
Fosfomycin: Pharmacological, Clinical and Future Perspectives

 ,
,  and
and
Abstract
:1. Introduction
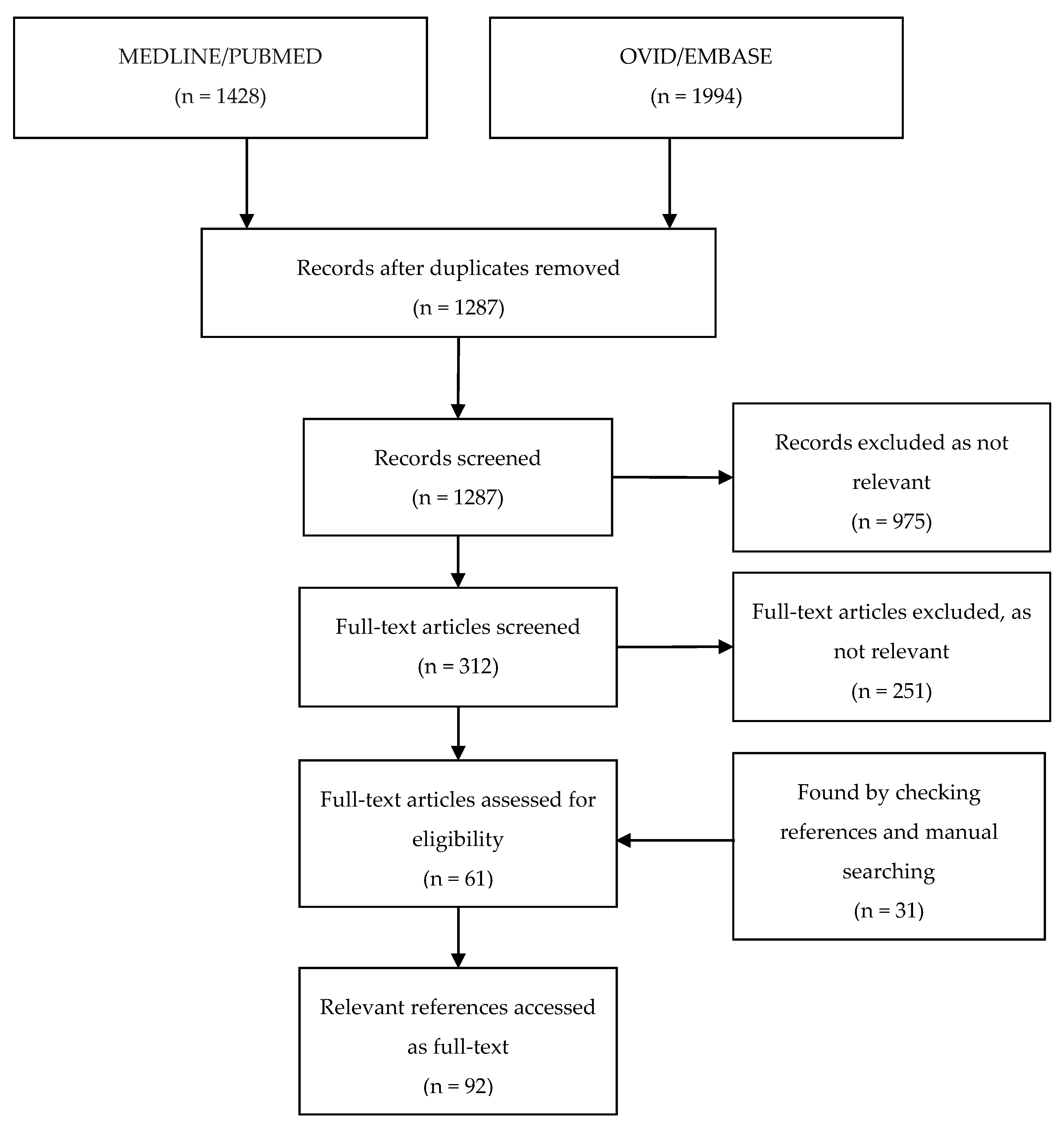
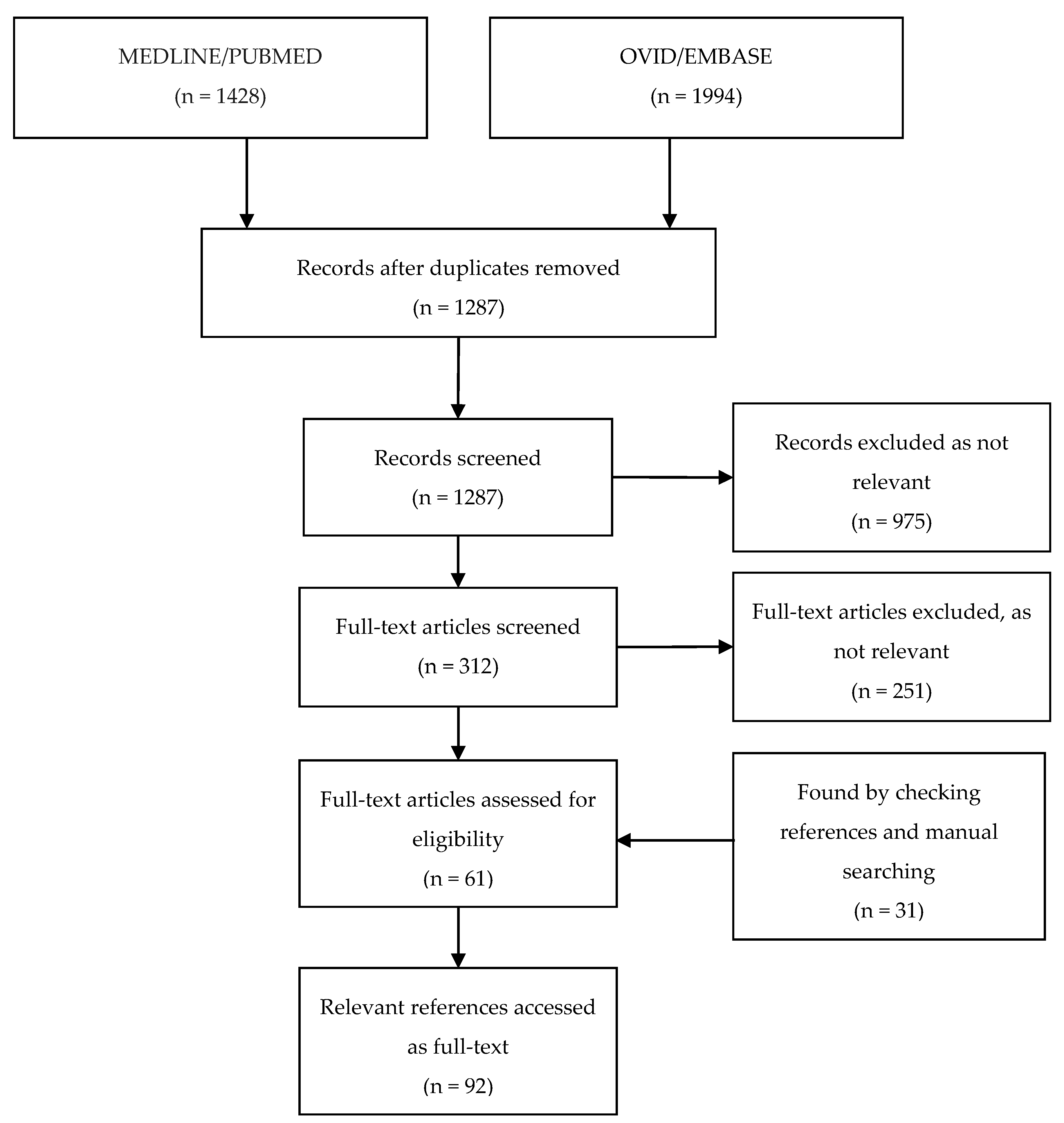
2. Methods
2.1. Systematic Search Strategy
2.2. PUBMED/MEDLINE
2.3. OVID/EMBASE
3. Results
4. Pharmacology of Fosfomycin for Treating MDR Bacteria
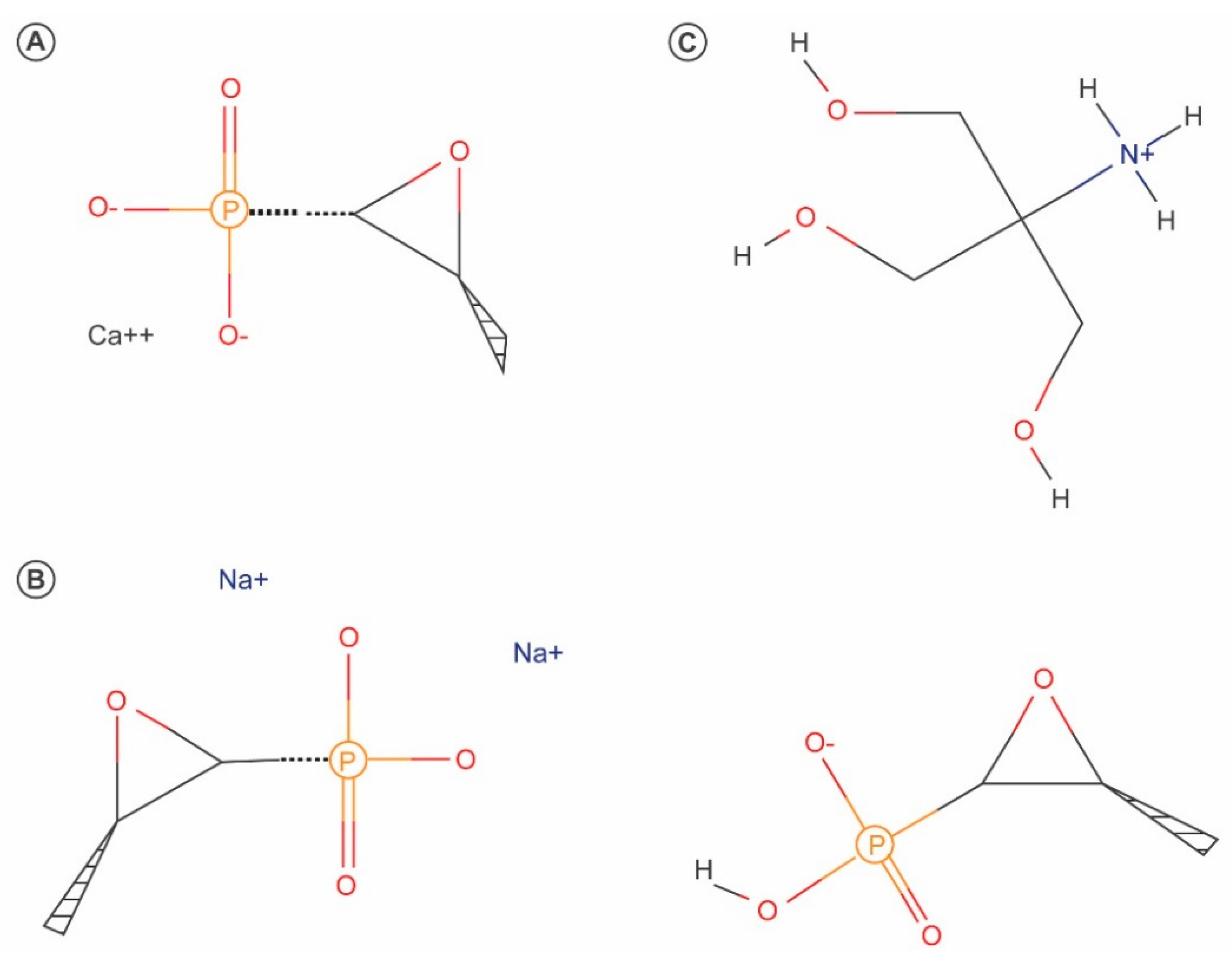
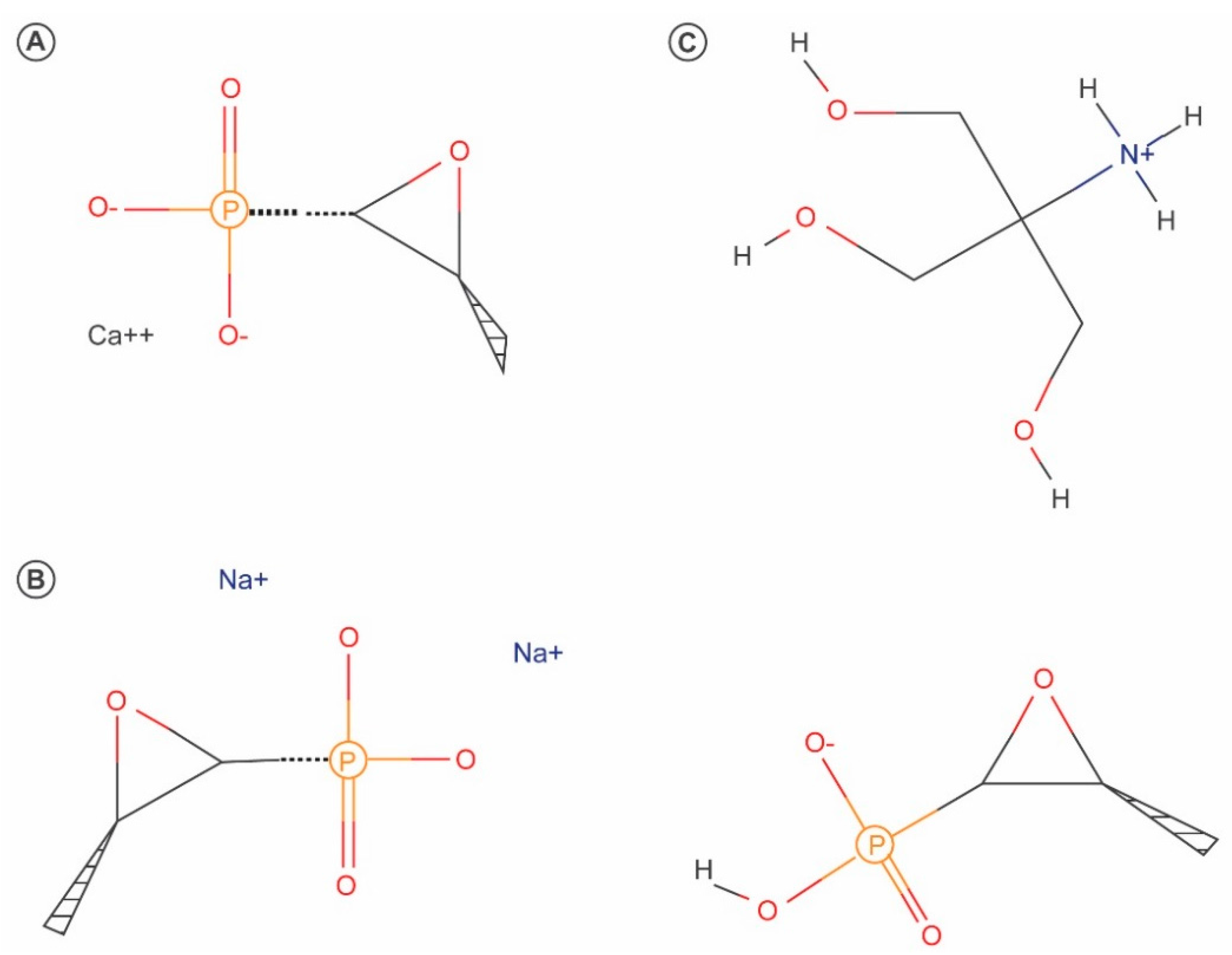
4.1. Chemistry
4.2. Pharmacokinetics of Fosfomycin
4.2.1. Absorption
4.2.2. Distribution and Tissue Penetration
4.2.3. Metabolism and Excretion
4.3. Pharmacodynamics of Fosfomycin
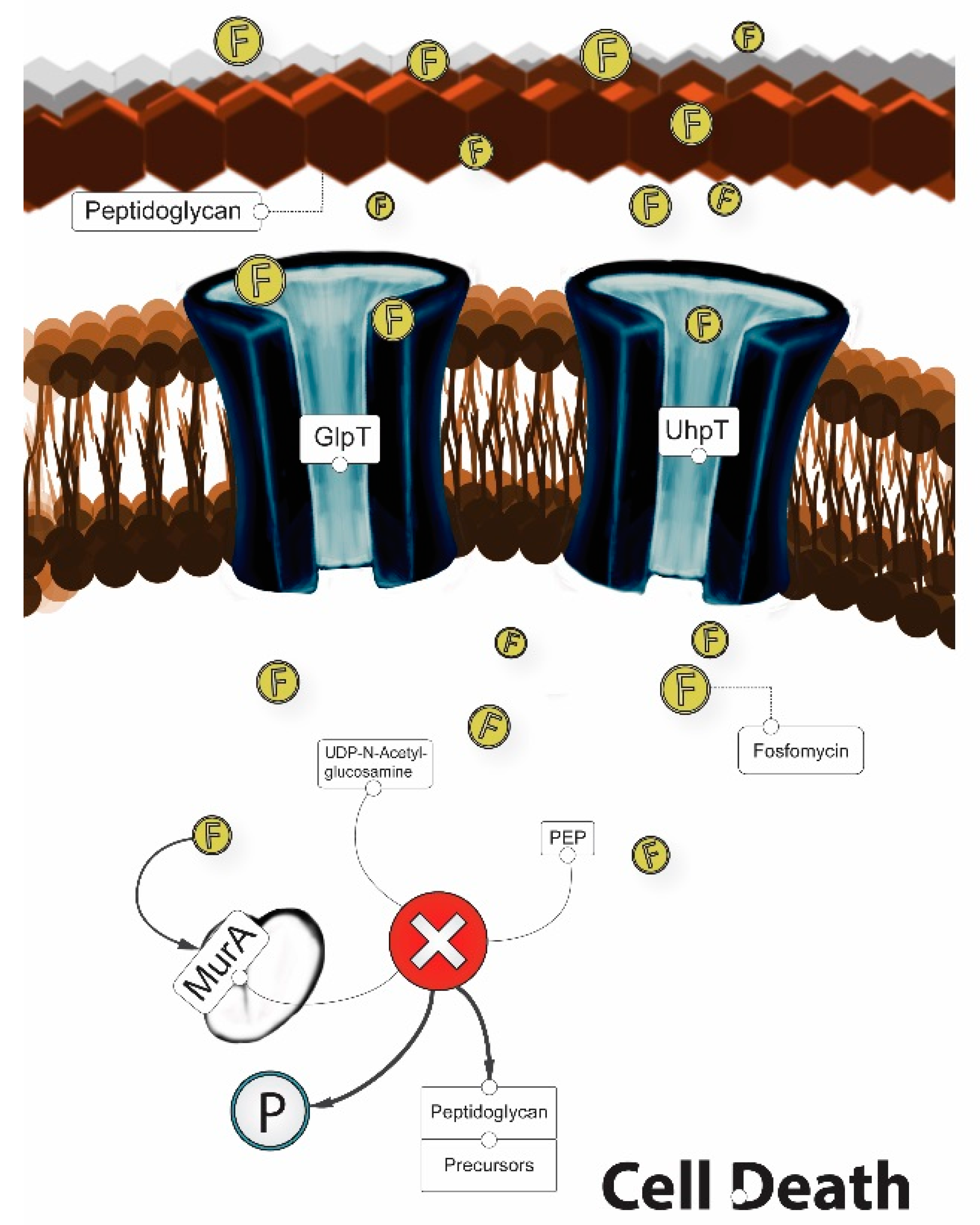
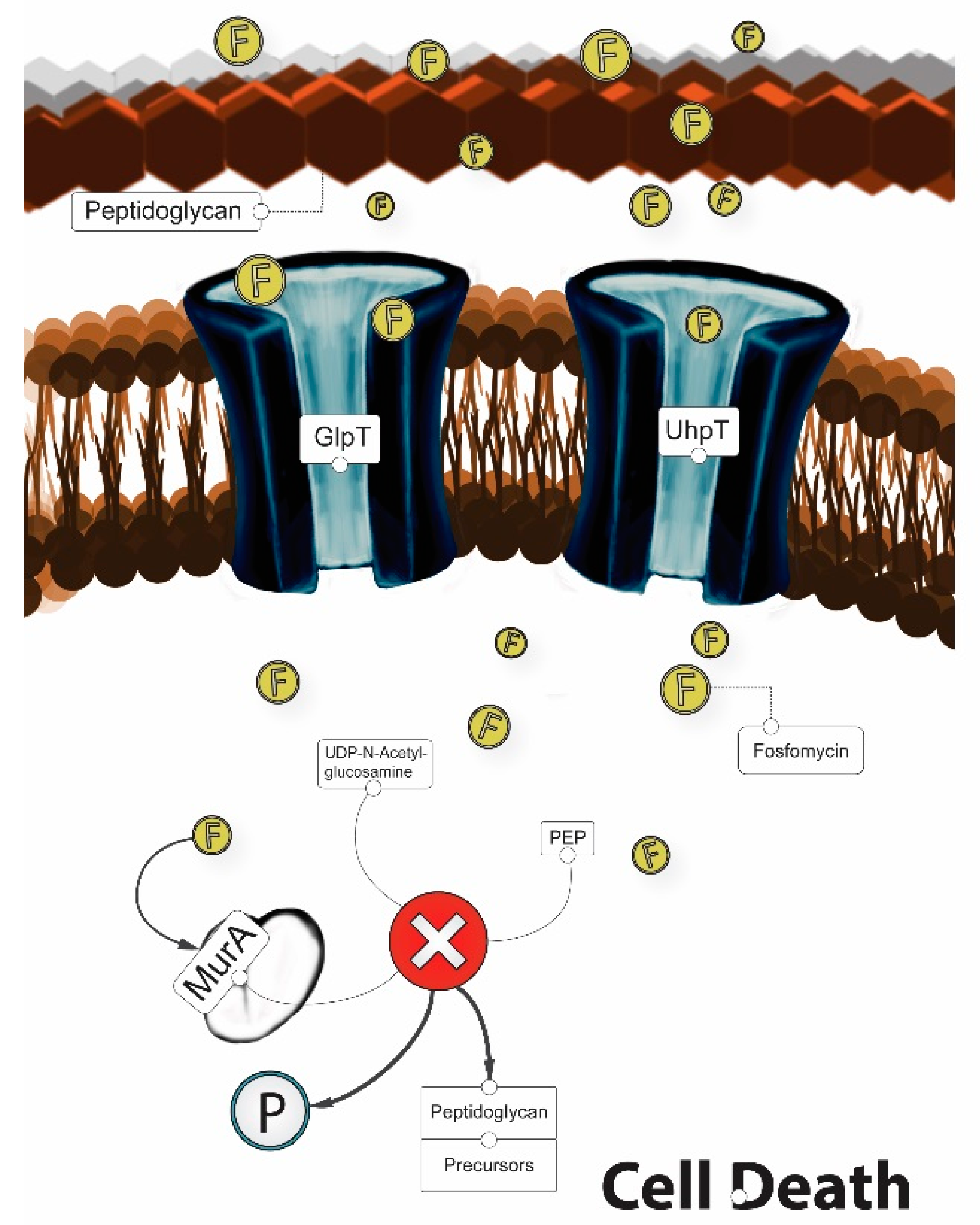
4.3.1. Mechanism of Action
4.3.2. Antibacterial Activity
5. Fosfomycin Resistance
5.1. In Vitro Synergy between Fosfomycin and Other Antibiotics
5.2. Properties of Fosfomycin
5.3. PK/PD Properties
5.4. Current Clinical Indications for Fosfomycin and Potential Future Applications
5.4.1. Intravenous Administration
5.4.2. Oral Administration
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Rice, L.B. Federal funding for the study of antimicrobial resistance in nosocomial pathogens: No ESKAPE. J. Infect. Dis. 2008, 197, 1079–1081. [Google Scholar] [CrossRef] [PubMed]
- Spellberg, B.; Guidos, R.; Gilbert, D.; Bradley, J.; Boucher, H.W.; Scheld, W.M.; Bartlett, J.G.; Edwards, J., Jr.; The Infectious Diseases Society of America. The epidemic of antibiotic-resistant infections: A call to action for the medical community from the Infectious Diseases Society of America. Clin. Infect. Dis. 2008, 46, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Alanis, A.J. Resistance to Antibiotics: Are We in the Post-Antibiotic Era? Arch. Med. Res. 2005, 36, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.M.; Wertheim, H.F.L.; Sumpradit, N.; Vlieghe, E.; Hara, G.L.; Gould, I.M.; Goossens, H.; et al. Antibiotic resistance—The need for global solutions. Lancet Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef]
- World Health Organization. Antimicrobial Resistance: Global Report on Surveillance 2014; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Boucher, H.W.; Talbot, G.H.; Bradley, J.S.; Edwards, J.E.; Gilbert, D.; Rice, L.B.; Scheld, M.; Spellberg, B.; Bartlett, J. Bad bugs, no drugs: No ESKAPE! An update from the Infectious Diseases Society of America. Clin. Infect. Dis. 2009, 48, 1–12. [Google Scholar] [CrossRef] [PubMed]
- ECDC; EMEA. The Bacterial Challenge: Time to React. Joint Technical Report; European Centre for Disease Prevention and Control: Stockholm, Sweden; European Medicines Agency: London, UK, 2009. [Google Scholar]
- Freire-Moran, L.; Aronsson, B.; Manz, C.; Gyssens, I.C.; So, A.D.; Monnet, D.L.; Cars, O.; the ECDC-EMA Working Group. Critical shortage of new antibiotics in development against multidrug-resistant bacteria—Time to react is now. Drug Resist. Updates 2011, 14, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Bergen, P.J.; Landersdorfer, C.B.; Lee, H.J.; Li, J.; Nation, R.L. “Old” antibiotics for emerging multidrug-resistant bacteria. Curr. Opin. Infect. Dis. 2012, 25, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Bush, K.; Courvalin, P.; Dantas, G.; Davies, J.; Eisenstein, B.; Huovinen, P.; Jacoby, G.A.; Kishony, R.; Kreiswirth, B.N.; Kutter, E.; et al. Tackling antibiotic resistance. Nat. Rev. Microbiol. 2011, 9, 894–896. [Google Scholar] [CrossRef] [PubMed]
- Mouton, J.W.; Ambrose, P.G.; Canton, R.; Drusano, G.L.; Harbarth, S.; MacGowan, A.; Theuretzbacher, U.; Turnidge, J. Conserving antibiotics for the future: New ways to use old and new drugs from a pharmacokinetic and pharmacodynamic perspective. Drug Resist. Updates 2011, 14, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Giannopoulou, K.P.; Kokolakis, G.N.; Rafailidis, P.I. Fosfomycin: Use beyond urinary tract and gastrointestinal infections. Clin. Infect. Dis. 2008, 46, 1069–1077. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Kastoris, A.C.; Karageorgopoulos, D.E.; Rafailidis, P.I. Fosfomycin for the treatment of infections caused by multidrug-resistant non-fermenting Gram-negative bacilli: A systematic review of microbiological, animal and clinical studies. Int. J. Antimicrob. Agents 2009, 34, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Kanellopoulou, M.D.; Karageorgopoulos, D.E.; Dimopoulos, G.; Rafailidis, P.I.; Skarmoutsou, N.D.; Papafrangas, E.A. Antimicrobial susceptibility of multidrug-resistant Gram negative bacteria to fosfomycin. Eur. J. Clin. Microbiol. Infect. Dis. 2008, 27, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Maraki, S.; Karageorgopoulos, D.E.; Kastoris, A.C.; Mavromanolakis, E.; Samonis, G. Antimicrobial susceptibility of multidrug-resistant (MDR) and extensively drug-resistant (XDR) Enterobacteriaceae isolates to fosfomycin. Int. J. Antimicrob. Agents 2010, 35, 240–243. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Kastoris, A.C.; Kapaskelis, A.M.; Karageorgopoulos, D.E. Fosfomycin for the treatment of multidrug-resistant, including extended-spectrum b-lactamase producing, Enterobacteriaceae infections: A systematic review. Lancet Infect. Dis. 2010, 10, 43–50. [Google Scholar] [CrossRef]
- Michalopoulos, A.; Virtzili, S.; Rafailidis, P.; Halevelakis, G.H.; Damala, M.; Falagas, M. Intravenous fosfomycin for the treatment of nosocomial infections caused by carbapenem-resistant Klebsiella pneumoniae in critically ill patients: A prospective evaluation. Clin. Microbiol. Infect. 2010, 16, 184–186. [Google Scholar] [CrossRef] [PubMed]
- Dinh, A.; Salomon, J.; Bru, J.P.; Bernard, L. Fosfomycin: Efficacy against infections caused by multidrug-resistant bacteria. Scand. J. Infect. Dis. 2012, 44, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Hendlin, D.; Stapley, E.O.; Jackson, M.; Wallick, H.; Miller, A.K.; Wolf, F.J.; Miller, T.W.; Chaiet, L.; Kahan, F.M.; Foltz, E.L.; et al. Phosphonomycin, a new antibiotic produced by strains of Streptomyces. Science 1969, 166, 122–123. [Google Scholar] [CrossRef] [PubMed]
- Popovic, M.; Steinort, D.; Pillai, S.; Joukhadar, C. Fosfomycin: An old, new friend? Eur. J. Clin. Microbiol. Infect. Dis. 2010, 29, 127–142. [Google Scholar] [CrossRef] [PubMed]
- Bergan, T. Degree of absorption, pharmacokinetics of fosfomycin trometamol and duration of urinary antibacterial activity. Infection 1990, 18, S65–S69. [Google Scholar] [CrossRef] [PubMed]
- Ishizawa, T.; Sadahiro, S.; Hosoi, K.; Tamai, I.; Terasaki, T.; Tsuji, A. Mechanisms of intestinal absorption of the antibiotic, fosfomycin, in brush-border membrane vesicles in rabbits and humans. J. Pharm. Dyn. 1992, 15, 481–489. [Google Scholar] [CrossRef]
- Bundgaard, H. Acid-catalyzed hydrolysis of fosfomycin and its implication in oral absorption of the drug. Int. J. Pharm. 1980, 6, 1–9. [Google Scholar] [CrossRef]
- Shimizu, K. Fosfomycin: Absorption and excretion. Chemotherapy 1977, 23, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Segre, G.; Bianchi, E.; Cataldi, A.; Zannini, G. Pharmacokinetic profile of fosfomycin trometamol (Monuril). Eur. Urol. 1986, 13, 56–63. [Google Scholar] [CrossRef]
- Bergan, T.; Thorsteinsson, S.B.; Albini, E. Pharmacokinetic profile of fosfomycin trometamol. Chemotherapy 1993, 39, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Goto, M.I.T.S.; Sugiyama, M.A.S.A.; Nakajima, S.H.I.N.; Yamashina, H. Fosfomycin kinetics after intravenous and oral administration to human volunteers. Antimicrob. Agents Chemother. 1981, 20, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Cadorniga, R.; Diaz Fierros, M.; Olay, T. Pharmacokinetic study of fosfomycin and its bioavailability. Chemotherapy 1977, 23, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Zambon Switzerland Ltd. Monurol® (Fosfomycin Tromethamine): US Prescribing Information; Zambon Switzerland Ltd.: Cadempino, Switzerland, 2011. [Google Scholar]
- Borsa, F.; Leroy, A.; Fillastre, J.P.; Godin, M.; Moulin, B. Comparative pharmacokinetics of tromethamine fosfomycin and calcium fosfomycin in young and elderly adults. Antimicrob. Agents Chemother. 1988, 32, 938–941. [Google Scholar] [CrossRef] [PubMed]
- Kirby, W.M.M. Pharmacokinetics of fosfomycin. Chemotherapy 1977, 23, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Pfausler, B.; Spiss, H.; Dittrich, P.; Zeitlinger, M.; Schmutzhard, E.; Joukhadar, C. Concentrations of fosfomycin in the cerebrospinal fluid of neurointensive care patients with ventriculostomy-associated ventriculitis. J. Antimicrob. Chemother. 2004, 53, 848–852. [Google Scholar] [CrossRef] [PubMed]
- Frossard, M.; Joukhadar, C.; Erovic, B.M.; Dittrich, P.; Mrass, P.E.; van Houte, M.; Burgmann, H.; Georgopoulos, A.; Müller, M. Distribution and antimicrobial activity of fosfomycin in the interstitial fluid of human soft tissues. Antimicrob. Agents Chemother. 2000, 44, 2728–2732. [Google Scholar] [CrossRef] [PubMed]
- Matzi, V.; Lindenmann, J.; Porubsky, C.; Kugler, S.A.; Maier, A.; Dittrich, P.; Smolle-Jüttner, F.M.; Joukhadar, C. Extracellular concentrations of fosfomycin in lung tissue of septic patients. J. Antimicrob. Chemother. 2010, 65, 995–998. [Google Scholar] [CrossRef] [PubMed]
- Joukhadar, C.; Klein, N.; Dittrich, P.; Zeitlinger, M.; Geppert, A.; Skhirtladze, K.; Frossard, M.; Heinz, G.; Müller, M. Target site penetration of fosfomycin in critically ill patients. J. Antimicrob. Chemother. 2003, 51, 1247–1252. [Google Scholar] [CrossRef] [PubMed]
- Sauermann, R.; Karch, R.; Langenberger, H.; Kettenbach, J.; Mayer-Helm, B.; Petsch, M.; Wagner, C.; Sautner, T.; Gattringer, R.; Karanikas, G.; et al. Antibiotic abscess penetration: Fosfomycin levels measured in pus and simulated concentration-time profiles. Antimicrob. Agents Chemother. 2005, 49, 4448–4454. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, B.J.; Mahony, A.A.; Ellis, A.G.; Lawrentschuk, N.; Bolton, D.M.; Zeglinski, P.T.; Frauman, A.G.; Grayson, M.L. Is fosfomycin a potential treatment alternative for multidrug-resistant gram-negative prostatitis? Clin. Infect. Dis. 2014, 58, e101–e105. [Google Scholar] [CrossRef] [PubMed]
- Müller, O.; Rückert, P.D.D.; Walter, W.; Haag, R.; Sauer, W. Fosfomycin-Konzentrationen im Serum und in der Galle. Infection 1982, 10, 18–20. [Google Scholar] [CrossRef] [PubMed]
- Schintler, M.V.; Traunmller, F.; Metzler, J.; Kreuzwirt, G.; Spendel, S.; Mauric, O.; Popovic, M.; Scharnagl, E.; Joukhadar, C. High fosfomycin concentrations in bone and peripheral soft tissue in diabetic patients presenting with bacterial foot infection. J. Antimicrob. Chemother. 2009, 64, 574–578. [Google Scholar] [CrossRef] [PubMed]
- Legat, F.J.; Maier, A.; Dittrich, P.; Zenahlik, P.; Kern, T.; Nuhsbaumer, S.; Frossard, M.; Salmhofer, W.; Kerl, H.; Müller, M. Penetration of fosfomycin into inflammatory lesions in patients with cellulitis or diabetic foot syndrome. Antimicrob. Agents Chemother. 2003, 47, 371–374. [Google Scholar] [CrossRef] [PubMed]
- Kjellsson, M.C.; Kern, S.; Sauermann, R.; Dartois, V.; Pillai, G. Modeling the permeability of fosfomycin into abscess fluid. In Proceedings of the 18th Meeting of the Population Approach Group in Europe PAGE, St. Petersburg, Russia, 23–26 June 2009. [Google Scholar]
- Kwan, K.C.; Wadke, D.A.; Foltz, E.L. Pharmacokinetics of phosphonomycin in man I: Intravenous administration. J. Pharm. Sci. 1971, 60, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Lastra, C.F.; Marino, E.L.; Dominguez-Gil, A.; Tabernero, J.M.; Lope, A.G.; Chaves, M.Y. The influence of uremia on the accessibility of phosphomycin into interstitial tissue fluid. Eur. J. Clin. Pharmacol. 1983, 25, 333–338. [Google Scholar] [CrossRef]
- Bergan, T. Pharmacokinetic comparison between fosfomycin and other phosphonic acid derivatives. Chemotherapy 1990, 36, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Woodruff, H.B.; Mata, J.M.; Agravendez, S.; Mochales, S.; Rodríguez, A.; Stapley, E.O.; Wallick, H.; Miller, A.K.; Hendlin, D. Fosfomycin: Laboratory studies. Chemotherapy 1977, 23, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Neuman, M.; Fluteau, G. Blood and urinary concentrations of fosfomycin as a function of the renal function value. Chemotherapy 1977, 23, 196–199. [Google Scholar] [CrossRef] [PubMed]
- Kahan, F.M.; Kahan, J.S.; Cassidy, P.J.; Kropp, H. The Mechanism of Action of Fosfomycin (Phosphonomycin). Ann. N. Y. Acad. Sci. 1974, 235, 364–386. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.D.; Vivas, E.I.; Walsh, C.T.; Kolter, R. MurA (MurZ), the enzyme that catalyzes the first committed step in peptidoglycan biosynthesis, is essential in Escherichia coli. J. Bacteriol. 1995, 177, 4194–4197. [Google Scholar] [CrossRef] [PubMed]
- Utsui, Y.; Ohya, S.; Magaribuchi, T.; Tajima, M.; Yokota, T. Antibacterial activity of cefmetazole alone and in combination with fosfomycin against methicillin- and cephem-resistant Staphylococcus aureus. Antimicrob. Agents Chemother. 1986, 30, 917–922. [Google Scholar] [CrossRef] [PubMed]
- Frimodt-Moller, N. Fosfomycin. In Kucers’ the Use of Antibiotics; Grayson, M.L., Crowe, S.M., McCarthy, J.S., Mills, J., Mouton, J.M., Norrby, S.R., Paterson, D.L., Pfaller, M.A., Eds.; Hodder Arnold/ASM Press: London, UK, 2010; pp. 935–944. [Google Scholar]
- Michalopoulos, A.S.; Livaditis, I.G.; Gougoutas, V. The revival of fosfomycin. Int. J. Infect. Dis. 2011, 15, e732–e739. [Google Scholar] [CrossRef] [PubMed]
- Barry, A.L.; Brown, S.D. Antibacterial spectrum of fosfomycin trometamol. J. Antimicrob. Chemother. 1995, 35, 228–230. [Google Scholar] [CrossRef] [PubMed]
- European Committee on Antimicrobial Susceptibility Testing. Fosfomycin: Rationale for the Clinical Breakpoints, Version 1.0; European Committee on Antimicrobial Susceptibility Testing: Växjö, Sweden, 2013. [Google Scholar]
- Paterson, D.L. Serious infections in the intensive care unit: Pseudomonas aeruginosa and Acinetobacter baumannii. Clin. Infect. Dis. 2006, 43, S41–S42. [Google Scholar] [CrossRef]
- Faruqi, S.; McCreanor, J.; Moon, T.; Meigh, R.; Morice, A.H. Fosfomycin for Pseudomonas-related exacerbations of cystic fibrosis. Int. J. Antimicrob. Agents 2008, 32, 461–463. [Google Scholar] [CrossRef] [PubMed]
- Mirakhur, A.; Gallagher, M.J.; Ledson, M.J.; Harta, C.A.; Walshawa, M.J. Fosfomycin therapy for multiresistant Pseudomonas aeruginosa in cystic fibrosis. J. Cyst. Fibros. 2003, 2, 19–24. [Google Scholar] [CrossRef]
- Lu, C.L.; Liu, C.Y.; Huang, Y.T.; Liao, C.H.; Teng, L.J.; Turnidge, J.D.; Liao, C.H.; Teng, L.J.; Turnidge, J.D.; Hsueh, P.R. Antimicrobial Susceptibilities of commonly encountered bacterial isolates to fosfomycin determined by agar dilution and disk diffusion methods. Antimicrob. Agents Chemother. 2011, 55, 4295–4301. [Google Scholar] [CrossRef] [PubMed]
- Walsh, C.C.; Landersdorfer, C.B.; McIntosh, M.P.; Peleg, A.Y.; Hirsch, E.B.; Kirkpatrick, C.M.; Bergen, P.J. Clinically relevant concentrations of fosfomycin combined with polymyxin B, tobramycin or ciprofloxacin enhance bacterial killing of Pseudomonas aeruginosa, but do not suppress the emergence of fosfomycin resistance. J. Antimicrob. Chemother. 2016, 71, 2218–2229. [Google Scholar] [CrossRef] [PubMed]
- Castaneda-Garcia, A.; Blazquez, J.; Rodriguez-Rojas, A. Molecular Mechanisms and Clinical Impact of Acquired and Intrinsic Fosfomycin Resistance. Antibiotics 2013, 2, 217–236. [Google Scholar] [CrossRef] [PubMed]
- Tsuruoka, T.; Yamada, Y. Charactertization of spontaneous fosfomycin (phosphonomycin)-resistant cells of Escherichia coli B in vitro. J. Antibiot. 1975, 28, 906–911. [Google Scholar] [CrossRef] [PubMed]
- Kadner, R.J.; Winkler, H.H. Isolation and characterization of mutations affecting the transport of hexose phosphates in Escherichia coli. J. Bacteriol. 1973, 113, 895–900. [Google Scholar] [PubMed]
- Kim, D.H.; Lees, W.J.; Kempsell, K.E.; Lane, W.S.; Duncan, K.; Walsh, C.T. Characterization of a Cys115 to Asp substitution in the Escherichia coli cell wall biosynthetic enzyme UDP-GlcNAc enolpyruvyl transferase (MurA) that confers resistance to inactivation by the antibiotic fosfomycin. Biochemistry 1996, 35, 4923–4928. [Google Scholar] [CrossRef] [PubMed]
- Horii, T.; Kimura, T.; Sato, K.; Shibayama, K.; Ohta, M. Emergence of fosfomycin-resistant isolates of Shiga-like toxin-producing Escherichia coli O26. Antimicrob. Agents Chemother. 1999, 43, 789–793. [Google Scholar] [PubMed]
- Rigsby, R.E.; Fillgrove, K.L.; Beihoffer, L.A.; Armstrong, R.N. Fosfomycin resistance proteins: A nexus of glutathione transferases and epoxide hydrolases in a metalloenzyme superfamily. Methods Enzymol. 2005, 401, 367–379. [Google Scholar] [PubMed]
- Kobayashi, S.; Kuzuyama, T.; Seto, H. Characterization of the fomA and fomB gene products from Streptomyces wedmorensis, which confer fosfomycin resistance on Escherichia coli. Antimicrob. Agents Chemother. 2000, 44, 647–650. [Google Scholar] [CrossRef] [PubMed]
- Kuzuyama, T.; Kobayashi, S.; O’Hara, K.; Hidaka, T.; Seto, H. Fosfomycin monophosphate and fosfomycin diphosphate, two inactivated fosfomycin derivatives formed by gene products of fomA and fomB from a fosfomycin producing organism Streptomyces wedmorensis. J. Antibiot. 1996, 49, 502–504. [Google Scholar] [CrossRef] [PubMed]
- Dellit, T.H.; Owens, R.C.; McGowan, J.E.; Gerding, D.N.; Weinstein, R.A.; Burke, J.P.; Huskins, W.C.; Paterson, D.L.; Fishman, N.O.; Brennan, C.F.C.P.J. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin. Infect. Dis. 2007, 44, 159–177. [Google Scholar] [CrossRef] [PubMed]
- Safdar, N.; Handelsman, J.; Maki, D.G. Does combination antimicrobial therapy reduce mortality in Gram-negative bacteraemia? A meta-analysis. Lancet Infect. Dis. 2004, 4, 519–527. [Google Scholar] [CrossRef]
- Kastoris, A.C.; Rafailidis, P.I.; Vouloumanou, E.K.; GkegkesMatthew, I.D.; Falagas, E. Synergy of fosfomycin with other antibiotics for Gram-positive and Gram-negative bacteria. Eur. J. Clin. Pharmacol. 2010, 66, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Samonis, G.; Maraki, S.; Karageorgopoulos, D.E.; Vouloumanou, E.K.; Falagas, M.E. Synergy of fosfomycin with carbapenems, colistin, netilmicin, and tigecycline against multidrug-resistant Klebsiella pneumoniae, Escherichia coli, and Pseudomonas aeruginosa clinical isolates. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Grossato, A.; Sartori, R.; Fontana, R. Effect of non-b-lactam antibiotics on penicillin-binding protein synthesis of Enterococcus hirae ATCC 9790. J. Antimicrob. Chemother. 1991, 27, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Totsuka, K.; Uchiyama, T.; Shimizu, K.; Kanno, Y.; Takata, T.; Yoshida, T. In vitro combined effects of fosfomycin and b-lactam antibiotics against penicillin-resistant Streptococcus pneumoniae. J. Infect. Chemother. 1997, 3, 49–54. [Google Scholar] [CrossRef]
- Yamada, S.; Hyo, Y.; Ohmori, S.; Ohuchi, M. Role of ciprofloxacin in its synergistic effect with fosfomycin on drug-resistant strains of Pseudomonas aeruginosa. Chemotherapy 2007, 53, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, M.; Suzuki, K.; Asano, N.; Araki, K.; Shukuya, N.; Egami, T.; Higurashi, Y.; Morita, K.; Uchimura, H.; Watanabe, T. Effectiveness of fosfomycin combined with other antimicrobial agents against multidrug-resistant Pseudomonas aeruginosa isolates using the efficacy time index assay. J. Infect. Chemother. 2002, 8, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Tessier, F.; Quentin, C. In vitro activity of fosfomycin combined with ceftazidime, imipenem, amikacin, and ciprofloxacin against Pseudomonas aeruginosa. Eur. J. Clin. Microbiol. Infect. Dis. 1997, 16, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Martinez, L.; Rodriguez, G.; Pascual, A.; Suárez, A.I.; Perea, E.J. In Vitro activity of antimicrobial agent combinations against multiresistant Acinetobacter baumannii. J. Antimicrob. Chemother. 1996, 38, 1107–1108. [Google Scholar] [CrossRef] [PubMed]
- Santimaleeworagun, W.; Wongpoowarak, P.; Chayakul, P.; Pattharachayakul, S.; Tansakul, P.; Garey, K.W. In vitro activity of colistin or sulbactam in combination with fosfomycin or imipenem against clinical isolates of carbapenem-resistant Acinetobacter baumannii producing OXA-23 carbapenemases. Southeast Asian J. Trop. Med. Public Health 2011, 42, 890–900. [Google Scholar] [PubMed]
- Inouye, S.; Watanabe, T.; Tsuruoka, T.; Kitasato, I. An increase in the antimicrobial activity in vitro of fosfomycin under anaerobic conditions. J. Antimicrob. Chemother. 1989, 24, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Yanagida, C.; Ito, K.; Komiya, I.; Horie, T. Protective effect of fosfomycin on gentamicin-induced lipid peroxidation of rat renal tissue. Chem. Biol. Interact. 2004, 148, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Kokuryo, T.; Hashimoto, Y.; Inui, K.I. Effects of fosfomycin and imipenem-cilastatin on the nephrotoxicity of vancomycin and cisplatin in rats. J. Pharm. Pharmacol. 1999, 51, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Craig, W.A. Pharmacokinetic/pharmacodynamic parameters: Rationale for antibacterial dosing of mice and men. Clin. Infect. Dis. 1998, 26, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Mouton, J.W.; Brown, D.F.J.; Apfalter, P.; Cantón, R.; Giske, C.G.; Ivanova, M.; MacGowan, A.P.; Rodloff, A.; Soussy, C.J.; Steinbakk, M.; et al. The role of pharmacokinetics/pharmacodynamics in setting clinical MIC breakpoints: The EUCAST approach. Clin. Microbiol. Infect. 2012, 18, E37–E45. [Google Scholar] [CrossRef] [PubMed]
- Mazzei, T.; Cassetta, M.I.; Fallani, S.; Arrigucci, S.; Novelli, A. Pharmacokinetic and pharmacodynamic aspects of antimicrobial agents for the treatment of uncomplicated urinary tract infections. Int. J. Antimicrob. Agents 2006, 28, 35–41. [Google Scholar] [CrossRef] [PubMed]
- VanScoy, B.; McCauley, J.; Bhavnani, S.M.; Ellis-Grosseb, E.J.; Ambrosea, P.G. Relationship between Fosfomycin Exposure and Amplification of Escherichia coli Subpopulations with Reduced Susceptibility in a Hollow-Fiber Infection Model. Antimicrob. Agents Chemother. 2016, 60, 5141–5145. [Google Scholar] [CrossRef] [PubMed]
- Roussos, N.; Karageorgopoulos, D.E.; Samonis, G.; Falagas, M.E. Clinical significance of the pharmacokinetic and pharmacodynamic characteristics of fosfomycin for the treatment of patients with systemic infections. Int. J. Antimicrob. Agents 2009, 34, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Kühnen, E.; Pfeifer, G.; Frenkel, C. Penetration of fosfomycin into cerebrospinal fluid across non-inflamed and inflamed meninges. Infection 1987, 15, 422–424. [Google Scholar] [CrossRef] [PubMed]
- Docobo-Perez, F.; Drusano, G.L.; Johnson, A.; Goodwin, J.; Whalley, S.; Ramos-Martín, V.; Ballestero-Tellez, M.; Rodriguez-Martinez, J.M.; Conejo, M.C.; van Guilder, M.; et al. Pharmacodynamics of fosfomycin: Insights into clinical use for antimicrobial resistance. Antimicrob. Agents Chemother. 2015, 59, 5602–5610. [Google Scholar] [CrossRef] [PubMed]
- Rosso-Fernandez, C.; Sojo-Dorado, J.; Barriga, A.; Lavín-Alconero, L.; Palacios, Z.; López-Hernández, I.; Merino, V.; Camean, M.; Pascual, A.; Rodríguez-Baño, J. Fosfomycin versus meropenem in bacteraemic urinary tract infections caused by extended-spectrum beta-lactamase-producing Escherichia coli (FOREST): Study protocol for an investigator-driven randomised controlled trial. BMJ Open 2015, 5, e007363. [Google Scholar] [CrossRef] [PubMed]
- Sádaba-Díaz De Rada, B.; Azanza-Perea, J.R.; García-Quetglas, E.; Honorato-Pérez, J. Fosfomicina trometamol. Dosis múltiples como pauta larga en el tratamiento de las infecciones urinarias bajas. Enferm. Infect. Microbiol. Clin. 2006, 24, 546–550. [Google Scholar] [CrossRef]
- Qiao, L.D.; Zheng, B.; Chen, S.; Yang, Y.; Zhang, K.; Guo, H.F.; Yang, B.; Niu, Y.J.; Wang, Y.; Shi, B.K.; et al. Evaluation of three-dose fosfomycin tromethamine in the treatment of patients with urinary tract infections: An uncontrolled, open-label, multicentre study. BMJ Open 2013, 3, e004157. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, N.K.; Amuh, D.; Goldman, M.P.; Riebel, W.J.; Tomford, W.J. Treatment of a complicated vancomycin-resistant enterococcal urinary tract infection with fosfomycin. Infect. Dis. Clin. Pract. 2000, 9, 368–371. [Google Scholar] [CrossRef]
- Multiple-Dose Regimen Of Intravenous and Oral Fosfomycin Tromethamine as a Potential Therapy for the Treatment of Systemic Infections Due to Multidrug-Resistantbacteria. Available online: https://www.escmid.org/research_projects/escmid_conferences/past_escmid_conferences/reviving_old_antibiotics/poster_presentations/ (accessed on 17 October 2017).

{kind=link}
{kind=link}
{kind=link}
| Ref | Dose | Study Group (N) | Tmax (h) | t1/2β (h) | Vd (L) | CL (L/h) | CLR | F (%) | ka | kel | Q |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Fosfomycin calcium | |||||||||||
| Cadorniga et al., 1977 [28] | 500 mg | HV (6) | 2–2.5 | 2.04 | 20.7 | ND | ND | 37 | ND | 0.12 | NA |
| Goto et al., 1981 [27] | 20 mg/kg | HV (7) | 2.3 (0.3) | 3.01 (0.67) g | 30.1 (4.6) | 7.1 (1.5) | ND | 28 (7.0) | 1.03 (0.38) | 0.24 (0.05) | NA |
| 40 mg/kg | HV (7) | 2.7 (0.2) | 5.05 (0.81) g | 60.2 (17.4) | 9.0 (1.7) | ND | 28 (8.0) | 0.92 (0.40) | 0.14 (0.02) | NA | |
| Borsa et al., 1988 [30] | 40 mg/kg SD | Young HV (5) | 1.41 (0.67) | 4.81 (1.90) g | 435.0 (144.0) | 59.3 (23.3) a | 5.0 (1.1) a | ND | ND | 0.170 (0.084) | NA |
| Elderly HV (8) | 2.58 (0.54) | 11.80 (6.86) g | 409.4 (100.4) | 33.4 (23.1) a | 3.3 (1.1) a | ND | ND | 0.082 (0.047) | NA | ||
| Bergan et al., 1990 [21] | 50 mg/kg | HV (8) | 2.9 (0.6) | 5.6 (1.8) g | ND | ND | ND | 12.0 (7.5) | ND | 0.135 (0.053) | NA |
| Fosfomycin tromethamine | |||||||||||
| Segre et al., 1987 [25] | 50 mg/kg | HV (5) | 2.2 (0.44) | 2.43 (0.31) | 10.4 (1.5) | 8.3 (1.6) | 7.0 (0.9) | 0.44 (0.09) 0.58 (0.04) e | Transit model k10: 1.24 (0.55) k12: 1.69 (0.62) k23: 0.34 (0.10) | k35: 0.69 (0.07) f | NA |
| Borsa et al., 1988 [30] | 25 mg/kg SD | Young HV (5) | 1.61 (0.23) | 5.37 (2.56) g | 186.3 (129.4) | 19.4 (8.4) a | 10.8 (1.5) a | ND | ND | 0.156 (0.073) | NA |
| Elderly HV (8) | 2.16 (0.72) | 8.28 (5.51) g | 101.1 (61.2) | 9.7 (4.2) a | 2.9 (1.0) a | ND | ND | 0.124 (0.078) | NA | ||
| Bergan et al., 1990 [21] | 25 mg/kg | HV (8) | 2.6 (0.5) | 3.9 (0.65) g | ND | ND | ND | ND | ND | 0.183 (0.031) | NA |
| 50 mg/kg | HV (8) | 2.5 (0.8) | 3.6 (0.44) g | ND | ND | ND | 40.6 (17.9) | ND | 0.197 (0.024) | NA | |
| Bergan et al., 1993 [26] | 2 g | HV (12) | 2.2 (0.9) | 4.1 (0.8) g | ND | ND | ND | ND | ND | 0.17b | NA |
| 3 g | HV (12) | 2.0 (0.6) | 4.5 (2.1) g | ND | ND | ND | 32.9 (7.9) | ND | 0.15b | NA | |
| 4 g | HV (12) | 2.0 (0.0) | 3.9 (0.7) g | ND | ND | ND | ND | ND | 0.18b | NA | |
| Fosfomycin disodium | |||||||||||
| Kwan et al., 1971 [42] | 250 or 500 mg, 10-min infusion, Single dose 500 mg every 6 h, 8 times. | HV (17) | NA | 1.1 c | Vc: 12.9 | 7.5 | 7.1 | NA | NA | K13: 0.62 | 12.4 b k12: 0.96 k21: 1.19 |
| Cadorniga et al., 1977 [28] | 500 mg, 5-min infusion | HV (6) | NA | t1/2α: 0.38 t1/2β: 2.04 | Vc: 12.9 Vp: 7.8 Vdss: 20.7 | ND | ND | NA | NA | K13: 0.67 | 6.9 b k12: 0.54 k21: 0.88 |
| Goto et al., 1981 [27] | 20 mg/kg, 5-min infusion | HV (7) | NA | 2.25 (0.74) | Vc: 8.7 (2.9) Vp: 9.8 (1.7) Vdss: 18.5 (4.6) | 7.2 (1.6) | 6.0 (2.2) | NA | NA | β: 0.34 (0.12) k10: 0.92 (0.31) | 14.2 b k12: 1.62 (0.76) k21: 1.45 (0.75) |
| 40 mg/kg, 5-min infusion | HV (7) | NA | 2.22 (0.46) | Vc: 8.7 (2.9) Vp: 12.7 (2.9) Vdss: 20.8 (3.5) | 8.0 (0.8) | 6.6 (0.9) | NA | NA | β: 0.32 (0.06) k10: 0.99 (0.22) | 16.2 b k12: 1.84 (0.85) k21: 1.30 (0.49) | |
| Lastra et al., 1983 [43] | 30 mg/kg | Patients with normal renal function (9) | NA | t1/2α: 0.18 (0.09) t1/2β:1.91 (0.50) | 21.2 (10.4) | 7.9 (3.2) | ND | NA | NA | k13: 1.91 (1.29) | k12: 2.22 (1.49) k21: 1.18 (0.68) |
| Patients with impaired renal function (8) | NA | t1/2α: 0.61 (0.18) t1/2β: 16.3 (11.9) | 17.8 (6.8) | 1.1 (0.8) | ND | NA | NA | k13: 0.21 (0.17) | k12: 0.66 (0.38) k21: 0.43 (0.13) | ||
| Segre et al., 1987 [25] | 50 mg/kg, Single injection | HV (5) | NA | 2.43 (0.31) | 10.4 (1.5) | 8.3 (1.6) | 7.0 (0.9) | NA | NA | k35: 0.69 (0.07) f | 10.6 b k34: 1.00 (0.92) k43: 1.40 (0.91) |
| Bergan et al., 1990 [21] | 50 mg/kg, 5-min infusion | HV (8) | NA | 3.4 (1.1) | ND | ND | ND | NA | NA | 0.206 (0.048) | ND |
| Bergan et al., 1993 [26] | 3 g | HV (12) | 0.02 (0.0) | 2.1 (0.1) | ND | ND | ND | NA | NA | 0.33 b | ND |
| Joukhadar et al., 2003 [35] | 8 g, 20-min infusion | Critically ill patients (9) | 0.4 (0.1) | 3.9 (0.9) | 31.5 (4.5) | 7.2 (1.3) | ND | NA | NA | 0.18 b | ND |
| Pfausler et al., 2004 [32] | 8 g, 30-min infusion, Single dose | Patients requiring extraventricular drainage (6) | 1.2 (0.4) | 3.0 (1.0) | 30.8 (10.2) | 7.4 (2.3) | ND | NA | NA | ND | ND |
| 8 g, 30-min infusion, every 8 h for 5 days | Patients requiring EVD | 1.5 (1.2) | 4.0 (0.5) | 26.3 (9.7) | 5.0 (2.0) | ND | NA | NA | ND | ND | |
| Sauermann et al., 2005 [36] | 8 g, 30-min infusion, Single dose | Patients (12) | 0.47 (0.12) | 3.7 (2.2) | Vc: 15.5 (4.5) Vdss: 28.6 (9.9) | 7.6 (4.1) | ND | NA | NA | 0.19 b | ND |
| Kjellsson et al., 2009 [41] | 8 g, 30-min infusion, Single dose | Patients (12) | NA | 1.2c | Vc: 10.1 (5.4–14.8) Vp: 9.80 (5.7–13.9) | 5.8 (3.8–7.8) | ND | NA | NA | 0.58 d | 15.4 (9.1–21.6) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dijkmans, A.C.; Zacarías, N.V.O.; Burggraaf, J.; Mouton, J.W.; Wilms, E.B.; Van Nieuwkoop, C.; Touw, D.J.; Stevens, J.; Kamerling, I.M.C. Fosfomycin: Pharmacological, Clinical and Future Perspectives. Antibiotics 2017, 6, 24. https://doi.org/10.3390/antibiotics6040024
Dijkmans AC, Zacarías NVO, Burggraaf J, Mouton JW, Wilms EB, Van Nieuwkoop C, Touw DJ, Stevens J, Kamerling IMC. Fosfomycin: Pharmacological, Clinical and Future Perspectives. Antibiotics. 2017; 6(4):24. https://doi.org/10.3390/antibiotics6040024
Chicago/Turabian StyleDijkmans, Anneke Corinne, Natalia Veneranda Ortiz Zacarías, Jacobus Burggraaf, Johan Willem Mouton, Erik Bert Wilms, Cees Van Nieuwkoop, Daniel Johannes Touw, Jasper Stevens, and Ingrid Maria Catharina Kamerling. 2017. "Fosfomycin: Pharmacological, Clinical and Future Perspectives" Antibiotics 6, no. 4: 24. https://doi.org/10.3390/antibiotics6040024
APA StyleDijkmans, A. C., Zacarías, N. V. O., Burggraaf, J., Mouton, J. W., Wilms, E. B., Van Nieuwkoop, C., Touw, D. J., Stevens, J., & Kamerling, I. M. C. (2017). Fosfomycin: Pharmacological, Clinical and Future Perspectives. Antibiotics, 6(4), 24. https://doi.org/10.3390/antibiotics6040024