Patient and Prescriber Views of Penicillin Allergy Testing and Subsequent Antibiotic Use: A Rapid Review

 , , , , and
, , , , and
Abstract
:1. Introduction
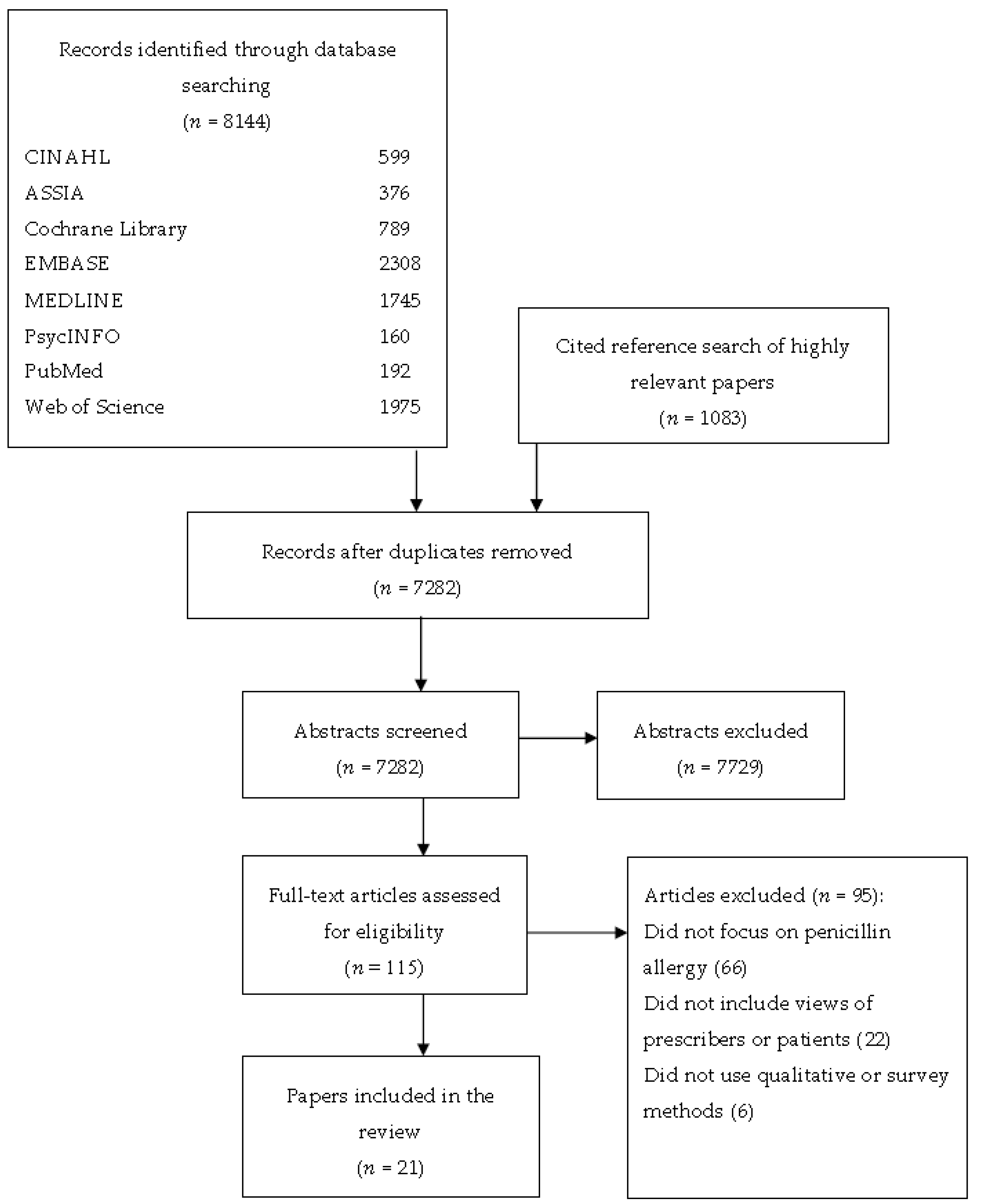
2. Materials and Methods
3. Results
3.1. Clinicians’ Views of Penicillin Allergy Testing
3.2. Patients’ Views of Penicillin Allergy Testing
3.3. Influences on Clinician Antibiotic Prescribing Behaviour when Treating Patients with Suspected Penicillin Allergy
3.4. Influences on Clinician Antibiotic Prescribing Behaviour and Patient Antibiotic Use Following a Penicllin Allergy Test
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- National Institute for Health and Care Excellence. Drug Allergy: Diagnosis and Management of Drug Allergy in Adults, Children and Young People; NICE Clinical Guideline 183; NICE: London, UK, 2014.
- Minh, H.-B.C.; Bousquet, P.J.; Fontaine, C.; Kvedariene, V.; Demoly, P. Systemic reactions during skin tests with β-lactams: A risk factor analysis. J. Allergy Clin. Immunol. 2006, 117, 466–468. [Google Scholar] [CrossRef] [PubMed]
- Charneski, L.; Deshpande, G.; Smith, S.W. Impact of an antimicrobial allergy label in the medical record on clinical outcomes in hospitalized patients. Pharmacotherapy 2011, 31, 742–747. [Google Scholar] [CrossRef] [PubMed]
- Mistry, A.; Arumugakani, G.; Toolan, J.; Ford, K.; Sandoe, J.; Wood, P.; Savic, S. Does de-labelling penicillin allergy lead to a respective change in primary care records? In Proceedings of the British Society for Allergy and Clinical Immunology Annual Meeting, Telford International Centre, Telford, UK, 4–6 September 2015. [Google Scholar]
- Salkind, A.R.; Cuddy, P.G.; Foxworth, J.W. Is this patient allergic to penicillin? An evidence-based analysis of the likelihood of penicillin allergy. JAMA 2001, 285, 2498–2505. [Google Scholar] [CrossRef] [PubMed]
- Li, J.T.; Markus, P.J.; Osmon, D.R.; Estes, L.; Gosselin, V.A.; Hanssen, A.D. Reduction of vancomycin use in orthopedic patients with a history of antibiotic allergy. Proc. Mayo Clin. 2000, 75, 902–906. [Google Scholar] [CrossRef] [PubMed]
- Vyles, D.; Chiu, A.; Routes, J.; Castells, M.; Phillips, E.J.; Kibicho, J.; Brousseau, D.C. Antibiotic Use After Removal of Penicillin Allergy Label. Pediatrics 2018, 141, e20173466. [Google Scholar] [CrossRef] [PubMed]
- Sacco, K.; Bates, A.; Brigham, T.; Imam, J.; Burton, M. Clinical outcomes following inpatient penicillin allergy testing: A systematic review and meta-analysis. Allergy 2017, 72, 1288–1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganann, R.; Ciliska, D.; Thomas, H. Expediting systematic reviews: Methods and implications of rapid reviews. Implement. Sci. 2010, 5, 56. [Google Scholar] [CrossRef] [PubMed]
- Khangura, S.; Polisena, J.; Clifford, T.J.; Farrah, K.; Kamel, C. Rapid review: An emerging approach to evidence synthesis in health technology assessment. Int. J. Technol. Assess. Health Care 2014, 30, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Haby, M.M.; Chapman, E.; Clark, R.; Barreto, J.; Reveiz, L.; Lavis, J.N. What are the best methodologies for rapid reviews of the research evidence for evidence-informed decision making in health policy and practice: A rapid review. Health Res. Policy Syst. 2016, 14, 83. [Google Scholar] [CrossRef] [PubMed]
- Al-Ahmad, M.; Rodriguez-Bouza, T. Drug allergy evaluation for betalactam hypersensitivity: Cross-reactivity with cephalosporines, carbapenems and negative predictive value. Asian Pac. J. Allergy Immunol. 2017. [Google Scholar] [CrossRef]
- Amin, W.; Hitch, G.; Molai, S.; Khan, I.; Mulla, R. A clinical audit on reporting and documentation of penicillin allergy at an NHS Foundation Trust Hospital. Int. J. Pharm. Pract. 2010, 18, 36–37. [Google Scholar]
- Andres, B.; Corominas, M.; Lleonart, R. Suspected allergy to betalactam antibiotic: The value of diagnostic evaluation. Allergy 2013, 68, 518. [Google Scholar]
- Blumenthal, K.G.; Shenoy, E.S.; Hurwitz, S.; Varughese, C.A.; Hooper, D.C.; Banerji, A. Effect of a drug allergy educational program and antibiotic prescribing guideline on inpatient clinical providers’ antibiotic prescribing knowledge. J. Allergy Clin. Immunol. Pract. 2014, 2, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Khateeb-Alabbasi, A.; Nusem, D.; Panassof, J. The real use of beta-lactams after “penicillin allergic” label removal. World Allergy Organ. J. 2012, 5, S102. [Google Scholar] [CrossRef]
- Elkhalifa, S.; Calisti, G.; Owens, L.; Garcez, T.; Dodgson, K.; Alexander, K. Management of patients with a history of penicillin allergy: Barriers to best practice and strategies to overcome them. Allergy 2017, 72, 224. [Google Scholar] [CrossRef]
- Eriksson, M.; Mincheva, R.; Pullerits, T. Are patients prone to using penicillin after testing negative for penicillin allergy at a specialist centre? Allergy 2017, 72, 263. [Google Scholar] [CrossRef]
- Gerace, K.; Phillips, E. Penicillin allergy label persists despite negative testing. J. Allergy Clin. Immunol. Pract. 2015, 3, 815–816. [Google Scholar] [CrossRef] [PubMed]
- Grillo, J.A.; Le, T.V. An assessment of current practice and knowledge of penicillin allergy at hospital-based pediatric centers. J. Allergy Clin. Immunol. 2015, 135. [Google Scholar] [CrossRef]
- Hayoun, M.B.; Bourrier, T.; Pognonec, C.; Sanfiorenzo, C.; Marquette, C.; Leroy, S. The impact of allergy to beta-lactam antibiotocs on general practitioners and patients in a cohort of154 French patients. Rev. Fr. Allergol. 2015, 55, 333–340. [Google Scholar] [CrossRef]
- Jose, J.; Ishmael, F.T. A drug allergy education handout is an easy and effective method to improve patient awareness of penicillin allergy and increase penicillin testing. J. Allergy Clin. Immunol. 2017, 139, AB29. [Google Scholar] [CrossRef]
- Phillips, E.J.; Knowles, S.R.; O’brien, L.; Weber, E.A. The utility of penicillin skin testing in a tertiary care clinic. J. Allergy Clin. Immunol. 2002, 109, S143. [Google Scholar] [CrossRef]
- Picard, M.; Bégin, P.; Bouchard, H.; Cloutier, J.; Lacombe-Barrios, J.; Paradis, J.; Des Roches, A.; Laufer, B.; Paradis, L. Treatment of patients with a history of penicillin allergy in a large tertiary-care academic hospital. J. Allergy Clin. Immunol. Pract. 2013, 1, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Ratzon, R.; Reshef, A.; Efrati, O.; Deutch, M.; Forschmidt, R.; Cukierman-Yaffe, T.; Kenett, R.; Kidon, M.I. Impact of an extended challenge on the effectiveness of beta-lactam hypersensitivity investigation. Ann. Allergy Asthma Immunol. 2016, 116, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Semedo, F.; Cruz, C.; Reis, R.; Tomaz, E.; Inacio, F. Full course drug provocation tests to penicillins-do we really need them? In Allergy; Wiley: Hoboken, NJ, USA, 2017; p. 282. [Google Scholar]
- Soni, D.; Ramsey, A.; Staicu, M. A clinical perspective: The prescriber’s true understanding of the ‘penicillin allergic’patient. Ann. Allergy Asthma Immunol. 2016, 117, S18. [Google Scholar] [CrossRef]
- Staicu, M.L.; Soni, D.; Conn, K.M.; Ramsey, A. A survey of inpatient practitioner knowledge of penicillin allergy at 2 community teaching hospitals. Ann. Allergy Asthma Immunol. 2017, 119, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Suetrong, N.; Klaewsongkram, J. The Differences and Similarities between Allergists and Non-Allergists for Penicillin Allergy Management. J. Allergy 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Sundquist, B.K.; Bowen, B.J.; Otabor, U.; Celestin, J.; Sorum, P.C. Proactive penicillin allergy testing in primary care patients labeled as allergic: Outcomes and barriers. Postgrad. Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- Trubiano, J.A.; Beekmann, S.E.; Worth, L.J.; Polgreen, P.M.; Thursky, K.A.; Slavin, M.A.; Grayson, M.L.; Phillips, E.J. Improving Antimicrobial Stewardship by Antibiotic Allergy Delabeling: Evaluation of Knowledge, Attitude, and Practices Throughout the Emerging Infections Network. Open Forum Infect. Dis. 2016, 3. [Google Scholar] [CrossRef] [PubMed]
- Warrington, R.J.; Lee, K.R.; McPhillips, S. The value of skin testing for penicillin allergy in an inpatient population: Analysis of the subsequent patient management. Allergy Asthma Proc. 2000, 21, 297–299. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Social Care. UK Five Year Antimicrobial Resistance Strategy 2013 to 2018; Department of Health and Social Care: London, UK, 2013.
- Arroliga, M.E.; Radojicic, C.; Gordon, S.M.; Popovich, M.J.; Bashour, C.A.; Melton, A.L.; Arroliga, A.C. A prospective observational study of the effect of penicillin skin testing on antibiotic use in the intensive care unit. Infect. Control Hosp. Epidemiol. 2003, 24, 347–350. [Google Scholar] [CrossRef] [PubMed]
- Nadarajah, K.; Green, G.R.; Naglak, M. Clinical outcomes of penicillin skin testing. Ann. Allergy Asthma Immunol. 2005, 95, 541–545. [Google Scholar] [CrossRef]


{kind=link}
| Authors | Title | Country, Setting | Year | Design | Research Aim | Population |
|---|---|---|---|---|---|---|
| Al-Ahmad, M. & Rodriguez-Bouza, T. [12] | Drug allergy evaluation for beta-lactam hypersensitivity: Cross-reactivity with cephalosporins, carbapenems, and negative predictive value | Kuwait, tertiary public allergy centre | 2017 | Telephone survey | To evaluate subsequent beta-lactam use following a negative test | 40 patients who had a negative penicillin allergy test |
| Amin, W., et al. [13] [Conference abstract] | A clinical audit on reporting and documentation of penicillin allergy at an NHS Foundation Trust Hospital | U.K., general hospital | 2010 | Questionnaire | To examine patients’ and professionals’ perceptions and knowledge regarding penicillin allergic reactions | 30 hospital clinicians |
| Andres, B. et al. [14] [Conference abstract] | Suspected allergy to beta-lactam antibiotic: The value of diagnostic evaluation | Spain, Allergy Department | 2013 | Telephone survey | To assess the number of patients with confirmed beta-lactam allergy, drugs involved in reactions, and the usefulness of the diagnostic tests | 40 patients who had a negative penicillin allergy test |
| Blumenthal, K.G. et al. [15] | Effect of a drug allergy educational program and antibiotic prescribing guideline on inpatient clinical providers’ antibiotic prescribing knowledge | U.S., tertiary care facility | 2014 | Questionnaire | To survey inpatient providers to ascertain their baseline drug allergy knowledge and preparedness in caring for patients with penicillin allergy | 258 inpatient providers from neurology, paediatrics, internal medicine, orthopaedic surgery, general surgery, attending hospital physicians, and nurse practitioners |
| Cohen, S. et al. [16] [Conference abstract] | The real use of beta-lactams after “penicillin allergic” label removal | Israel, allergy clinic | 2012 | Telephone questionnaire | To assess patients’ confidence in their allergy test results and whether they have taken penicillin since testing | 106 patients who had a negative penicillin allergy test |
| Elkhalifa, S. et al. [17] [Conference abstract] | Management of patients with a history of penicillin allergy: Barriers to best practice and strategies to overcome them | U.K., general hospital | 2017 | Email survey | To investigate prescribers’ knowledge of penicillin allergy diagnosis and management and their views about the barriers to correct management | 164 hospital doctors including doctors in training, consultants, and non-medical prescribers |
| Eriksson, M. et al. [18] [Conference abstract] | Are patients prone to using penicillin after testing negative for penicillin allergy at a specialist centre? | Sweden, allergy clinic | 2017 | Questionnaire | To assess, if tested negatively for penicillin allergy, patients’ attitude to future penicillin treatment | 103 patients who had a negative penicillin allergy test |
| Gerace, K. & Phillips, E. [19] | Penicillin allergy label persists despite negative testing | U.S., allergy clinic | 2015 | Email or telephone survey | To elucidate patient interpretation of their results and antibiotic utilisation after penicillin allergy testing (PAT) | 42 patients who underwent PAT |
| Grillo, J. A. & Le, T.V. [20] [Conference abstract] | An assessment of current practice and knowledge of penicillin allergy at hospital-based paediatric centres | U.S., hospital-based centres | 2015 | Online survey | To assess current knowledge of clinicians and management of penicillin allergy | Inpatient paediatric providers at hospital-based centres |
| Hayoun, M.B. et al. [21] | The impact of allergy to beta-lactam antibiotics on general practitioners and patients in a cohort of 154 French patients | France, primary care | 2015 | Telephone questionnaire | To evaluate the role of the general practitioner (GP) in the management of allergy to Beta Lactams, and to analyse the interpretation of the allergological assessment by the GPs or patients themselves | 80 GPs and 26 patients (when GP not available) |
| Jose, J. & Ishmael, F. T. [22] [Conference abstract] | A drug allergy education handout is an easy and effective method to improve patient awareness of penicillin allergy and increase penicillin testing | U.S., allergy clinic | 2017 | Survey | To assess patients’ prior knowledge of penicillin allergy and whether they were interested in being allergy tested | 67 patients who attended a general allergy clinic |
| Phillips, E. J. et al. [23] [Conference abstract] | The Utility of Penicillin Skin Testing in a Tertiary Care Clinic | Canada, Drug Safety Clinic | 2002 | Telephone survey | To determine how the information provided from penicillin skin testing affects beta-lactam antibiotic use or patient attitudes towards future use of beta-lactam antibiotics | 348 patients who had a negative penicillin allergy test |
| Picard, M. et al. [24] | Treatment of Patients with a History of Penicillin Allergy in a Large Tertiary-Care Academic Hospital | Canada, general hospital | 2013 | Survey | To assess allergy referral habits for patients with a history of penicillin allergy | 44 attending physicians |
| Ratzon, R. et al., [25] | Impact of an extended challenge on the effectiveness of beta-lactam hypersensitivity investigation | Israel, medical centre | 2016 | Survey | To evaluate the effectiveness of a 7-day Drug Provocation Test (DPT) and a 1-day (short) DPT for beta-lactam allergy | 49 patients who had a negative penicillin allergy test |
| Semedo, F.M. [26] [Conference abstract] | Full course drug provocation tests to penicillins—do we really need them? | Portugal, not known | 2017 | Survey | To evaluate diagnosis of penicillin allergy | 54 patients who had a negative penicillin allergy test |
| Soni, D. et al. [27] [Conference abstract] | A clinical perspective: the prescribers’ true understanding of the penicillin-allergic patient | U.S., not known | 2016 | Survey | To survey knowledge of inpatient providers from different specialties regarding penicillin allergy | 121 inpatients providers |
| Staicu, M.L. et al. [28] | A survey of inpatient practitioner knowledge of penicillin allergy at 2 community teaching hospitals | U.S., community-based teaching hospitals | 2017 | Online survey | To describe health care practitioner behaviour and identify potential knowledge gaps pertinent to the management of the penicillin-allergic patient | 276 healthcare practitioners including attending physicians, advanced practice practitioners, pharmacists, and residents |
| Suetrong, N. & Klaewsongkram, J. [29] | The Differences and Similarities between Allergists and Non-Allergists for Penicillin Allergy Management | Thailand | 2014 | Email survey | To assess knowledge of penicillin allergy skin testing and attitudes towards the management of patients with a history of penicillin allergy | 205 physicians including general practitioners, internists, paediatricians, allergists |
| Sundquist, B. K. et al. [30] | Proactive penicillin allergy testing in primary care patients labelled as allergic: outcomes and barriers | U.S., academic Internal Medicine practice | 2017 | Telephone survey (patients); Online survey (general practitioners) | To determine patient satisfaction with PAT to determine barriers to referring patients to testing | 31 patients who had a negative penicillin allergy test 7 primary care clinicians who referred patients to the study |
| Trubiano, J. A. [31] | Improving Antimicrobial Stewardship by Antibiotic Allergy Delabelling: Evaluation of Knowledge, Attitude, and Practices Throughout the Emerging Infections Network | U.S. and Canada, the Emerging Infections Network | 2016 | Email survey | To assess receptiveness for incorporating antibiotic allergy testing in hospitals | 736 active members of the Emerging Infections Network clinicians: Adult and paediatric Infectious Disease physicians |
| Warrington, R. J. et al. [32] | The value of skin testing for penicillin allergy in an inpatient population: analysis of the subsequent patient management. | Canada, allergy clinic | 2000 | Telephone survey | To assess why antibiotics were not taken after a negative skin test for penicillin allergy | 84 patients who had a negative penicillin allergy skin test |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wanat, M.; Anthierens, S.; Butler, C.C.; Wright, J.M.; Dracup, N.; Pavitt, S.H.; Sandoe, J.A.T.; Tonkin-Crine, S. Patient and Prescriber Views of Penicillin Allergy Testing and Subsequent Antibiotic Use: A Rapid Review. Antibiotics 2018, 7, 71. https://doi.org/10.3390/antibiotics7030071
Wanat M, Anthierens S, Butler CC, Wright JM, Dracup N, Pavitt SH, Sandoe JAT, Tonkin-Crine S. Patient and Prescriber Views of Penicillin Allergy Testing and Subsequent Antibiotic Use: A Rapid Review. Antibiotics. 2018; 7(3):71. https://doi.org/10.3390/antibiotics7030071
Chicago/Turabian StyleWanat, Marta, Sibyl Anthierens, Christopher C. Butler, Judy M. Wright, Naila Dracup, Sue H. Pavitt, Jonathan A. T. Sandoe, and Sarah Tonkin-Crine. 2018. "Patient and Prescriber Views of Penicillin Allergy Testing and Subsequent Antibiotic Use: A Rapid Review" Antibiotics 7, no. 3: 71. https://doi.org/10.3390/antibiotics7030071