

Role of B Cells beyond Antibodies in HBV-Induced Oncogenesis: Fulminant Cancer in Common Variable Immunodeficiency—Clinical and Immunotransplant Implications with a Review of the Literature



Abstract
:
1. Introduction
2. Results
2.1. Initial Diagnosis
2.2. Results of Time-Lapse Analysis of the Patient’s History
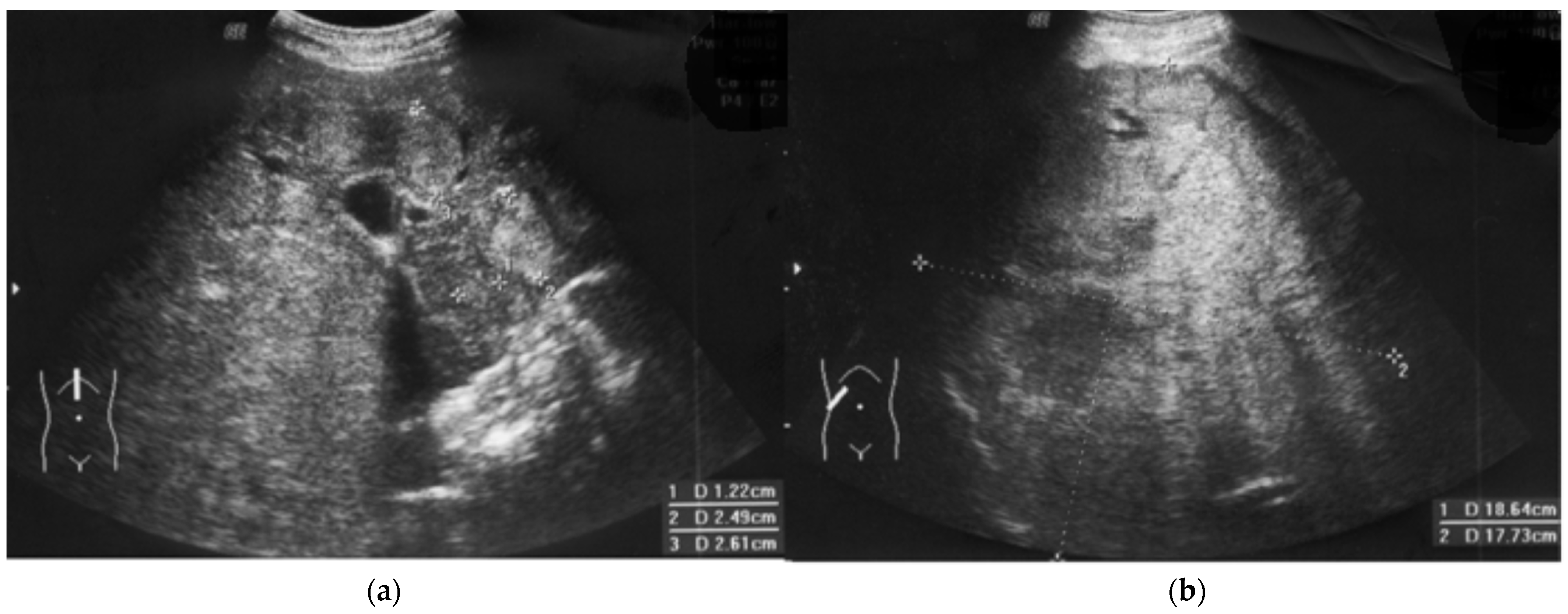
2.3. Clinical Course of HCC and Outcome
3. Discussion
3.1. Efficacy: Anti-HBs Immunogloibulins Are Not Protective Per Se
3.2. HDV Probability
3.3. Specific IgG Substitution Effectiveness and Safety
3.4. Crucial Role of Lymphocyte Cooperation In Viral and Cancer Immunosurveillance
4. Materials and Methods
4.1. Material: Case Presentation
4.2. Methods (Time-Lapse Analysis of CVID Presentation)
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fonseca, M.O.; Pang, L.W.; de Paula Cavalheiro, N.; Barone, A.A.; Heloisa Lopes, M. Randomized trial of recombinant hepatitis B vaccine in HIV-infected adult patients comparing a standard dose to a double dose. Vaccine 2005, 23, 2902–2908. [Google Scholar] [CrossRef] [PubMed]
- Daza-Cajigal, V.; Segura-Guerrero, M.; López-Cueto, M.; Robles-Marhuenda, Á.; Camara, C.; Gerra-Galán, T.; Gómez-De-La-Torre, R.; Avendaño-Monje, C.L.; Sánchez-Ramón, S.; Bosque-Lopez, M.J.; et al. Clinical manifestations and approach to the management of patients with common variable immunodeficiency and liver disease. Front. Immunol. 2023, 14, 1197361. [Google Scholar] [CrossRef] [PubMed]
- Zdziarski, P.; Gamian, A.; Majda, J.; Korzeniowska-Kowal, A. Passive blood anaphylaxis: Subcutaneous immunoglobulins are a cause of ongoing passive anaphylactic reaction. Allergy Asthma Clin. Immunol. 2017, 13, 41. [Google Scholar] [CrossRef]
- Walter, J.E.; Armanios, M.; Shah, U.; Friedmann, A.M.; Spitzer, T.; Sharatz, S.M.; Hagen, C. Case 41-2015. A 14-Year-Old Boy with Immune and Liver Abnormalities. N. Engl. J. Med. 2015, 373, 2664–2676. [Google Scholar] [CrossRef]
- Rizzo, G.E.M.; Cabibbo, G.; Craxì, A. Hepatitis B Virus-Associated Hepatocellular Carcinoma. Viruses 2022, 14, 986. [Google Scholar] [CrossRef] [PubMed]
- Zdziarski, P. CMV-Specific Immune Response-New Patients, New Insight: Central Role of Specific IgG during Infancy and Long-Lasting Immune Deficiency after Allogenic Stem Cell Transplantation. Int. J. Mol. Sci. 2019, 20, 271. [Google Scholar] [CrossRef] [PubMed]
- Saleem Kamili Laboratory Procedure Manual Analyte: Hepatitis B Surface Antibody (Anti-HBS) CDC September, 2013. Hepatitis B Surface Antibody (Anti-HBS)—CDC. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2007-2008/labmethods/hepb_s_e_met_hep_b_surface_antibody.pdf (accessed on 20 January 2023).
- Mast, E.E.; Weinbaum, C.M.; Fiore, A.E.; Alter, M.J.; Bell, B.P.; Finelli, L.; Rodewald, L.; Douglas, J.M.; Janssen, R.S.; Ward, J.W.; et al. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: Recommendations of the Advisory Committee on Immunization Practices (ACIP) Part II: Immunization of adults. In MMWR Recomm. Rep.; 2006; 55, pp. 1–33. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5516a1.htm (accessed on 31 January 2023).
- Stevens, C.E.; Toy, P.T.; Taylor, P.E.; Lee, T.; Yip, H.Y. Prospects for control of hepatitis B virus infection: Implications of childhood vaccination and long-term protection. Pediatrics 1992, 90, 170–173. [Google Scholar] [CrossRef] [PubMed]
- Hadler, S.C.; Coleman, P.J.; O’Malley, P.; Judson, F.N.; Altman, N. Evaluation of long-term protection by hepatitis B vaccine for seven to nine years in homosexual men. In Viral Hepatitis and Liver Disease: Proceedings of the 1990 International Symposium on Viral Hepatitis and Liver Disease; Hollinger, F.B., Lemon, S.M., Margolis, H., Eds.; Williams & Wilkins: Baltimore, MD, USA, 1991; pp. 776–778. [Google Scholar]
- Banatvala, J.E.; Van Damme, P. Hepatitis B vaccine—Do we need boosters? J. Viral Hepat. 2003, 10, 1–6. [Google Scholar] [CrossRef]
- Hwang, S.; Moon, D.B.; Lee, S.G.; Park, K.M.; Kim, K.H.; Ahn, C.S.; Lee, Y.J.; Chu, C.W.; Yang, H.S.; Cho, S.H.; et al. Safety of anti-hepatitis B core antibody-positive donors for living-donor liver transplantation. Transplantation 2003, 75 (Suppl. S3), S45–S48. [Google Scholar] [CrossRef]
- Ardeniz, Ö.; Unger, S.; Onay, H.; Ammann, S.; Keck, C.; Cianga, C.; Gerçeker, B.; Martin, B.; Fuchs, I.; Salzer, U.; et al. β2-Microglobulin deficiency causes a complex immunodeficiency of the innate and adaptive immune system. JACI 2015, 136, 392–401. [Google Scholar] [CrossRef]
- Giordano, C.; Picardi, M.; Pugliese, N.; Vincenzi, A.; Abagnale, D.P.; De Fazio, L.; Giannattasio, M.L.; Fatigati, C.; Ciriello, M.; Salemme, A.; et al. Lamivudine 24-month-long prophylaxis is a safe and efficient choice for the prevention of hepatitis B virus reactivation in HBsAg-negative/HBcAb-positive patients with advanced DLBCL undergoing upfront R-CHOP-21. Front. Oncol. 2023, 13, 1130899. [Google Scholar] [CrossRef] [PubMed]
- Zdziarski, P. Importance of the Tumor Boards’ decisions for the patientcentered care—Case studies in the COVID-19 era. Pol. Merkur. Lekarski. 2022, 50, 78–85. [Google Scholar] [PubMed]
- Mas, A.; Castells, L.; Abradelo, M.; Bernardos, A.; Páez, A.; Woodward, M.K.; Sousa, J.M. Evaluation of Anti-HBs serum levels and pharmacokinetic profile after intravenous administration of Niuliva, a new hepatitis B immunoglobulin, following liver transplantation. Transplant. Proc. 2009, 41, 4253–4258. [Google Scholar] [CrossRef] [PubMed]
- Cholongitas, E.; Goulis, J.; Akriviadis, E.; Papatheodoridis, G.V. Hepatitis B immunoglobulin and/or nucleos(t)ide analogues for prophylaxis against hepatitis B virus recurrence after liver transplantation: A systematic review. Liver Transpl. 2011, 17, 1176–1190. [Google Scholar] [CrossRef]
- Beckebaum, S.; Herzer, K.; Bauhofer, A.; Gelson, W.; De Simone, P.; de Man, R.; Engelmann, C.; Müllhaupt, B.; Vionnet, J.; Salizzoni, M.; et al. Recurrence of Hepatitis B Infection in Liver Transplant Patients Receiving Long-Term Hepatitis B Immunoglobulin Prophylaxis. Ann. Transplant. 2018, 23, 789–801. [Google Scholar] [CrossRef] [PubMed]
- Roque-Afonso, A.M.; Feray, C.; Samuel, D.; Simoneau, D.; Roche, B.; Emile, J.F.; Gigou, M.; Shouval, D.; Dussaix, E. Antibodies to hepatitis B surface antigen prevent viral reactivation in recipients of liver grafts from anti-HBC positive donors. Gut 2002, 50, 95–99. [Google Scholar] [CrossRef]
- Donataccio, M.; Dalle Ore, G.; Donataccio, D. Acute renal failure following intravenous administration of hepatitis B im-munoglobulin in liver transplantation. Minerva Gastroenterol. Dietol. 2009, 55, 501–504. [Google Scholar]
- Blanchong, C.A.; Chung, E.K.; Rupert, K.L.; Yang, Y.; Yang, Z.; Zhou, B.; Moulds, J.M.; Yu, C.Y. Genetic, structural and functional diversities of human complement components C4A and C4B and their mouse homologues, Slp and C4. Int. Immunopharmacol. 2001, 1, 365–392. [Google Scholar] [CrossRef]
- Wang, X.; Song, A.; Lin, X.; Lu, J.; Zheng, S.; Ma, L.; Ren, S.; Zheng, Y.; Chen, X. Clinical characteristics of hepatitis flares during pregnancy and postpartum in Chinese chronic hepatitis B virus carriers—A prospective cohort study of 417 cases. Front. Immunol. 2022, 13, 1031291. [Google Scholar] [CrossRef]
- Guo, Y.; Liu, J.; Meng, L.; Meina, H.; Du, Y. Survey of HBsAg-positive pregnant women and their infants regarding measures to prevent maternal-infantile transmission. BMC Infect. Dis. 2010, 10, 26. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, R.M.; Reddy, P.B.; Arava, J.; Rao, P.; Mitnala, S.; Gupta, R.; Reddy, D. Relationship between serum HBsAg level, HBV DNA level, and peripheral immune cells in patients with chronic hepatitis B virus infection. Hepat. Med. 2010, 2, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.; Yang, L.; Bi, X.; Deng, W.; Jiang, T.; Lin, Y.; Wang, S.; Zhang, L.; Liu, R.; Chang, M.; et al. Cytokine profiles CD8+ T cells in the occurrence of acute chronic hepatitis, B. Front. Immunol. 2022, 13, 1036612. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Ji, T.; Xin, S.; Xu, J.; Yu, Y. A case report of hepatitis B virus reactivation 19 months after cessation of chemotherapy with rituximab. Front. Immunol. 2022, 13, 1083862. [Google Scholar] [CrossRef] [PubMed]
- Wehr, C.; Kivioja, T.; Schmitt, C.; Ferry, B.; Witte, T.; Eren, E.; Vlkova, M.; Hernandez, M.; Detkova, D.; Bos, P.R.; et al. The EUROclass trial: Defining subgroups in common variable immunodeficiency. Blood 2008, 111, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Buonomo, A.R.; Viceconte, G.; Scotto, R.; De Angelis, M.; Tozza, S.; Manganelli, F.; Lanza, A.G.; Di Costanzo, G.G.; Gentile, I. Seronegative occult HBV reactivation complicated with fulminant acute liver failure after rituximab for chronic inflammatory demyelinating polyneuropathy. Infect. Dis. 2020, 52, 216–218. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Ubreva, J.; Arutyunyan, A.; Bonder, M.J.; Del Pino-Molina, L.; Clark, S.J.; de la Calle-Fabregat, C.; Garcia-Alonso, L.; Handfield, L.F.; Ciudad, L.; Andrés-León, E.; et al. Single-cell Atlas of common variable immunodeficiency shows germinal center-associated epigenetic dysregulation in B-cell responses. Nat. Commun. 2022, 13, 1779. [Google Scholar] [CrossRef] [PubMed]
- Aramburu, J.; Azzoni, L.; Rao, A.; Perussia, B. Activation and expression of the nuclear factors of activated T cells, NFATp and NFATc, in human natural killer cells: Regulation upon CD16 ligand binding. J. Exp. Med. 1995, 182, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Lupberger, J.; Hildt, E. Hepatitis B virus-induced oncogenesis. World J. Gastroenterol. 2007, 13, 74–81. [Google Scholar] [CrossRef]
- Levrero, M.; Zucman-Rossi, J. Mechanisms of HBV-induced hepatocellular carcinoma. J. Hepatol. 2016, 64 (Suppl. S1), S84–S101. [Google Scholar] [CrossRef] [PubMed]
- Zdziarski, P. Cellular transplantation–orthotopic liver transplantation alternative. Pol. Merkur. Lekarski. 2007, 23, 297–301. [Google Scholar] [PubMed]
- Roosens, W.; Staels, F.; Van Loo, S.; Humblet-Baron, S.; Meyts, I.; De Samblanx, H.; Verslype, C.; van Malenstein, H.; van der Merwe, S.; Laleman, W.; et al. Rituximab and improved nodular regenerative hyperplasia-associated non-cirrhotic liver disease in common variable immunodeficiency: A case report and literature study. Front. Immunol. 2023, 14, 1264482. [Google Scholar] [CrossRef] [PubMed]
- Zdziarski, P.; Gamian, A. Lymphoid Interstitial Pneumonia in Common Variable Immune Deficiency—Case Report With Disease Monitoring in Various Therapeutic Options: Pleiotropic Effects of Rituximab Regimens. Front. Pharmacol. 2019, 9, 1559. [Google Scholar] [CrossRef] [PubMed]
- Zea-Vera, A.F. Common variable immunodeficiency and chronic hepatitis B: Therapeutic challenge. Clin. Res. Hepatol. Gastroenterol. 2020, 44, e38–e40. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| %lymphocytes | Cells/μL | Normal Range | |
|---|---|---|---|
| CD3 | 54.4 | 706.6 | 700–2100 |
| CD4 | 42.7 | 555.5 | 300–1400 |
| CD8 | 9.9 | 128.7 | 200–900 |
| CD27+CD8+ | 7.9 | 102.2 | |
| CD27+CD4+ | 40.2 | 522.1 | |
| CD27+CD8+CD45 RO+ | 2.2 | 29.0 | |
| CD27+CD8+CD45 RO- | 5.6 | 73.2 | |
| CD27+CD4+CD45 RO+ | 14.2 | 184.7 | |
| CD27+CD4+CD45 RO- | 26.0 | 337.4 | |
| CD16 | 5.2 | 67.5 | |
| CD56+CD3+ | 1.0 | 12.5 | 250–320 |
| CD56+CD16+ | 3.9 | 50.4 | 90–600 |
| CD19 | 0.9 | 11.2 | 100–500 |
| CD27+CD19+ | 0.7 | 9.1 | |
| IVIG replacement therapy | Initial phase | Stable period | Normal range |
| IgG [mg/dL] | 80 | 505–1055 | 700–1600 |
| IgA [mg/dL] | <5 | NT | 70–150 |
| IgM [mg/dL] | <10 | NT | 40–230 |
| Anti-HBs | <5 * | 111–220 | NA |
| Anti HBc total | Negative | Positive ** | Negative |
| β2m (mg/L) | 0.98 | 0.9–1.7 | 0.8–2.2 |
| C4 [mg/dL] | 38 | 29 | 10–40 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zdziarski, P.; Gamian, A. Role of B Cells beyond Antibodies in HBV-Induced Oncogenesis: Fulminant Cancer in Common Variable Immunodeficiency—Clinical and Immunotransplant Implications with a Review of the Literature. Diseases 2024, 12, 80. https://doi.org/10.3390/diseases12050080
Zdziarski P, Gamian A. Role of B Cells beyond Antibodies in HBV-Induced Oncogenesis: Fulminant Cancer in Common Variable Immunodeficiency—Clinical and Immunotransplant Implications with a Review of the Literature. Diseases. 2024; 12(5):80. https://doi.org/10.3390/diseases12050080
Chicago/Turabian StyleZdziarski, Przemyslaw, and Andrzej Gamian. 2024. "Role of B Cells beyond Antibodies in HBV-Induced Oncogenesis: Fulminant Cancer in Common Variable Immunodeficiency—Clinical and Immunotransplant Implications with a Review of the Literature" Diseases 12, no. 5: 80. https://doi.org/10.3390/diseases12050080