
Streptococcus mitis as a New Emerging Pathogen in Pediatric Age: Case Report and Systematic Review
 ,
, 
Abstract
:1. Introduction
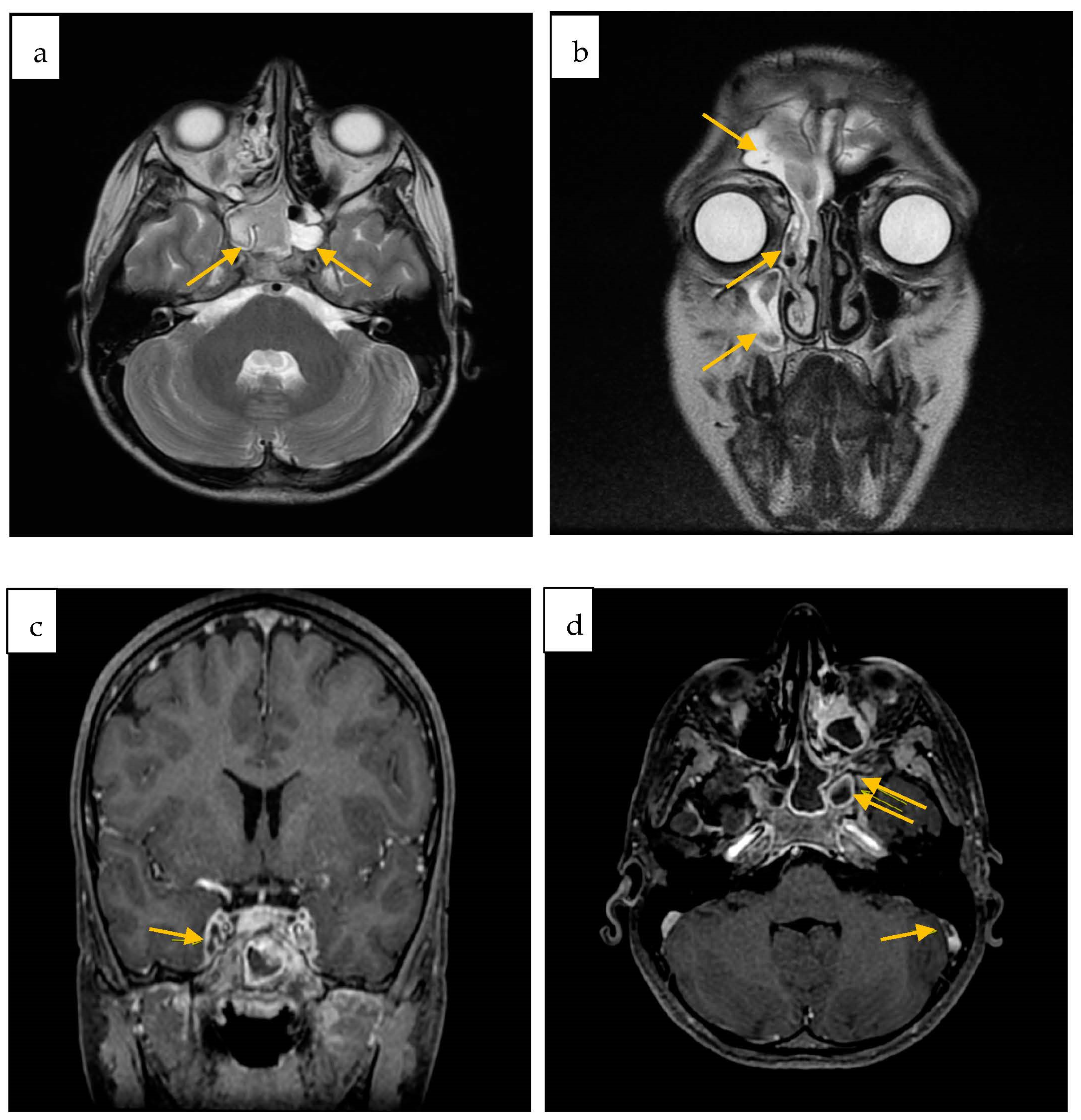
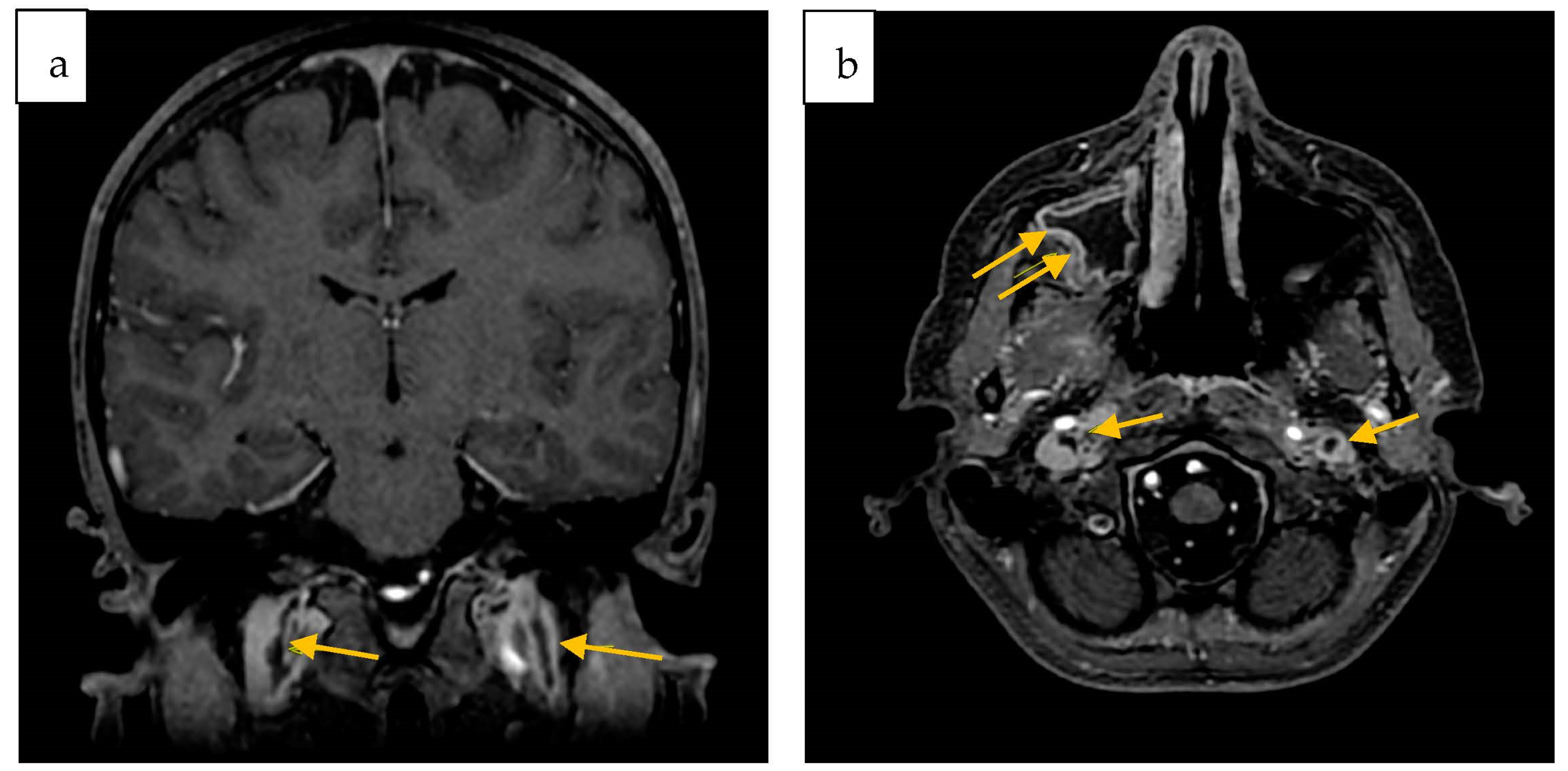
2. Case Report
3. Material and Methods
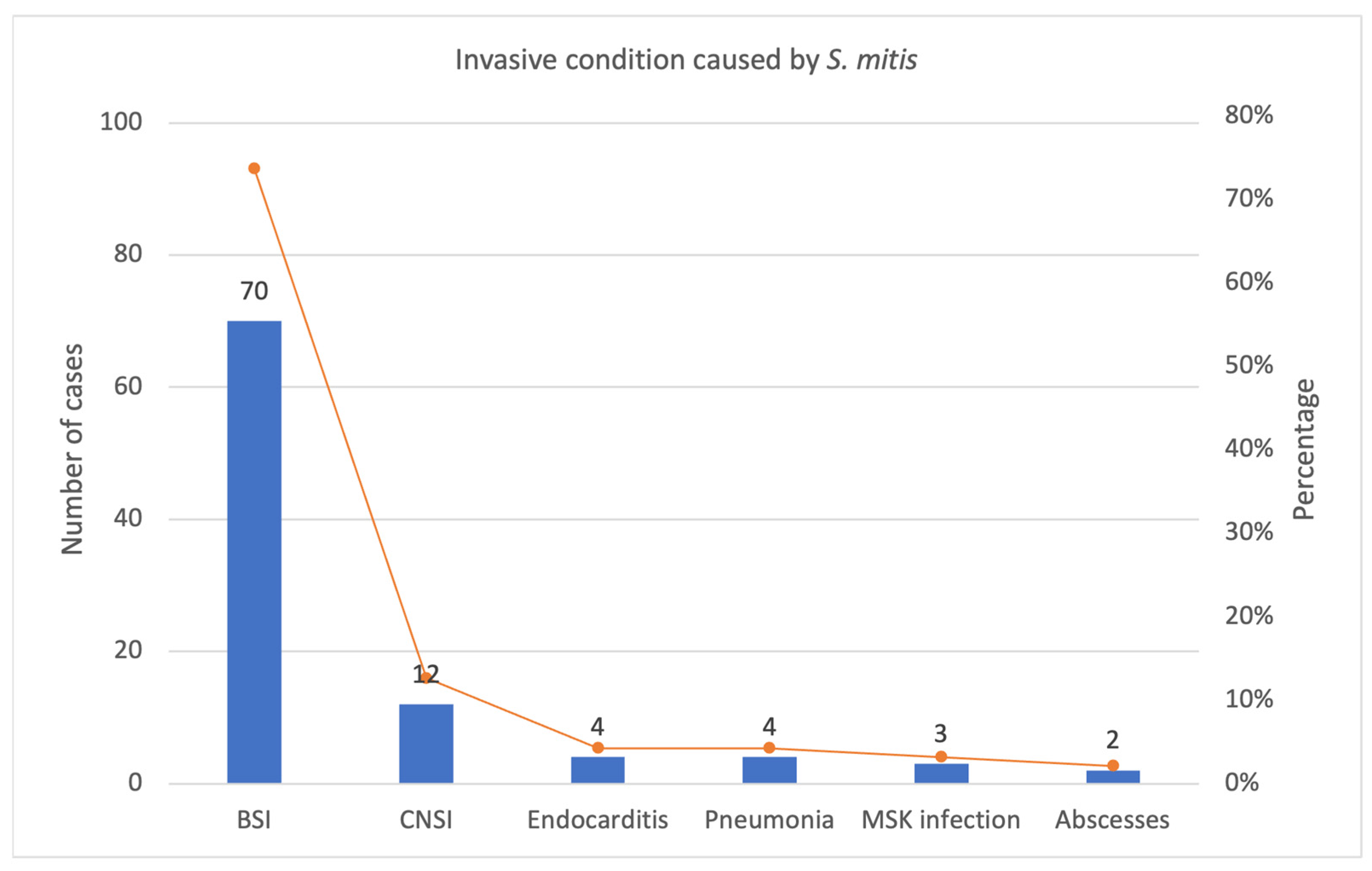
4. Results
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Facklam, R. What Happened to the Streptococci: Overview of Taxonomic and Nomenclature Changes. Clin. Microbiol. Rev. 2002, 15, 613–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yiş, R.; Yüksel, C.N.; Derundere, U.; Yiş, U. Önceden Sağlıklı Bir Çocukta Streptococcus mitis’e Bağlı Menenjit ve Beyaz Cevher Lezyonları “Meningitis and white matter lesions due to Streptococcus mitis in a previously healthy child”. Mikrobiyol. Bul. 2011, 45, 741–745. (In Turkish) [Google Scholar]
- Shelburne, S.A.; Sahasrabhojane, P.; Saldana, M.; Yao, H.; Su, X.; Horstmann, N.; Thompson, E.; Flores, A.R. Streptococcus mitis Strains Causing Severe Clinical Disease in Cancer Patients. Emerg. Infect. Dis. 2014, 20, 762–771. [Google Scholar] [CrossRef] [PubMed]
- Fukayama, H.; Shoji, K.; Yoshida, M.; Iijima, H.; Maekawa, T.; Ishiguro, A.; Miyairi, I. Bacterial meningitis due to the Streptococcus mitis group in children with cerebrospinal fluid leak. IDCases 2022, 27, e01406. [Google Scholar] [CrossRef] [PubMed]
- Jaing, T.-H.; Chiu, C.-H.; Hung, I.-J. Successful treatment of meningitis caused by highly-penicillin-resistant Streptococcus mitis in a leukemic child. Chang Gung Med. J. 2002, 25, 190–193. [Google Scholar] [PubMed]
- Balkundi, D.R.; Murray, D.L.; Patterson, M.J.; Gera, R.; Scott-Emuakpor, A.; Kulkarni, R. Penicillin-Resistant Streptococcus mitis as a Cause of Septicemia with Meningitis in Febrile Neutropenic Children. J. Pediatr. Hematol. 1997, 19, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ Clin. Res. Ed. 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basaranoglu, S.T.; Ozsurekci, Y.; Aykac, K.; Aycan, A.E.; Bıcakcigil, A.; Altun, B.; Sancak, B.; Cengiz, A.B.; Kara, A.; Ceyhan, M. Streptococcus mitis/oralis Causing Blood Stream Infections in Pediatric Patients. Jpn. J. Infect. Dis. 2019, 72, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Blázquez-Gamero, D.; Epalza, C.; Cadenas, J.A.A.; Gero, L.C.; Calvo, C.; Rodríguez-Molino, P.; Méndez, M.; Santos, M.D.M.; Fumadó, V.; Guzmán, M.F.; et al. Fever without source as the first manifestation of SARS-CoV-2 infection in infants less than 90 days old. Eur. J. Pediatr. 2021, 180, 2099–2106. [Google Scholar] [CrossRef]
- Nomura, R.; Nakano, K.; Mäkelä, K.; Vaara, M.; Salo, E.; Alaluusua, S.; Ooshima, T. Isolation and characterization of Streptococcus mitis from blood of child with osteomyelitis. Int. J. Paediatr. Dent. 2010, 21, 192–199. [Google Scholar] [CrossRef]
- Ahmed, R.; Hassall, T.; Morland, B.; Gray, J. Viridans streptococcus Bacteremia in Children on Chemotherapy for Cancer: An Underestimated Problem. Pediatr. Hematol. Oncol. 2003, 20, 439–444. [Google Scholar] [CrossRef]
- Buldu, M.T.; Raman, R. Hip adductor pyomyositis from Streptococcus mitis in a four-year-old child. J. Clin. Orthop. Trauma 2016, 7, 69–71. [Google Scholar] [CrossRef] [PubMed]
- Imhof, L.; Schrading, S.; Braunschweig, T.; Steinau, G.; Spillner, J.W.; Puzik, A.; Lassay, L.; Kontny, U. Abscessing Infection by Streptococcus mitis Mimicking Metastatic Lesions in a 5-Year-Old Girl with Nephroblastoma: A Case Report. J. Pediatr. Hematol. 2018, 40, e429–e431. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Nagao, Y.; Endo, H.; Yamane, I.; Hirata, M.; Hatakeyama, K. An intubated 7-month-old infant with a retropharyngeal abscess and multidrug-resistant Streptococcus mitis. Clin. Case Rep. 2019, 7, 2443–2448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rieske, K.; Handrick, W.; Spencker, F.-B.; Günther, E. Sepsis durch vergrünende Streptokokken bei Kindern mit malignen hämatologischen Erkrankungen. Klin. Padiatr. 1997, 209, 364–372. [Google Scholar] [CrossRef]
- Bignardi, G.E.; Isaacs, D. Neonatal Meningitis Due to Streptococcus mitis. Clin. Infect. Dis. 1989, 11, 86–88. [Google Scholar] [CrossRef]
- Tobias, J.D.; Bozeman, P.M.; Stokes, D.C. Postsepsis bradycardia in children with leukemia. Crit. Care Med. 1991, 19, 1172–1176. [Google Scholar] [CrossRef]
- Nielsen, M.J.; Claxton, S.; Pizer, B.; Lane, S.; Cooke, R.P.; Paulus, S.; Carrol, E.D. Viridans Group Streptococcal Infections in Children After Chemotherapy or Stem Cell Transplantation. Medicine 2016, 95, e2952. [Google Scholar] [CrossRef]
- Melendez, E.L.V.; Farrell, J.J.; Hujer, A.M.; Lowery, K.S.; Sampath, R.; A Bonomo, R. Culture negative empyema in a critically ill child: An opportunity for rapid molecular diagnostics. BMC Anesthesiol. 2014, 14, 107. [Google Scholar] [CrossRef] [Green Version]
- Taketani, T.; Kanai, R.; Fukuda, S.; Uchida, Y.; Yasuda, K.; Mishima, S.; Suyama, T.; Kodama, R.; Yoshino, I.; Kunishi, H.; et al. Pure Red Cell Precursor Toxicity by Linezolid in a Pediatric Case. J. Pediatr. Hematol. 2009, 31, 684–686. [Google Scholar] [CrossRef]
- Kennedy, M.J.; Jackson, M.A.; Kearns, G.L. Delayed diagnosis of penicillin-resistant Streptococcus mitis endocarditis following single-dose amoxicillin prophylaxis in a child. Clin. Pediatr. 2004, 43, 773–776. [Google Scholar] [CrossRef] [PubMed]
- Yiş, U.; Carman, K.B.; Yiş, R.; Derundere, U. Brain magnetic resonance imaging findings suggestive of widespread white matter involvement in children with Streptococcus mitis meningitis. Turk. J. Pediatr. 2013, 54, 425–428. [Google Scholar]
- Legendre, A.; Guérin, P.; Gournay, V.; Baron, O.; Leveiller, D.; Lefevre, M. Osler endocarditis of a ventricular septal defect in a 21-month old child. Arch. Mal. Coeur Vaiss. 2000, 93, 631–634. [Google Scholar]
- Goldfarb, J.; Wormser, G.P.; Glaser, J.H. Meningitis caused by multiply antibiotic-resistant viridans streptococci. J. Pediatr. 1984, 105, 891–895. [Google Scholar] [CrossRef]
- Hellwege, H.; Ram, W.; Scherf, H.; Fock, R. Neonatal Meningitis Caused by Streptococcus mitis. Lancet 1984, 323, 743–744. [Google Scholar] [CrossRef]
- Esposito, S.; Mayer, A.; Krzysztofiak, A.; Garazzino, S.; Lipreri, R.; Galli, L.; Osimani, P.; Fossali, E.; Di Gangi, M.; Lancella, L.; et al. Infective Endocarditis in Children in Italy from 2000 to 2015. Expert Rev. Anti-Infect. Ther. 2016, 14, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.; Scholz, C.B.; Kilian, M. Re-evaluation of the taxonomy of the Mitis group of the genus Streptococcus based on whole genome phylogenetic analyses, and proposed reclassification of Streptococcus dentisani as Streptococcus oralis subsp. dentisani comb. nov., Streptococcus tigurinus as Streptococcus oralis subsp. tigurinus comb. nov., and Streptococcus oligofermentans as a later synonym of Streptococcus cristatus. Int. J. Syst. Evol. Microbiol. 2016, 66, 4803–4820. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.A.; Garber, D.; Hu, S.; Kamat, A. Systematic review and case report: Intracranial complications of pediatric sinusitis. Int. J. Pediatr. Otorhinolaryngol. 2016, 86, 200–212. [Google Scholar] [CrossRef] [PubMed]
- Sadowy, E.; Hryniewicz, W. Identification of Streptococcus pneumoniae and other Mitis streptococci: Importance of molecular methods. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 2247–2256. [Google Scholar] [CrossRef]
- Tunkel, A.R.; Sepkowitz, K.A. Infections Caused by Viridans Streptococci in Patients with Neutropenia. Clin. Infect. Dis. 2002, 34, 1524–1529. [Google Scholar] [CrossRef]
- Mikulska, M.; Viscoli, C.; Orasch, C.; Livermore, D.M.; Averbuch, D.; Cordonnier, C.; Akova, M. Aetiology and resistance in bacteraemias among adult and paediatric haematology and cancer patients. J. Infect. 2013, 68, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J. Streptococcus mitis: Walking the line between commensalism and pathogenesis. Mol. Oral Microbiol. 2011, 26, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Chiang, A.D.; Sinaii, N.; Palmore, T.N. Risk Factors for Viridans Group Streptococcal Bacteremia in Neutropenic and Non-neutropenic Patients: A Single Center Case-Case-Control Study. Open Forum Infect. Dis. 2017, 5, ofx260. [Google Scholar] [CrossRef] [Green Version]
- Denapaite, D.; Brückner, R.; Nuhn, M.; Reichmann, P.; Henrich, B.; Maurer, P.; Schähle, Y.; Selbmann, P.; Zimmermann, W.; Wambutt, R.; et al. The Genome of Streptococcus mitis B6—What Is a Commensal? PLoS ONE 2010, 5, e9426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero, P.; Croucher, N.J.; Hiller, N.L.; Hu, F.Z.; Ehrlich, G.D.; Bentley, S.D.; García, E.; Mitchell, T.J. Comparative Genomic Analysis of Ten Streptococcus pneumoniae Temperate Bacteriophages. J. Bacteriol. 2009, 191, 4854–4862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mundy, L.S.; Janoff, E.N.; Schwebke, K.E.; Shanholtzer, C.J.; Willard, K.E. Ambiguity in the Identification of Streptococcus pneumoniae Optochin, Bile Solubility, Quellung, and the AccuProbe DNA Probe Tests. Am. J. Clin. Pathol. 1998, 109, 55–61. [Google Scholar] [CrossRef]
- Arbique, J.C.; Poyart, C.; Trieu-Cuot, P.; Quesne, G.; Carvalho, M.d.G.S.; Steigerwalt, A.G.; Morey, R.E.; Jackson, D.; Davidson, R.J.; Facklam, R.R. Accuracy of Phenotypic and Genotypic Testing for Identification of Streptococcus pneumoniae and Description of Streptococcus pseudopneumoniae sp. nov. J. Clin. Microbiol. 2004, 42, 4686–4696. [Google Scholar] [CrossRef] [Green Version]
- Balsalobre, L.; Hernández-Madrid, A.; Llull, D.; Martín-Galiano, A.J.; García, E.; Fenoll, A.; de la Campa, A.G. Molecular Characterization of Disease-Associated Streptococci of the Mitis Group That Are Optochin Susceptible. J. Clin. Microbiol. 2006, 44, 4163–4171. [Google Scholar] [CrossRef] [Green Version]
- Ikryannikova, L.; Lapin, K.; Malakhova, M.; Filimonova, A.; Ilina, E.; Dubovickaya, V.; Sidorenko, S.; Govorun, V. Misidentification of alpha-hemolytic streptococci by routine tests in clinical practice. Infect. Genet. Evol. 2011, 11, 1709–1715. [Google Scholar] [CrossRef]
- Rolo, D.; Simões, S.A.; Domenech, A.; Fenoll, A.; Liñares, J.; de Lencastre, H.; Ardanuy, C.; Sá-Leão, R. Disease isolates of Streptococcus pseudopneumoniae and non-typeable S. pneumoniae presumptively identified as atypical S. pneumoniae in Spain. PLoS ONE 2013, 8, e57047. [Google Scholar] [CrossRef] [Green Version]
- Simões, A.S.; Tavares, D.A.; Rolo, D.; Ardanuy, C.; Goossens, H.; Henriques-Normark, B.; Linares, J.; de Lencastre, H.; Sá-Leão, R. lytA-based identification methods can misidentify Streptococcus pneumoniae. Diagn. Microbiol. Infect. Dis. 2016, 85, 141–148. [Google Scholar] [CrossRef]
- Sadowy, E.; Bojarska, A.; Kuch, A.; Skoczyńska, A.; Jolley, K.A.; Maiden, M.C.J.; van Tonder, A.J.; Hammerschmidt, S.; Hryniewicz, W. Relationships among streptococci from the mitis group, misidentified as Streptococcus pneumoniae. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1865–1878. [Google Scholar] [CrossRef] [PubMed]
- Sanguinetti, L.; Toti, S.; Reguzzi, V.; Bagnoli, F.; Donati, C. A Novel Computational Method Identifies Intra- and Inter-Species Recombination Events in Staphylococcus aureus and Streptococcus pneumoniae. PLoS Comput. Biol. 2012, 8, e1002668. [Google Scholar] [CrossRef] [PubMed]
- Hakenbeck, R.; Madhour, A.; Denapaite, D.; Brückner, R. Versatility of choline metabolism and choline-binding proteins in Streptococcus pneumoniae and commensal streptococci. FEMS Microbiol. Rev. 2009, 33, 572–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jefferies, J.; Nieminen, L.; Kirkham, L.-A.; Johnston, C.; Smith, A.; Mitchell, T.J. Identification of a Secreted Cholesterol-Dependent Cytolysin (Mitilysin) from Streptococcus mitis. J. Bacteriol. 2007, 189, 627–632. [Google Scholar] [CrossRef] [Green Version]
- Llull, D.; López, R.; García, E. Characteristic Signatures of the lytA Gene Provide a Basis for Rapid and Reliable Diagnosis of Streptococcus pneumoniae Infections. J. Clin. Microbiol. 2006, 44, 1250–1256. [Google Scholar] [CrossRef] [Green Version]
- Muzzi, A.; Donati, C. Population genetics and evolution of the pan-genome of Streptococcus pneumoniae. Int. J. Med. Microbiol. 2011, 301, 619–622. [Google Scholar] [CrossRef]
- Donati, C.; Hiller, N.L.; Tettelin, H.; Muzzi, A.; Croucher, N.J.; Angiuoli, S.V.; Oggioni, M.; Hotopp, J.C.D.; Hu, F.Z.; Riley, D.R.; et al. Structure and dynamics of the pan-genome of Streptococcus pneumoniae and closely related species. Genome Biol. 2010, 11, R107. [Google Scholar] [CrossRef] [Green Version]
- Tavares, D.A.; Handem, S.; Carvalho, R.J.; Paulo, A.C.; de Lencastre, H.; Hinds, J.; Sá-Leão, R. Identification of Streptococcus pneumoniae by a real-time PCR assay targeting SP2020. Sci. Rep. 2019, 9, 3285. [Google Scholar] [CrossRef] [Green Version]
- AlEraky, D.M.; Madi, M.; El Tantawi, M.; AlHumaid, J.; Fita, S.; AbdulAzeez, S.; Borgio, J.F.; Al-Harbi, F.A.; Alagl, A.S. Predominance of non-Streptococcus mutans bacteria in dental biofilm and its relation to caries progression. Saudi J. Biol. Sci. 2021, 28, 7390–7395. [Google Scholar] [CrossRef]
- Neves, B.G.; Stipp, R.N.; Bezerra, D.D.S.; Guedes, S.F.D.F.; Rodrigues, L.K.A. Quantitative analysis of biofilm bacteria according to different stages of early childhood caries. Arch. Oral Biol. 2018, 96, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, T.J. The pathogenesis of streptococcal infections: From Tooth decay to meningitis. Nat. Rev. Genet. 2003, 1, 219–230. [Google Scholar] [CrossRef]
- Amat, F. Complications des sinusites bactériennes du grand enfant. À propos d’un cas et revue de la littérature. Arch. Pédiatrie 2010, 17, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, A.; Patadia, M.; Stankiewicz, J. Neurological Complications of Acute and Chronic Sinusitis. Curr. Neurol. Neurosci. Rep. 2018, 18, 5. [Google Scholar] [CrossRef] [PubMed]
- Nicoli, T.K.; Oinas, M.; Niemelä, M.; Mäkitie, A.A.; Atula, T. Intracranial Suppurative Complications of Sinusitis. Scand. J. Surg. 2016, 105, 254–262. [Google Scholar] [CrossRef]
- Kombogiorgas, D.; Seth, R.; Athwal, R.; Modha, J.; Singh, J. Suppurative intracranial complications of sinusitis in adolescence. Single institute experience and review of literature. Br. J. Neurosurg. 2007, 21, 603–609. [Google Scholar] [CrossRef]
- Gilony, D.; Talmi, Y.P.; Bedrin, L.; Ben-Shosan, Y.; Kronenberg, J. The clinical behavior of isolated sphenoid sinusitis. Otolaryngol. Neck Surg. 2007, 136, 610–615. [Google Scholar] [CrossRef]
- Sobol, S.E.; Marchand, J.; Tewfik, T.L.; Manoukian, J.J.; Schloss, M.D. Orbital Complications of Sinusitis in Children. J. Otolaryngol. 2002, 31, 131–136. [Google Scholar] [CrossRef]
- Leung, A.K.; Kellner, J.D. Acute sinusitis in children: Diagnosis and management. J. Pediatr. Health Care 2004, 18, 72–76. [Google Scholar] [CrossRef]
- Blackmore, T.K.; Morley, H.I.; Gordon, D.L. Streptococcus mitis-induced Bacteremia and Meningitis after Spinal Anesthesia. Anesthesiology 1993, 78, 592–593. [Google Scholar] [CrossRef]
- Kilpatrick, M.E.; Girgis, N.I. Meningitis—A complication of spinal anesthesia. Anesth. Analg. 1983, 62, 513–515. [Google Scholar] [CrossRef]
- Villevieille, T.; Vincenti-Rouquette, I.; Petitjeans, F.; Koulmann, P.; Legulluche, Y.; Rousseau, J.-M.; Diraison, Y.; Brinquin, L. Streptococcus mitis-induced Meningitis After Spinal Anesthesia. Anesth. Analg. 2000, 90, 500. [Google Scholar] [CrossRef] [PubMed]
- Selvitop, O.; Poretti, A.; Huisman, T.A.; Wagner, M.W. Cerebral sinovenous thrombosis in a child with Crohn’s disease, otitis media, and meningitis. Neuroradiol. J. 2015, 28, 274–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bracken, J.; Barnacle, A.; Ditchfield, M. Potential pitfalls in imaging of paediatric cerebral sinovenous thrombosis. Pediatr. Radiol. 2012, 43, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Tuomanen, E.I. Molecular and Cellular Mechanisms of Pneumococcal Meningitis. Ann. N. Y. Acad. Sci. 1996, 797, 42–52. [Google Scholar] [CrossRef]
- Agrawal, S.; Nadel, S. Acute Bacterial Meningitis in Infants and Children. Pediatr. Drugs 2011, 13, 385–400. [Google Scholar] [CrossRef]
- Visintin, C.; Mugglestone, M.A.; Fields, E.J.; Jacklin, P.; Murphy, M.S.; Pollard, A.J.; on behalf of the Guideline Development Group. Management of bacterial meningitis and meningococcal septicaemia in children and young people: Summary of NICE guidance. BMJ 2010, 340, c3209. [Google Scholar] [CrossRef]
- Bruckner, L.B.; Korones, D.N.; Karnauchow, T.; Hardy, D.J.; Gigliotti, F. High incidence of penicillin resistance among α-hemolytic streptococci isolated from the blood of children with cancer. J. Pediatr. 2002, 140, 20–26. [Google Scholar] [CrossRef]
- Davidovich, N.V.; Galieva, A.S.; Davydova, N.G.; Malygina, O.G.; Kukalevskaya, N.N.; Simonova, G.V.; Bazhukova, T.A. Spectrum and resistance determinants of oral streptococci clinical isolates. Russ. Clin. Lab. Diagn. 2020, 65, 632–637. [Google Scholar] [CrossRef]
- Wald, E.R.; Applegate, K.E.; Bordley, C.; Darrow, D.H.; Glode, M.P.; Marcy, S.M.; Nelson, C.E.; Rosenfeld, R.M.; Shaikh, N.; Smith, M.J.; et al. Clinical Practice Guideline for the Diagnosis and Management of Acute Bacterial Sinusitis in Children Aged 1 to 18 Years. Pediatrics 2013, 132, e262–e280. [Google Scholar] [CrossRef] [Green Version]
- Wilson, W.R.; Taubert, K.A.; Gewitz, M.H.; Lockhart, P.B.; Baddour, L.M.; E Levison, M.; Bolger, A.F.; Cabell, C.H.; Takahashi, M.; Baltimore, R.S.; et al. Prevention of Infective Endocarditis. Circulation 2007, 116, 1736–1754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Júnior, A.G.A.; Costa, M.L.V.A.; Silva, F.R.P.; Arcanjo, D.D.R.; Moura, L.F.A.D.; Oliveira, F.A.A.; Soares, M.J.S.; Quelemes, P.V. Amoxicillin-Resistant Streptococci Carriage in the Mouths of Children: A Systematic Review and Meta-Analysis. Pathogens 2022, 11, 1114. [Google Scholar] [CrossRef] [PubMed]
- Moreillon, P.; Que, Y.A.; Bayer, A.S. Pathogenesis of streptococcal and staphylococcal endocarditis. Infect. Dis. Clin. N. Am. 2002, 16, 297–318. [Google Scholar] [CrossRef] [PubMed]
- Hakenbeck, R.; Balmelle, N.; Weber, B.; Gardès, C.; Keck, W.; de Saizieu, A. Mosaic Genes and Mosaic Chromosomes: Intra- and Interspecies Genomic Variation of Streptococcus pneumoniae. Infect. Immun. 2001, 69, 2477–2486. [Google Scholar] [CrossRef] [Green Version]
- Hannan, S.; Ready, D.; Jasni, A.S.; Rogers, M.; Pratten, J.; Roberts, A.P. Transfer of antibiotic resistance by transformation with eDNA within oral biofilms. FEMS Immunol. Med. Microbiol. 2010, 59, 345–349. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Results | Measuring Unit | Reference Values | |
|---|---|---|---|
| WBC | 12.8 | 103/uL | 4.00–10.00 |
| Neutrophils | 11.6 | 103/uL | 2.70–6.70 |
| Lymphocytes | 0.50 | 103/uL | 1.00–2.20 |
| RBC | 4.1 | 106/uL | 3.74–4.92 |
| Hemoglobin | 10.8 | g/dL | 11.0–14.3 |
| Platelet count | 255 | 103/uL | 180.0–299.0 |
| C-reactive protein | 16.86 | mg/dL | <0.5 |
| Author/Country/ Year [Ref.] | Age | Sex | Pre-Existing Disease | Risk Factors | S. mitis Isolation Sample | Medical Condition | Therapy | Outcome |
|---|---|---|---|---|---|---|---|---|
| Goldfarb et al./ USA/1984 [24] | 9 d | M | Hydrocephalus | ventriculoperitoneal shunt | CSF | meningitis | nafcillin + ampicillin + gentamicin → vancomycin | healed |
| 2 y | F | AML | CVC | CSF | meningitis | Penicillin + gentamicin → ampicillin | healed | |
| Hellwege et al./ Germany/1984 [25] | 2 d | F | No | No | CSF | meningitis | ampicillin + gentamicin → penicillina G | healed |
| Bignardi et al./ UK/1989 [16] | 2 d | F | No | No | CSF | meningitis | penicillin G + netilmicin → penicillin G | healed |
| Tobias et al./ USA/1991 [17] | 5 y | M | AML | CVC | blood culture | sepsis | vancomycin + amikacin + ticarcillin | healed |
| 6 y | M | AML | CVC | blood culture | sepsis | vancomycin + amikacin + ceftazidime | healed | |
| 10 y | F | AML | CVC | blood culture | sepsis | vancomycin + amikacin + ceftazidime | healed | |
| 1 y | F | AML | CVC | blood culture | sepsis | vancomycin + ceftazidime | healed | |
| Balkundi et al./ USA/1997 [6] | 7 y | F | Burkitt lymphoma | CVC | NR | meningitis | tobramycin + nafcillin + ticarcillin → vancomycin | healed |
| 6 y | F | ALL | CVC | NR | meningitis | vancomycin + ceftazidime → intraventricular vancomycin | died | |
| 9 y | M | ALL | CVC | NR | meningitis | vancomycin + ceftazidime → vancomycin | healed | |
| Rieske et al./ Germania/1997 [15] | 15 y | M | ALL | CVC | blood culture | bacteremia | erythromycin → ampicillin | healed |
| 8 y | F | ALL | CVC | blood culture | pneumonia | cefotaxime + gentamicin → azlocillin | healed | |
| 6 m | M | AML | CVC | blood culture | pneumonia | imipenem + vancomycin | healed | |
| 4 y | M | AML | CVC | blood culture | septic shock | cefotaxime + gentamicin + vancomycin | died | |
| 6 y | F | AML | CVC | blood culture | otomastoiditis | ceftazidime + gentamicin + ampicillin | healed | |
| 10 y | M | AML | CVC | blood culture | pneumonia | azlocillin + ceftazidime + gentamicin | healed | |
| 15 y | M | AML | CVC | blood culture | sepsis | piperacillina + ceftazidime + gentamicina | died | |
| 10 y | F | AML | CVC | blood culture | NR | ceftazidime + gentamicin → piperacillin | healed | |
| 6 m | M | Osteopetrosis | CVC | blood culture | bacteremia | NR | healed | |
| Legendre et al./ France/2000 [23] | 1 y | F | No | ventricular septal defect | NR | endocarditis | NR | healed |
| Jaing et al./ Japan/2002 [5] | 6 y | M | ANLL | CVC | blood culture and CSF | meningitis | vancomycin + ceftriaxone | healed |
| Ahmed et al./ UK/2003 [11] | 6.6 y * | 13 M, 9 F | Oncological disease | CVC | blood culture | sepsis | NR | 21 healed 1 died |
| Kennedy et al./ USA/2004 [21] | 8 y | F | No | ventricular septal defect | blood culture | endocarditis | vancomycin + ceftriaxone + gentamicin | healed |
| Taketani et al./ Japan/2009 [20] | 2 y | M | No | No | blood culture | endocarditis | ampicillin/sulbactam + meropenem → vancomycin + gentamicin + rifampicin → linezolid | healed |
| Nomura et al./ Finland/2011 [10] | 7 y | F | No | No | blood culture | osteomyelitis | clindamycin | healed |
| Yiş R et al./ Turkey/2011 [2] | 8y | F | No | No | CSF | meningitis | ceftriaxone | healed |
| Yiş U et al./ Turkey/2012 [22] | 6 y | M | No | No | CSF | sinusitis meningitis | ceftriaxone + vancomycin | healed |
| Vazquez Melendez et al./ USA/2014 [19] | 2 y | F | No | No | pleural fluid | pneumonia | clindamycin + ceftriaxone → amoxicillin/clavulanate | healed |
| Nielsen et al./ UK/2015 [18] | 9 y * | 28 NR | hematological diseases | CVC | blood culture | sepsis | NR | 28 healed |
| 2 y | NR | Medulloblastoma | CVC | blood culture | septic shock | ceftazidime + amikacin → teicoplanin | healed | |
| 11 y | NR | ALL | CVC | blood culture | septic shock | ceftazidime + amikacin + teicoplanin | healed | |
| 17 y | NR | ALL | CVC | blood culture | septic shock | piperacillin/tazobactam + gentamicin → teicoplanin | died | |
| 16 y | NR | aplastic anemia | CVC | blood culture | septic shock | piperacillin/tazobactam + teicoplanin | died | |
| 18 y | NR | ALL | CVC | blood culture | septic shock | piperacillin/tazobactam + gentamicin → teicoplanin | died | |
| 7 y | NR | ALL | CVC | blood culture | septic shock | piperacillin/tazobactam + gentamicin → teicoplanin | healed | |
| Esposito et al./ Italy/2015 [26] | 9.5 y * | 5 NR | heart disease | heart disease | blood culture | endocarditis | NR | healed |
| Buldu et al./ UK/2016 [12] | 4 y | M | No | No | blood culture | pyomyositis of the hip | benzylpenicillin → phenoxymethylpenicillin | healed |
| Basaranoglu et al./ Japan/2018 [8] | 9 y | M | AML | CVC | blood culture | bacteremia | NR | healed |
| 2 y | M | AML | CVC | blood culture | bacteremia | NR | healed | |
| 13 y | M | AML | CVC | blood culture | bacteremia | NR | healed | |
| 6 m | M | Osteopetrosis | CVC | blood culture | bacteremia | NR | healed | |
| Imhof et al./ Germany/2018 [13] | 5 y | F | metastatic nephroblastoma | CVC | biopsy sample | liver and lung abscess | cefuroxime | healed |
| Watanabe et al./ Japan/2019 [14] | 7 m | F | No | No | drainage material | retropharyngeal abscess | meropenem | healed |
| Blázquez-Gamero et al./ Spain/2021 [9] | 3 m | M | Swachman-Diamond Syndrome, COVID-19 | No | blood culture | bacteremia | NR | healed |
| Fukayama et al./ Japan/2021 [4] | 14 y | F | Gorham-Stout syndrome | skull base osteolysis and CSF leak | CSF | meningitis | penicillin G | healed |
| Colomba C. et al./Italy/2023 | 12 y | M | No | No | sinus drainage material | sinusitis, meningitis, CSVT | ceftriaxone + vancomycin + metronidazole → cefotaxime | healed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colomba, C.; Garbo, V.; Boncori, G.; Albano, C.; Bagarello, S.; Condemi, A.; Giordano, S.; Canduscio, L.A.; Gallo, C.; Parrinello, G.; et al. Streptococcus mitis as a New Emerging Pathogen in Pediatric Age: Case Report and Systematic Review. Antibiotics 2023, 12, 1222. https://doi.org/10.3390/antibiotics12071222
Colomba C, Garbo V, Boncori G, Albano C, Bagarello S, Condemi A, Giordano S, Canduscio LA, Gallo C, Parrinello G, et al. Streptococcus mitis as a New Emerging Pathogen in Pediatric Age: Case Report and Systematic Review. Antibiotics. 2023; 12(7):1222. https://doi.org/10.3390/antibiotics12071222
Chicago/Turabian StyleColomba, Claudia, Valeria Garbo, Giovanni Boncori, Chiara Albano, Sara Bagarello, Anna Condemi, Salvatore Giordano, Laura A. Canduscio, Cristina Gallo, Gaspare Parrinello, and et al. 2023. "Streptococcus mitis as a New Emerging Pathogen in Pediatric Age: Case Report and Systematic Review" Antibiotics 12, no. 7: 1222. https://doi.org/10.3390/antibiotics12071222