

Are Drugs Associated with Microscopic Colitis? A Systematic Review and Meta-Analysis
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Methods
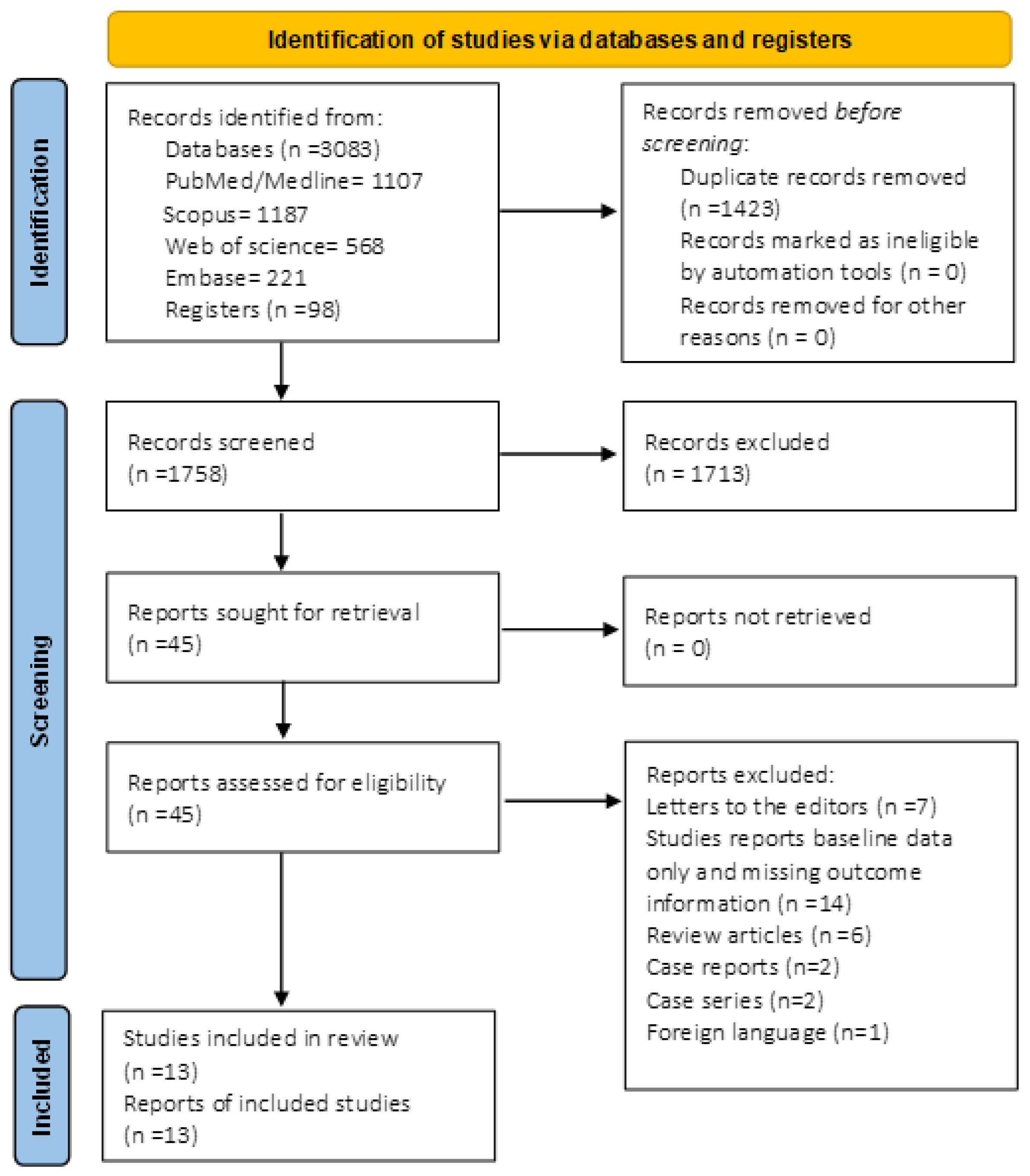
2.1. Data Search and Screening
2.2. Eligibility Criteria and Study Selection
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Search Results and Study Characteristics
3.2. Pooled Odds of MC in Patients Taking PPIs and Subgroup Analysis Based on Control Groups
3.3. Pooled Odds of MC in Patients Taking SSRIs and Subgroup Analysis Based on Control Groups
3.4. Pooled Odds of MC in Patients Taking NSAIDs and Subgroup Analysis Based on Control Groups
3.5. Pooled Odds of MC in Patients Taking Statins with Subgroup Analysis of Diarrhea versus Random Controls
3.6. Pooled Odds of MC in Patients Taking H2RA and Subgroup Analysis Based on Control Groups
3.7. Subgroup Analysis on the Association of LC and CC with the Use of PPIs and NSAIDs
4. Quality Assessment
5. Publication Bias
6. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miehlke, S.; Verhaegh, B.; Tontini, G.E.; Madisch, A.; Langner, C.; Munch, A. Microscopic colitis: Pathophysiology and clinical management. Lancet Gastroenterol. Hepatol. 2019, 4, 305–314. [Google Scholar] [CrossRef]
- Miehlke, S.; Guagnozzi, D.; Zabana, Y.; Tontini, G.E.; Kanstrup Fiehn, A.M.; Wildt, S.; Bohr, J.; Bonderup, O.; Bouma, G.; D’Amato, M.; et al. European guidelines on microscopic colitis: United European Gastroenterology and European Microscopic Colitis Group statements and recommendations. United Eur. Gastroenterol. J. 2021, 9, 13–37. [Google Scholar] [CrossRef]
- Tome, J.; Sehgal, K.; Kamboj, A.K.; Harmsen, W.S.; Kammer, P.P.; Loftus, E.V., Jr.; Tremaine, W.J.; Khanna, S.; Pardi, D.S. The Epidemiology of Microscopic Colitis in Olmsted County, Minnesota: Population-Based Study from 2011 to 2019. Clin. Gastroenterol. Hepatol. 2022, 20, 1085–1094. [Google Scholar] [CrossRef]
- Gentile, N.M.; Khanna, S.; Loftus, E.V., Jr.; Smyrk, T.C.; Tremaine, W.J.; Harmsen, W.S.; Zinsmeister, A.R.; Kammer, P.P.; Pardi, D.S. The epidemiology of microscopic colitis in Olmsted County from 2002 to 2010: A population-based study. Clin. Gastroenterol. Hepatol. 2014, 12, 838–842. [Google Scholar] [CrossRef] [Green Version]
- Andrews, C.N.; Beck, P.L.; Wilsack, L.; Urbanski, S.J.; Storr, M. Evaluation of endoscopist and pathologist factors affecting the incidence of microscopic colitis. Can. J. Gastroenterol. 2012, 26, 515–520. [Google Scholar] [CrossRef]
- Pardi, D.S. Diagnosis and Management of Microscopic Colitis. Am. J. Gastroenterol. 2017, 112, 78–85. [Google Scholar] [CrossRef]
- Rasmussen, M.A.; Munck, L.K. Systematic review: Are lymphocytic colitis and collagenous colitis two subtypes of the same disease-microscopic colitis? Aliment. Pharmacol. Ther. 2012, 36, 79–90. [Google Scholar] [CrossRef]
- Sandler, R.S.; Keku, T.O.; Woosley, J.T.; Galanko, J.A.; Peery, A.F. Medication use and microscopic colitis. Aliment. Pharmacol. Ther. 2021, 54, 1193–1201. [Google Scholar] [CrossRef]
- Zylberberg, H.M.; Kamboj, A.K.; De Cuir, N.; Lane, C.M.; Khanna, S.; Pardi, D.S.; Lebwohl, B. Medication use and microscopic colitis: A multicentre retrospective cohort study. Aliment. Pharmacol. Ther. 2021, 53, 1209–1215. [Google Scholar] [CrossRef]
- Bohr, J.; Wickbom, A.; Hegedus, A.; Nyhlin, N.; Hultgren Hornquist, E.; Tysk, C. Diagnosis and management of microscopic colitis: Current perspectives. Clin. Exp. Gastroenterol. 2014, 7, 273–284. [Google Scholar]
- Fernandez-Banares, F.; Esteve, M.; Espinos, J.C.; Rosinach, M.; Forne, M.; Salas, A.; Viver, J.M. Drug consumption and the risk of microscopic colitis. Am. J. Gastroenterol. 2007, 102, 324–330. [Google Scholar] [CrossRef]
- Guagnozzi, D.; Lucendo, A.J.; Angueira, T.; Gonzalez-Castillo, S.; Tenias, J.M. Drug consumption and additional risk factors associated with microscopic colitis: Case-control study. Rev. Esp. Enferm. Dig. 2015, 107, 347–353. [Google Scholar]
- Keszthelyi, D.; Jansen, S.V.; Schouten, G.A.; de Kort, S.; Scholtes, B.; Engels, L.G.; Masclee, A.A. Proton pump inhibitor use is associated with an increased risk for microscopic colitis: A case-control study. Aliment. Pharmacol. Ther. 2010, 32, 1124–1128. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Fernandez-Banares, F.; de Sousa, M.R.; Salas, A.; Beltran, B.; Piqueras, M.; Iglesias, E.; Gisbert, J.P.; Lobo, B.; Puig-Divi, V.; Garcia-Planella, E.; et al. Epidemiological risk factors in microscopic colitis: A prospective case-control study. Inflamm. Bowel Dis. 2013, 19, 411–417. [Google Scholar]
- Bonderup, O.K.; Fenger-Gron, M.; Wigh, T.; Pedersen, L.; Nielsen, G.L. Drug exposure and risk of microscopic colitis: A nationwide Danish case-control study with 5751 cases. Inflamm. Bowel Dis. 2014, 20, 1702–1707. [Google Scholar] [CrossRef]
- Mohammed, A.; Ghoneim, S.; Paranji, N.; Waghray, N. Quantifying risk factors for microscopic colitis: A nationwide, retrospective cohort study. Indian J. Gastroenterol. 2022, 41, 181–189. [Google Scholar] [CrossRef]
- Verhaegh, B.P.; de Vries, F.; Masclee, A.A.; Keshavarzian, A.; de Boer, A.; Souverein, P.C.; Pierik, M.J.; Jonkers, D.M. High risk of drug-induced microscopic colitis with concomitant use of NSAIDs and proton pump inhibitors. Aliment. Pharmacol. Ther. 2016, 43, 1004–1013. [Google Scholar] [CrossRef] [Green Version]
- Weimers, P.; Vedel Ankersen, D.; Lophaven, S.N.; Bonderup, O.K.; Munch, A.; Lynge, E.; Lokkegaard, E.C.L.; Munkholm, P.; Burisch, J. Microscopic Colitis in Denmark: Regional Variations in Risk Factors and Frequency of Endoscopic Procedures. J. Crohns Colitis 2022, 16, 49–56. [Google Scholar] [CrossRef]
- Bonderup, O.K.; Nielsen, G.L.; Dall, M.; Pottegard, A.; Hallas, J. Significant association between the use of different proton pump inhibitors and microscopic colitis: A nationwide Danish case-control study. Aliment. Pharmacol. Ther. 2018, 48, 618–625. [Google Scholar] [CrossRef] [Green Version]
- Masclee, G.M.; Coloma, P.M.; Kuipers, E.J.; Sturkenboom, M.C. Increased risk of microscopic colitis with use of proton pump inhibitors and non-steroidal anti-inflammatory drugs. Am. J. Gastroenterol. 2015, 110, 749–759. [Google Scholar] [CrossRef]
- Pascua, M.F.; Kedia, P.; Weiner, M.G.; Holmes, J.; Ellenberg, J.; Lewis, J.D. Microscopic colitis and Medication Use. Clin. Med. Insights Gastroenterol. 2010, 2010, 11–19. [Google Scholar] [CrossRef] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Imhann, F.; Bonder, M.J.; Vich Vila, A.; Fu, J.; Mujagic, Z.; Vork, L.; Tigchelaar, E.F.; Jankipersadsing, S.A.; Cenit, M.C.; Harmsen, H.J.; et al. Proton pump inhibitors affect the gut microbiome. Gut 2016, 65, 740–748. [Google Scholar] [CrossRef] [Green Version]
- Lewis, S.J.; Franco, S.; Young, G.; O’Keefe, S.J. Altered bowel function and duodenal bacterial overgrowth in patients treated with omeprazole. Aliment. Pharmacol. Ther. 1996, 10, 557–561. [Google Scholar] [CrossRef]
- Mullin, J.M.; Gabello, M.; Murray, L.J.; Farrell, C.P.; Bellows, J.; Wolov, K.R.; Kearney, K.R.; Rudolph, D.; Thornton, J.J. Proton pump inhibitors: Actions and reactions. Drug Discov. Today 2009, 14, 647–660. [Google Scholar] [CrossRef]
- Law, E.H.; Badowski, M.; Hung, Y.T.; Weems, K.; Sanchez, A.; Lee, T.A. Association Between Proton Pump Inhibitors and Microscopic Colitis. Ann. Pharmacother. 2017, 51, 253–263. [Google Scholar] [CrossRef]
- Gleeson, M.H.; Davis, A.J. Non-steroidal anti-inflammatory drugs, aspirin and newly diagnosed colitis: A case-control study. Aliment. Pharmacol. Ther. 2003, 17, 817–825. [Google Scholar] [CrossRef]
- Keszthelyi, D.; Penders, J.; Masclee, A.A.; Pierik, M. Is microscopic colitis a drug-induced disease? J. Clin. Gastroenterol. 2012, 46, 811–822. [Google Scholar] [CrossRef]
- Aktunc, E.; Kayhan, B.; Arasli, M.; Gun, B.D.; Barut, F. The effect of atorvastatin and its role on systemic cytokine network in treatment of acute experimental colitis. Immunopharmacol. Immunotoxicol. 2011, 33, 667–675. [Google Scholar] [CrossRef]
- Guimbaud, R.; Bertrand, V.; Chauvelot-Moachon, L.; Quartier, G.; Vidon, N.; Giroud, J.P.; Couturier, D.; Chaussade, S. Network of inflammatory cytokines and correlation with disease activity in ulcerative colitis. Am. J. Gastroenterol. 1998, 93, 2397–2404. [Google Scholar] [CrossRef] [PubMed]
- El-Salhy, M.; Gundersen, D.; Hatlebakk, J.G.; Hausken, T. High densities of serotonin and peptide YY cells in the colon of patients with lymphocytic colitis. World J. Gastroenterol. 2012, 18, 6070–6075. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y.; Camilleri, M. Serotonin: A mediator of the brain-gut connection. Am. J. Gastroenterol. 2000, 95, 2698–2709. [Google Scholar] [CrossRef]
- Khan, W.I.; Ghia, J.E. Gut hormones: Emerging role in immune activation and inflammation. Clin. Exp. Immunol. 2010, 161, 19–27. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarar, Z.I.; Farooq, U.; Gandhi, M.; Kamal, F.; Tarar, M.F.; Tahan, V.; Chela, H.K.; Daglilar, E. Are Drugs Associated with Microscopic Colitis? A Systematic Review and Meta-Analysis. Diseases 2023, 11, 6. https://doi.org/10.3390/diseases11010006
Tarar ZI, Farooq U, Gandhi M, Kamal F, Tarar MF, Tahan V, Chela HK, Daglilar E. Are Drugs Associated with Microscopic Colitis? A Systematic Review and Meta-Analysis. Diseases. 2023; 11(1):6. https://doi.org/10.3390/diseases11010006
Chicago/Turabian StyleTarar, Zahid Ijaz, Umer Farooq, Mustafa Gandhi, Faisal Kamal, Moosa Feroze Tarar, Veysel Tahan, Harleen Kaur Chela, and Ebubekir Daglilar. 2023. "Are Drugs Associated with Microscopic Colitis? A Systematic Review and Meta-Analysis" Diseases 11, no. 1: 6. https://doi.org/10.3390/diseases11010006