano, A.; Pintado, V.; Castelo-Corral, L.; Sousa, A.; et al. Impact of ceftazidime/avibactam versus best available therapy on mortality from infections caused by carbapenemase-producing Enterobacterales (CAVICOR study). J. Antimicrob. Chemother. 2022, 77, 1452–1460. [Google Scholar] [CrossRef] [PubMed]
- Shields, R.K.; McCreary, E.K.; Marini, R.V.; Kline, E.G.; Jones, C.E.; Hao, B.; Chen, L.; Kreiswirth, B.N.; Doi, Y.; Clancy, C.J.; et al. Early experience with meropenem- vaborbactam for treatment of carbapenem-resistant enterobacteriaceae infections. Clin. Infect. Dis. 2020, 71, 667–671. [Google Scholar] [CrossRef] [PubMed]
- EMA Zavicefta|European Medicines Agency. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/zavicefta (accessed on 31 August 2023).
- Torres, A.; Zhong, N.; Pachl, J.; Timsit, J.F.; Kollef, M.; Chen, Z.; Song, J.; Taylor, D.; Laud, P.J.; Stone, G.G.; et al. Ceftazidime-avibactam versus meropenem in nosocomial pneumonia, including ventilator-associated pneumonia (REPROVE): A randomised, double-blind, phase 3 non-inferiority trial. Lancet Infect. Dis. 2018, 18, 285–295. [Google Scholar] [CrossRef] [PubMed]
- Vazquez, J.A.; González Patzán, L.D.; Stricklin, D.; Duttaroy, D.D.; Kreidly, Z.; Lipka, J.; Sable, C. Efficacy and safety of ceftazidime-avibactam versus imipenem-cilastatin in the treatment of complicated urinary tract infections, including acute pyelonephritis, in hospitalized adults: Results of a prospective, investigator-blinded, randomized study. Curr. Med. Res. Opin. 2012, 28, 1921–1931. [Google Scholar] [CrossRef] [PubMed]
- Mazuski, J.E.; Gasink, L.B.; Armstrong, J.; Broadhurst, H.; Stone, G.G.; Rank, D.; Llorens, L.; Newell, P.; Pachl, J. Efficacy and safety of ceftazidime-avibactam plus metronidazole versus meropenem in the treatment of complicated intra-abdominal infection: Results from a randomized, controlled, double-blind, phase 3 program. Clin. Infect. Dis. 2016, 62, 1380–1389. [Google Scholar] [CrossRef]
- Sternbach, N.; Weissman, Y.L.; Avni, T.; Yahav, D. Efficacy and safety of ceftazidime/avibactam: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2018, 73, 2021–2029. [Google Scholar] [CrossRef]
- Isler, B.; Ezure, Y.; Romero, J.L.G.F.; Harris, P.; Stewart, A.G.; Paterson, D.L. Is ceftazidime/avibactam an option for serious infections due to extended-spectrum-β-lactamase- and ampc-producing enterobacterales?: A systematic review and meta-analysis. Antimicrob. Agents Chemother. 2021, 65, e01052-20. [Google Scholar] [CrossRef]
- Giddins, M.J.; Macesic, N.; Annavajhala, M.K.; Stump, S.; Khan, S.; McConville, T.H.; Mehta, M.; Gomez-Simmonds, A.; Uhlemanna, A.C. Successive emergence of ceftazidime-avibactam resistance through distinct genomic adaptations in blaKPC-2-harboring klebsiella pneumoniae sequence type 307 isolates. Antimicrob. Agents Chemother. 2018, 62, e02101-17. [Google Scholar] [CrossRef] [PubMed]
- Gaibani, P.; Campoli, C.; Lewis, R.E.; Volpe, S.L.; Scaltriti, E.; Giannella, M.; Pongolini, S.; Berlingeri, A.; Cristini, F.; Bartoletti, M.; et al. In vivo evolution of resistant subpopulations of KPC-producing Klebsiella pneumoniae during ceftazidime/avibactam treatment. J. Antimicrob. Chemother. 2018, 73, 1525–1529. [Google Scholar] [CrossRef] [PubMed]
- Shields, R.K.; Potoski, B.A.; Haidar, G.; Hao, B.; Doi, Y.; Chen, L.; Press, E.G.; Kreiswirth, B.N.; Clancy, C.J.; Nguyen, M.H. Clinical Outcomes, Drug Toxicity, and Emergence of Ceftazidime-Avibactam Resistance among Patients Treated for Carbapenem-Resistant Enterobacteriaceae Infections. Clin. Infect. Dis. 2016, 63, 1615–1618. [Google Scholar] [CrossRef] [PubMed]
- Ackley, R.; Roshdy, D.; Meredith, J.; Minor, S.; Anderson, W.E.; Capraro, G.A.; Polk, C. Meropenem-vaborbactam versus ceftazidime-avibactam for treatment of carbapenem-resistant enterobacteriaceae infections. Antimicrob. Agents Chemother. 2020, 64, e02313-19. [Google Scholar] [CrossRef] [PubMed]
- Shields, R.K.; Chen, L.; Cheng, S.; Chavda, K.D.; Press, E.G.; Snyder, A.; Pandey, R.; Doi, Y.; Kreiswirth, B.N.; Nguyen, M.H.; et al. Emergence of ceftazidime-avibactam resistance due to plasmid-borne blaKPC-3 mutations during treatment of carbapenem-resistant Klebsiella pneumoniae infections. Antimicrob. Agents Chemother. 2017, 61, e02097-16. [Google Scholar] [CrossRef] [PubMed]
- Barnes, M.D.; Winkler, M.L.; Taracila, M.A.; Page, M.G.; Desarbre, E.; Kreiswirth, B.N.; Shields, R.K.; Nguyen, M.H.; Clancy, C.; Spellberg, B.; et al. Klebsiella pneumoniae carbapenemase-2 (KPC-2), substitutions at ambler position Asp179, and resistance to ceftazidime-avibactam: Unique antibiotic-resistant phenotypes emerge from β-lactamase protein engineering. MBio 2017, 8, e00528-17. [Google Scholar] [CrossRef] [PubMed]
- Compain, F.; Arthur, M. Impaired inhibition by avibactam and resistance to the ceftazidime-avibactam combination due to the D179Y substitution in the KPC-2 β-lactamase. Antimicrob. Agents Chemother. 2017, 61, e00451-17. [Google Scholar] [CrossRef]
- Soriano, A.; Montravers, P.; Bassetti, M.; Klyasova, G.; Daikos, G.; Irani, P.; Stone, G.; Chambers, R.; Peeters, P.; Shah, M.; et al. The Use and Effectiveness of Ceftazidime–Avibactam in Real-World Clinical Practice: EZTEAM Study. Infect. Dis. Ther. 2023, 12, 891–917. [Google Scholar] [CrossRef]
- Jorgensen, S.C.J.; Trinh, T.D.; Zasowski, E.J.; Lagnf, A.M.; Bhatia, S.; Melvin, S.M.; Steed, M.E.; Simon, S.P.; Estrada, S.J.; Morrisette, T.; et al. Real-world experience with ceftazidime-avibactam for multidrug-resistant gram-negative bacterial infections. Open Forum Infect. Dis. 2019, 6, ofz522. [Google Scholar] [CrossRef]
- Zurriaga, I.; Herráiz, R.E.; Abánades, P.M.; Béjar, S.C.; Baladrón, M.A. Ceftazidime-avibactam: Effectiveness and safety in the clinical practice. A third hospital level experience. Ofil·Ilaphar 2022, 32, 57–62. [Google Scholar]
- Yang, P.; Li, Y.; Wang, X.; Chen, N.; Lu, X. Efficacy and safety of ceftazidime-avibactam versus polymyxins in the treatment of carbapenem-resistant Enterobacteriaceae infection: A systematic review and meta-analysis. BMJ Open 2023, 13, e070491. [Google Scholar] [CrossRef] [PubMed]
- Kaye, K.S.; Bhowmick, T.; Metallidis, S.; Bleasdale, S.C.; Sagan, O.S.; Stus, V.; Vazquez, J.; Zaitsev, V.; Bidair, M.; Chorvat, E.; et al. Effect of meropenem-vaborbactam vs piperacillin-Tazobactam on clinical cure or improvement and microbial eradication in complicated urinary tract infection the TANGO I randomized clinical trial. J. Am. Med. Assoc. 2018, 319, 788–799. [Google Scholar] [CrossRef] [PubMed]
- Wunderink, R.G.; Giamarellos-Bourboulis, E.J.; Rahav, G.; Mathers, A.J.; Bassetti, M.; Vazquez, J.; Cornely, O.A.; Solomkin, J.; Bhowmick, T.; Bishara, J.; et al. Effect and Safety of Meropenem–Vaborbactam versus Best-Available Therapy in Patients with Carbapenem-Resistant Enterobacteriaceae Infections: The TANGO II Randomized Clinical Trial. Infect. Dis. Ther. 2018, 7, 439–455. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Giacobbe, D.R.; Patel, N.; Tillotson, G.; Massey, J. Efficacy and Safety of Meropenem–Vaborbactam Versus Best Available Therapy for the Treatment of Carbapenem-Resistant Enterobacteriaceae Infections in Patients Without Prior Antimicrobial Failure: A Post Hoc Analysis. Adv. Ther. 2019, 36, 1771–1777. [Google Scholar] [CrossRef] [PubMed]
- Alosaimy, S.; Lagnf, A.M.; Morrisette, T.; Scipione, M.R.; Zhao, J.J.; Jorgensen, S.C.J.; Mynatt, R.; Carlson, T.J.; Jo, J.; Garey, K.W.; et al. Real-world, Multicenter Experience with Meropenem-Vaborbactam for Gram-Negative Bacterial Infections including Carbapenem-Resistant Enterobacterales and Pseudomonas aeruginosa. Open Forum Infect. Dis. 2021, 8, ofab371. [Google Scholar] [CrossRef] [PubMed]
- Tumbarello, M.; Raffaelli, F.; Cascio, A.; Falcone, M.; Signorini, L.; Mussini, C.; De Rosa, F.G.; Losito, A.R.; De Pascale, G.; Pascale, R.; et al. Compassionate use of meropenem/vaborbactam for infections caused by KPC-producing Klebsiella pneumoniae: A multicentre study. JAC-Antimicrobial Resist. 2022, 4, dlac022. [Google Scholar] [CrossRef] [PubMed]
- Tiseo, G.; Suardi, L.R.; Leonildi, A.; Giordano, C.; Barnini, S.; Falcone, M. Meropenem/vaborbactam plus aztreonam for the treatment of New Delhi metallo-β-lactamase-producing Klebsiella pneumoniae infections. J. Antimicrob. Chemother. 2023, 78, 2377–2379. [Google Scholar] [CrossRef] [PubMed]
- Belati, A.; Bavaro, D.F.; Saracino, A.; Diella, L.; De Gennaro, N.; Di Gennaro, F. Meropenem/Vaborbactam Plus Aztreonam as a Possible Treatment Strategy for Bloodstream Infections Caused by Ceftazidime/Avibactam-Resistant Klebsiella pneumoniae: A Retrospective Case Series and Literature Review. Antibiotics 2022, 11, 373. [Google Scholar] [CrossRef]
- Rogers, T.M.; Kline, E.G.; Griffith, M.P.; Jones, C.E.; Rubio, A.M.; Squires, K.M.; Shields, R.K. Impact of ompk36 genotype and KPC subtype on the in vitro activity of ceftazidime/avibactam, imipenem/relebactam and meropenem/vaborbactam against KPC-producing K. pneumoniae clinical isolates. JAC-Antimicrobial Resist. 2023, 5, dlad022. [Google Scholar] [CrossRef]
- Hackel, M.A.; Lomovskaya, O.; Dudley, M.N.; Karlowsky, J.A.; Sahm, D.F. In vitro activity of meropenem-vaborbactam against clinical isolates of KPC-positive Enterobacteriaceae. Antimicrob. Agents Chemother. 2018, 62, 1904-17. [Google Scholar] [CrossRef]
- El-Sokkary, R.; Erdem, H.; Kullar, R.; Pekok, A.U.; Amer, F.; Grgić, S.; Carevic, B.; El-Kholy, A.; Liskova, A.; Özdemir, M.; et al. Self-reported antibiotic stewardship and infection control measures from 57 intensive care units: An international ID-IRI survey. J. Infect. Public Health 2022, 15, 950–954. [Google Scholar] [CrossRef]
- Gordon, J.; Gheorghe, M.; Goldenberg, S.; Miller, R.; Dennis, J.; Al-Taie, A. Capturing Value Attributes in the Economic Evaluation of Ceftazidime with Avibactam for Treating Severe Aerobic Gram-Negative Bacterial Infections in the United Kingdom. Pharmacoeconomics 2023, 2023, 1–17. [Google Scholar] [CrossRef]
- Marino, A.; Stracquadanio, S.; Campanella, E.; Munafò, A.; Gussio, M.; Ceccarelli, M.; Bernardini, R.; Nunnari, G.; Cacopardo, B. Intravenous Fosfomycin: A Potential Good Partner for Cefiderocol. Clinical Experience and Considerations. Antibiotics 2023, 12, 49. [Google Scholar] [CrossRef]
- Karaiskos, I.; Galani, I.; Souli, M.; Giamarellou, H. Novel β-lactam-β-lactamase inhibitor combinations: Expectations for the treatment of carbapenem-resistant Gram-negative pathogens. Expert Opin. Drug Metab. Toxicol. 2019, 15, 133–149. [Google Scholar] [CrossRef]
- Rapporto CRE—Dati. Available online: https://www.epicentro.iss.it/antibiotico-resistenza/cre-dati (accessed on 13 September 2023).
- Bongiorno, D.; Bivona, D.A.; Cicino, C.; Trecarichi, E.M.; Russo, A.; Marascio, N.; Mezzatesta, M.L.; Musso, N.; Privitera, G.F.; Quirino, A.; et al. Omic insights into various ceftazidime-avibactam-resistant Klebsiella pneumoniae isolates from two southern Italian regions. Front. Cell. Infect. Microbiol. 2023, 12, 1010979. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marino, A.; Campanella, E.; Stracquadanio, S.; Calvo, M.; Migliorisi, G.; Nicolosi, A.; Cosentino, F.; Marletta, S.; Spampinato, S.; Prestifilippo, P.; et al. Ceftazidime/Avibactam and Meropenem/Vaborbactam for the Management of Enterobacterales Infections: A Narrative Review, Clinical Considerations, and Expert Opinion. Antibiotics 2023, 12, 1521. https://doi.org/10.3390/antibiotics12101521
Marino A, Campanella E, Stracquadanio S, Calvo M, Migliorisi G, Nicolosi A, Cosentino F, Marletta S, Spampinato S, Prestifilippo P, et al. Ceftazidime/Avibactam and Meropenem/Vaborbactam for the Management of Enterobacterales Infections: A Narrative Review, Clinical Considerations, and Expert Opinion. Antibiotics. 2023; 12(10):1521. https://doi.org/10.3390/antibiotics12101521
Chicago/Turabian StyleMarino, Andrea, Edoardo Campanella, Stefano Stracquadanio, Maddalena Calvo, Giuseppe Migliorisi, Alice Nicolosi, Federica Cosentino, Stefano Marletta, Serena Spampinato, Pamela Prestifilippo, and et al. 2023. "Ceftazidime/Avibactam and Meropenem/Vaborbactam for the Management of Enterobacterales Infections: A Narrative Review, Clinical Considerations, and Expert Opinion" Antibiotics 12, no. 10: 1521. https://doi.org/10.3390/antibiotics12101521