Survival and Prognostic Factors in Mixed Cryoglobulinemia: Data from 246 Cases


Abstract
:1. Introduction
2. Patients and Methods
- (1)
- Virological response: effect of treatment on HCV-RNA. Sustained virological response (SVR): loss of HCV-RNA at the end of follow-up. Relapse: loss of HCV-RNA at the end of treatment but reappearance of viral replication during follow-up. No response: persistent HCV-RNA positivity during therapy and follow-up.
- (2)
- Biochemical response: effect of therapy on ALT, normal value was considered 40 IU/L. Complete responses: normalization of the serum ALT level during treatment followed by normal ALT values lasting for 6 months after discontinuation of therapy. No response: ALT out of normal value during treatment and follow-up. Relapse: normalization of the serum ALT level during treatment followed by return to abnormal values during follow-up. In some patients, this parameter was not considered, since the ALT level was normal at the beginning of the treatment.
- (3)
- Immune response: effect of therapy on serum RF concentration and on cryocrit level. Complete response: normalization of serum RF concentration and disappearance of circulating cryoglobulins. Partial response: reduction (but not normalization) of RF and cryoglobulins >50%. No response: Reduction <50% of RF and cryocrit levels or stable levels. Relapse: partial or complete normalization of serum RF and cryoglobulins during therapy followed by return to higher values during follow-up.
- (4)
- Clinical response: effect of therapy on the clinical manifestations of the disease (including purpura, arthralgia and weakness). Complete response: disappearance of all clinical signs of the disease. Partial response: improvement of the clinical symptoms (reduction of the purpura score >50%). No response: reduction of the purpura score <50% or stable disease. Relapse: partial or complete normalization of clinical symptoms during therapy followed by return to higher score after the end of treatment.
3. Statistical Analysis
4. Results
4.1. Patient Characteristics
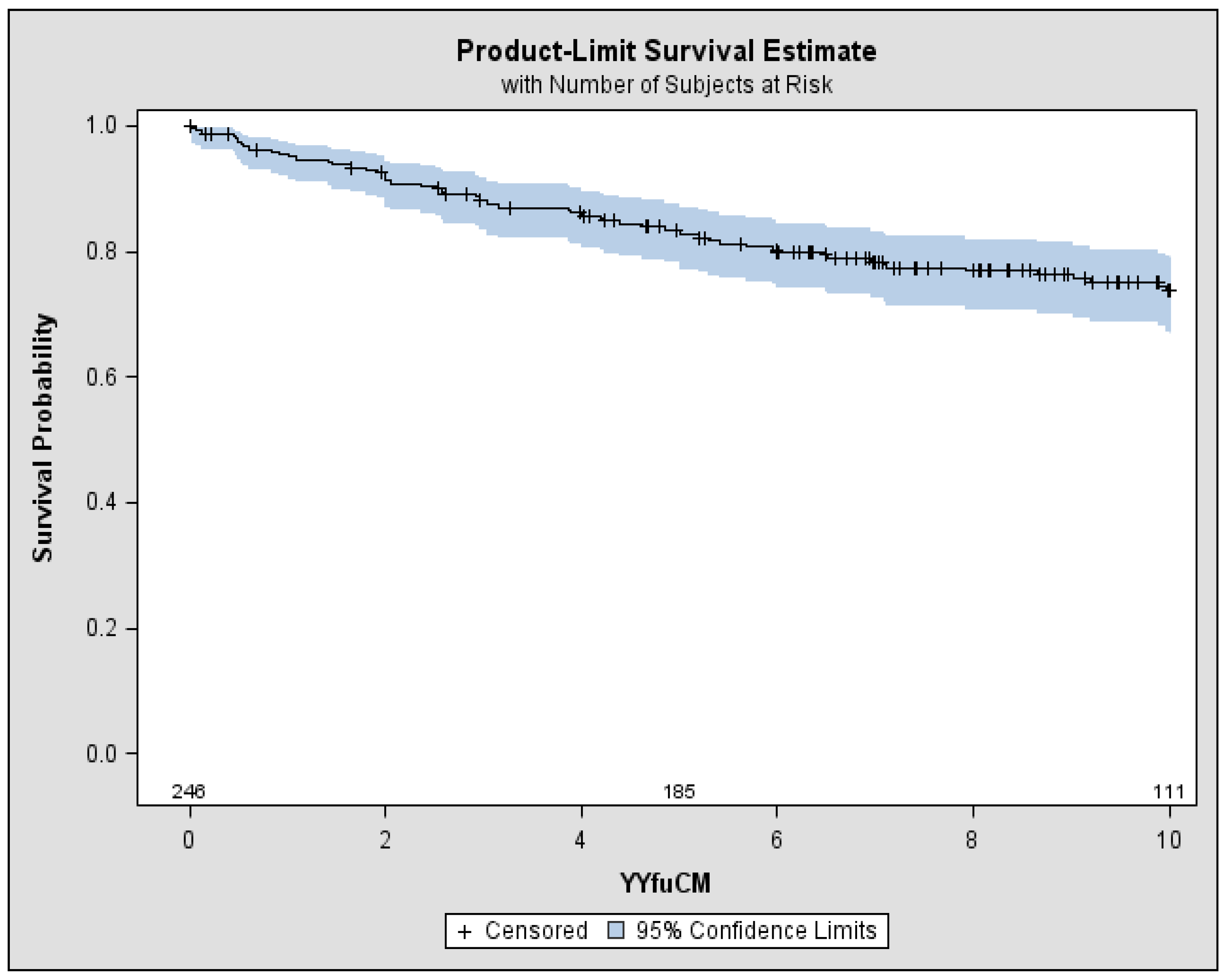
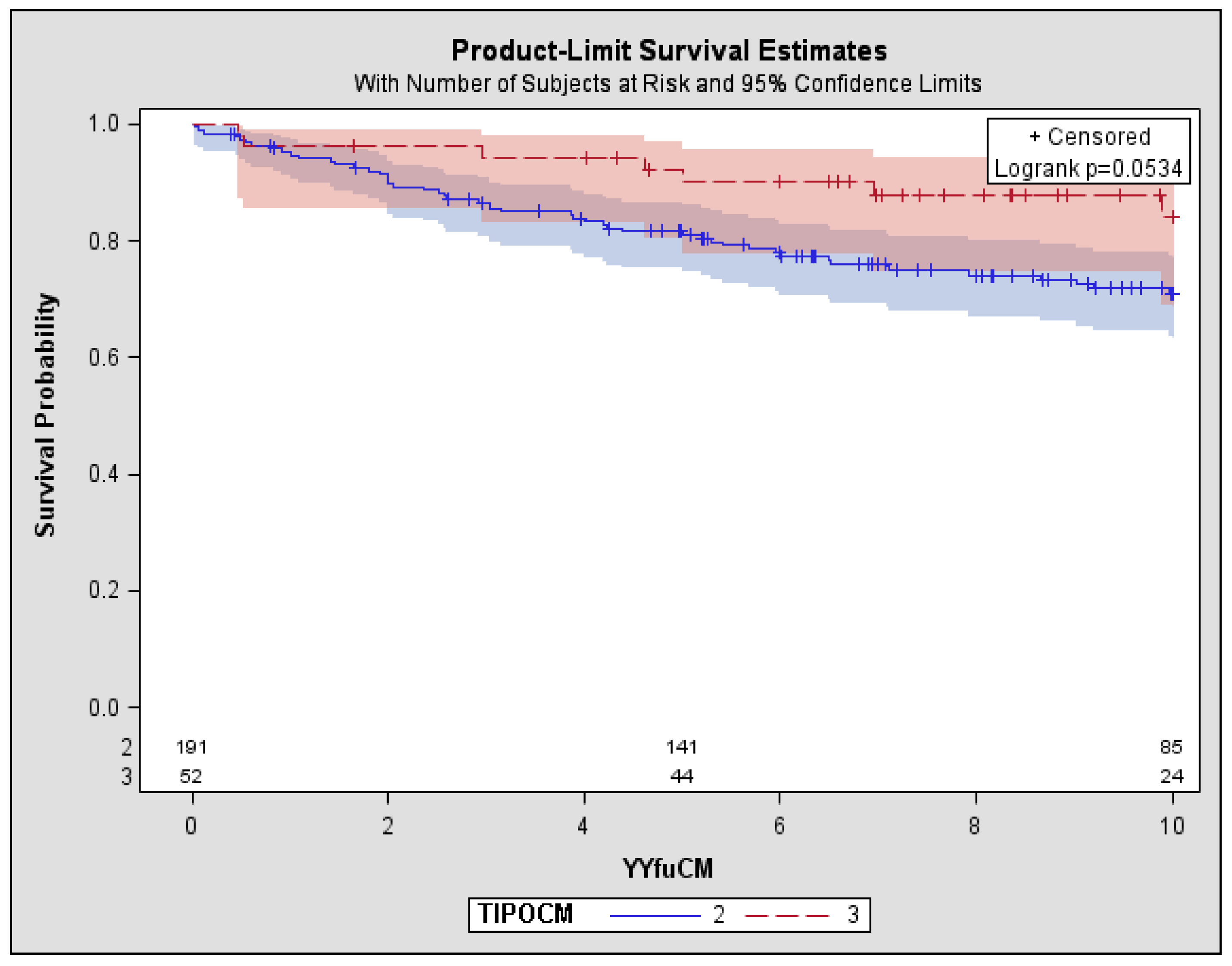
4.2. Follow-Up of the Patients
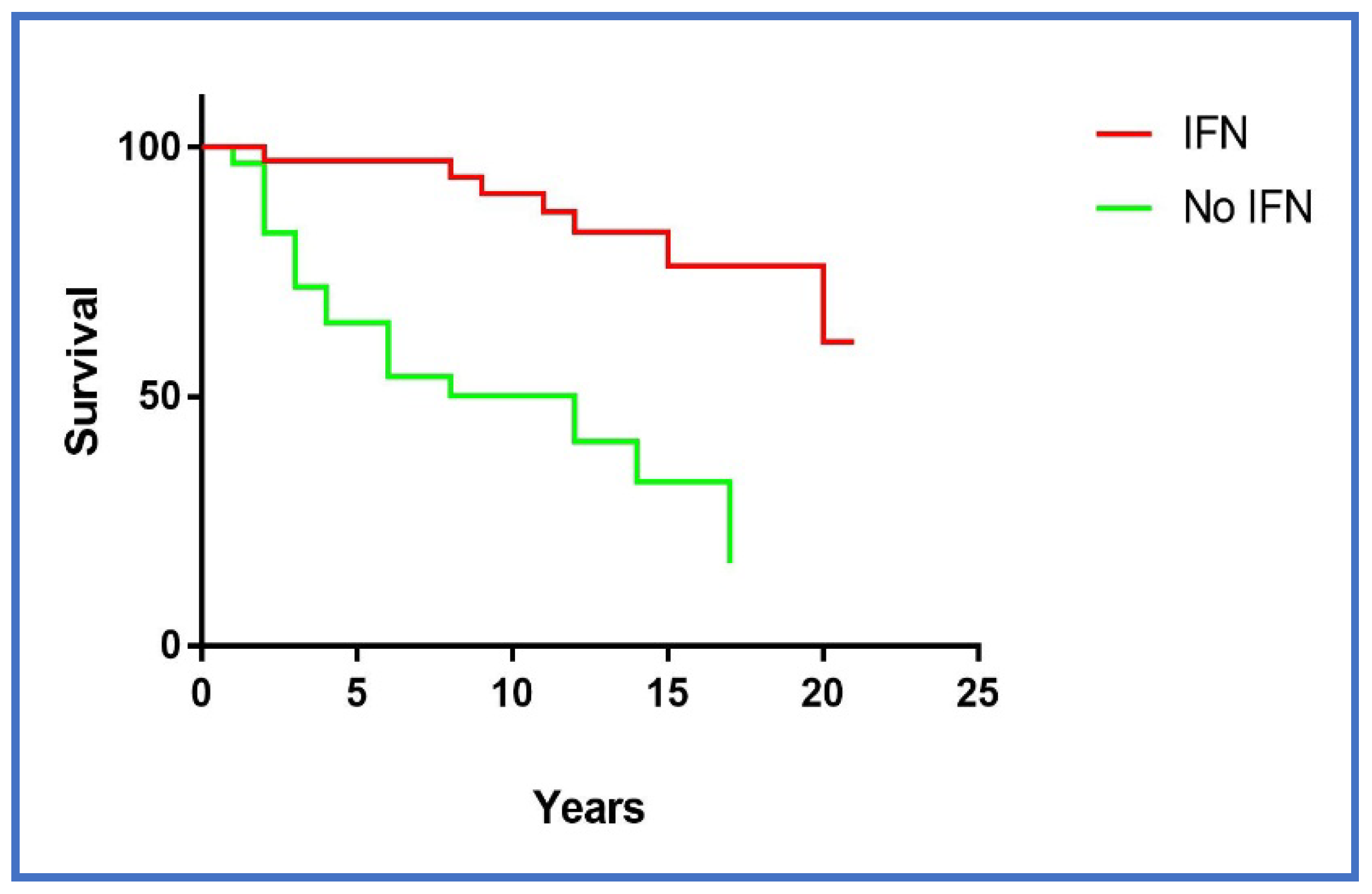
4.3. Effects of Therapeutic Regimens
5. Discussion
Author Contributions
Conflicts of Interest
References
- Brouet, J.C.; Clauvel, J.P.; Danon, F.; Klein, M.; Seligmann, M. Biologic and clinical significance of cryoglobulins. A report of 86 cases. Am. J. Med. 1974, 57, 775–788. [Google Scholar] [CrossRef]
- Ferri, C.; Zignego, A.L.; Giuggioli, D.; Sebastiani, M.; Cazzato, M.; Antonelli, A.; La Civita, L.; Fadda, P.; Longombardo, G.; Pileri, S. HCV and cryoglobulinemic vasculitis. Clevel. Clin. J. Med. 2002, 69, SII20–SII32. [Google Scholar] [CrossRef]
- Gorevic, P.; Kassab, H.; Levo, Y. Mixed cryoglobulinemia: Clinical aspects and long-term follow-up of forty patients. Am. J. Med. 1980, 69, 287–308. [Google Scholar] [CrossRef]
- Cacoub, P.; Hausfater, P.; Musset, L.; Piette, J.C. Mixed cryoglobulinemia in Hepatitis C patients. GERMIVIC. Ann. Med. Interne (Paris) 2000, 151, 20–29. [Google Scholar] [PubMed]
- Agnello, G.; Chung, R.T.; Kaplan, L.M. A role for Hepatitis C virus infection in Type II cryoglobulinemia? N. Engl. J. Med. 1992, 327, 1490–1496. [Google Scholar] [CrossRef] [PubMed]
- Ferri, C.; La Civita, L.; Longombardo, G.; Greco, F.; Bombardieri, S. Hepatitis C virus and mixed cryoglobulinaemia. Eur. J. Clin. Investig. 1993, 23, 399–405. [Google Scholar] [CrossRef]
- Mazzaro, C.; Tulissi, P.; Moretti, M.; Mazzoran, L.; Pussini, E.; Crovatto, M.; Santini, G.F.; Pozzato, G. Clinical and virological findings in mixed cryoglobulinemia. J. Int. Med. 1995, 238, 153–160. [Google Scholar] [CrossRef]
- Ferri, C.; Cacoub, P.; Mazzaro, C.; Roccatello, D.; Scaini, P.; Sebastiani, M.; Tavoni, A.; Zignego, A.L.; De Vita, S. Treatment with rituximab in patients with mixed cryoglobulinemia syndrome: Results of multicenter cohort study and review of the literature. Autoimmun. Rev. 2011, 11, 48–55. [Google Scholar] [CrossRef] [PubMed]
- De Vita, S.; Quartuccio, L.; Isola, M.; Mazzaro, C.; Scaini, P.; Lenzi, M.; Campanini, M.; Naclerio, C.; Tavoni, A.; Pietrogrande, M.; et al. A randomized controlled trial of rituximab for the treatment of severe cryoglobulinemic vasculitis. Arthritis Rheum. 2012, 64, 843–853. [Google Scholar] [CrossRef] [PubMed]
- Bedossa, P.; Poynard, T. An algorithm for the grading of activity in chronic Hepatitis C. The METAVIR Cooperative Study Group. Hepatology 1996, 24, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J.; Vardiman, J.W. WHO Classification of Tumours of Haematopoetic and Lymphoid Tissues, 4th ed.; International Agency for Research on Cancer (IARC): Lyon, France, 2008. [Google Scholar]
- Mazzaro, C.; Zorat, F.; Comar, C.; Nascimben, F.; Bianchini, D.; Baracetti, S.; Donada, C.; Donadon, V.; Pozzato, G. Interferon plus ribavirin in patients with Hepatitis C virus positive mixed cryoglobulinemia resistant to interferon. J. Rheumatol. 2003, 30, 1775–1781. [Google Scholar] [PubMed]
- Terrier, B.; Semoun, O.; Saadoun, D.; Sène, D.; Resche-Rigon, M.; Cacoub, P. Prognostic factors in patients with hepatitis C virus infection and systemic vasculitis. Arthritis Rheum. 2011, 63, 1748–1757. [Google Scholar] [CrossRef] [PubMed]
- Saadoun, D.; Sellam, J.; Ghillani-Dalbin, P.; Crecel, R.; Piette, J.C.; Cacoub, P. Increased risks of lymphoma and death among patients with Non-Hepatitis C virus-related mixed cryoglobulinemia. Arch. Intern. Med. 2006, 166, 2101–2108. [Google Scholar] [CrossRef] [PubMed]
- Mazzaro, C.; Panarello, G.; Tesio, F.; Santini, G.; Crovatto, M.; Mazzi, G.; Zorat, F.; Tulissi, P.; Pussini, E.; Baracetti, S.; et al. Hepatitis C virus risk: A Hepatitis C virus related syndrome. J. Intern. Med. 2000, 247, 535–545. [Google Scholar] [CrossRef] [PubMed]
- Ferri, C.; Zignego, A.L.; Pileri, S.A. Cryoglobulins. J. Clin. Pathol. 2002, 55, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Cordonnier, D.; Martin, H.; Groslambert, P.; Micouin, C.; Chenais, F.; Stoebner, P. Mixed IgG-IgM cryoglobulinemia with glomerulonephritis. Immunochemical, fluorescent and ultrastructural study of kidney and in vitro cryoprecipitate. Am. J. Med. 1975, 59, 867–872. [Google Scholar] [CrossRef]
- Frankel, A.H.; Singer, D.R.; Winearls, C.G.; Evans, D.J.; Rees, A.J.; Pusey, C.D. Type II essential mixed cryoglobulinaemia: Presentation, treatment and outcome in 13 patients. Q. J. Med. 1992, 82, 101–124. [Google Scholar] [PubMed]
- Tarantino, A.; De Vecchi, A.; Montagnino, G.; Imbasciati, E.; Mihatsch, M.J.; Zollinger, H.U.; Di Belgiojoso, G.B.; Busnach, G.; Ponticelli, C. Renal disease in essential mixed cryoglobulinaemia. Long-term follow-up of 44 patients. Q. J. Med. 1981, 50, 1–30. [Google Scholar] [PubMed]
- Artemova, M.; Abdurakhmanov, D.; Ignatova, T.; Mukhin, N. Persistent Hepatitis C virus-associated cryoglobulinemic vasculitis following virus eradication after direct-acting antiviral therapy. Hepatology 2017, 65, 1770–1771. [Google Scholar] [CrossRef] [PubMed]
- Mazzaro, C.; Dal Maso, L.; Quartuccio, L.; Ghersetti, M.; Lenzi, M.; Mauro, E.; Bond, M.; Casarin, P.; Gattei, V.; Crosato, I.M.; et al. Long-term effects of the new direct antiviral agents (DAAs) therapy for HCV-related mixed cryoglobulinaemia: A multicentre open-label study. Clin. Exp. Rheumatol. 2018. (Epub ahead of print). [Google Scholar] [PubMed]
- Mazzaro, C.; De Re, V.; Spina, M.; Dal Maso, L.; Festini, G.; Comar, C.; Tirelli, U.; Pozzato, G. Pegylated-interferon plus ribavirin for HCV-positive indolent non-Hodgkin lymphomas. Br. J. Haematol. 2009, 145, 255–257. [Google Scholar] [CrossRef] [PubMed]
- Merli, M.; Carli, G.; Arcaini, L.; Visco, C. Antiviral therapy of Hepatitis C as curative treatment of indolent B-cell lymphoma. World J. Gastroenterol. 2016, 22, 8447–8458. [Google Scholar] [CrossRef] [PubMed]
- Conca, P.; Cafaro, G.; De Renzo, A.; Coppola, A.; Cimino, E.; Tarantino, G. Successful and Safe Long-Term Standard Antiviral Therapy in a Patient with “Explosive” Immune Response in Course of HCV-Related Liver Cirrhosis. Int. J. Mol. Sci. 2015, 16, 14075–14085. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Cases (246) | Type II MC (191 Cases) | Type III MC (55 Cases) | p Type II vs. Type III |
|---|---|---|---|---|
| Male/Female ratio | 0.53 | 0.52 | 0.57 | ns |
| Mean age at the diagnosis (range) | 60 (26–83) | 60 (26–77) | 60 (34–83) | ns |
| Mean follow-up (years) (range) | 9.2 (1–27) | 9.0 (1–10) | 9.7 (0.5–10) | ns |
| Clinical features at presentation | ||||
| Purpura (%) | 177 (72%) | 148 (77%) | 29 (53%) | <0.01 |
| Arthralgias (%) | 143 (58%) | 120 (63%) | 23 (42%) | <0.04 |
| Sicca syndrome (%) | 22 (9%) | 21 (11%) | 1 (2%) | ns |
| Raynaud phenomenon (%) | 34 (14%) | 29 (15%) | 5 (9%) | ns |
| Skin ulcers (%) | 7 (3%) | 7 (4%) | 0 | ns |
| Peripheral neuropathy (%) | 52 (21%) | 47 (25%) | 5 (9%) | <0.03 |
| Chronic hepatitis (%) | 173 (70%) | 134 (70%) | 39 (71%) | ns |
| Glomerulonephritis (%) | 19 (8%) | 17 (9%) | 2 (4%) | ns |
| Non-Hodgkin’s lymphoma (%) | 38 (15%) | 35 (18%) | 3 (5%) | <0.01 |
| Biochemical and virological features | ||||
| Cryocrit (%) | 3.8 ± 4.0 | 4.6 ± 4.6 | 2.0 ± 1.5 | <0.05 |
| Rheumatoid factor (U/L) NV < 40 | 296 ± 691 | 343 ± 748 | 157 ± 382 | <0.03 |
| C4 NV > 10 | 9.4 ± 7.0 | 9.0 ± 7.3 | 10 ± 4.5 | <0.04 |
| Anti-HCV antibodies | 238 | |||
| HCV genotype 1–4 | 116 (47%) | 93 (49%) | 23 (42%) | ns |
| HCV genotype 2–3 | 34 (14%) | 22 (12%) | 12 (23%) | ns |
| HBsAg | 11 (4.5%) | 8 (5%) | 3 (5%) | |
| Anti-HBs | 22 (9%) | 14 (7%) | 6 (11%) | ns |
| AST U/L NV < 36 | 66 ± 64 | 68 ± 61 | 60 ± 37 | ns |
| ALT U/L NV < 45 | 69 ± 58 | 71 ± 62 | 62 ± 38 | ns |
| GGT U/L NV < 36 | 66 ± 23 | 68 ± 22 | 63 ± 24 | ns |
| Creatinine NV < 1.0 mg% | 1.0 ± 0.2 | 1.0 ± 0.2 | 1.0 ± 0.2 | ns |
| Outcomes | ||||
| Death | 72 (29%) | 63 (33%) | 9 (17%) | <0.05 |
| Causes of Death | All Patients | Type II MC | Type III MC |
|---|---|---|---|
| Liver cirrhosis | 38 | 32 (51%) | 6 (67%) |
| Heart failure | 11 | 10 (16%) | 1 (11%) |
| Renal insufficiency | 8 | 6 (10%) | 2 (22%) |
| Severe infections | 8 | 8 (13%) | 0 |
| Vasculitis | 3 | 3 (5%) | 0 |
| B-cell lymphoma | 3 | 3 (5%) | 0 |
| Myocardial infarction | 1 | 1 (2%) | 0 |
| Total cases | 72 | 63 | 9 |
| Type of Therapy | All Patients | CM Type II | CM Type III | Clinical Response | Immunological Response | SVR | Refractory Disease | Severe Infection after Therapy |
|---|---|---|---|---|---|---|---|---|
| IFN as monotherapy (%) | 61 | 50 | 11 | 15 (24%) | 14 (22%) | 15 (4%) | 6 (9%) | 2 (3%) |
| IFN+Ribavirine (%) | 20 | 15 | 5 | 8 (40%) | 4 (20%) | 8 (40%) | 2 (10%) | 1 (5%) |
| Peg-IFN + Ribavirine (%) | 21 | 18 | 3 | 7 (33%) | 4 (19%) | 7 (33%) | 6 (28%) | 0 |
| Corticosteroids alone (%) | 52 | 43 | 9 | 4 (7%) | 3 (6%) | 0 | 12 (23%) | 2 (3%) |
| Alkylant + Corticosteroids (%) | 8 | 8 | 0 | 3 (37%) | 3 (37%) | 0 | 3 (37%) | 2 (25%) |
| Plasmaferesys + steroids (%) | 12 | 11 | 1 | 4 (33%) | 4 (33%) | 0 | 1 (8%) | 1 (8%) |
| Rituximab (%) | 6 | 6 | 0 | 4 (66%) | 4 (66%) | 0 | 2 (33%) | 1 (16%) |
| DAAs (%) | 19 | 14 | 5 | 8 (42%) | 6 (32%) | 19 (100%) | 1 (5%) | 0 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazzaro, C.; Dal Maso, L.; Mauro, E.; Gattei, V.; Ghersetti, M.; Bulian, P.; Moratelli, G.; Grassi, G.; Zorat, F.; Pozzato, G. Survival and Prognostic Factors in Mixed Cryoglobulinemia: Data from 246 Cases. Diseases 2018, 6, 35. https://doi.org/10.3390/diseases6020035
Mazzaro C, Dal Maso L, Mauro E, Gattei V, Ghersetti M, Bulian P, Moratelli G, Grassi G, Zorat F, Pozzato G. Survival and Prognostic Factors in Mixed Cryoglobulinemia: Data from 246 Cases. Diseases. 2018; 6(2):35. https://doi.org/10.3390/diseases6020035
Chicago/Turabian StyleMazzaro, Cesare, Luigino Dal Maso, Endri Mauro, Valter Gattei, Michela Ghersetti, Pietro Bulian, Giulia Moratelli, Gabriele Grassi, Francesca Zorat, and Gabriele Pozzato. 2018. "Survival and Prognostic Factors in Mixed Cryoglobulinemia: Data from 246 Cases" Diseases 6, no. 2: 35. https://doi.org/10.3390/diseases6020035
APA StyleMazzaro, C., Dal Maso, L., Mauro, E., Gattei, V., Ghersetti, M., Bulian, P., Moratelli, G., Grassi, G., Zorat, F., & Pozzato, G. (2018). Survival and Prognostic Factors in Mixed Cryoglobulinemia: Data from 246 Cases. Diseases, 6(2), 35. https://doi.org/10.3390/diseases6020035