
Stenotrophomonas maltophilia Infections: A Systematic Review and Meta-Analysis of Comparative Efficacy of Available Treatments, with Critical Assessment of Novel Therapeutic Options

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria
2.3. Data Source and Search Strategy
2.4. Data Extraction
2.5. Outcomes Assessed
2.6. Quality Assessment
2.7. Statistical Analyses
2.8. Narrative Synthesis
2.9. Ethics
3. Results
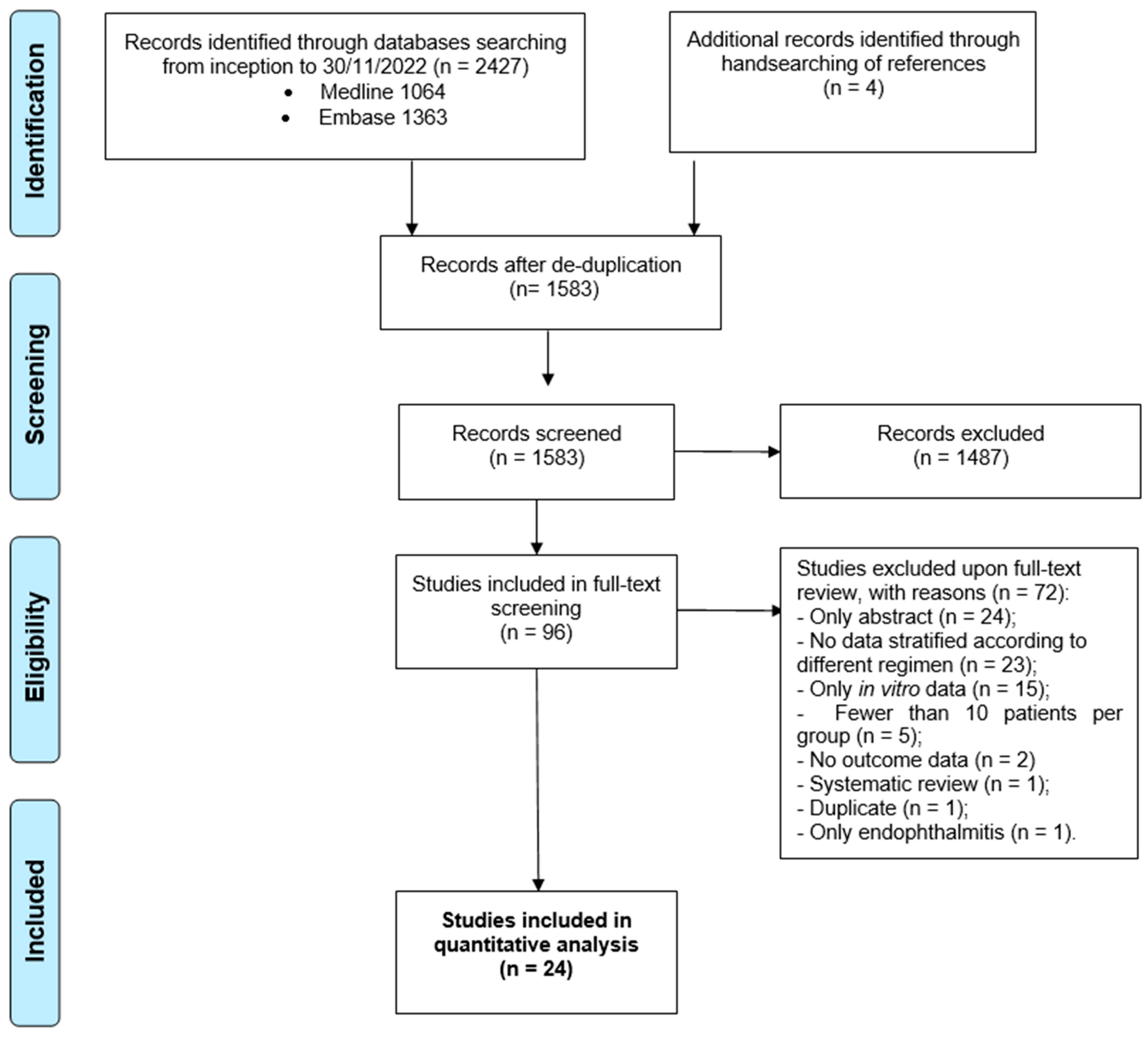
3.1. Literature Search
3.2. Study Description
3.3. Outcomes: Overview
3.4. Mortality
3.5. Clinical Failure
3.6. Safety
3.7. Length of Stay
3.8. Sources of Heterogeneity and Sensitivity Analyses
3.9. Publication Bias and Quality Assessment
4. Discussion
5. New Therapeutic Options
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brooke, J.S. Stenotrophomonas maltophilia: An Emerging Global Opportunistic Pathogen. Clin. Microbiol. Rev. 2012, 25, 2–41. [Google Scholar] [CrossRef] [PubMed]
- Brooke, J.S. Advances in the Microbiology of Stenotrophomonas maltophilia. Clin. Microbiol. Rev. 2021, 34, e0003019. [Google Scholar] [CrossRef] [PubMed]
- Mojica, M.F.; Humphries, R.; Lipuma, J.J.; Mathers, A.J.; Rao, G.G.; Shelburne, S.A.; Fouts, D.E.; Van Duin, D.; Bonomo, R.A. Clinical challenges treating Stenotrophomonas maltophilia infections: An update. JAC-Antimicrob. Resist. 2022, 4, dlac040. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.T.; Lin, C.Y.; Chen, Y.H.; Hsueh, P.R. Update on infections caused by Stenotrophomonas maltophilia with particular attention to resistance mechanisms and therapeutic options. Front. Microbiol. 2015, 6, 893. [Google Scholar] [CrossRef]
- Wang, Y.; He, T.; Shen, Z.; Wu, C. Antimicrobial Resistance in Stenotrophomonas spp. Microbiol. Spectr. 2018, 6, 409–423. [Google Scholar] [CrossRef]
- Coppola, N.; Maraolo, A.E.; Onorato, L.; Scotto, R.; Calò, F.; Atripaldi, L.; Borrelli, A.; Corcione, A.; De Cristofaro, M.G.; Durante-Mangoni, E.; et al. Epidemiology, Mechanisms of Resistance and Treatment Algorithm for Infections Due to Carbapenem-Resistant Gram-Negative Bacteria: An Expert Panel Opinion. Antibiotics 2022, 11, 1263. [Google Scholar] [CrossRef]
- Falagas, M.E.; Kastoris, A.C.; Vouloumanou, E.K.; Rafailidis, P.I.; Kapaskelis, A.M.; Dimopoulos, G. Attributable mortality of Stenotrophomonas maltophilia infections: A systematic review of the literature. Future Microbiol. 2009, 4, 1103–1109. [Google Scholar] [CrossRef]
- Kullar, R.; Wenzler, E.; Alexander, J.; Goldstein, E.J.C. Overcoming Stenotrophomonas maltophilia Resistance for a More Rational Therapeutic Approach. Open Forum Infect. Dis. 2022, 9, ofac095. [Google Scholar] [CrossRef]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America Guidance on the Treatment of AmpC β-Lactamase–Producing Enterobacterales, Carbapenem-Resistant Acinetobacter baumannii, and Stenotrophomonas maltophilia Infections. Clin. Infect. Dis. 2022, 74, 2089–2114. [Google Scholar] [CrossRef]
- Ko, J.-H.; Kang, C.-I.; Cornejo-Juárez, P.; Yeh, K.-M.; Wang, C.-H.; Cho, S.Y.; Gözel, M.G.; Kim, S.-H.; Hsueh, P.-R.; Sekiya, N.; et al. Fluoroquinolones versus trimethoprim-sulfamethoxazole for the treatment of Stenotrophomonas maltophilia infections: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2019, 25, 546–554. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm (accessed on 2 January 2023).
- IntHout, J.; Ioannidis, J.P.A.; Rovers, M.M.; Goeman, J.J. Plea for routinely presenting prediction intervals in meta-analysis. BMJ Open 2016, 6, e010247. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Sedgwick, P. Meta-analyses: What is heterogeneity? BMJ 2015, 350, h1435. [Google Scholar] [CrossRef]
- VanderWeele, T.J.; Ding, P. Sensitivity Analysis in Observational Research: Introducing the E-Value. Ann. Intern. Med. 2017, 167, 268. [Google Scholar] [CrossRef]
- Garcia Paez, J.I.; Tengan, F.M.; Barone, A.A.; Levin, A.S.; Costa, S.F. Factors associated with mortality in patients with bloodstream infection and pneumonia due to Stenotrophomonas maltophilia. Eur. J. Clin. Microbiol. Infect. Dis. 2008, 27, 901–906. [Google Scholar] [CrossRef]
- Czosnowski, Q.A.; Wood, G.C.; Magnotti, L.J.; Croce, M.A.; Swanson, J.M.; Boucher, B.A.; Fabian, T.C. Clinical and Microbiologic Outcomes in Trauma Patients Treated for Stenotrophomonas maltophilia Ventilator-Associated Pneumonia. Pharmacotherapy 2011, 31, 338–345. [Google Scholar] [CrossRef]
- Tekçe, Y.T.; Erbay, A.; Çabadak, H.; Şen, S. Tigecycline as a therapeutic option in Stenotrophomonas maltophilia infections. J. Chemother. 2012, 24, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.Y.; Kang, C.-I.; Kim, J.; Ha, Y.E.; Chung, D.R.; Lee, N.Y.; Peck, K.R.; Song, J.-H. Can Levofloxacin Be a Useful Alternative to Trimethoprim-Sulfamethoxazole for Treating Stenotrophomonas maltophilia Bacteremia? Antimicrob. Agents Chemother. 2014, 58, 581–583. [Google Scholar] [CrossRef]
- Wang, Y.L.; Scipione, M.R.; Dubrovskaya, Y.; Papadopoulos, J. Monotherapy with Fluoroquinolone or Trimethoprim-Sulfamethoxazole for Treatment of Stenotrophomonas maltophilia Infections. Antimicrob. Agents Chemother. 2014, 58, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Gokhan Gozel, M.; Celik, C.; Elaldi, N. Stenotrophomonas maltophilia Infections in Adults: Primary Bacteremia and Pneumonia. Jundishapur J. Microbiol. 2015, 8, e23569. [Google Scholar] [CrossRef] [PubMed]
- Hand, E.; Davis, H.; Kim, T.; Duhon, B. Monotherapy with minocycline or trimethoprim/sulfamethoxazole for treatment of Stenotrophomonas maltophilia infections. J. Antimicrob. Chemother. 2016, 71, 1071–1075. [Google Scholar] [CrossRef]
- Wang, C.-H.; Lin, J.-C.; Lin, H.-A.; Chang, F.-Y.; Wang, N.-C.; Chiu, S.-K.; Lin, T.-Y.; Yang, Y.-S.; Kan, L.-P.; Yang, C.-H.; et al. Comparisons between patients with trimethoprim–sulfamethoxazole-susceptible and trimethoprim–sulfamethoxazole-resistant Stenotrophomonas maltophilia monomicrobial bacteremia: A 10-year retrospective study. J. Microbiol. Immunol. Infect. 2016, 49, 378–386. [Google Scholar] [CrossRef]
- Chen, X.; Wu, W.; He, J.; Yang, L.; Zheng, G.; Zhao, Y.; Han, X.; Wei, G.; Huang, H.; Cai, Z. Retrospective analysis of Stenotrophomonas maltophilia bacteremia: Clinical features, risk factors and therapeutic choices. Int. J. Clin. Exp. Med. 2017, 10, 12268–12276. [Google Scholar]
- Ebara, H.; Hagiya, H.; Haruki, Y.; Kondo, E.; Otsuka, F. Clinical Characteristics of Stenotrophomonas maltophilia Bacteremia: A Regional Report and a Review of a Japanese Case Series. Intern. Med. 2017, 56, 137–142. [Google Scholar] [CrossRef]
- Kim, S.H.; Cho, S.Y.; Kang, C.I.; Seok, H.; Huh, K.; Ha, Y.E.; Chung, D.R.; Lee, N.Y.; Peck, K.R.; Song, J.H. Clinical predictors of Stenotrophomonas maltophilia bacteremia in adult patients with hematologic malignancy. Ann. Hematol. 2018, 97, 343–350. [Google Scholar] [CrossRef]
- Velázquez-Acosta, C.; Zarco-Márquez, S.; Jiménez-Andrade, M.C.; Volkow-Fernández, P.; Cornejo-Juárez, P. Stenotrophomonas maltophilia bacteremia and pneumonia at a tertiary-care oncology center: A review of 16 years. Support. Care Cancer 2018, 26, 1953–1960. [Google Scholar] [CrossRef] [PubMed]
- Watson, L.; Esterly, J.; Jensen, A.O.; Postelnick, M.; Aguirre, A.; McLaughlin, M. Sulfamethoxazole/trimethoprim versus fluoroquinolones for the treatment of Stenotrophomonas maltophilia bloodstream infections. J. Glob. Antimicrob. Resist. 2018, 12, 104–106. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.J.; Kim, Y.C.; Ahn, J.Y.; Jeong, S.J.; Ku, N.S.; Choi, J.Y.; Yeom, J.-S.; Song, Y.G. Risk factors for mortality in patients with Stenotrophomonas maltophilia bacteremia and clinical impact of quinolone–resistant strains. BMC Infect. Dis. 2019, 19, 754. [Google Scholar] [CrossRef] [PubMed]
- Nys, C.; Cherabuddi, K.; Venugopalan, V.; Klinker, K.P. Clinical and Microbiologic Outcomes in Patients with Monomicrobial Stenotrophomonas maltophilia Infections. Antimicrob. Agents Chemother. 2019, 63, e00788-19. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.D.; Coe, K.E.; El Boghdadly, Z.; Wardlow, L.C.; Dela-Pena, J.C.; Stevenson, K.B.; Reed, E.E. Efficacy of combination therapy versus monotherapy in the treatment of Stenotrophomonas maltophilia pneumonia. J. Antimicrob. Chemother. 2019, 74, 2055–2059. [Google Scholar] [CrossRef]
- Latzer, I.T.; Nahum, E.; Cavari, Y.; Lazar, I.; Ben-Ari, Y.; Ben-Shimol, S.; Ben-Shalom, G.; Geffen, Y.; Goldberg, L.; Rubinstein, M.; et al. Treatment Outcomes of Stenotrophomonas maltophilia Bacteremia in Critically Ill Children: A Multicenter Experience. Pediatr. Crit. Care Med. 2019, 20, e231–e239. [Google Scholar] [CrossRef]
- Alsuhaibani, M.; Aljarbou, A.; Althawadi, S.; Alsweed, A.; Al-Hajjar, S. Stenotrophomonas maltophilia bacteremia in children: Risk factors and mortality rate. Antimicrob. Resist. Infect. Control. 2021, 10, 19. [Google Scholar] [CrossRef]
- Junco, S.J.; Bowman, M.C.; Turner, R.B. Clinical outcomes of Stenotrophomonas maltophilia infection treated with trimethoprim/sulfamethoxazole, minocycline, or fluoroquinolone monotherapy. Int. J. Antimicrob. Agents 2021, 58, 106367. [Google Scholar] [CrossRef]
- Puech, B.; Canivet, C.; Teysseyre, L.; Miltgen, G.; Aujoulat, T.; Caron, M.; Combe, C.; Jabot, J.; Martinet, O.; Allyn, J.; et al. Effect of antibiotic therapy on the prognosis of ventilator-associated pneumonia caused by Stenotrophomonas maltophilia. Ann. Intensive Care 2021, 11, 160. [Google Scholar] [CrossRef]
- Tuncel, T.; Akalın Sr, H.; Payaslıoğlu, M.; Yılmaz, E.; Kazak, E.; Heper, Y.; Özakın, C.; Akalın, H. Healthcare-Associated Stenotrophomonas maltophilia Bacteraemia: Retrospective Evaluation of Treatment and Outcome. Cureus 2021, 13, e18916. [Google Scholar] [CrossRef]
- Zha, L.; Zhang, D.; Pan, L.; Ren, Z.; Li, X.; Zou, Y.; Li, S.; Luo, S.; Yang, G.; Tefsen, B. Tigecycline in the Treatment of Ventilator-Associated Pneumonia Due to Stenotrophomonas maltophilia: A Multicenter Retrospective Cohort Study. Infect. Dis. Ther. 2021, 10, 2415–2429. [Google Scholar] [CrossRef] [PubMed]
- Ahlström, M.G.; Knudsen, J.D.; Hertz, F.B. Stenotrophomonas maltophilia bacteraemia: 61 cases in a tertiary hospital in Denmark. Infect. Dis. 2022, 54, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Sarzynski, S.H.; Warner, S.; Sun, J.; Matsouaka, R.; Dekker, J.P.; Babiker, A.; Li, W.; Lai, Y.L.; Danner, R.L.; Fowler, V.G., Jr.; et al. Trimethoprim-Sulfamethoxazole Versus Levofloxacin for Stenotrophomonas maltophilia Infections: A Retrospective Comparative Effectiveness Study of Electronic Health Records from 154 US Hospitals. Open Forum Infect. Dis. 2022, 9, ofab644. [Google Scholar] [CrossRef]
- Veroniki, A.A.; Pavlides, M.; Patsopoulos, N.A.; Salanti, G. Reconstructing 2 × 2 contingency tables from odds ratios using the Di Pietrantonj method: Difficulties, constraints and impact in meta-analysis results. Res. Syn. Methods 2013, 4, 78–94. [Google Scholar] [CrossRef]
- Prawang, A.; Chanjamlong, N.; Rungwara, W.; Santimaleeworagun, W.; Paiboonvong, T.; Manapattanasatein, T.; Pitirattanaworranat, P.; Kitseree, P.; Kanchanasurakit, S. Combination Therapy versus Monotherapy in the Treatment of Stenotrophomonas maltophilia Infections: A Systematic Review and Meta-Analysis. Antibiotics 2022, 11, 1788. [Google Scholar] [CrossRef]
- Schmid, A.; Wolfensberger, A.; Nemeth, J.; Schreiber, P.W.; Sax, H.; Kuster, S.P. Monotherapy versus combination therapy for multidrug-resistant Gram-negative infections: Systematic Review and Meta-Analysis. Sci. Rep. 2019, 9, 15290. [Google Scholar] [CrossRef]
- Fiore, M.; Alfieri, A.; Di Franco, S.; Pace, M.C.; Simeon, V.; Ingoglia, G.; Cortegiani, A. Ceftazidime-Avibactam Combination Therapy Compared to Ceftazidime-Avibactam Monotherapy for the Treatment of Severe Infections Due to Carbapenem-Resistant Pathogens: A Systematic Review and Network Meta-Analysis. Antibiotics 2020, 9, 388. [Google Scholar] [CrossRef] [PubMed]
- Babich, T.; Naucler, P.; Valik, J.K.; Giske, C.G.; Benito, N.; Cardona, R.; Rivera, A.; Pulcini, C.; Fattah, M.A.; Haquin, J.; et al. Combination versus monotherapy as definitive treatment for Pseudomonas aeruginosa bacteraemia: A multicentre retrospective observational cohort study. J. Antimicrob. Chemother. 2021, 76, 2172–2181. [Google Scholar] [CrossRef]
- Adegoke, A.A.; Stenström, T.A.; Okoh, A.I. Stenotrophomonas maltophilia as an Emerging Ubiquitous Pathogen: Looking Beyond Contemporary Antibiotic Therapy. Front. Microbiol. 2017, 8, 2276. [Google Scholar] [CrossRef] [PubMed]
- Humphries, R.M.; Hindler, J.A. Emerging Resistance, New Antimicrobial Agents… but No Tests! The Challenge of Antimicrobial Susceptibility Testing in the Current US Regulatory Landscape. Clin. Infect. Dis. 2016, 63, 83–88. [Google Scholar] [CrossRef]
- Martínez-Servat, S.; Yero, D.; Huedo, P.; Marquez, R.; Molina, G.; Daura, X.; Gibert, I. Heterogeneous Colistin-Resistance Phenotypes Coexisting in Stenotrophomonas maltophilia Isolates Influence Colistin Susceptibility Testing. Front. Microbiol. 2018, 9, 2871. [Google Scholar] [CrossRef] [PubMed]
- Shi-Qi, A.; Berg, G. Stenotrophomonas maltophilia. Trends Microbiol. 2018, 26, 637–638. [Google Scholar] [CrossRef]
- EUCAST. EUCAST Guidance Document for S. maltophilia. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/General_documents/S_maltophilia_EUCAST_guidance_note_20120201.pdf (accessed on 2 January 2023).
- Fratoni, A.J.; Nicolau, D.P.; Kuti, J.L. Levofloxacin pharmacodynamics against Stenotrophomonas maltophilia in a neutropenic murine thigh infection model: Implications for susceptibility breakpoint revision. J. Antimicrob. Chemother. 2021, 77, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, E.B.; Bixby, M.L. What’s New in 2022 From the CLSI Subcommittee on Antimicrobial Susceptibility Testing. Contagion 2022, 7, 5. Available online: https://www.contagionlive.com/view/what-s-new-in-2022-from-the-clsi-subcommittee-on-antimicrobial-susceptibility-testing (accessed on 2 January 2023).
- Gales, A.C.; Seifert, H.; Gur, D.; Castanheira, M.; Jones, R.N.; Sader, H.S. Antimicrobial Susceptibility of Acinetobacter calcoaceticus–Acinetobacter baumannii Complex and Stenotrophomonas maltophilia Clinical Isolates: Results From the SENTRY Antimicrobial Surveillance Program (1997–2016). Open Forum Infect. Dis. 2019, 6 (Suppl. 1), S34–S46. [Google Scholar] [CrossRef] [PubMed]
- Rhoads, D.D. Stenotrophomonas maltophilia Susceptibility Testing Challenges and Strategies. J. Clin. Microbiol. 2021, 59, e01094-21. [Google Scholar] [CrossRef] [PubMed]
- Baek, J.H.; Kim, C.O.; Jeong, S.J.; Ku, N.S.; Han, S.H.; Choi, J.Y.; Yong, D.; Song, Y.G.; Lee, K.; Kim, J.M. Clinical Factors Associated with Acquisition of Resistance to Levofloxacin in Stenotrophomonas maltophilia. Yonsei Med. J. 2014, 55, 987. [Google Scholar] [CrossRef]
- Chen, C.H.; Huang, C.C.; Chung, T.C.; Hu, R.M.; Huang, Y.W.; Yang, T.C. Contribution of Resistance-Nodulation-Division Efflux Pump Operon smeU1-V-W-U2-X to Multidrug Resistance of Stenotrophomonas maltophilia. Antimicrob. Agents Chemother. 2011, 55, 5826–5833. [Google Scholar] [CrossRef]
- Rodvold, K.A.; George, J.M.; Yoo, L. Penetration of Anti-Infective Agents into Pulmonary Epithelial Lining Fluid: Focus on Antibacterial Agents. Clin. Pharmacokinet. 2011, 50, 637–664. [Google Scholar] [CrossRef]
- Yahav, D.; Lador, A.; Paul, M.; Leibovici, L. Efficacy and safety of tigecycline: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2011, 66, 1963–1971. [Google Scholar] [CrossRef]
- Stracquadanio, S.; Torti, E.; Longshaw, C.; Henriksen, A.S.; Stefani, S. In vitro activity of cefiderocol and comparators against isolates of Gram-negative pathogens from a range of infection sources: SIDERO-WT-2014–2018 studies in Italy. J. Glob. Antimicrob. Resist. 2021, 25, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Chen, I.H.; Kidd, J.M.; Abdelraouf, K.; Nicolau, D.P. Comparative In Vivo Antibacterial Activity of Human-Simulated Exposures of Cefiderocol and Ceftazidime against Stenotrophomonas maltophilia in the Murine Thigh Model. Antimicrob. Agents Chemother. 2019, 63, e01558-19. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Echols, R.; Matsunaga, Y.; Ariyasu, M.; Doi, Y.; Ferrer, R.; Lodise, T.P.; Naas, T.; Niki, Y.; Paterson, D.L.; et al. Efficacy and safety of cefiderocol or best available therapy for the treatment of serious infections caused by carbapenem-resistant Gram-negative bacteria (CREDIBLE-CR): A randomised, open-label, multicentre, pathogen-focused, descriptive, phase 3 trial. Lancet Infect. Dis. 2021, 21, 226–240. [Google Scholar] [CrossRef] [PubMed]
- Biagi, M.; Lamm, D.; Meyer, K.; Vialichka, A.; Jurkovic, M.; Patel, S.; Mendes, R.E.; Bulman, Z.P.; Wenzler, E. Activity of Aztreonam in Combination with Avibactam, Clavulanate, Relebactam, and Vaborbactam against Multidrug-Resistant Stenotrophomonas maltophilia. Antimicrob. Agents Chemother. 2020, 64, e00297-20. [Google Scholar] [CrossRef]
- Mauri, C.; Maraolo, A.E.; Di Bella, S.; Luzzaro, F.; Principe, L. The Revival of Aztreonam in Combination with Avibactam against Metallo-β-Lactamase-Producing Gram-Negatives: A Systematic Review of In Vitro Studies and Clinical Cases. Antibiotics 2021, 10, 1012. [Google Scholar] [CrossRef]
- Sutcliffe, J.A.; O’Brien, W.; Fyfe, C.; Grossman, T.H. Antibacterial Activity of Eravacycline (TP-434), a Novel Fluorocycline, against Hospital and Community Pathogens. Antimicrob. Agents Chemother. 2013, 57, 5548–5558. [Google Scholar] [CrossRef]
- Xiao, M.; Huang, J.J.; Zhang, G.; Yang, W.H.; Kong, F.; Kudinha, T.; Xu, Y.C. Antimicrobial activity of omadacycline in vitro against bacteria isolated from 2014 to 2017 in China, a multi-center study. BMC Microbiol. 2020, 20, 350. [Google Scholar] [CrossRef]
- Giannella, M.; Malosso, P.; Scudeller, L.; Bussini, L.; Rebuffi, C.; Gatti, M.; Bartoletti, M.; Ianniruberto, S.; Pancaldi, L.; Pascale, R.; et al. Quality of care indicators in the management of bloodstream infections caused by Enterobacteriaceae (MAMBOO-E study): State of the art and research agenda. Int. J. Antimicrob. Agents 2021, 57, 106320. [Google Scholar] [CrossRef]
- Bavaro, D.F.; Diella, L.; Belati, A.; De Gennaro, N.; Fiordelisi, D.; Papagni, R.; Guido, G.; De Vita, E.; Frallonardo, L.; Camporeale, M.; et al. Impact of a Multistep Bundles Intervention in the Management and Outcome of Gram-Negative Bloodstream Infections: A Single-Center “Proof-of-Concept” Study. Open Forum Infect. Dis. 2022, 9, ofac488. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year [Ref.] | Country, Design and No. Centers | Study Period | Main Inclusion and Exclusion Criteria | Type of Infection | Study Population | Group | Mortality (Definition) | Safety Assessment (Definition) | Length of Stay(Definition) | Multivariable Analysis on Mortality (Type and Variables) | Comments | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reference Regimen (Number of Patients, Daily Dose, Treatment Duration, Combination Therapy [%]) | Comparator (Number of Patients, Daily Dose, Treatment Duration, Combination Therapy [%, Drug]) | Other Comparators (Number of Patients, Daily Dose, Treatment Duration, Combination Therapy [%, Drug]) If Any | |||||||||||
| Garcia Paez et al., 2008 [21] | Brazil—Retrospective -single center | From July 1999 to July 2005 | Inclusion: only adult patients. Exclusion: colonization and not infection by SM, medical record unavailable | BSI: 87% Pneumonia: 13% | Adults Male: 70% Mean age 48.9 years Malignancy: 45% | Regimen: TMP/SMX (Dosage not specified) Duration undefined | Regimen: others (Dosage not specified) Duration undefined | N/A | TMP/SMX: 26% Others: 46% (14-day) | Not addressed | Not addressed | Not addressed | Absence of therapy excluded from comparator; not clear if TMP/SMX used as monotherapy or not Polymicrobial infection: 30% Non-comparative study |
| Czosnowski et al., 2011 [22] | United States, Retrospective- Single center | January 1997–December 2007 | Inclusion: only adult, ICU. Exclusion: incomplete medical record data. | VAP | Adults Male: 76% Mean age 40 years Traumatic brain injury: 56% | Regimen: TMP/SMX (11.2 ± 3.8 mg/kg/day) Duration undefined Combination allowed | Regimen: Others (Dosage not specified) Duration undefined Combination allowed | N/A | N/A | Not addressed | Not addressed | Not addressed | Polymicrobial infection: 66% No data on mortality, only on clinical failure Treatment failure defined as either clinical failure, or microbiologic plus clinical failure: TMP/SMX: 14% Others: 8% Overall treatment duration was 11.4 days (mean) Non-comparative study |
| Tekce et al., 2012 [23] | Turkey—Retrospective cohort—Single center | From January 2008 to December 2010 | Inclusion: Patients who had received more than 3 days of TMP/SMX or tigecycline for nosocomial SM infection | Pneumonia: 51% SSI: 29% | Adults. Male: 53% Mean age 65.4 years Malignancy: 29% ICU stay: 87% | Regimen: TMP/SMX (Dosage not specified) Duration undefined 0% combination | Regimen: Tigecycline (Dosage not specified) Duration undefined 0% combination | N/A | TMP/SMX: 31% Tigecycline: 21% (30-day) | Not addressed | Not addressed | Not reported | Polymicrobial infection: 29 (64.4%) patients Comparative study |
| Cho et al., 2014 [24] | South Korea—Retrospective cohort—Single center | From 2000 to 2012 | Inclusion: only adult patients. Exclusion: combination therapy between TMP/SMX and levofloxacin, death within the first 2 days after the start of the therapy | BSI | Adults Median age 58 years (IQR 45–67) Malignancy: 52% MV: 16% | Regimen: TMP/SMX 51-patients (15–20 mg/kg of body weight/day TMP) Duration undefined 18% combination | Regimen: Levofloxacin—35 patients (750 mg/day) Duration undefined 9% combination | N/A | TMP/SMX: 27% Levofloxacin: 20% (30-day) | TMP/SMX: 24% Levofloxacin: 0% (adverse events) | TMP/SMX: median 25 days (IQR 12–51) FQs: median 27 days (IQR 15–52) (hospital stay) | Levofloxacin use versus TMP/SMX: aOR 0.62 (95% CI 0.19–2.04) Adjusted was made for septic shock and pneumonia | Data could be stratified according to monotherapy and combination therapy. Polymicrobial infection: 20% Recurrence (30-day): TMP/SMX = 12% Levofloxacin = 6% Comparative study |
| Wang YL et al., 2014 [25] | United States—Retrospective cohort—Single center | From January 2008 to December 2011 | Adult patients with nosocomial SM infection received monotherapy with TMP/SMX or an FQ for at least 48 h. | Pulmonary infection: 56% SSTI: 19% UTI: 9% IAI: 9% Secondary BSI: 6% | Adults Male: 61% Mean age: 73 years Solid organ malignancy: 39% MV: 30% | Regimen: TMP/SMX 35-patients (Dosage not specified) Median duration 8 days (IQR 2–28) 0% combination | Regimen: FQs—63 patients Levofloxacin = 76% Ciprofloxacin = 24% (Dosage not specified) Median duration 9 days (IQR 2–8) 0% combination | N/A | TMP/SMX: 22% FQs: 31% (30-day) | Not addressed | TMP/SMX: median 16 days (IQR 8–42) FQs: median 25 days (IQR 15–37) (hospital stay) | Not reported | Polymicrobial infection: 77% ICU admission at time of culture: 24% Comparative study |
| Gokhan Gozel et al., 2015 [26] | Turkey— Retrospective, Single center | From January 2006 to December 2013 | Inclusion: only adult patients. Exclusion: polymicrobial infection | BSI: 49% Pneumonia 51% | Adults Male: 66% Median age 68 years (IQR 20–87) Malignancy: 24% | Regimen: TMP/SMX—26 patients (Dosage not specified) Duration undefined 0% combination | Regimen: Levofloxacin-31 patients (Dosage not specified) Duration undefined 0% combination | N/A | TMP/SMX: 31% Levofloxacin: 23% (14-day) | Not addressed | Not addressed | Not addressed | Unpublished data of the original article were retrieved from the paper of Ko et al. [10] Polymicrobial infection: 11% Non-comparative study |
| Hand et al., 2016 [27] | United States—Retrospective—Single center | From January 2006 to December 2012 | Inclusion: adult and pediatric patients with; one positive culture for SM. Exclusion: combination therapy, concomitant antibiotics with anti-SM activity other than the ones studied. | Mixed | Male: 47% Mean age: 52 years (calculated combining two means) MV: 51% | Regimen: TMP/SMX—22 patients (average daily doses of 200 mg/day SMX and 8.5 mg/kg/day TMP) Median duration 7 days (IQR 3–15) 0% combination | Regimen: Minocycline-23 patients (200 mg daily) Median duration 14 days (IQR 4–12) 0% combination | N/A | TMP/SMX: 9% Minocycline: 9% (30-day) | Not addressed | TMP/SMX: median 54 days (IQR 4–265) Minocycline: median 41 days (IQR 6–136) (hospital stay) | Not addressed | Polymicrobial infection: 73% Treatment failure (isolation of SM on follow-up culture from the same site as the initial infection within 30 days of the initial culture or in-hospital death within 30 days of the initial positive culture or receipt of an alternative or additional antibiotic possessing in vitro activity against SM during any point of initial therapy): TMP/SMX = 39% Minocycline = 48% Comparative study |
| Wang CH et al., 2016 [28] | Taiwan—Retrospective—Single center | From January 2004 to December 2013 | Inclusion: All patients with monomicrobial SM BSI. Exclusion: patients who had polymicrobial BSI or who were aged <18 years. | BSI | Adults Male: 73% Mean age: 68.3 years Malignancy: 38% MV: 64% | Regimen: TMP/SMX—64 patients (Dosage not specified) Duration undefined 0% combination | Regimen: FQs—23 patients (Dosage not specified) Duration undefined 0% combination | N/A | TMP/SMX: 59% FQs: 9% (in-hospital) | Not addressed | Not addressed | Not addressed | Unpublished data of the original article were retrieved from the paper of Ko et al. [10] Non-comparative study |
| Chen et al., 2017 [29] | China—Retrospective cohort—Single center | From January 2009 to March 2015 | Inclusion: only adult patients. Exclusion: patients without adequate medical records or any clinical manifestation. | BSI | Adults Male: 64% Solid tumors: 26% ICU: 26% | Monotherapy—51 patients (Dosage not specified) Duration undefined | Combination therapy—27 patients (Dosage not specified) Duration undefined | N/A | Monotherapy: 25% Combination therapy: 26% (30-day) | Not addressed | Not addressed | Not addressed | In two-thirds of cases combo based on levofloxacin Non-comparative study |
| Ebara et al., 2017 [30] | South Korea—Retrospective cohort—Multicenter | From January 2007 to December 2013 | Inclusion: Adults and pediatrics with SM BSI | BSI | Adults Male: 64% | Regimen: FQs—15 patients (Dosage not specified) Duration undefined 0% combination | Regimen: Minocycline—10 patients (Dosage not specified) Duration undefined 0% combination | N/A | FQs: 53% Minocycline: 40% (90-day) | Not addressed | Not addressed | Not addressed | Unpublished data of the original article were retrieved from the paper of Ko et al. [10] Non-comparative study |
| Kim SH et al., 2018 [31] | South Korea—Retrospective cohort—Single center | From January 2006 to December 2016 | Inclusion: Adults, cancer patients; Exclusion: combination therapy | BSI | Adults Male: 59% Mean age: 55.7 years | Regimen: TMP/SMX—31 patients (Dosage not specified) Duration undefined 0% combination | Regimen: Levofloxacin—40 patients (Dosage not specified) Duration undefined 0% combination | N/A | TMP/SMX: 43% Levofloxacin: 36% (30-day) | Not addressed | Not addressed | Not addressed | Case-control study (controls being not-SM BSI) Non-comparative study |
| Velázquez-Acosta et al., 2018 [32] | Mexico—Retrospective cohort—Single center | From January 2000 to December 2016 | Adult patients with BSI or pneumonia by SM | BSI: 55% Pneumonia: 45 | Adults Male: 42% Mean age: 46.9 years Solid tumors: 63% Hematologic malignancies: 37% | Regimen: TMP/SMX—87 patients (Dosage not specified) Duration undefined 22% combination | Regimen: FQs—39 patients (Dosage not specified) Duration undefined Combination allowed | Regimen: Other—84 patients Not reported | TMP/SMX: 44% FQs: 18% Other: 24% (30-day) | Not addressed | Not addressed | No TMP/SMX use versus its use: aOR 0.87 (95% CI 0.3–2.65) Adjusting was made for age and appropriateness of therapy | Polymicrobial bacteremia: 20% (out of 95 BSI) All study population was composed of oncologic/ onco-hematologic patients Non-comparative study |
| Watson et al., 2018 [33] | United States—Retrospective cohort—Single center | From January 2004 to October 2014 | Inclusion: patients at least 18 years of age that received at least 48 h of monotherapy with FQ or TMP/SMX. Exclusion: combination active therapy or therapy for less than 48 h. | BSI | Adults Male: 48% Mean age: 51.4 years (calculated combining two means) MV: 33% | Regimen: TMP/SMX—32 patients (Dosage not specified) Duration undefined 0% combination | Regimen: FQs—22 patients (Dosage not specified) Duration undefined 0% combination | N/A | TMP/SMX: 31% FQs: 14% (in-hospital) | TMP/SMX: 6% FQs: 5% (drug discontinuation) | TMP/SMX: 15 (IQR 7–38) days Levofloxacin:9 (IQR 5–16) days (hospital LOS) | Not addressed | Comparative study |
| Kim EJ, 2019 [34] | South Korea—Retrospective cohort—Multicenter | From January 2006 to December 2014 | Inclusion: patients at least 18 years of age and positive blood culture for SM | BSI | Adults Solid tumor: 40% Hematological malignancy: 14 | Regimen: TMP/SMX—31 patients (Dosage not specified) Duration undefined Combination allowed | Regimen: FQs—40 patients (Dosage not specified) Duration undefined Combination allowed | N/A | TMP/SMX: 87% FQs: 48% (60-day) | Not addressed | Not addressed | Not addressed | Non-comparative study |
| Nys et al., 2019 [35] | United States—Retrospective cohort—Single center | From January 2012 to October 2016 | Inclusion: Adults Exclusion: polymicrobial infections. | Lung infection: 92% UTI: 3%. | Adults Male: 54% Median age: 63 (IQR 51–70) years MV: 37% | Regimen: TMP/SMX—45 patients (median dose 10.3 mg/kg/day) Median duration 13 days (IQR 8-15) 0% combination | Regimen: Levofloxacin—31 patients (median dose 750 mg/day) Median duration 13 days (8–15) 0% combination | N/A | TMP/SMX: 16% Levofloxacin: 13% (28-day) | TMP/SMX: 7% Levofloxacin: 0% (Adverse events) | Not addressed | Not addressed | Clinical cure (at the end of therapy): TMP/SMX = 82% Levofloxacin = 74% Comparative study |
| Shah et al., 2019 [36] | United States—Retrospective cohort | From November 2011 to October 2017 | Patients with SM pneumonia. Exclusion: Less than 48 h of effective therapy. | Pneumonia | Adults Mean age 62 years (derived from combining group) Male: 62% Immunocompromised: 20% Polymicrobial pneumonia: 54% | Regimen: Monotherapy—214 patients TMP/SMX= 66% FQs = 30% Other = 4% (Dosage not specified) Duration undefined | Regimen: Combination therapy—38 patients TMP/STX + FQ = 50% TMP/STX + minocycline = 16% FQs + minocycline = 13% Duration undefined (Dosage not specified) | Not reported | Monotherapy: 23% Combination therapy: 40%% (30-day) | Not addressed | Monotherapy: 22 (IQR 14–35) days Combination therapy: 22.5 (IQR 14–44) days (hospital LOS) | Not addressed | Recurrence (30-day): Monotherapy = 8% Combination therapy = 11% Clinical cure (Improvement in signs and symptoms of infection after 7 days of effective therapy): Monotherapy = 60% Combination therapy = 53% Comparative study |
| Tokatly Latzer et al., 2019 [37] | Israel—Retrospective cohort—Multicenter | From 2012 to 2017 | Patients hospitalized in pediatric ICU affected by BSI related to SM with or without a culture from a commonly sterile respiratory site | BSI: 42% CVC-related BSI: 22% BSI + Pleural fluid: 22% | Children younger than 18 years old. Oncologic: 22% Cerebral palsy: 22% Congenital cardiac disease: 15% Immunodeficiency: 9% End-stage renal disease: 7% Burss: 4% | Regimen: TMP/SMX—22 patients (Dosage not specified) Duration undefined Combination allowed | Regimen: Ciprofloxacin—13 patients (Dosage not specified) Duration undefined Combination allowed | Regimens Ciprofloxacin + TMP/SMX Ciprofloxacin + TMP/SMX + Minocycline Ceftazidime (Dosage not specified) Duration undefined Combination allowed | TMP/SMX: 27% Ciprofloxacin: 21% Ciprofloxacin + TMP/SMX: 10% Ciprofloxacin + TMP/SMX + Minocycline: 17% Ceftazidime: 14% (7-day) | Not addressed | Not addressed | Not addressed | Polymicrobial infection 37 (55%) When considering only monotherapy, just 35 cases were taken into account Non-comparative study |
| Alsuhaibani et al., 2021 [38] | Saudi Arabia,—Retrospective cohort—Single center | From January 2007 to December 2018 | Inclusion: Pediatrics patients; Exclusion: asymptomatic patients, no therapy | BSI | Pediatrics. Male: 50% Under 12 months: 38% Malignancy: 29% Polymicrobial infection 30.9% | Regimen: TMP/SMX—36 patients (Dosage not specified) Duration undefined 0% combination | Regimen: TMP/SMX + others—11 patients (Dosage not specified) Duration undefined 100% combination | N/A | TMP/SMX: 31% TMP/SMX + others: 36% (7-day) | Not addressed | Not addressed | Not addressed | Comparative study (monotherapy versus combination therapy) |
| Junco et al., 2021 [39] | United States—Retrospective cohort—Multicenter | From January 2010 to January 2016 | Inclusion: Adults; Exclusion: combination therapy, less than 48 h of monotherapy, patients with diagnosis of cystic fibrosis, resistance to initial therapy; SM infection in the previous 12 months | Pneumonia: 68%; BSI: 10%; UTI: 9%; ABSSSI: 11%; Other infections: 2%. | Adults Male: 61% Mean age: 59.6 years MV: 56% | Regimen: TMP/SMX—217 patients (median dose 9.7 mg/kg/day) Median duration 12 days 0% combination | Regimen: FQs—28 patients (Ciprofloxacin 800 mg/day or levofloxacin 750 mg/daily or moxifloxacin 400 mg/day) Median duration 12 days 0% combination | Regimen: Minocycline—39 patients (200 mg/day) Median duration 12 days 0% combination | TMP/SMX: 15% FQs: 29% Minocycline: 5% (30-day) | TMP/SMX: 47% FQs: 75% Minocycline: 74% (KDIGO AKI stage 1-2-3) | Median values TMP/SMX: 12 days (IQR 8–17) FQs: 12.5 days (IQR 8–19) Minocycline: 14 days (IQR 11–18) (infection-related LOS) | FQ use: aOR 0.3 (95% CI 0.1–2.1)— Adjusted for vasopressor support, APACHE, age, LOS prior to culture—FQ versus TMP/SMX Minocycline use: aOR 0.2 (95% CI 0.1–0–7)— Adjusted for vasopressor support, APACHE, age, LOS prior to culture-minocycline versus TMP/SMX) | Polymicrobial infection included but not specificied Clinical failure (isolation of SM from a subsequently collected culture from the same site of index culture after at least 48 h of therapy or alteration of monotherapy after at least 48 h of treatment for either an adverse event or concern for clinical failure or 30-day in-hospital all-cause mortality): TMP/SMX = 35% FQs = 29% Minocycline = 39% Comparative study (for the meta-analysis the “others” group comprised FQs plus TDs) |
| Puech et al., 2021 [40] | Reunion Island (French overseas department)—Retrospective cohort—Single center | From January 2010 to December 2018 | Patients ICU-admitted with VAP by SM | 100% VAP | Adults Male: 64% Median age: 61 [IQR 51–70] years Median SOFA: 9 [IQR 7–12] Immunoompromised: 5%; BSI: 3% Polymicrobial 58% | Regimen: TMP/SMX—80 patients (1200 mg/240 mg each 6 h) Duration undefined Combination allowed | Regimen: FQs—84 patients (ciprofloxacin 400 mg/8 h or moxifloxacin 400 mg/day) Duration undefined Combination allowed | Regimen (Other)—132 patients: Ticarcillin/ clavulanate 4 g/8 h; or ceftazidime 2 g/6 h Duration undefined Combination allowed | TMP/SMX: 50% FQs: 52% Ticarcillin/ clavulanate: 79% Ceftazidime 56% (in-hospital) | Not addressed | Not addressed | Not addressed | Monomicrobial infections in 55% cases. Monotherapy only in 4 patients (0.03%) Median MV duration: 21 [IQR 14–37] days Non-comparative study |
| Tuncel et al., 2021 [41] | Turkey—Retrospective cohort—Single center | From January 2002 to December 2016 | Adult patients with nosocomial SM BSI | Catheter-related BSI: 21% Pneumonia: 7% Intraabdominal Infection: 6% Undetected source: 67% | Median (IQR) age: 54 (18–84) years Male: 58% ICU: 51%; Inpatient clinic: 49% Solid organ malignancy 30%.; Hematological malignancy 23%; Cerebrovascular disease: 17%; Multiple underlying diseases: 31% | Regimen: TMP/SMX—49 patients Duration undefined (Dosage not specified) Combination allowed | Regimen: Levofloxacin—17 patients Duration undefined (Dosage not specified) Combination allowed | Regimen: Other—28 patients | 14-day mortality TMP/SMX: 22% Levofloxacin: 24% Other: 36% 30-day mortality TMP/SMX: 37% Levofloxacin: 24% Other: 55% | Not addressed | Not addressed | Not addressed | Polymicrobial infections: 34% Exclusion of 38 patients under TMP/SMX plus levofloxacin Non-comparative study |
| Zha et al., 2021 [42] | China—Retrospective cohort—Multicenter | From January 2017 to December 2020 | Adult patients ICU-admitted with VAP by SM | 100% VAP | Median (IQR) age = 76 (64.25–85) years Male: 79% Median APACHE II Score: 21 (IQR 16.25–24) Median Charlson index comorbidity score: 5 (IQR 4–6) Malignancy: 10 (12.2%) | Regimen: FQs—36 patients (dosage Levofloxacin 750 mg/daily; Moxifloxacin 400 mg/daily) 0% combination | Regimen: Tigecycline—46 patients (dosage: 100 mg followed by 50 mg × 2/daily) 0% combination | N/A | FQs: 28% Tigecycline: 48% (28-day) | Not addressed | Not addressed | Tigecycline versus FQs: aOR 1.64 (95% CI 0.58–4.77) Adjusting was made for the following variable: age, gender, chronic kidney disease, coagulation disorder, malignancy, polymicrobial infection, definitive antibiotic therapy, combination therapy with carbapenems, APACHE II score and Charlson comorbidity index score | Polymicrobial infections: 71% A. baumannii: 45% P. aeruginosa: 17% Clinical cure (complete resolution of all signs and symptoms of pneumonia at 14 days after the initial given dose of target antibiotics): FQs = 64% Tigecycline = 33% Comparative study |
| Ahlstrom et al., 2022 [43] | Denmark—Retrospective cohort—Single center | From January 2015 to June 2020 | Patients with positive blood culture with detectable SM | 100% BSI | Mainly adult patients with median age 41 (IQR 16–67) Male: 64% ICU: 23% | Regimen: TMP/SMX—48 patients (Dosage not specified) Duration undefined Combination allowed | Regimen: Ciprofloxacin —22 patients Duration undefined Combination allowed | N/A | TMP/SMX: 19% FQs: 18% (90-day) | Not addressed | Not addressed | TMP/SMX use: Adjusted HR 0.76 (95% CI 0.23–2.54) | 14/48 of TMP/SMX patients received ciprofloxacin, 14/22 viceversa Non-comparative study |
| Sarzynski et al., 2022 [44] | United States—Retrospective cohort—Multicenter | From January 2005 to December 2017 | Adult patients with BSI or LRTI by SM infection Exclusion: Inconsistent/no therapy | TMP/SMX: BSI = 8,4%; LRTI = 91.6% FQs: BSI = 12%; LRTI = 88% | Adults Male: 57% TMP-SMX median age: 60 [IQR, 31–72] years MV: 38.7% ICU stay: 33.5% Immunocompromised: 1% Levofloxacin: age 66 [IQR, 53–76] years MV: 31.2% ICU stay: 28.8% Immunocompromised: 1.7% | Regimen: TMP/SMX—758 patients (Dosage not specified) Duration undefined 0% combination | Regimen: Levofloxacin—823 patients (Dosage not specified) Duration undefined 0% combination | N/A | In-hospital: TMP/SMX =14.2% Levofloxacin = 10.6% Total mortality: TMP/SMX =17.7% Levofloxacin = 15.2% | Not addressed | TMP/SMX: 17 (9–31.8) days Levofloxacin:10 (5–21) days (hospital LOS) | FQs versus TMP/SMX: aOR 0.76 (95% CI 0.58–1.00). Adjusted values were computed using logistic regression after controlling for baseline patient and hospital level factors. | Polymicrobial infection: Levofloxacin = 42%, TMP/SMX = 42% Comparative study |
| Outcome: Mortality (All-Cause) | |||||||
| Comparison | Included Studies | Number of Patients | OR, 95% CI | I² | Prediction Interval | E-Value | Comments |
| TMP/SMX versus FQs | 11 | 2407 | 1.46 (1.15–1.86) | 33% | 1.10–1.93 | For point estimate: 1.71; for CI: 1.35. | See forest plot (Figure 2) for subgroup analysis about different timing of mortality. All monotherapy studies. One pediatric study [27]. FQs: five studies about levofloxacin [24,26,31,35,44], one about ciprofloxacin [37], five mixed [25,28,32,33,39]. |
| TMP/SMX versus FQs-BSI | 4 | 234 | 2.61 0.75–9.02 | 67% | 0.01–503.12 | For point estimate: 2.61; for CI: 1. | Different timing of mortality: 30-day [24], in-hospital [28,33], 7-day [37]. One pediatric study [37]. FQs: one study about levofloxacin [24], one about ciprofloxacin [37], two mixed [28,33]. |
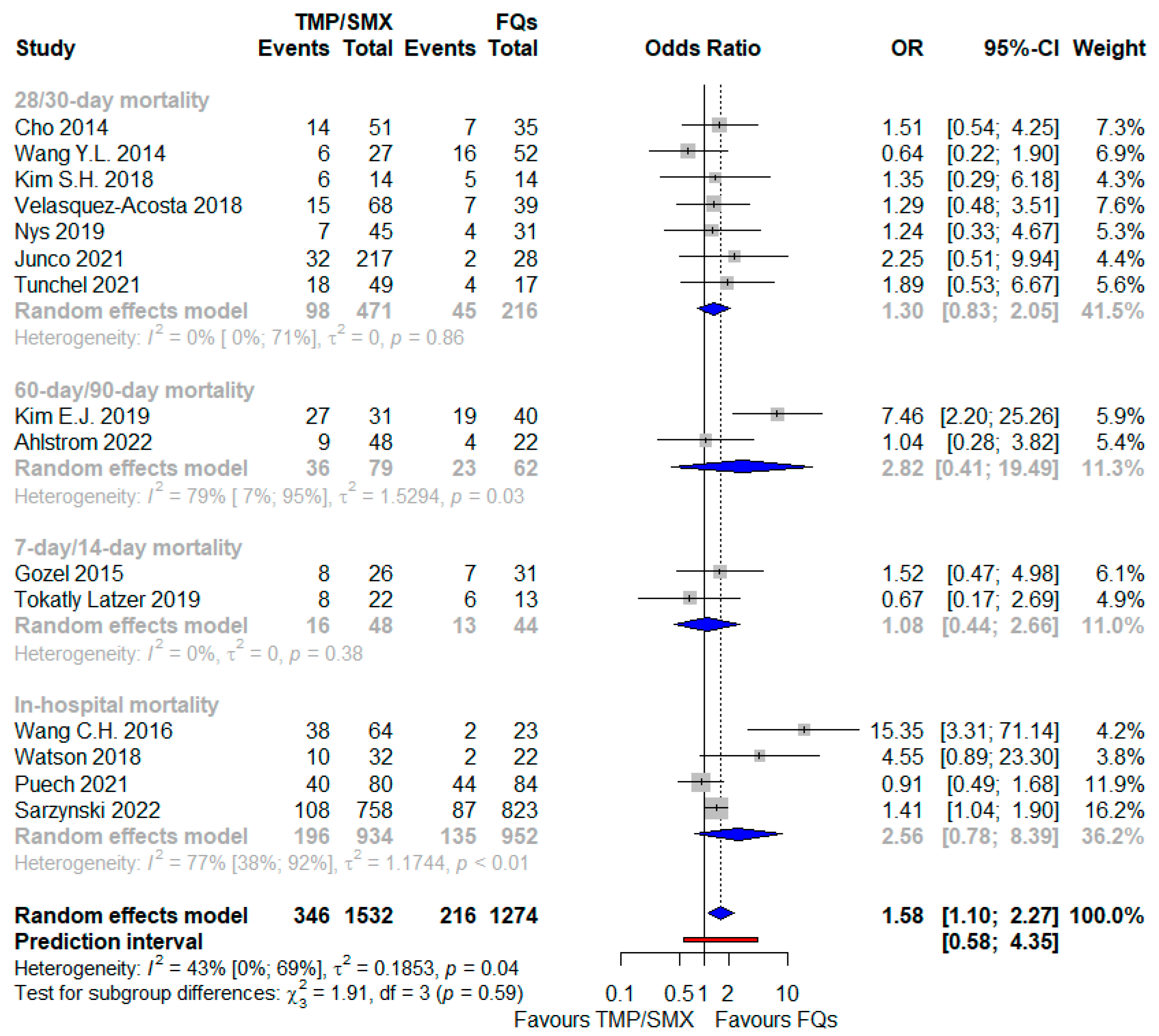
| TMP/SMX versus FQs not only monotherapy | 15 | 2806 | 1.58 (1.10–2.27) | 43% | 0.58–4.35 | For point estimate: 1.83; for CI: 1.28. | See forest plot for subgroup analysis about different timing of mortality (Figure 4). One pediatric study [37]. FQs: six studies about levofloxacin [24,26,31,35,36,44], two about ciprofloxacin [37,43], seven mixed [25,28,32,33,34,39,40]. |
| TMP/SMX versus FQs not only monotherapy-BSI | 7 | 469 | 2.45 (1.13–5.31) | 59% | 0.24–24.76 | For point estimate: 2.51; for CI: 1.32. | Different timing of mortality: 30-day [24,41], in-hospital [28,33], 60-day [34], 90-day [43], 7-day [37]. One pediatric study [37]. FQs: two studies about levofloxacin [24,41], two about ciprofloxacin [37,43], three mixed [28,33,34] |
| TMP/SMX versus TDs | 3 | 346 | 1.95 (0.79–4.82) | 0% | 0.01–685.99 | For point estimate: 2.14; for CI: 1. | All monotherapy studies. 30-day mortality. TDs: minocycline in two studies [27,39]. tigecycline in the other [23]. |
| TMP/SMX versus others | 5 | 791 | 1.33 (0.74–2.37) | 58% | 0.22–8.14 | For point estimate: 1.57; for CI: 1. | Different timing of mortality: 14-day [21], 30-day [32,39,41], in-hospital [40]. |
| FQs vs TDs | 3 | 174 | 0.80 (0.28–2.23) | 28% | 0.00–13,453.68 | For point estimate: 1.48; for CI: 1. | Different timing of mortality: 28-day [42], 30-day [39], 90-day [30]. TDs: minocycline as monotherapy in two studies [30,39], tigecycline in the other one mostly in combination for VAP [42]. |
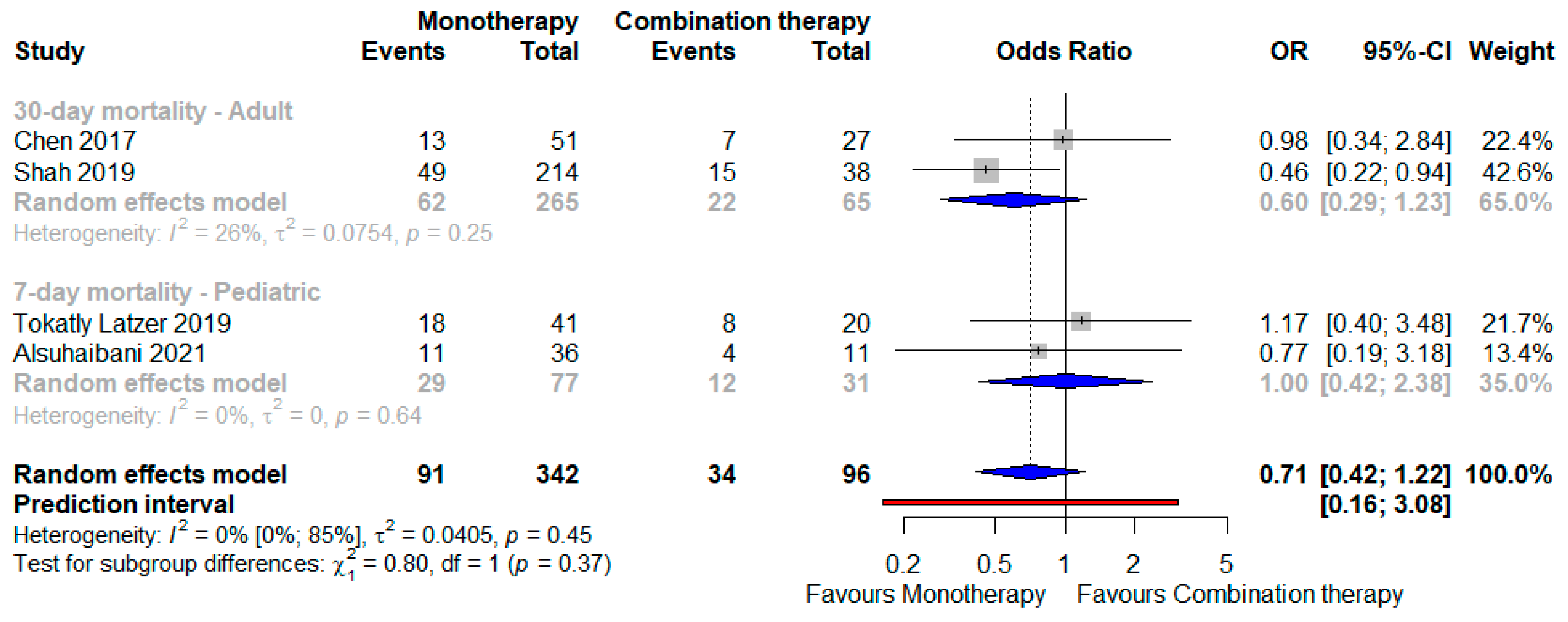
| Monotherapy versus combination | 4 | 438 | 0.71 (0.41–1.22) | 0% | 0.16–3.08 | For point estimate: 1.66; for CI: 1. | See forest plot (Figure 5) for a subgroup analysis about different timing of mortality and population. |
| Outcome: Mortality—Adjusted Effect Size | |||||||
| Comparison | Included Studies | Number of Patients | OR, 95% CI | I² | Prediction Interval | E-Value | Comments |
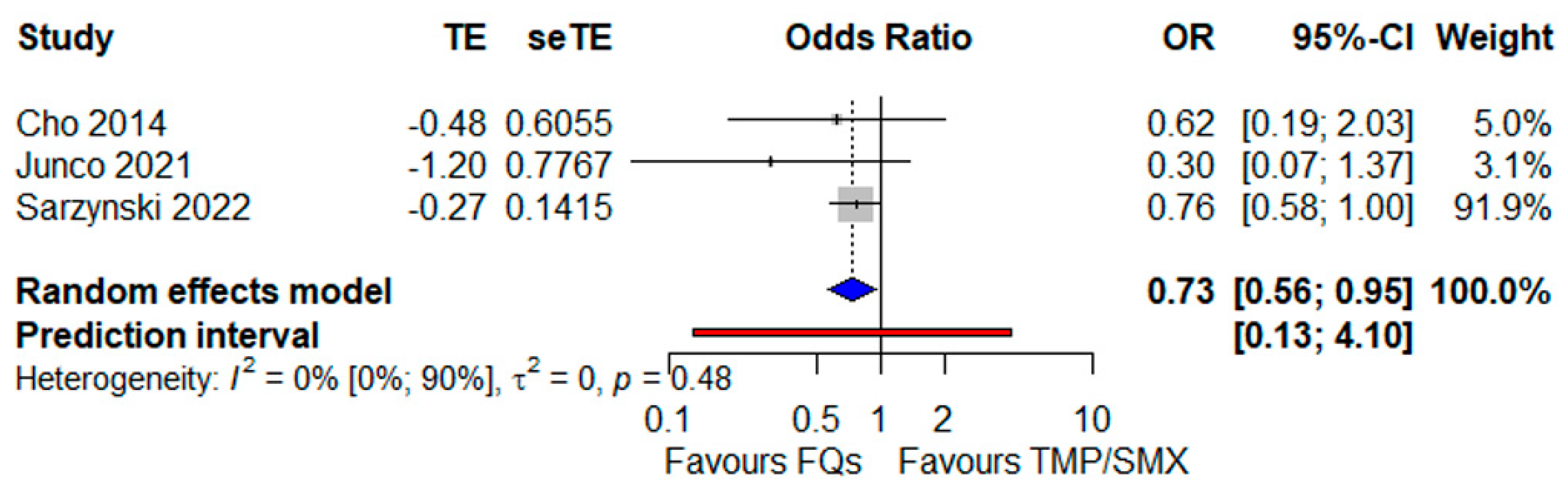
| FQs versus TMP/SMX | 3 | 1912 | 0.73 (0.56–0.95) | 0% | 0.13–4.10 | For point estimate: 1.62; for CI: 1.19. | All monotherapy studies (Figure 3). |
| Outcome: Clinical Failure | |||||||
| Comparison | Included Studies | Number of Patients | OR, 95% CI | I² | Prediction Interval | E-Value | Comments |
| TMP/SMX versus FQs | 3 | 360 | 0.94 (0.53–1.67) | 0% | 0.02–39.64 | For point estimate: 1.21; for CI: 1. | All monotherapy studies. Different definitions of clinical failure. |
| TMP/SMX versus TDs | 3 | 346 | 0.78 (0.24–2.54) | 70% | 0.00–659,171.29 | For point estimate: 1.52; for CI: 1. | All monotherapy studies. Different definitions of clinical failure. TDs: minocycline in two studies [27,39], tigecycline in the other [23]. |
| TMP/SMX versus Others | 2 | 385 | 1.35 (0.77–2.35) | 0% | Incalculable | For point estimate: 1.6; for CI: 1. | TMP/SMX always in monotherapy, comparator group based prevalently (89%) on various combination regimens. Different definitions of clinical failure. |
| FQs vs TDs | 2 | 149 | 0.48 (0.15–1.54) | 64% | Incalculable | For point estimate: 2.24: for CI: 1. | TDs: minocycline as monotherapy in one study [39], tigecycline in the other one mostly in combination for VAP [42]. Different definitions of clinical failure. |
| Outcome: Safety-Adverse Events Onset | |||||||
| Comparison | Included Studies | Number of Patients | OR, 95% CI | I² | Prediction Interval | E-Value | Comments |
| TMP/SMX versus FQs | 4 | 461 | 1.89 (0.26–13.60) | 81% | 0.00–7492.40 | For point estimate: 2.09; for CI: 1. | All monotherapy studies. Definitions: “any adverse event” for 2 studies [24,35], drug discontinuation in another [33], acute kidney injury in the last one [39]. |
| Outcome: Length of Stay | |||||||
| Comparison | Included Studies | Number of Patients | MD, 95% CI | I² | Prediction Interval | E-Value | Comments |
| TMP/SMX versus FQs | 5 | 2064 | 2.90 (−4.19–9.99) | 84% | −14.25– 20.05 | For point estimate: 1.56; for CI: 1. | All monotherapy studies except a minority of patients in Cho et al. [24] Infection-related LOS in Junco et al. [39] |
| TMP/SMX versus TDs (minocycline) | 2 | 301 | 16.33 (−252.49– 285.15) | 85% | Incalculable | For point estimate: 1.66; for CI: 1. | All monotherapy studies. Infection-related LOS in Junco et al. [39] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maraolo, A.E.; Licciardi, F.; Gentile, I.; Saracino, A.; Belati, A.; Bavaro, D.F. Stenotrophomonas maltophilia Infections: A Systematic Review and Meta-Analysis of Comparative Efficacy of Available Treatments, with Critical Assessment of Novel Therapeutic Options. Antibiotics 2023, 12, 910. https://doi.org/10.3390/antibiotics12050910
Maraolo AE, Licciardi F, Gentile I, Saracino A, Belati A, Bavaro DF. Stenotrophomonas maltophilia Infections: A Systematic Review and Meta-Analysis of Comparative Efficacy of Available Treatments, with Critical Assessment of Novel Therapeutic Options. Antibiotics. 2023; 12(5):910. https://doi.org/10.3390/antibiotics12050910
Chicago/Turabian StyleMaraolo, Alberto Enrico, Federica Licciardi, Ivan Gentile, Annalisa Saracino, Alessandra Belati, and Davide Fiore Bavaro. 2023. "Stenotrophomonas maltophilia Infections: A Systematic Review and Meta-Analysis of Comparative Efficacy of Available Treatments, with Critical Assessment of Novel Therapeutic Options" Antibiotics 12, no. 5: 910. https://doi.org/10.3390/antibiotics12050910