
Efficacy and Safety of Tixagevimab/Cilgavimab to Prevent COVID-19 (Pre-Exposure Prophylaxis): A Systematic Review and Meta-Analysis

 , and
, and
Abstract
:1. Introduction
Aim of the Study
2. Methods
2.1. Design
2.2. Search Strategy and Selection Criteria
2.3. Inclusion Criteria
2.4. Participants
2.5. Intervention
2.6. Study Variables
2.7. Searching Keywords
2.8. Exclusion Criteria
2.9. Data Extraction and Analysis
2.10. Risk of Biased Evaluation of Included Studies
2.11. Assessment of Heterogeneity
2.12. Statistical Analysis
3. Results
3.1. Study Characteristics and Quality
3.2. Demographic and Clinical Characteristics of Patients in the TGM/CGM and Control Groups
3.3. TGM/CGM and Outcomes
3.4. Clinical Outcomes
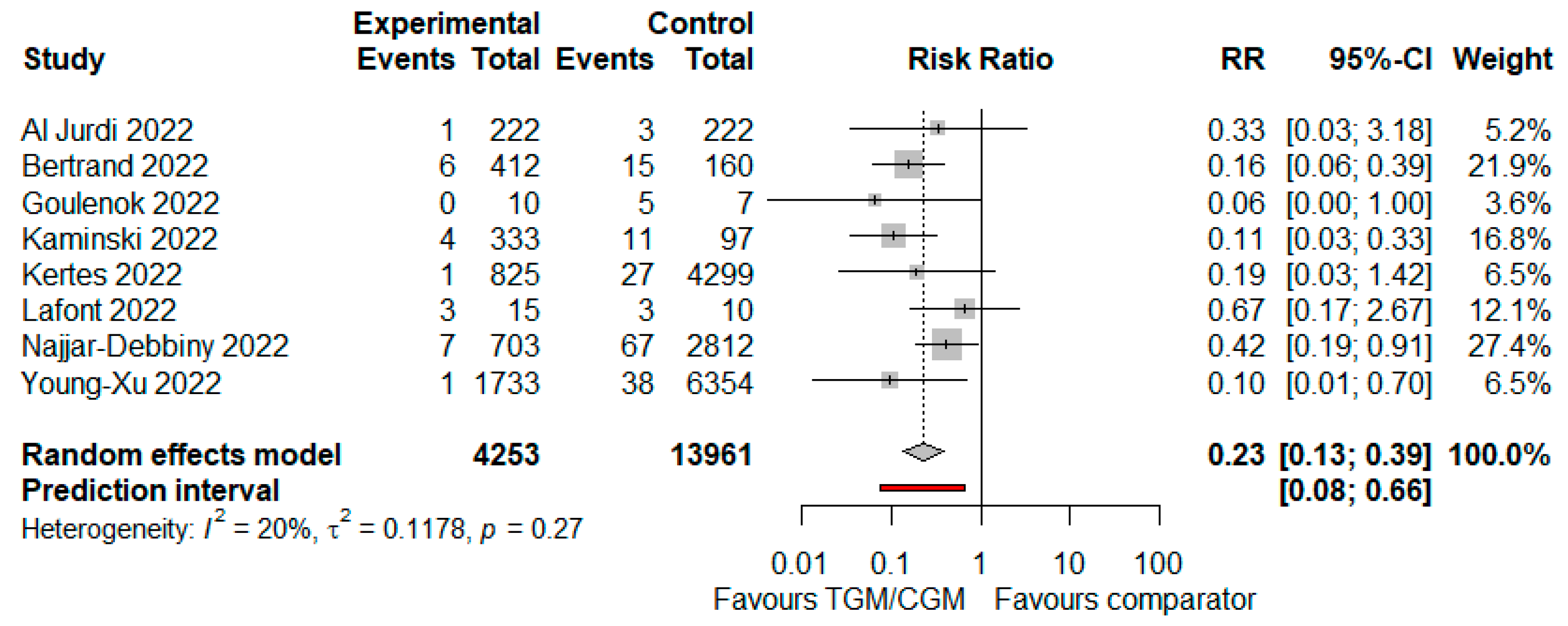
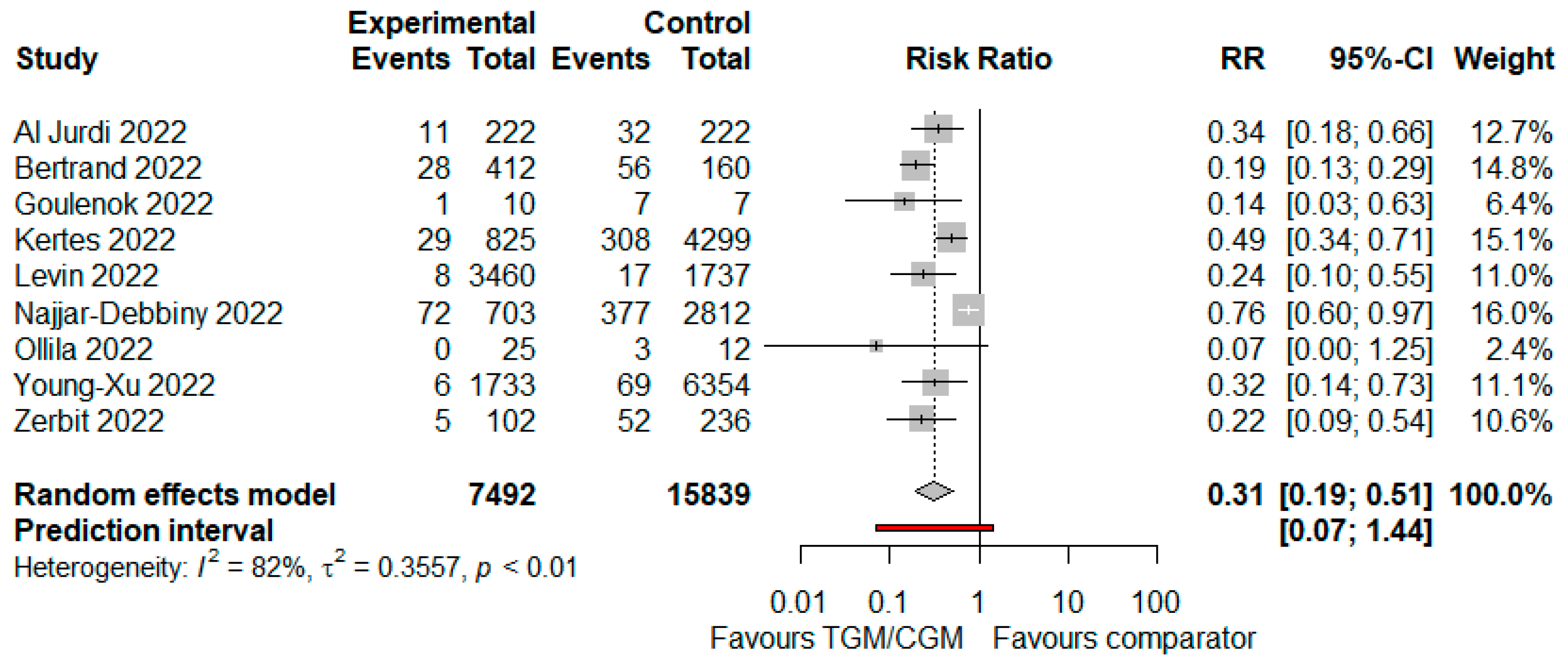
3.4.1. COVID-19-Related Hospitalization
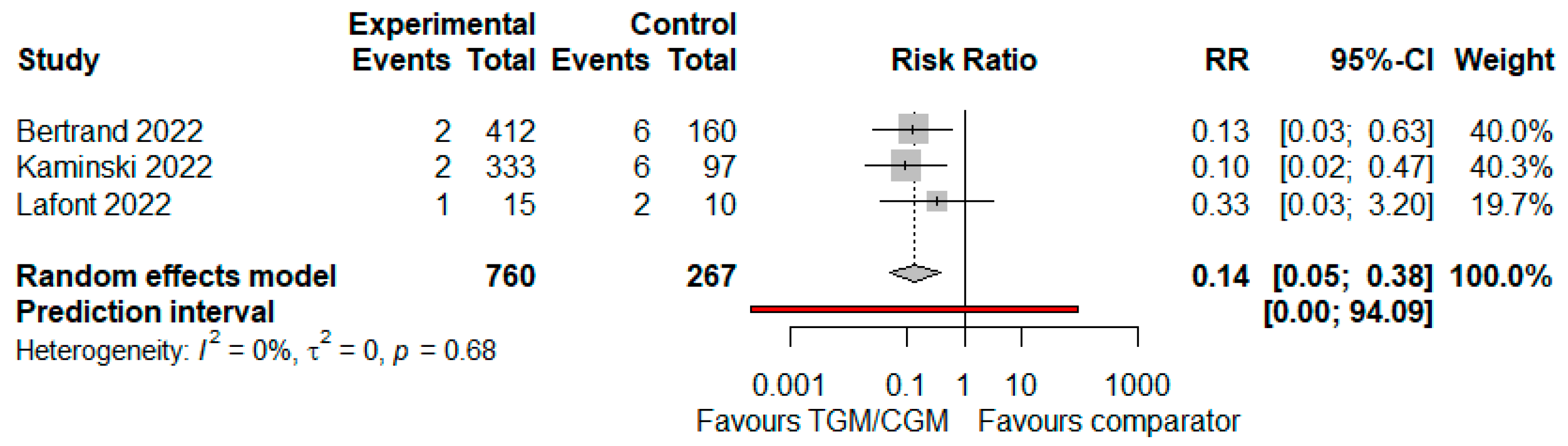
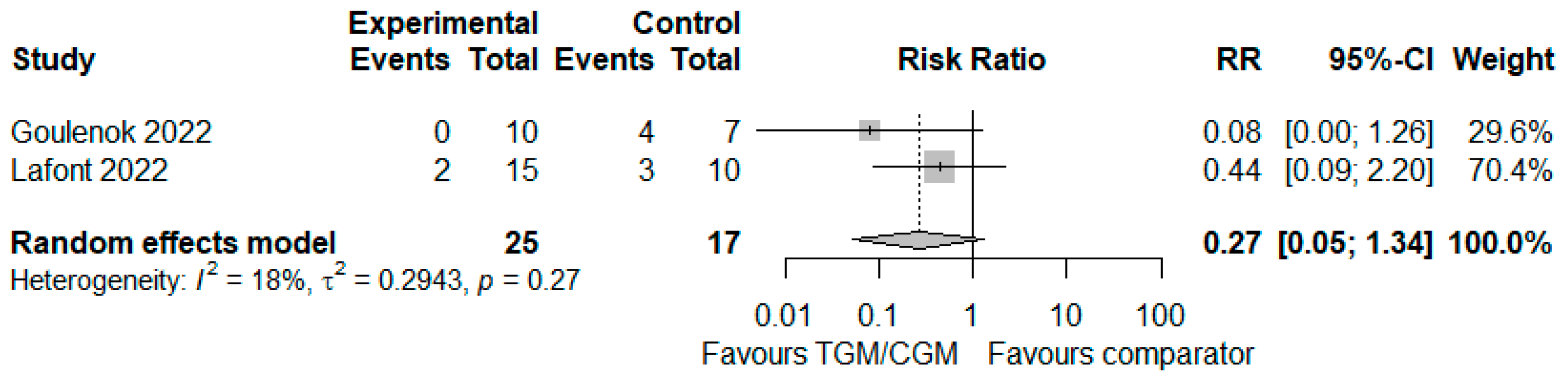
3.4.2. ICU Admission
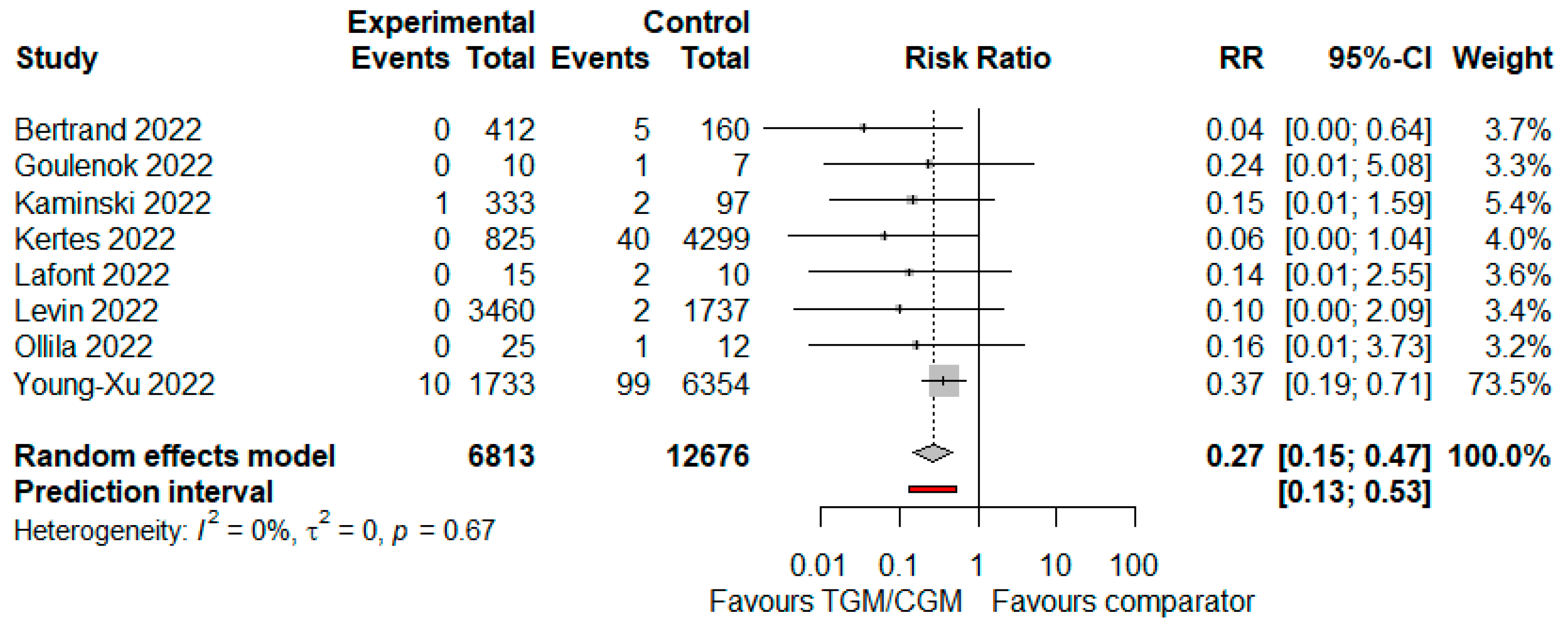
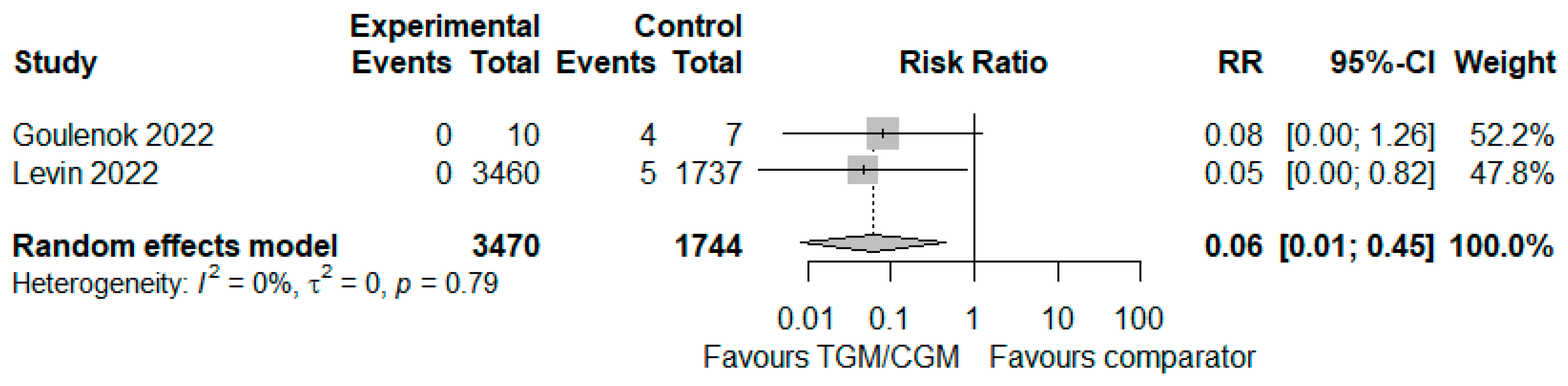
3.4.3. Mortality
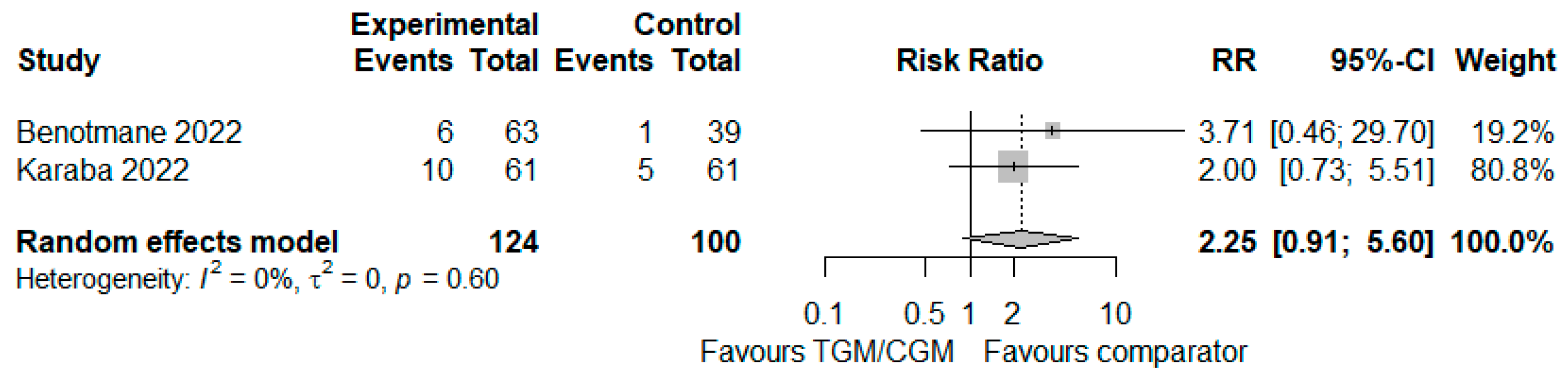
3.4.4. Neutralization of COVID-19 Omicron Variant
3.4.5. Need for Oxygen Therapy
3.4.6. RT-PCR SARS-CoV-2 Positivity
3.4.7. Severity of COVID-19
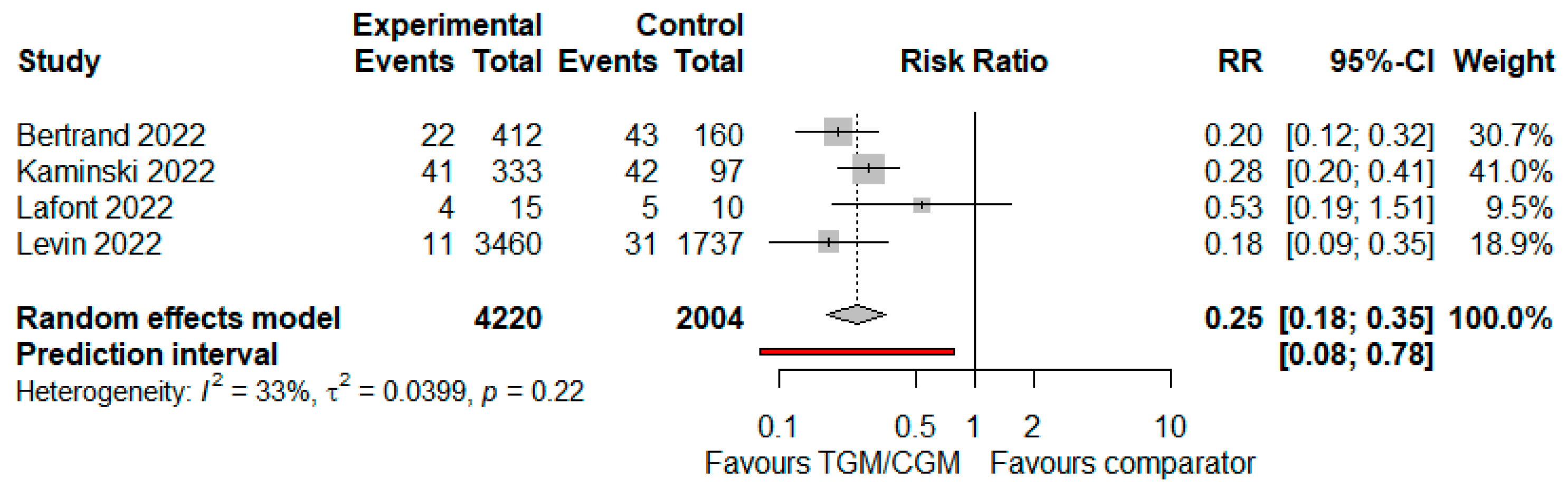
3.4.8. Symptomatic COVID-19
3.5. Safety and Tolerability
4. Discussion
Limitation of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Prendecki, M.; Clarke, C.; Edwards, H.; McIntyre, S.; Mortimer, P.; Gleeson, S.; Martin, P.; Thomson, T.; Randell, P.; Shah, A. Humoral and T-cell responses to SARS-CoV-2 vaccination in patients receiving immunosuppression. Ann. Rheum. Dis. 2021, 80, 1322–1329. [Google Scholar] [CrossRef]
- Rusk, D.S.; Strachan, C.C.; Hunter, B.R. Lack of immune response after mRNA vaccination to SARS-CoV-2 in a solid organ transplant patient. J. Med. Virol. 2021, 93, 5623–5625. [Google Scholar] [CrossRef] [PubMed]
- Belsky, J.A.; Tullius, B.P.; Lamb, M.G.; Sayegh, R.; Stanek, J.R.; Auletta, J.J. COVID-19 in immunocompromised patients: A systematic review of cancer, hematopoietic cell and solid organ transplant patients. J. Infect. 2021, 82, 329–338. [Google Scholar] [CrossRef]
- Dumortier, J.; Duvoux, C.; Roux, O.; Altieri, M.; Barraud, H.; Besch, C.; Caillard, S.; Coilly, A.; Conti, F.; Dharancy, S. COVID-19 in liver transplant recipients: The French SOT COVID registry. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101639. [Google Scholar] [CrossRef] [PubMed]
- Abkhoo, A.; Shaker, E.; Mehrabinejad, M.-M.; Azadbakht, J.; Sadighi, N.; Salahshour, F. Factors predicting outcome in intensive care unit-admitted COVID-19 patients: Using clinical, laboratory, and radiologic characteristics. Crit. Care Res. Pract. 2021, 2021, 9941570. [Google Scholar] [CrossRef] [PubMed]
- Benotmane, I.; Velay, A.; Vargas, G.G.; Olagne, J.; Cognard, N.; Heibel, F.; Braun-Parvez, L.; Martzloff, J.; Perrin, P.; Pszczolinski, R. A rapid decline in the anti-receptor binding domain of the SARS-CoV-2 spike protein IgG titer in kidney transplant recipients after tixagevimab-cilgavimab administration. Kidney Int. 2022, 102, 1188–1190. [Google Scholar] [CrossRef] [PubMed]
- US Food and Drug Administration. Fact Sheet for Healthcare Providers: Emergency Use Authorization for Evusheld (Tixagevimab Co-Packaged with Cilgavimab). Available online: https://www.fda.gov/media/154701/download (accessed on 22 August 2022).
- Wise, J. COVID-19: Evusheld is approved in UK for prophylaxis in immunocompromised people. BMJ 2022, 376, o722. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.J.; Ustianowski, A.; De Wit, S.; Launay, O.; Avila, M.; Templeton, A.; Yuan, Y.; Seegobin, S.; Ellery, A.; Levinson, D.J. Intramuscular AZD7442 (tixagevimab–cilgavimab) for prevention of COVID-19. N. Engl. J. Med. 2022, 386, 2188–2200. [Google Scholar] [CrossRef] [PubMed]
- Al Jurdi, A.; Morena, L.; Cote, M.; Bethea, E.; Azzi, J.; Riella, L.V. Tixagevimab/cilgavimab pre-exposure prophylaxis is associated with lower breakthrough infection risk in vaccinated solid organ transplant recipients during the omicron wave. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2022. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, D.; Laurent, C.; Lemée, V.; Lebourg, L.; Hanoy, M.; Le Roy, F.; Nezam, D.; Pruteanu, D.; Grange, S.; de Nattes, T. Efficacy of anti–SARS-CoV-2 monoclonal antibody prophylaxis and vaccination on the Omicron variant of COVID-19 in kidney transplant recipients. Kidney Int. 2022, 102, 440. [Google Scholar] [CrossRef] [PubMed]
- Kaminski, H.; Gigan, M.; Vermorel, A.; Charrier, M.; Guirle, L.; Jambon, F.; Lacapère, A.; Ménard, C.; Moreau, K.; Neau-Cransac, M. COVID-19 morbidity decreases with Tixagevimab/cilgavimab preexposure prophylaxis in kidney transplant recipients non/low vaccine responders. Kidney Int. 2022, 102, 936–938. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group*, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ott. Ott. Hosp. Res. Inst. 2011, 2, 1–12. [Google Scholar]
- Bazerbachi, F.; Sawas, T.; Vargas, E.J.; Prokop, L.J.; Chari, S.T.; Gleeson, F.C.; Levy, M.J.; Martin, J.; Petersen, B.T.; Pearson, R.K. Metal stents versus plastic stents for the management of pancreatic walled-off necrosis: A systematic review and meta-analysis. Gastrointest. Endosc. 2018, 87, 30–42.e15. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Benotmane, I.; Velay, A.; Gautier-Vargas, G.; Olagne, J.; Obrecht, A.; Cognard, N.; Heibel, F.; Braun-Parvez, L.; Keller, N.; Martzloff, J. Breakthrough COVID-19 cases despite prophylaxis with 150 mg of tixagevimab and 150 mg of cilgavimab in kidney transplant recipients. Am. J. Transplant. 2022, 22, 2675–2681. [Google Scholar] [CrossRef] [PubMed]
- Benotmane, I.; Velay, A.; Vargas, G.G.; Olagne, J.; Thaunat, O.; Fafi-Kremer, S.; Caillard, S. Pre-exposure prophylaxis with 300 mg Evusheld™ elicits limited neutralizing activity against the Omicron variant. Kidney Int. 2022, 102, 442–444. [Google Scholar] [CrossRef]
- Bruel, T.; Hadjadj, J.; Maes, P.; Planas, D.; Seve, A.; Staropoli, I.; Guivel-Benhassine, F.; Porrot, F.; Bolland, W.-H.; Nguyen, Y. Serum neutralization of SARS-CoV-2 Omicron sublineages BA. 1 and BA. 2 in patients receiving monoclonal antibodies. Nat. Med. 2022, 28, 1297–1302. [Google Scholar] [CrossRef]
- Conte, W.L.; Golzarri-Arroyo, L. Tixagevimab and Cilgavimab (Evusheld) boosts antibody levels to SARS-CoV-2 in patients with multiple sclerosis on b-cell depleters. Mult. Scler. Relat. Disord. 2022, 63, 103905. [Google Scholar] [CrossRef]
- Fourati, S.; Robin, C.; Rodriguez, C.; Leclerc, M.; Beckerich, F.; Pawlotsky, J.M.; Redjoul, R.; Maury, S. Breakthrough COVID-19 infections in vaccinated recipients of allogeneic stem cell transplantation. EJHaem 2022, 3, 980–982. [Google Scholar] [CrossRef] [PubMed]
- Goulenok, T.; Delaval, L.; Delory, N.; François, C.; Papo, T.; Descamps, D.; Ferré, V.M.; Sacré, K. Pre-exposure anti-SARS-CoV-2 monoclonal antibodies in severely immunocompromised patients with immune-mediated inflammatory diseases. Lancet Rheumatol. 2022, 4, e458–e461. [Google Scholar] [CrossRef] [PubMed]
- Karaba, A.H.; Kim, J.; Chiang, T.P.-Y.; Alejo, J.L.; Abedon, A.T.; Mitchell, J.; Chang, A.; Eby, Y.; Johnston, T.S.; Aytenfisu, T.Y. Omicron BA. 1 and BA. 2 Neutralizing Activity Following Pre-Exposure Prophylaxis with Tixagevimab plus Cilgavimab in Vaccinated Solid Organ Transplant Recipients. medRxiv 2022. [Google Scholar]
- Kertes, J.; David, S.S.B.; Engel-Zohar, N.; Rosen, K.; Hemo, B.; Kantor, A.; Adler, L.; Stein, N.S.; Reuveni, M.M.; Shahar, A. Association between AZD7442 (tixagevimab-cilgavimab) administration and SARS-CoV-2 infection, hospitalization and mortality. Clin. Infect. Dis. 2022, ciac625. [Google Scholar] [CrossRef]
- Kleiboeker, H.L.; Jorgenson, M.R.; Smith, J.A. Myalgia in liver transplant recipients after receiving tixagevimab/cilgavimab for pre-exposure prophylaxis of COVID-19: A case series. Transpl. Infect. Dis. Off. J. Transplant. Soc. 2022. [Google Scholar] [CrossRef] [PubMed]
- Lafont, E.; Pere, H.; Lebeaux, D.; Cheminet, G.; Thervet, E.; Guillemain, R.; Flahault, A. Targeted SARS-CoV-2 treatment is associated with decreased mortality in immunocompromised patients with COVID-19. J. Antimicrob. Chemother. 2022, 77, 2688–2692. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, Y.; Flahault, A.; Chavarot, N.; Melenotte, C.; Cheminant, M.; Deschamps, P.; Carlier, N.; Lafont, E.; Thomas, M.; Flamarion, E. Pre-exposure prophylaxis with tixagevimab and cilgavimab (Evusheld©) for COVID-19 among 1112 severely immunocompromised patients. Clin. Microbiol. Infect. 2022, 28, 1654.e1–1654.e4. [Google Scholar] [CrossRef]
- Ollila, T.A.; Masel, R.H.; Reagan, J.L.; Lu, S.; Rogers, R.D.; Paiva, K.J.; Taher, R.; Burguera-Couce, E.; Zayac, A.S.; Yakirevich, I. Seroconversion and outcomes after initial and booster COVID-19 vaccination in adults with hematologic malignancies. Cancer 2022, 128, 3319–3329. [Google Scholar] [CrossRef] [PubMed]
- Ordaya, E.E.; Beam, E.; Yao, J.D.; Razonable, R.R.; Vergidis, P. Characterization of Early-Onset Severe Acute Respiratory Syndrome Coronavirus 2 Infection in Immunocompromised Patients Who Received Tixagevimab-Cilgavimab Prophylaxis. In Open Forum Infectious Diseases; Oxford University Press: Oxford, UK, 2022; p. ofac283. [Google Scholar]
- Stuver, R.; Shah, G.L.; Korde, N.S.; Roeker, L.E.; Mato, A.R.; Batlevi, C.L.; Chung, D.J.; Doddi, S.; Falchi, L.; Gyurkocza, B. Activity of AZD7442 (tixagevimab-cilgavimab) against Omicron SARS-CoV-2 in patients with hematologic malignancies. Cancer Cell 2022, 40, 590–591. [Google Scholar] [CrossRef]
- Woopen, C.; Konofalska, U.; Akgün, K.; Ziemssen, T. Case report: Variant-specific pre-exposure prophylaxis of SARS-CoV-2 infection in multiple sclerosis patients lacking vaccination responses. Front. Immunol. 2022, 13, 897748. [Google Scholar] [CrossRef] [PubMed]
- Young-Xu, Y.; Epstein, L.; Marconi, V.C.; Davey, V.; Zwain, G.; Smith, J.; Korves, C.; Cunningham, F.; Bonomo, R.; Ginde, A.A. Tixagevimab/Cilgavimab for Prevention of COVID-19 during the Omicron Surge: Retrospective Analysis of National VA Electronic Data. medRxiv 2022. [Google Scholar] [CrossRef]
- Aqeel, F.; Geetha, D. Tixagevimab and Cilgavimab (Evusheld©) in Rituximab-treated ANCA Vasculitis Patients. Kidney Int. Rep. 2022, 7, 2537–2538. [Google Scholar] [CrossRef] [PubMed]
- Zerbit, J.; Detroit, M.; Meyer, A.; Decroocq, J.; Deau-Fischer, B.; Deschamps, P.; Birsen, R.; Mondesir, J.; Franchi, P.; Miekoutima, E. Patients with Hematological Malignancies Treated with T-Cell or B-Cell Immunotherapy Remain at High Risk of Severe Forms of COVID-19 in the Omicron Era. Viruses 2022, 14, 2377. [Google Scholar] [CrossRef] [PubMed]
- Totschnig, D.; Augustin, M.; Niculescu, I.; Laferl, H.; Jansen-Skoupy, S.; Lehmann, C.; Wenisch, C.; Zoufaly, A. SARS-CoV-2 Pre-Exposure Prophylaxis with Sotrovimab and Tixagevimab/Cilgavimab in Immunocompromised Patients—A Single-Center Experience. Viruses 2022, 14, 2278. [Google Scholar] [CrossRef] [PubMed]
- Ocon, A.J.; Mustafa, S.S. Real-World Experience of Tixagevimab and Cilgavimab (Evusheld) in Rheumatologic Patients on Rituximab. JCR J. Clin. Rheumatol. 2022. [Google Scholar] [CrossRef]
- Najjar-Debbiny, R.; Gronich, N.; Weber, G.; Stein, N.; Saliba, W. Effectiveness of Evusheld in Immunocompromised Patients: Propensity Score-Matched Analysis. Clin. Infect. Dis. 2022. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.A.; Granger, K.; Roubal, K.; Smith, D.; Gaffney, K.J.; McGann, M.; Cendagorta, A.; Thurlapati, A.; Herbst, A.; Hendrickson, L. Efficacy of tixagevimab-cilgavimab in preventing SARS-CoV-2 for patients with B-cell malignancies. Blood 2022. [Google Scholar] [CrossRef]
- Cochran, W.; Salto-Alejandre, S.; Barker, L.; Langlee, J.; Freed, K.; Carter, D.; Bannon, J.; Goddard, D.; Mostafa, H.; Werbel, W. COVID-19 Outcomes in Solid Organ Transplant Recipients Who Received Tixagevimab-cilgavimab Prophylaxis and/or Bebtelovimab Treatment in a Nurse-driven Monoclonal Antibody Program during the Omicron Surge. Transplantation 2022. [Google Scholar] [CrossRef]
- Calabrese, C.; Kirchner, E.; Villa-Forte, A.; Hajj-Ali, R.A.; Moss, B.P.; Fernandez, J.P.; Calabrese, L. Early experience with tixagevimab/cilgavimab pre-exposure prophylaxis in patients with immune-mediated inflammatory disease undergoing B cell depleting therapy and those with inborn errors of humoral immunity. RMD Open 2022, 8, e002557. [Google Scholar] [CrossRef]
- Al-Obaidi, M.M.; Gungor, A.B.; Kurtin, S.E.; Mathias, A.E.; Tanriover, B.; Zangeneh, T.T. The prevention of COVID-19 in high-risk patients using tixagevimab–cilgavimab (Evusheld): Real-world experience at a large academic center. Am. J. Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Pelfrene, E.; Mura, M.; Sanches, A.C.; Cavaleri, M. Monoclonal antibodies as anti-infective products: A promising future? Clin. Microbiol. Infect. 2019, 25, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.C.; Adams, A.C.; Hufford, M.M.; De La Torre, I.; Winthrop, K.; Gottlieb, R.L. Neutralizing monoclonal antibodies for treatment of COVID-19. Nat. Rev. Immunol. 2021, 21, 382–393. [Google Scholar] [CrossRef] [PubMed]
- Zost, S.J.; Gilchuk, P.; Case, J.B.; Binshtein, E.; Chen, R.E.; Nkolola, J.P.; Schäfer, A.; Reidy, J.X.; Trivette, A.; Nargi, R.S. Potently neutralizing and protective human antibodies against SARS-CoV-2. Nature 2020, 584, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Planas, D.; Saunders, N.; Maes, P.; Guivel-Benhassine, F.; Planchais, C.; Buchrieser, J.; Bolland, W.-H.; Porrot, F.; Staropoli, I.; Lemoine, F. Considerable escape of SARS-CoV-2 Omicron to antibody neutralization. Nature 2022, 602, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Funk, T.; Pharris, A.; Spiteri, G.; Bundle, N.; Melidou, A.; Carr, M.; Gonzalez, G.; Garcia-Leon, A.; Crispie, F.; O’Connor, L. Characteristics of SARS-CoV-2 variants of concern B. 1.1. 7, B. 1.351 or P. 1: Data from seven EU/EEA countries, weeks 38/2020 to 10/2021. Eurosurveillance 2021, 26, 2100348. [Google Scholar] [CrossRef] [PubMed]
- Hachmann, N.P.; Miller, J.; Collier, A.-r.Y.; Ventura, J.D.; Yu, J.; Rowe, M.; Bondzie, E.A.; Powers, O.; Surve, N.; Hall, K. Neutralization escape by SARS-CoV-2 Omicron subvariants BA. 2.12. 1, BA. 4, and BA. 5. N. Engl. J. Med. 2022, 387, 86–88. [Google Scholar] [CrossRef] [PubMed]
- Takashita, E.; Yamayoshi, S.; Simon, V.; van Bakel, H.; Sordillo, E.M.; Pekosz, A.; Fukushi, S.; Suzuki, T.; Maeda, K.; Halfmann, P. Efficacy of antibodies and antiviral drugs against omicron BA. 2.12. 1, BA. 4, and BA. 5 subvariants. N. Engl. J. Med. 2022, 387, 468–470. [Google Scholar] [CrossRef] [PubMed]
- Birabaharan, M.; Hill, E.; Begur, M.; Kaelber, D.C.; Martin, T.; Mehta, S.R. Cardiovascular outcomes after tixagevimab and cilgavimab use for pre-exposure prophylaxis against COVID-19: A population-based propensity-matched cohort study. Clin. Infect. Dis. 2022. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Laukkanen, J.A. Incidence of venous and arterial thromboembolic complications in COVID-19: A systematic review and meta-analysis. Thromb. Res. 2020, 196, 27–30. [Google Scholar] [CrossRef]
- Lodigiani, C.; Iapichino, G.; Carenzo, L.; Cecconi, M.; Ferrazzi, P.; Sebastian, T.; Kucher, N.; Studt, J.-D.; Sacco, C.; Bertuzzi, A. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb. Res. 2020, 191, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Piazza, G.; Campia, U.; Hurwitz, S.; Snyder, J.E.; Rizzo, S.M.; Pfeferman, M.B.; Morrison, R.B.; Leiva, O.; Fanikos, J.; Nauffal, V. Registry of arterial and venous thromboembolic complications in patients with COVID-19. J. Am. Coll. Cardiol. 2020, 76, 2060–2072. [Google Scholar] [CrossRef] [PubMed]
- Rabaan, A.A.; Bakhrebah, M.A.; Mutair, A.A.; Alhumaid, S.; Al-Jishi, J.M.; AlSihati, J.; Albayat, H.; Alsheheri, A.; Aljeldah, M.; Garout, M. Systematic review on pathophysiological complications in severe COVID-19 among the non-vaccinated and vaccinated population. Vaccines 2022, 10, 985. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, C.; Park, Y.S.; Piechotta, V.; Chai, K.L.; Estcourt, L.J.; Monsef, I.; Salomon, S.; Wood, E.M.; So-Osman, C.; McQuilten, Z. SARS-CoV-2-neutralising monoclonal antibodies to prevent COVID-19. Cochrane Database Syst. Rev. 2022. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year [Reference], Study Location | Study Design and Setting | Age (Year) | Male, n (%) | Population | Intervention | Control | Time from TGM/CGM Administration to First Episode of Symptomatic COVID-19 (Days) | Outcome | AEs in TGM/CGM and Control Arm | Assessment of Study Risk of Bias (Tool Used; Finding) | Remark |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Al Jurdi et al., 2022 [10], United States | Retrospective cohort; multicenter | Median (IQR), 65 (55–72) | 136 (61.3) | SOTRs | 222 SOTRs received TGM/CGM (IM) TGM/CGM (IM) (150–150 mg dose) (n = 90), TGM/CGM (IM) (300–300 mg dose) (n = 131), and TGM/CGM (IM) (450–450 mg dose) (n = 1) | 222 SOTRs received placebo | Median (IQR), 81 (15–97) | RT-PCR positivity for SARS-CoV-2: positive PCR for SARS-CoV-2 was lower in the TGM/CGM group vs. placebo (11 vs. 32, p < 0.001). SARS-CoV-2 infection was higher in those who received the lower (150–150 mg) dose of TGM/CGM compared to those who received the higher dose of 300–300 mg (p = 0.025). COVID-19-related hospitalization: percentage of patients admitted to hospital was lower among TGM/CGM group vs. placebo group (1 vs. 3, p > 0.05). Mortality: 0 patients allocated to TGM/CGM and 3 patients allocated to placebo died (p > 0.05). | AEs in the TGM/CGM group occurred in 9 SOTRs. Most common AEs were nausea, vomiting, or diarrhea (n = 4), headache (n = 3), and abdominal pain (n = 2). Two patients developed new lung infiltrates with negative infectious evaluation, thought to be pneumonitis. One patient developed a mild heart failure exacerbation, and one developed new atrial fibrillation. | NOS, 8 | Control group had similar characteristics to the TGM/CGM group. |
| Al-Obaidi et al., 2022 [44], United States | Retrospective cohort; single center | Median (IQR), 68 (58–75) | 238 (51.4) | ICHs | 463 ICH participants received TGM/CGM (IM) (300–300 mg dose) | No comparator group | Median (IQR), 48 (27.5–69) | RT-PCR positivity for SARS-CoV-2: 6/98 developed COVID-19. COVID-19-related hospitalization: 42/463 required hospitalization. Mortality: 0 patients died attributed to COVID-19. | No severe AEs were recorded for TGM/CGM in all patients. | NOS, 8 | All patients meeting the criteria for therapy did not have a recent exposure or an acute COVID-19 infection. |
| Aqeel et al., 2022 [36], United States | Retrospective cohort; single center | Mean (SD), 66 (15.5) | Not reported | AAV patients | 20 AVV participants received TGM/CGM (IM) (300–300 mg dose) | No comparator group | 114, 57, and 125 | RT-PCR positivity for SARS-CoV-2: 3/20 developed COVID-19. COVID-19-related hospitalization: 0 patients required hospitalization. Severity of COVID-19: 3 cases were classified as mild disease. | Not reported | NOS, 6 | All patients received the COVID-19 vaccine. |
| Benotmane et al., 2022 [20], France | Retrospective cohort; multicenter | Median (IQR), 60.1 (52.3–71.9) | 23/39 (59) | KTRs | 416 SOTRs received TGM/CGM (IM) (150–150 mg dose) | No comparator group | Median (IQR), 20 (9.5–34.5) | RT-PCR positivity for SARS-CoV-2: 39 patients developed COVID-19. COVID-19-related hospitalization: 14 patients required hospitalization. ICU admission: 3 patients were transferred to ICU. Mortality: 2 patients died of COVID-19-related ARDS. | Not reported | NOS, 6 | Patients who had already received the CRM-IDM combination were not excluded (n = 25). |
| Benotmane et al., 2022 [21], France | Retrospective cohort; multicenter | Not reported | Not reported | KTRs | 63 KTRs received TGM/CGM (IM) (150–150 mg dose) | 39 KTRs received CRM/IDM (IV) (600–600 mg dose) and 14 KTRs were infected with SARS-CoV-2 | Median (IQR), 29 (29–33) | Neutralization of COVID-19 Omicron variant: 6/63 (TGM/CGM), 1/39 (CRM/IDM), and 10/14 (patients who were infected with COVID-19) were able to neutralize Omicron. | Not reported | NOS, 6 | High interindividual variability in the formed neutralizing antibodies was observed in the TGM/CGM group, which was explained largely by the patients’ BMI. |
| Benotmane et al., 2022 [6], France | Retrospective cohort; single center | Median (IQR), 55.5 (50–67.8) | 53 (54) | KTRs | 98 KTRs received TGM/CGM (IM) (150–150 mg dose) | Same KTR patients before receiving TGM/CGM (at baseline) | Not reported | Neutralization of COVID-19 Omicron variant: neutralizing activity decreased from 2.7 log10 to 2.4 log10 between 1 month and month 4–5 following TGM/CGM injection, p = 0.007. | Not reported | NOS, 7 | Seventy-two patients had been previously treated with the CRM/IDM combination before the emergence of the Omicron variant. |
| Bertrand et al., 2022 [11], France | Retrospective cohort; single center | Mean (SD), 60.2 (14.2) | 254 (61.6) | KTRs | 412 KTRs received TGM/CGM (IM) (150–150 mg dose) | 62 KTRs received CRM/IDM (IV) (600–600 mg dose) and 98 KTRs received no mAbs | Not reported | RT-PCR positivity for SARS-CoV-2: positive PCR for SARS-CoV-2 was lower in the TGM/CGM group vs. CRM/IDM and no mAbs group (28 vs. 56, p < 0.001). Symptomatic COVID-19: 22 developed symptomatic COVID-19 in the TGM/CGM group compared to 43 among those who received CRM/IDM or no mAbs (p < 0.001). COVID-19-related hospitalization: percentage of patients admitted to hospital was lower among TGM/CGM group vs. CRM/IDM or no mAbs group (6 vs. 15, p < 0.001). ICU admission: lower number of patients in the TGM/CGM group required ICU admission compared to patients in the CRM/IDM or no mAbs group (2 vs. 6, p = 0.0009). Mortality: 0 patients allocated to TGM/CGM and 5 patients allocated to CRM/IDM or no mAbs died, p = 0.0026. | No severe AEs were recorded for TGM/CGM in all patients. | NOS, 7 | Most patients received CRM/IDM as a 1st step protection (n = 267). |
| Bruel et al., 2022 [22], France | Prospective cohort; multicenter | Median (IQR), 61 (31–92) | 15 (52) | Immunocompromised patients (RA, kidney graft, vasculitis, polychondritis, and SLE) | 29 immunocompromised patients received TGM/CGM (IM) (300–300 mg dose) | No comparator group | Median (IQR), 18 (12.7–22.5) | RT-PCR positivity for SARS-CoV-2: 4 patients developed COVID-19 (all cases were Omicron). Severity of COVID-19: 3 cases were classified as mild disease, whereas 1 case was classified as severe. COVID-19-related hospitalization: 1 patient required hospitalization. | Not reported | NOS, 7 | Most patients (n = 18) were previously treated with CRM/IDM before TGM/CGM administration. |
| Calabrese et al., 2022 [43], United States | Retrospective cohort; multicenter | Median, 64 | 4 (33.3) | IMIDs or IEI patients | 412 IMIDs or IEI patients received TGM/CGM (IM) (150–150 mg dose) (n = 6), TGM/CGM (IM) (300–300 mg dose) (n = 6), and TGM/CGM (IM) dose was not reported (n = 400) | No comparator group | Median (IQR), 19 (13–84) after TGM/ CGM (IM) (150–150 mg dose) and Median (IQR), 38.5 (19–72) after TGM/ CGM (IM) (300–300 mg dose) | RT-PCR positivity for SARS-CoV-2: 12/412 IMIDs and IEI patients developed COVID-19. Severity of COVID-19: eleven patients who developed COVID-19 following TGM/CGM combination were classified as mild and recovered at home. COVID-19-related hospitalization: 1/12 IMID or IEI patients required hospitalization. Mortality: 0 IMID or IEI patients died attributed to COVID-19. | One possible serious AE in a patient with COVID-19 with ITP. | NOS, 8 | All cases who developed a breakthrough SARS-CoV-2 infection had been vaccinated against COVID-19. |
| Cochran et al., 2022 [42], United States | Retrospective cohort; single center | Not reported | Not reported | SOTRs | 205 SOTR patients received TGM/CGM (IM) (150–150 mg dose (n = 14) or 300–300 mg dose (n = 191)) | No comparator group | Not reported | RT-PCR positivity for SARS-CoV-2: percentage of patients with positive SARS-CoV-2 PCR was higher in the TGM/CGM group who received the lower (150–150 mg) dose of TGM/CGM compared to those who received the higher dose of 300–300 mg (4/14 vs. 12/156). COVID-19-related hospitalization: 1/14 in the lower (150–150 mg) dose of TGM/CGM group compared to 2/156 in the higher (300–300 mg) dose of TGM/CGM required hospitalization. Mortality: 1/14 in the lower (150–150 mg) dose of TGM/CGM group compared to 1/156 in the higher (300–300 mg) dose of TGM/CGM died due to COVID-19. | 5/205 developed cardiac events due to TGM/CGM combination: one event was an atrial fibrillation and other events were pericarditis, recurrent atrial flutter, mild/moderate cardiac allograft rejection, and complete heart block in a patient with history of LBBB. | NOS, 8 | SOTRs received TGM/CGM during the period corresponding to the peak of the BA.2 and BA.5 (Omicron) wave in their region. |
| Conte et al., 2022 [23], United States | Retrospective cohort; single center | Median (IQR), 50 (27–72) | 8 (44.4) | MS patients treated with OCR/OFA | 18 MS patients received TGM/CGM (IM) (150–150 mg dose) | Same MS patients before receiving TGM/CGM (at baseline) | Mean, 14 | Antibody level: all patients had antibody level >250 U/mL. At baseline there were 12 patients lower than 0.8 U/mL and 6 higher than the threshold. After TGM/CGM, all 18 subjects were above the threshold (p < 0.001). | Not reported | NOS, 6 | Study was completed prior to the FDA’s update to 300 mg each of TGM/CGM. |
| Davis et al., 2022 [41], United States | Retrospective cohort; single center | Median (IQR), 66 (18–91) | 149 (59) | B-cell malignancies patients [CLL, DLBCL and MM] | 251 B-cell malignancy patients received TGM/CGM (IM) (150–150 mg dose (n = 14) or 300–300 mg dose (n = 237)) | No comparator group | Median (IQR), 91 (3–162) | RT-PCR positivity for SARS-CoV-2: 27/251 developed COVID-19. COVID-19-related hospitalization: 4/27 had severe COVID-19 and required hospitalization. Mortality: 0 patients allocated to TGM/CGM combination died. | Two patients experienced diarrhea and rash. One patient with a history of epilepsy experienced a self-resolving seizure. | NOS, 8 | Twenty-three infections occurred when Omicron variant BA.5 was dominant among the local population. |
| Fourati et al., 2022 [24], France | Retrospective case reports; single center | 59 and 69 | 1 (33.3) | HSCTRs | 3 HSCTR patients received TGM/CGM (IM) (150–150 mg dose) | No comparator group | 9 and 11 | RT-PCR positivity for SARS-CoV-2: 2/3 developed COVID-19 (both cases were Omicron). Symptomatic COVID-19: 2/3 developed symptomatic COVID-19 in the TGM/CGM group. Severity of COVID-19: 2/3 who developed COVID-19 following TGM/CGM combination were classified as mild. COVID-19-related hospitalization: 2/3 required hospitalization. | Not reported | Modified NOS, moderate | Patients had a medical history of AML. |
| Goulenok et al., 2022 [25], France | Retrospective case-series; single center | Median (IQR), 52 (19–75) | 4 (40) | IMIDs patients (AIDs and systemic vasculitis) | 10 severely immunocompromised patients received TGM/CGM (IM) (150–150 mg dose) | 7 severely immunocompromised patients received no mAbs | 21 | RT-PCR positivity for SARS-CoV-2: positive PCR for SARS-CoV-2 was lower in the TGM/CGM group vs. no mAbs group (1 (Omicron, n = 1) vs. 7 (Omicron, n = 6 and Delta, n = 1)). Severity of COVID-19: severity of SARS-CoV-2 infection was lower in the TGM/CGM group compared to no mAbs group (0 vs. 4). COVID-19-related hospitalization: hospital admission was lower among TGM/CGM group vs. no mAbs group (0 vs. 5). Need for oxygen therapy: oxygen therapy requirement was lower among TGM/CGM group vs. no mAbs group (0 vs. 4). Mortality: 0 patients allocated to TGM/CGM and 1 patient allocated to no mAbs died. | No severe AEs were recorded for TGM/CGM in all patients. | Modified NOS, high | The sample size was small, and the study was conducted at a single center. |
| Kaminski et al., 2022 [12], France | Retrospective cohort; single center | Mean (SD), 60 (14.4) | 204 (61.2) | KTRs | 333 KTRs received TGM/CGM (IM) (150–150 mg dose) | 97 KTRs received placebo | Not reported | Symptomatic COVID-19: 41 developed symptomatic COVID-19 in the TGM/CGM group compared to 42 among those who received placebo (HR 0.011 [CI 95% 0.063–0.198]; p < 0.001). COVID-19-related hospitalization: hospital admission was lower among TGM/CGM group vs. placebo group (4 vs. 11, HR 0.046 [CI 95% 0.013–0.158]; p < 0.001). ICU admission: ICU admission in the TGM/CGM group was lower compared to patients in the placebo group (2 vs. 6, HR 0.045 [CI 95% 0.008–0.240]; p < 0.001). Mortality: 1 patient allocated to TGM/CGM and 2 patients allocated to placebo died [HR 0.076 (CI 95% 0.005–1.161); p = 0.066]. | Not reported | NOS, 7 | KTRs received TGM/CGM during the period corresponding to the peak of the Omicron wave in their region. Some patients (TGM/CGM group: n = 137 and placebo group: n = 43) were previously treated with CRM-IDM. |
| Karaba et al., 2022 [26], United States | Prospective cohort; single center | 62.5 (57.7–68.5) | 25 (41) | SOTRs (KTRs, HTRs, and LTRs) | 61 SOTRs received: TGM/CGM (IM) (300–300 mg dose) | Same SOTRs patients before receiving TGM/CGM (at baseline) | Not reported | Neutralization of COVID-19 Omicron variant: proportion of patients who received TGM/CGM exhibited higher neutralizing inhibition against the Omicron compared to the pre-TGM/CGM patients’ group (10/61 vs. 5/61, p = 0.06). | Reported reactions were mild or moderate and were more frequent after 300–300 mg dosing vs. 150–150 mg dosing. | NOS, 6 | Patients received SARS-CoV-2 vaccines before receiving TGM/CGM as a 1st step protection. |
| Kertes et al., 2022 [27], Israel | Retrospective cohort; multicenter | TGM/CGM group: 40–59 (29.9%), 60–69 (28.6%), and 70–79 (30.5) | 512 (62.1) | Immunocompromised patients | 825 immunocompromised patients received TGM/CGM (IM) (150–150 mg dose) | 4299 immunocompromised patients received no treatment | Not reported | RT-PCR positivity for SARS-CoV-2: positive PCR for SARS-CoV-2 was lower in the TGM/CGM group vs. the non-TGM/CGM group (29 vs. 308, p < 0.001, (OR: 0.51, 95% CI: 0.30–0.84)). COVID-19-related hospitalization: percentage of patients admitted to hospital was lower among TGM/CGM group vs. the non-TGM/CGM group (1 vs. 27, p = 0.07; (OR: 0.08, 95% CI: 0.01–0.54)). Mortality: 0 patients allocated to TGM/CGM and 40 patients allocated to the non-TGM/CGM died, p = 0.005. | Not reported | NOS, 6 | TGM/CGM group was more likely to have CVD, diabetes, HTN and CKD, and more likely to have been vaccinated against COVID-19 than those who never received TGM/CGM. |
| Kleiboeker et al., 2022 [28], United States | Retrospective case-series, single center | Median (IQR), 54 (52–54) | 2 (66.7) | LTRs | 77 LTRs received: TGM/CGM (IM) (150–150 mg dose) | No comparator group | 1, 0, and 29 | Not reported | In the TGM/CGM group, patients had myalgia (n = 3), arthralgia (n = 2), fatigue (n = 2), nausea and vomiting (n = 1), diarrhea (n = 1), intermittent fevers (n = 1), chills (n = 1), and malaise (n = 1). | Modified NOS, high | In the same cohort, 139 kidney and 101 liver transplant recipients received TGM/CGM without any reports of myalgia. |
| Lafont et al., 2022 [29], France | Retrospective case-series; single center | Median (IQR), 56 (44–63) | 8 (53) | Immunocompromised patients | 15 immunocompromised patients received TGM/CGM (IM) (150–150 mg dose) | 10 immunocompromised patients received no treatment | Not reported | Asymptomatic COVID-19: 2 developed asymptomatic COVID-19 in the TGM/CGM group compared to 2 among those who received no treatment. Symptomatic COVID-19: 4 and 4 developed fever and dyspnea in the TGM/CGM group compared to 5 and 3 in the no treatment group; however, cough prevalence was the same in both groups (6 vs. 9). Need for oxygen therapy: lower number required oxygen in the TGM/CGM group compared to the no treatment group (2 vs. 3). COVID-19-related hospitalization: percentage of patients admitted to hospital was lower among TGM/CGM group vs. no treatment group (3 vs. 3). ICU admission: lower number of patients in the TGM/CGM group required ICU admission compared to patients in the no treatment group (1 vs. 2). Mortality: 0 patients allocated to TGM/CGM and 2 patients allocated to no treatment died. | Not reported | Modified NOS, high | Most patients in the TGM/CGM group received at least 3 doses of SARS-CoV-2 vaccines or CRM/IDM. |
| Levin et al., 2022 [9], Multicounty | Randomized double-blind controlled trial; multicenter | Mean (SD), 53.6 (15) | 1865 (53.9) | Immunocompromised patients | 3460 patients received TGM/CGM (IM) (150–150 mg dose) | 1737 patients received placebo (IM) 1.5 mL injections consecutively | Not reported | RT-PCR positivity for SARS-CoV-2: positive PCR for SARS-CoV-2 was lower in the TGM/CGM group vs. placebo (8/3441 vs. 17/1731, RRR (95% CI) = 76.7 (46 to 90); p < 0.001). Severity of COVID-19: number of patients with severe or critical COVID-19 illness was lower in the TGM/CGM group vs. placebo (0/3441 vs. 5/1731). Mortality: 0 patients allocated to TGM/CGM and 2 patients allocated to placebo treatment died. Symptomatic COVID-19: 11 developed symptomatic COVID-19 in the TGM/CGM group compared to 31 among those who received placebo. | Most AEs were mild (761 vs. 369) or moderate (387 vs. 191) in intensity. Incidence of serious AEs was similar in the two groups (64 vs. 27). Most common AE was injection site reaction: n = 82 in the TGM/CGM group compared to n = 36 in the placebo group. | RoB 2, low risk of bias | SARS-CoV-2 variants: in the TGM/CGM group, 1 participant was infected with a SARS-CoV-2 B.1.351 (beta) variant, while 10 participants in the placebo group (5 participants with B.1.1.7_1 (an alpha subvariant) and 5 participants with B.1.617.2 (Delta)). |
| Najjar-Debbiny et al., 2022 [40], Israel | Retrospective cohort; multicenter | Mean (SD), 66.2 (13.7) | 402 (57.2) | Immunocompromised patients | 703 immunocompromised patients received TGM/CGM (IM) (150–150 mg dose) | 2812 immunocompromised patients received no TGM/CGM | Not reported | RT-PCR positivity for SARS-CoV-2: positive PCR for SARS-CoV-2 was lower in the TGM/CGM group vs. the non-TGM/CGM group (72 vs. 377, HR 0.75 [CI 95% 0.58–0.96]; p = 0.02). COVID-19-related hospitalization: percentage of patients who needed hospitalization due to COVID-19 was lower in the TGM/CGM group vs. the non-TGM/CGM group (7 vs. 67, HR 0.41 (CI 95% 0.19–0.89); p = 0.045). | Not reported | NOS, 8 | Patients in the TGM/CGM group were matched by propensity score to patients in the non-TGM/CGM group (controls) in a 1:4 ratio. |
| Nguyen et al., 2022 [30], France | Retrospective cohort; multicenter | Mean (SD), 58.9 (20.7) | Not reported | Immunocompromised patients (SOTRs, hematologic malignancies, immunosuppressants, or IEI) | 1112 immunocompromised patients received TGM/CGM (IM) (150–150 mg dose) | No comparator group | Median (IQR), 21 (13–36) | RT-PCR positivity for SARS-CoV-2: 49 patients had confirmed infection (29/49 patients were Omicron). Severity of COVID-19: 43/49 cases were classified as mild disease, whereas 6/49 cases were classified as moderate to severe. COVID-19-related hospitalization: 10/49 patients required hospitalization. Need for oxygen therapy: 6/49 patients required oxygen therapy. Non-invasive ventilation: 2/49 patients required non-invasive ventilation. Mortality: 2/49 patients died. | Not reported | NOS, 7 | Patients with confirmed SARS-CoV-2 infection < 5 days following TGM/CGM administration were excluded from the analyses. |
| Ocon et al., 2022 [39], United States | Retrospective cohort; single center | Mean (SD), 59 (15) | 13 (30.2) | SARD patients (RA, AAV, other vasculitis, immune-mediated myositis, Sjögren disease, and SLE) | 43 SARD patients received TGM/CGM (IM) (150–150 mg dose (n = 5) or 300–300 mg dose (n = 38)) | No comparator group | Not reported | RT-PCR positivity for SARS-CoV-2: 1/43 patients developed COVID-19. COVID-19-related hospitalization: 0 SARD patients required hospitalization. | Reported AEs included myalgia (n = 3), flu-like symptoms (n = 2), fever (n = 2), injection site pain (n = 1), and/or headache (n = 1). | NOS, 8 | Thirty-five SARD patients had received SARS-CoV-2 vaccinations before receiving TGM/GM. |
| Ollila et al., 2022 [31], United States | Retrospective cohort; single center | Not reported | Not reported | Hematologic malignancy patients | 25 hematologic malignancy patients received TGM/CGM (IM) (150–150 mg dose) | 12 hematologic malignancies patients received no treatment | Not reported | RT-PCR positivity for SARS-CoV-2: positive PCR for SARS-CoV-2 was lower in the TGM/CGM group vs. the non-TGM/CGM group (0 vs. 3, p = 0.007). Mortality: 0 patients allocated to TGM/CGM and 1 patient allocated to no treatment died. | Not reported | NOS, 6 | Hematologic malignancy patients included any type of lymphoid, myeloid, or plasma cell malignancy. |
| Ordaya et al., 2022 [32], United States | Retrospective case-series; single center | Median (IQR), 57 (28.7–71.5) | 2 (25) | Immunocompromised patients (hematological malignancies, AIDs, SOTRs, HSCTRs, and other immunocompromising conditions) | 674 immunocompromised patients received TGM/CGM (IM) (150–150 mg dose) | No comparator group | Median (IQR), 2.5 (1–7) | RT-PCR positivity for SARS-CoV-2: 8 patients developed COVID-19 (one case was Omicron). Severity and asymptomatic COVID-19: 6 cases were classified as mild disease, whereas 2 cases were classified as asymptomatic. Mortality: none of the 8 patients who developed COVID-19 following TGM/CGM combination died. Need for oxygen therapy: 1/8 patients required oxygen therapy. COVID-19-related hospitalization: 2/8 patients required hospitalization. | Not reported | Modified NOS, high | Seven patients had received COVID-19 vaccines. |
| Stuver et al., 2022 [33], United States | Prospective cohort; single center | Median (IQR), 62 (35–89) | Not reported | Hematologic malignancy patients | 52 hematologic malignancy patients received TGM/CGM (IM) (150–150 mg dose (n = 30) or 300–300 mg dose (n = 22)) | No comparator group | 8 and 30 | Neutralization of COVID-19 Omicron variant: plasma from 10/22 patients who received TGM/CGM 300 mg dose achieved significantly higher neutralization of Omicron-RBD (p = 0.003) compared to single TGM/CGM 150 mg dose patients. RT-PCR positivity for SARS-CoV-2: 2 patients developed COVID-19 (both had received a single TGM/CGM 150 mg dose). Mortality: neither of the 2 patients who developed COVID-19 following TGM/CGM combination died. COVID-19-related hospitalization: neither of the 2 patients who developed COVID-19 following TGM/CGM combination required hospitalization. Severity of COVID-19: both patients who developed COVID-19 following TGM/CGM combination were classified as symptomatic. | Not reported | NOS, 7 | Most common diagnosis was non-Hodgkin lymphoma. Nearly one-half were HSCTRs or received prior chimeric antigen receptor T cell therapy. |
| Totschnig et al., 2022 [38], Austria | Prospective cohort; single center | Mean (SD), 59.6 (15.1) | 53 (59.5) | Immunocompromised patients (hematologic malignancy, AIDs, MS, IEIs, and SOTRs) | 89 immunocompromised patients received TGM/CGM (IM) (150–150 mg dose) | No comparator group | Median, 40 | Antibody level: median antibody values 1 and 3 months after TGM/CGM were 3965 (p < 0.0001) and 1647 (p = 0.0007) binding antibody units/mL, respectively. RT-PCR positivity for SARS-CoV-2: 2/13 patients developed COVID-19. COVID-19-related hospitalization: 1/13 patients required hospitalization. Need for oxygen therapy: 0 patients required oxygen therapy. | Not reported | NOS, 8 | Patients had been vaccinated against SARS-CoV-2 with a mean dose frequency of 3.7 times, mostly with mRNA vaccines. |
| Woopen et al., 2022 [34], Germany | Retrospective case-series; single center | Median (IQR), 58.5 (48.5–64.2) | 4 (66.7) | MS patients | 6 MS patients received TGM/CGM (IM) (150–150 mg dose) | No comparator group | No case developed COVID-19 | RT-PCR positivity for SARS-CoV-2: 0/6 patients developed COVID-19 | No severe AEs were recorded for TGM/CGM in all patients. | Modified NOS, high | Six MS patients had received SARS-CoV-2 vaccines before start of TGM/CGM. |
| Young-Xu et al., 2022 [35], United States | Retrospective cohort; multicenter | Mean (SD), 67.4 (11) | 1579 (91) | Immunocompromised patients (cancer, immunosuppressants, immunocompromised, and renal disease) | 1733 immunocompromised patients received TGM/CGM (IM) (150–150 mg dose) | 6354 immunocompromised patients received placebo | Not reported | RT-PCR positivity for SARS-CoV-2: positive PCR for SARS-CoV-2 was lower in the TGM/CGM group vs. placebo (6 vs. 69, (HR 0.34; 95% CI, 0.13–0.87)). COVID-19-related hospitalization: percentage of patients admitted to hospital was lower among TGM/CGM group vs. placebo group (1 vs. 38, (HR 0.13; 95% CI, 0.02–0.99)). Mortality: 10 patients allocated to TGM/CGM and 99 patients allocated to placebo died (HR 0.36; 95%CI, 0.18–0.73). | Not reported | NOS, 8 | A small proportion of patients who received TGM/CGM were not immunocompromised. |
| Zerbit et al., 2022 [37], France | Prospective cohort; single center | Median (IQR), 71 (63–78) | 36/57 (63) | Hematologic malignancy patients | 102 hematologic malignancy patients received TGM/CGM (IM) (150–150 mg dose) | 236 hematologic malignancy patients received no TGM/CGM | Not reported | RT-PCR positivity for SARS-CoV-2: positive PCR for SARS-CoV-2 was lower in the TGM/CGM group vs. the non-TGM/CGM group (5/102 vs. 52/236, p < 0.05). | Not reported | NOS, 8 | Proportion of COVID-19 patients who were hospitalized was not different between those who received TGM/CGM or not. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhumaid, S.; Al Mutair, A.; Alali, J.; Al Dossary, N.; Albattat, S.H.; Al HajjiMohammed, S.M.; Almuaiweed, F.S.; AlZaid, M.R.; Alomran, M.J.; Alqurini, Z.S.; et al. Efficacy and Safety of Tixagevimab/Cilgavimab to Prevent COVID-19 (Pre-Exposure Prophylaxis): A Systematic Review and Meta-Analysis. Diseases 2022, 10, 118. https://doi.org/10.3390/diseases10040118
Alhumaid S, Al Mutair A, Alali J, Al Dossary N, Albattat SH, Al HajjiMohammed SM, Almuaiweed FS, AlZaid MR, Alomran MJ, Alqurini ZS, et al. Efficacy and Safety of Tixagevimab/Cilgavimab to Prevent COVID-19 (Pre-Exposure Prophylaxis): A Systematic Review and Meta-Analysis. Diseases. 2022; 10(4):118. https://doi.org/10.3390/diseases10040118
Chicago/Turabian StyleAlhumaid, Saad, Abbas Al Mutair, Jalal Alali, Nourah Al Dossary, Sami Hussain Albattat, Sarah Mahmoud Al HajjiMohammed, Fatimah Saad Almuaiweed, Maryam Radhi AlZaid, Mohammed Jaber Alomran, Zainab Sabri Alqurini, and et al. 2022. "Efficacy and Safety of Tixagevimab/Cilgavimab to Prevent COVID-19 (Pre-Exposure Prophylaxis): A Systematic Review and Meta-Analysis" Diseases 10, no. 4: 118. https://doi.org/10.3390/diseases10040118