
Safety and Efficacy of Convalescent Plasma Combined with Other Pharmaceutical Agents for Treatment of COVID-19 in Hospitalized Patients: A Systematic Review and Meta-Analysis

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Literature Search
2.2. Types of Studies, Participants, Interventions and Outcome Measures Included
2.3. Quality Assessment
2.4. Statistical Analysis
3. Results
3.1. Study Flow Diagram
3.2. Study Characteristics
3.3. Mortality Outcome
3.4. Safety
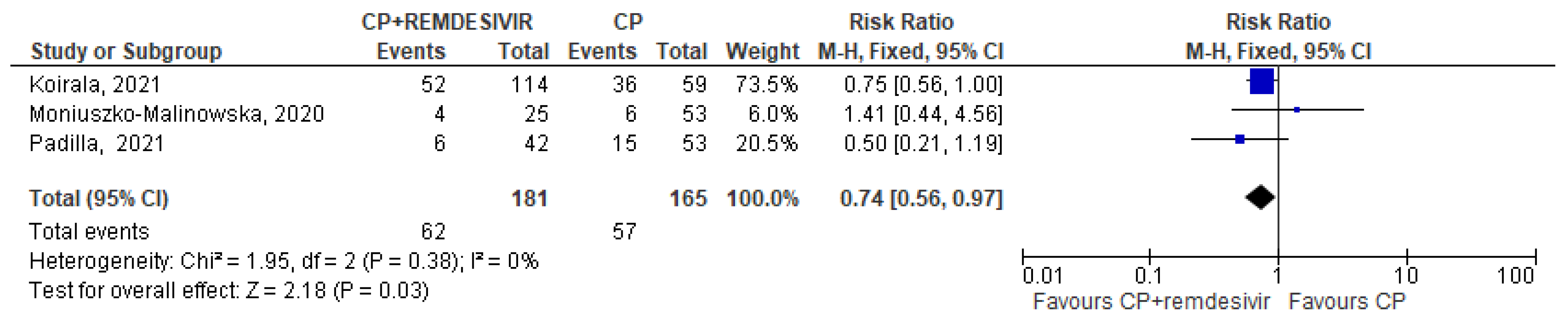
3.5. Meta-Analysis
3.6. Certainty of Evidence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 7 September 2023).
- Yuan, Y.; Jiao, B.; Qu, L.; Yang, D.; Liu, R. The development of COVID-19 treatment. Front. Immunol. 2023, 14, 1125246. [Google Scholar] [CrossRef] [PubMed]
- Casadevall, A.; Pirofski, L.A. The convalescent sera option for containing COVID-19. J. Clin. Investig. 2020, 130, 1545–1548. [Google Scholar] [CrossRef] [PubMed]
- Senefeld, J.W.; Franchini, M.; Mengoli, C.; Cruciani, M.; Zani, M.; Gorman, E.K.; Focosi, D.; Casadevall, A.; Joyner, M.J. COVID-19 Convalescent Plasma for the Treatment of Immunocompromised Patients: A Systematic Review and Meta-analysis. JAMA Netw. Open 2023, 6, e2250647. [Google Scholar] [CrossRef] [PubMed]
- Senefeld, J.W.; Gorman, E.K.; Johnson, P.W.; Moir, M.E.; Klassen, S.A.; Carter, R.E.; Paneth, N.S.; Sullivan, D.J.; Morkeberg, O.H.; Wright, R.S.; et al. Rates Among Hospitalized Patients with COVID-19 Treated with Convalescent Plasma: A Systematic Review and Meta-Analysis. Mayo Clin. Proc. Innov. Qual. Outcomes 2023, 7, 499–513. [Google Scholar] [CrossRef] [PubMed]
- Bloch, E.M.; Focosi, D.; Shoham, S.; Senefeld, J.; Tobian, A.A.R.; Baden, L.R.; Tiberghien, P.; Sullivan, D.J.; Cohn, C.; Dioverti, V.; et al. Guidance on the Use of Convalescent Plasma to Treat Immunocompromised Patients with Coronavirus Disease 2019. Clin. Infect. Dis. 2023, 76, 2018–2024. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, D.J.; Focosi, D.; Hanley, D.F.; Cruciani, M.; Franchini, M.; Ou, J.; Casadevall, A.; Paneth, N. Outpatient regimens to reduce COVID-19 hospitalisations: A systematic review and meta-analysis of randomized controlled trials. medRxiv 2023, preprint. [Google Scholar] [CrossRef]
- Chen, C.; Fang, J.; Chen, S.; Rajaofera, M.J.N.; Li, X.; Wang, B.; Xia, Q. The efficacy and safety of remdesivir alone and in combination with other drugs for the treatment of COVID-19: A systematic review and meta-analysis. BMC Infect. Dis. 2023, 23, 672. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0 [updated March 2011]; The Cochrane Collaboration: London, UK, 2011; Available online: http://www.cochranehandbook.org (accessed on 7 September 2023).
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, 4–10. [Google Scholar] [CrossRef]
- Schünemann, H.J.; Oxman, A.D.; Higgins, J.P.; Vist, G.E.; Glasziou, P.; Guyatt, G.H. Chapter 11: Presenting results and ’Summary of findings’ tables. In Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0 (updated March, 2011); Higgins, J.P., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011; Available online: http://handbook.cochrane.org (accessed on 7 September 2023).
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Vist, G.E.; Falck-Ytter, Y.; Schünemann, H.J. What is ‘quality of evidence’ and why is it important to clinicians? BMJ 2008, 336, 995–998. [Google Scholar] [CrossRef]
- Moniuszko-Malinowska, A.; Czupryna, P.; Zarębska-Michaluk, D.; Tomasiewicz, K.; Pancewicz, S.; Rorat, M.; Dworzańska, A.; Sikorska, K.; Bolewska, B.; Lorenc, B.; et al. Convalescent Plasma Transfusion for the Treatment of COVID-19-Experience from Poland: A Multicenter Study. J. Clin. Med. 2020, 10, 28. [Google Scholar] [CrossRef] [PubMed]
- Koirala, J.; Gyanwali, P.; Gerzoff, R.B.; Bhattarai, S.; Nepal, B.; Manandhar, R.; Jha, R.; Sharma, S.; Sharma, Y.R.; Bastola, A.; et al. Experience of Treating COVID-19 with Remdesivir and Convalescent Plasma in a Resource-Limited Setting: A Prospective, Observational Study. Open Forum Infect. Dis. 2021, 8, ofab391. [Google Scholar] [CrossRef] [PubMed]
- Arquiette, J.; Padilla, R.; Mai, Y.; Singh, G.; Galang, K.; Liang, E. Clinical Outcomes of COVID-19 Patients Treated with Convalescent Plasma or Remdesivir Alone and in Combination at a Community Hospital in California’s Central Valley. J. Pharm. Pharm. Sci. 2021, 24, 210–219. [Google Scholar] [CrossRef]
- Menichetti, F.; Popoli, P.; Puopolo, M.; Spila Alegiani, S.; Tiseo, G.; Bartoloni, A.; De Socio, G.V.; Luchi, S.; Blanc, P.; Puoti, M.; et al. Effect of High-Titer Convalescent Plasma on Progression to Severe Respiratory Failure or Death in Hospitalized Patients with COVID-19 Pneumonia: A Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e2136246, Erratum in JAMA Netw. Open 2021, 4, e2144236; Erratum in JAMA Netw. Open 2022, 5, e2146944. [Google Scholar] [CrossRef] [PubMed]
- Ortigoza, M.B.; Yoon, H.; Goldfeld, K.S.; Troxel, A.B.; Daily, J.P.; Wu, Y.; Li, Y.; Wu, D.; Cobb, G.F.; Baptiste, G.; et al. Efficacy and Safety of COVID-19 Convalescent Plasma in Hospitalized Patients: A Randomized Clinical Trial. JAMA Intern. Med. 2022, 182, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Libster, R.; Pérez Marc, G.; Wappner, D.; Coviello, S.; Bianchi, A.; Braem, V.; Esteban, I.; Caballero, M.T.; Wood, C.; Berrueta, M.; et al. Early High-Titer Plasma Therapy to Prevent Severe COVID-19 in Older Adults. N. Engl. J. Med. 2021, 384, 610–618. [Google Scholar] [CrossRef] [PubMed]
- Bégin, P.; Callum, J.; Jamula, E.; Cook, R.; Heddle, N.M.; Tinmouth, A.; Zeller, M.P.; Beaudoin-Bussières, G.; Amorim, L.; Bazin, R.; et al. Convalescent plasma for hospitalized patients with COVID-19: An open-label, randomized controlled trial. Nat. Med. 2021, 27, 2012–2024, Erratum in Nat. Med. 2022, 28, 212. [Google Scholar] [CrossRef]
- Avendaño-Solá, C.; Ramos-Martínez, A.; Muñez-Rubio, E.; Ruiz-Antorán, B.; Malo de Molina, R.; Torres, F.; Fernández-Cruz, A.; Calderón-Parra, J.; Payares-Herrera, C.; Díaz de Santiago, A.; et al. A multicenter randomized open-label clinical trial for convalescent plasma in patients hospitalized with COVID-19 pneumonia. J. Clin. Investig. 2021, 131, e152740. [Google Scholar] [CrossRef]
- Bar, K.J.; Shaw, P.A.; Choi, G.H.; Aqui, N.; Fesnak, A.; Yang, J.B.; Soto-Calderon, H.; Grajales, L.; Starr, J.; Andronov, M.; et al. A randomized controlled study of convalescent plasma for individuals hospitalized with COVID-19 pneumonia. J. Clin. Investig. 2021, 131, e155114. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group. Convalescent plasma in patients admitted to hospital with COVID-19 (RECOVERY): A randomised controlled, open-label, platform trial. Lancet 2021, 397, 2049–2059. [Google Scholar] [CrossRef]
- Lacombe, K.; Hueso, T.; Porcher, R.; Mekinian, A.; Chiarabini, T.; Georgin-Lavialle, S.; Ader, F.; Saison, J.; Martin-Blondel, G.; De Castro, N.; et al. Use of covid-19 convalescent plasma to treat patients admitted to hospital for covid-19 with or without underlying immunodeficiency: Open label, randomised clinical trial. BMJ Med. 2023, 2, e000427. [Google Scholar] [CrossRef] [PubMed]
- Herman, J.D.; Wang, C.; Loos, C.; Yoon, H.; Rivera, J.; Eugenia Dieterle, M.; Haslwanter, D.; Jangra, R.K.; Bortz, R.H., 3rd; Bar, K.J.; et al. Functional convalescent plasma antibodies and pre-infusion titers shape the early severe COVID-19 immune response. Nat. Commun. 2021, 12, 6853. [Google Scholar] [CrossRef] [PubMed]
- Hilfenhaus, J.; De Clercq, E.; Köhler, R.; Geursen, R.; Seiler, F. Combined antiviral effects of acyclovir or bromovinyldeoxyuridine and human immunoglobulin in herpes simplex virus-infected mice. Antivir. Res. 1987, 7, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Bravo, F.J.; Bourne, N.; Harrison, C.J.; Mani, C.; Stanberry, L.R.; Myers, M.G.; Bernstein, D.I. Effect of antibody alone and combined with acyclovir on neonatal herpes simplex virus infection in guinea pigs. J. Infect. Dis. 1996, 173, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Cross, R.W.; Bornholdt, Z.A.; Prasad, A.N.; Woolsey, C.; Borisevich, V.; Agans, K.N.; Deer, D.J.; Abelson, D.M.; Kim, D.H.; Shestowsky, W.S.; et al. Combination therapy with remdesivir and monoclonal antibodies protects nonhuman primates against advanced Sudan virus disease. JCI Insight 2022, 7, e159090. [Google Scholar] [CrossRef]
- Scotto, R.; Buonomo, A.R.; Iuliano, A.; Foggia, M.; Sardanelli, A.; Villari, R.; Pinchera, B.; Gentile, I.; Federico II COVID-Team. Remdesivir Alone or in Combination with Monoclonal Antibodies as an Early Treatment to Prevent Severe COVID-19 in Patients with Mild/Moderate Disease at High Risk of Progression: A Single Centre, Real-Life Study. Vaccines 2023, 11, 200. [Google Scholar] [CrossRef] [PubMed]
- Hirai, J.; Mori, N.; Sakanashi, D.; Ohashi, W.; Shibata, Y.; Asai, N.; Kato, H.; Hagihara, M.; Mikamo, H. Real-World Experience of the Comparative Effectiveness and Safety of Combination Therapy with Remdesivir and Monoclonal Antibodies versus Remdesivir Alone for Patients with Mild-to-Moderate COVID-19 and Immunosuppression: A Retrospective Single-Center Study in Aichi, Japan. Viruses 2023, 15, 1952. [Google Scholar] [CrossRef]
- Nair, M.P.; Schwartz, S.A. Immunomodulatory effects of corticosteroids on natural killer and antibody-dependent cellular cytotoxic activities of human lymphocytes. J. Immunol. 1984, 132, 2876–2882. [Google Scholar] [CrossRef]
- Jones, C.J.; Morris, K.J.; Jayson, M.I. Prednisolone inhibits phagocytosis by polymorphonuclear leucocytes via steroid receptor mediated events. Ann. Rheum. Dis. 1983, 42, 56–62. [Google Scholar] [CrossRef]
- Ullah, I.; Beaudoin-Bussières, G.; Symmes, K.; Cloutier, M.; Ducas, E.; Tauzin, A.; Laumaea, A.; Grunst, M.W.; Dionne, K.; Richard, J.; et al. The Fc-effector function of COVID-19 convalescent plasma contributes to SARS-CoV-2 treatment efficacy in mice. Cell Rep. Med. 2023, 4, 100893. [Google Scholar] [CrossRef]
- Casadevall, A.; Sullivan, D.J. Late administration and corticosteroid usage explain inefficacy in COVID-19 convalescent plasma trial. J. Infect. Dis. 2024, 229, 617–618. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.; Schauer, J.; Bryant, S.; Graves, C.R. The use of convalescent plasma therapy and remdesivir in the successful management of a critically ill obstetric patient with novel coronavirus 2019 infection: A case report. Case Rep. Women Health 2020, 27, e00221. [Google Scholar] [CrossRef] [PubMed]
- Magyari, F.; Pinczés, L.I.; Páyer, E.; Farkas, K.; Ujfalusi, S.; Diószegi, Á.; Sik, M.; Simon, Z.; Nagy, G.; Hevessy, Z.; et al. Early administration of remdesivir plus convalescent plasma therapy is effective to treat COVID-19 pneumonia in B-cell depleted patients with hematological malignancies. Ann. Hematol. 2022, 101, 2337–2345. [Google Scholar] [CrossRef] [PubMed]
- Malsy, J.; Veletzky, L.; Heide, J.; Hennigs, A.; Gil-Ibanez, I.; Stein, A.; Lütgehetmann, M.; Rosien, U.; Jasper, D.; Peine, S.; et al. Sustained Response After Remdesivir and Convalescent Plasma Therapy in a B-Cell-Depleted Patient with Protracted Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2021, 73, e4020–e4024. [Google Scholar] [CrossRef] [PubMed]
- Dell’Isola, G.B.; Felicioni, M.; Ferraro, L.; Capolsini, I.; Cerri, C.; Gurdo, G.; Mastrodicasa, E.; Massei, M.S.; Perruccio, K.; Brogna, M.; et al. Case Report: Remdesivir and Convalescent Plasma in a Newly Acute B Lymphoblastic Leukemia Diagnosis with Concomitant Sars-CoV-2 Infection. Front. Pediatr. 2021, 9, 712603. [Google Scholar] [CrossRef] [PubMed]
- Weinbergerova, B.; Mayer, J.; Kabut, T.; Hrabovsky, S.; Prochazkova, J.; Kral, Z.; Herout, V.; Pacasova, R.; Zdrazilova-Dubska, L.; Husa, P.; et al. Successful early treatment combining remdesivir with high-titer convalescent plasma among COVID-19-infected hematological patients. Hematol. Oncol. 2021, 39, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Jamir, I.; Lohia, P.; Pande, R.K.; Setia, R.; Singhal, A.K.; Chaudhary, A. Convalescent plasma therapy and remdesivir duo successfully salvaged an early liver transplant recipient with severe COVID-19 pneumonia. Ann. Hepatobiliary Pancreat. Surg. 2020, 24, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Schenker, C.; Hirzel, C.; Walti, L.N.; Zeerleder, S.S.; Andres, M.; Ramette, A.; Barbani, M.T.; Suter-Riniker, F.; Holbro, A.; Tritschler, T. Convalescent plasma and remdesivir for protracted COVID-19 in a patient with chronic lymphocytic leukaemia: A case report of late relapse after rapid initial response. Br. J. Haematol. 2022, 196, e27–e29. [Google Scholar] [CrossRef]
- Raho, G.; Cordeddu, W.; Firinu, D.; Del Giacco, S.W.; Angioni, G. Successful combination of remdesivir and convalescent plasma to treat a patient with rituximab-related B-cell deficiency and prolonged COVID-19: A case report. Anti-Infect. Agents 2023, 21, 79–85. [Google Scholar] [CrossRef]
- Iaboni, A.; Wong, N.; Betschel, S.D. A Patient with X-Linked Agammaglobulinemia and COVID-19 Infection Treated with Remdesivir and Convalescent Plasma. J. Clin. Immunol. 2021, 41, 923–925. [Google Scholar] [CrossRef]
- Furlan, A.; Forner, G.; Cipriani, L.; Vian, E.; Rigoli, R.; Gherlinzoni, F.; Scotton, P. Dramatic Response to Convalescent Hyperimmune Plasma in Association with an Extended Course of Remdesivir in 4 B Cell-Depleted Non-Hodgkin Lymphoma Patients with SARS-Cov-2 Pneumonia After Rituximab Therapy. Clin. Lymphoma Myeloma Leuk. 2021, 21, e731–e735. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author, State, Year [Ref.] | Study Design | Patients Enrolled (n) | Outcome (Death) | Safety |
|---|---|---|---|---|
| CCP plus remdesivir | ||||
| Moniuszko-Malinowska, Poland, 2020 [14] | Prospective | 78 patients hospitalized for COVID-19 - CCP + remdesivir: 25/78 (32.1%) - CCP: 53/78 (67.9%) | 30-day mortality: - CCP + remdesivir: 4/25 (16.0%) - CCP: 6/53 (11.3%) No difference was observed in the duration of hospitalization, the necessity of mechanical ventilation, or the duration of oxygen therapy between the two groups. | No side effects were recorded. |
| Koirala, Nepal, 2021 [15] | Prospective | 1083 patients hospitalized for moderate, severe, or life-threatening COVID-19 - CCP + remdesivir: 114/173 (65.9%) - CCP: 59/173 (34.1%) | Mortality: - CCP + remdesivir: 52/114 (45.6%) - CCP: 36/59 (61.0%) | Adverse events to remdesivir and CCP were reported in 4.5% (increased liver enzymes and serum creatinine levels) and 4.6% (fever, rash) of patients, respectively. |
| Arquiette, USA, 2021 [16] | Retrospective | 213 patients hospitalized for COVID-19 - CCP + remdesivir: 42/95 (44.2%) - CCP: 53/95 (55.8%) | Mortality: - CCP + remdesivir: 6/42 (14.3%) - CCP: 15/53 (28.3%) Patients with CCP monotherapy had decreased ventilation days and duration of hospitalization compared to those treated with combination therapy. | Six adverse (4 increased liver enzymes and 2 serum creatinine levels) reactions were recorded with remdesivir, 2 adverse reactions after CCP infusion. |
| TSUNAMI, Italy, 2021 [17] | RCT | 487 patients hospitalized with COVID-19 pneumonia. - CCP + remdesivir: 157/232 (67.7%) - CCP: 74/232 (31.9%) | Composite of worsening respiratory failure (PaO2/FiO2 ratio < 150 mmHg) or death within 30 days from randomization (primary endpoint): - CCP + remdesivir: 42/157 (26.8%) - CCP: 17/74 (23.0%) | NA |
| CONTAIN COVID-19, USA, 2021 [18] | RCT | 941 patients hospitalized with COVID-19 - CCP + remdesivir: 273/468 (58.3%) - CCP: 195/468 (41.7%) | The OR for mortality at day 28 for CCP alone was lower than that for CCP + remdesivir (0.77; 95% CI 0.43–1.36 versus 1.0; 95% CI 0.52–1.96). | NA |
| CCP plus corticosteroids | ||||
| CONTAIN COVID-19, USA, 2021 [18] | RCT | 941 patients hospitalized with COVID-19 - CCP + steroids: 407/468 (87.0%) - CCP: 61/468 (13.0%) | The OR for mortality at day 28 for CCP alone was lower than that for CCP + steroids (0.77; 95% CI 0.43–1.36 versus 0.86; 95% CI 0.49–1.52). | NA |
| PlasmAr, Argentina, 2021 [19] | RCT | 333 patients hospitalized with COVID-19 - CCP + steroids: 209/228 (91.7%) - CCP: 19/228 (8.3%) | No interaction between CCP and steroids was found. | NA |
| CONCOR-1, Canada, 2021 [20] | RCT | 940 patients hospitalized with COVID-19 - CCP + steroids: 496/614 (80.8%) - CCP alone: 118/614 (19.2%) | Primary outcome (intubation or death by 30 days): - CCP + steroids: 159/496 (32.1%) - CCP alone: 40/118 (33.9%) | NA |
| Conplas-19, Spain, 2021 [21] | RCT | 350 patients hospitalized with COVID-19 - CCP + steroids: 127/179 (70.9%) - CCP alone: 52/179 (29.1%) | Outcome (primary and secondary) at 14 days: - CCP + steroids: 18/127 (14.2%) - CCP alone: 3/52 (5.8%) Outcome (primary and secondary) at 28 days: - CCP + steroids: 12/127 (9.5%) - CCP alone: 3/52 (5.8%) | NA |
| PennCCP2, USA, 2021 [22] | RCT | 79 patients hospitalized with COVID-19 - CCP + steroids: 31/40 (77.5%) - CCP alone: 9/40: 22.5%) | Mortality at 28 days: - CCP + steroids: 2/31 (6.5%) - CCP alone: 0/9 | NA |
| RECOVERY, UK, 2021 [23] | RCT | 11,558 patients hospitalized with COVID-19 - CCP + steroids: 5370/5795 (92.7%) - CCP alone: 391/5795 (6.7%) | Outcome (28-day invasive mechanical ventilation or death) - CCP + steroids: 1491/5100 (29.2%) - CCP alone: 66/360 (18.3%) | NA |
| CORIPLASM, France, 2023 [24] | RCT | 120 patients hospitalized with COVID-19 - CCP + steroids: 30/60 (50.0%) - CCP alone: 30/60 (50.0%) | Outcome (14-day mortality) - CCP + steroids: 11/30 (36.7%) - CCP alone: 8/30 (26.7%) | NA |
| Settings: Hospitalized Patients with COVID-19 Intervention: Convalescent Plasma (CCP) Comparison: CCP + Remdesivir, CCP + Steroids | ||||||
|---|---|---|---|---|---|---|
| Outcome: Mortality | Illustrative comparative risks * (95% CI) | Relative effect (95% CI) | No. of Participants(studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Controls (CCP + Other) | Intervention (CCP) | |||||
| CCP+ Remdesivir | 342 per 1000 | 253 per 1000 (from 191 to 331) | RR 0.74 (95% CIs, 0.56 to 0.97) | 346 patients from 3 non-RCTs | Moderate. Downgraded twice for nonserious ROB | CCP in combination with remdesivir had a lower mortality rate compared to CCP alone. |
| CCP+ steroids | 639 per 1000 | 460 per 1000 (from 217 to 964) | RR 0.72 (0.34/1.51) | 100 patients from 2 RCTs | Very low. Downgraded for serious imprecision and indirectness | Rates of mortality were not significantly different in CCP recipients compared to CCP + steroids recipients. |
| * The basis for the assumed risk is the mean control group risk across studies. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franchini, M.; Focosi, D.; Cruciani, M.; Joyner, M.J.; Pirofski, L.-a.; Senefeld, J.W.; Shoham, S.; Sullivan, D.J.; Casadevall, A. Safety and Efficacy of Convalescent Plasma Combined with Other Pharmaceutical Agents for Treatment of COVID-19 in Hospitalized Patients: A Systematic Review and Meta-Analysis. Diseases 2024, 12, 41. https://doi.org/10.3390/diseases12030041
Franchini M, Focosi D, Cruciani M, Joyner MJ, Pirofski L-a, Senefeld JW, Shoham S, Sullivan DJ, Casadevall A. Safety and Efficacy of Convalescent Plasma Combined with Other Pharmaceutical Agents for Treatment of COVID-19 in Hospitalized Patients: A Systematic Review and Meta-Analysis. Diseases. 2024; 12(3):41. https://doi.org/10.3390/diseases12030041
Chicago/Turabian StyleFranchini, Massimo, Daniele Focosi, Mario Cruciani, Michael J. Joyner, Liise-anne Pirofski, Jonathon W. Senefeld, Shmuel Shoham, David J. Sullivan, and Arturo Casadevall. 2024. "Safety and Efficacy of Convalescent Plasma Combined with Other Pharmaceutical Agents for Treatment of COVID-19 in Hospitalized Patients: A Systematic Review and Meta-Analysis" Diseases 12, no. 3: 41. https://doi.org/10.3390/diseases12030041