Attitudes and Recommendations of Physicians towards Alcohol Consumption and Cardiovascular Health: A Perspective from Argentina

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design
2.3. Study Distribution
2.4. Statistical Analysis
3. Results
3.1. Population Demographics
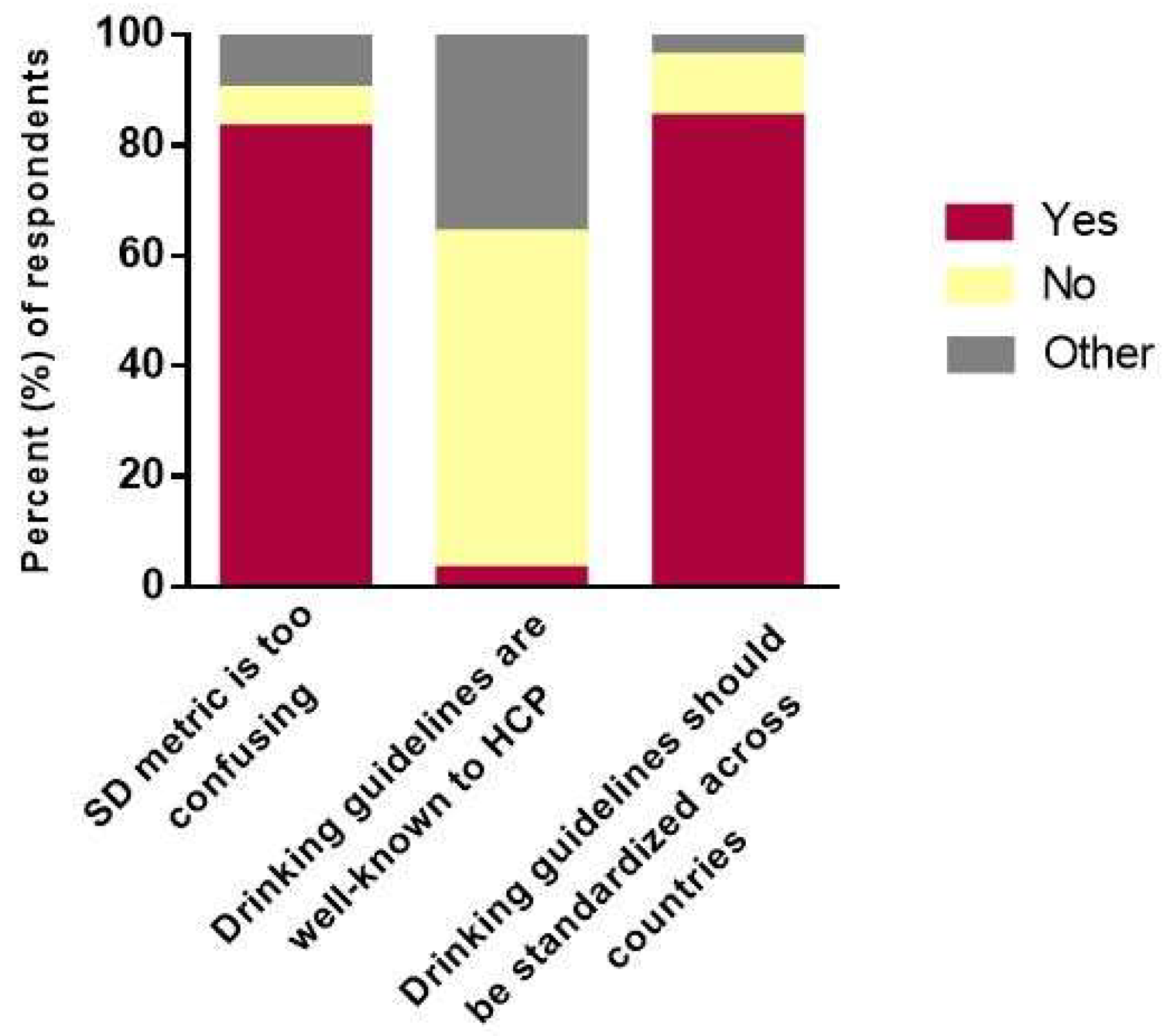
3.2. Perceptions on Alcohol and Cardiovascular Health
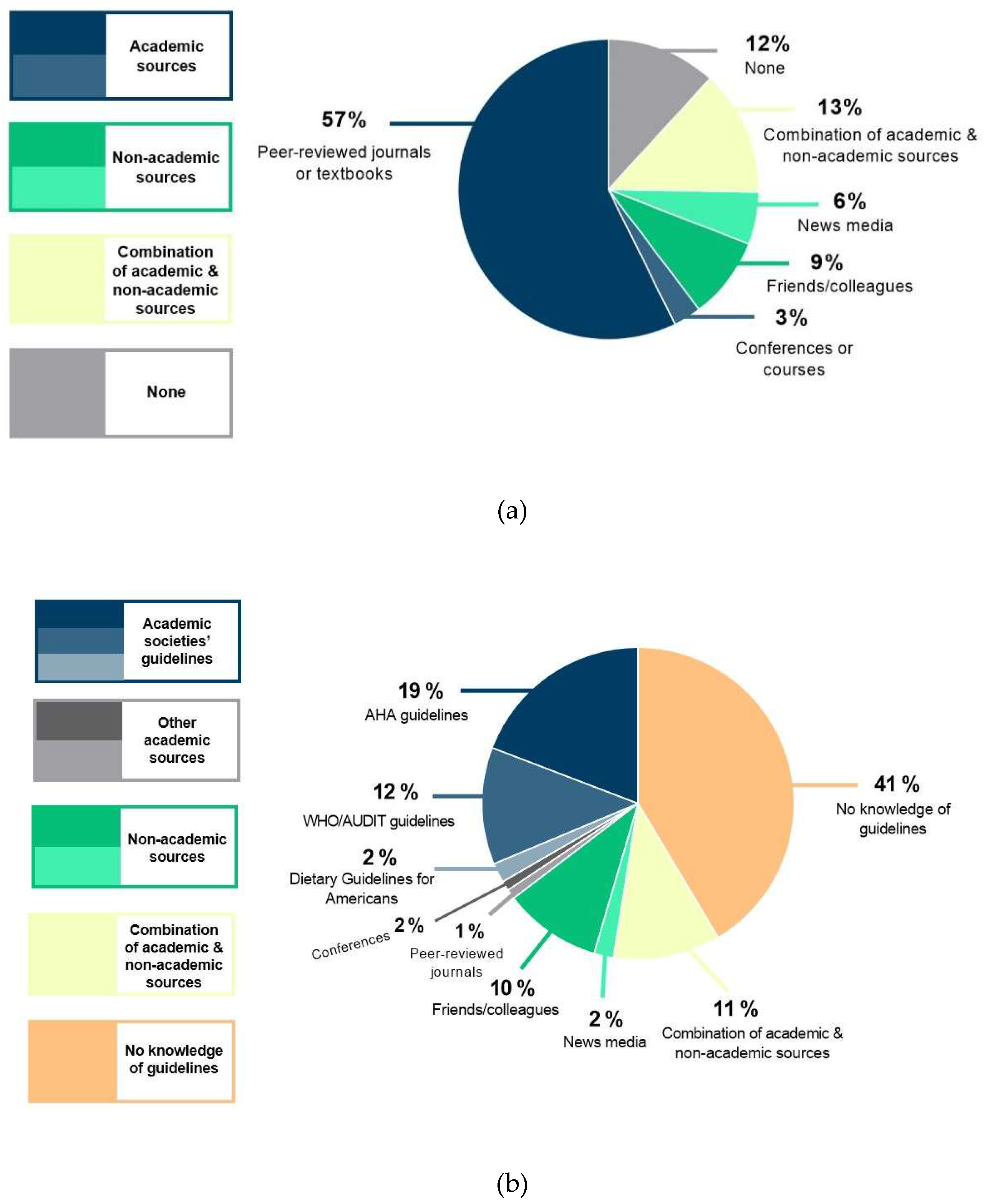
3.3. Knowledge of Drinking Guidelines
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Haseeb, S.; Alexander, B.; Baranchuk, A. Wine and cardiovascular health: A comprehensive review. Circulation 2017, 136, 1434–1448. [Google Scholar] [CrossRef] [PubMed]
- Haseeb, S.; Alexander, B.; Santi, R.L.; Liprandi, A.S.; Baranchuk, A. What’s in wine? A clinician’s perspective. Trends Cardiovasc. Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Baranchuk, A.; Haseeb, S.; Alexander, B. Wine Consumption and Cardiovascular Health: An Expert Opinion. Intern Soc Cardiovas Pharmacother, 2018. Available online: http://www.iscpcardio.org/expert-opinions/wine-consumption-and-cardiovascular-health-an-expert-opinion/ (accessed on 1 May 2018).
- International Organisation of Vine and Wine OIV Statistical Report on World Vitiviniculture. Available online: http://www.oiv.int/public/medias/5958/oiv-state-of-the-vitiviniculture-world-market-april-2018.pdf (accessed on 5 July 2018).
- O′Keefe, E.L.; DiNicolantonio, J.J.; O′Keefe, J.H.; Lavie, C.J. Alcohol and CV health: Jekyll and Hyde J-curves. Prog. Cardiovasc. Dis. 2018, 61, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.; Roerecke, M. Cardiovascular effects of alcohol consumption. Trends Cardiovasc. Med. 2017, 27, 534–538. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Solà, J. Cardiovascular risks and benefits of moderate and heavy alcohol consumption. Nat. Rev. Cardiol. 2015, 12, 576–587. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.; Mathers, C.; Popova, S.; Thavorncharoensap, M.; Teerawattananon, Y.; Patra, J. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet 2009, 373, 2223–2233. [Google Scholar] [CrossRef]
- Rehm, J.; Gmel, G.E.; Gmel, G.; Hasan, O.S.M.; Imtiaz, S.; Popova, S.; Probst, C.; Roerecke, M.; Room, R.; Samokhvalov, A.V.; et al. The relationship between different dimensions of alcohol use and the burden of disease—An update. Addiction 2017, 112, 968–1001. [Google Scholar] [CrossRef] [PubMed]
- O′Keefe, J.H.; Bhatti, S.K.; Bajwa, A.; DiNicolantonio, J.J.; Lavie, C.J. Alcohol and cardiovascular health: The dose makes the poiso or the remedy. Mayo Clin. Proc. 2014, 89, 382–393. [Google Scholar] [CrossRef] [PubMed]
- Roerecke, M.; Rehm, J. Alcohol consumption, drinking patterns, and ischemic heart disease: A narrative review of meta-analyses and a systematic review and meta-analysis of the impact of heavy drinking occasions on risk for moderate drinkers. BMC Med. 2014, 12, 182. [Google Scholar] [CrossRef] [PubMed]
- Ronksley, P.E.; Brien, S.E.; Turner, B.J.; Mukamal, K.J.; Ghali, W.A. Association of alcohol consumption with selected cardiovascular disease outcomes: A systematic review and meta-analysis. BMJ 2011, 342, d671. [Google Scholar] [CrossRef] [PubMed]
- Roerecke, M.; Rehm, J. The cardioprotective association of average alcohol consumption and ischaemic heart disease: A systematic review and meta-analysis. Addiction 2012, 107, 1246–1260. [Google Scholar] [CrossRef] [PubMed]
- Haseeb, S.; Alexander, B.; Baranchuk, A. Response by Haseeb et al to letter regarding article, “Wine and Cardiovascular Health: A comprehensive review”. Circulation 2018, 137, 1880–1881. [Google Scholar] [CrossRef] [PubMed]
- Baranchuk, A.; Alexander, B.; Haseeb, S. Drinking Red Wine is Good for You—or Maybe Not. The Washington Post. 2017. Available online: https://www.washingtonpost.com/national/health-science/drinking-red-wine-is-good-for-you--or-maybe-not/2017/12/01/49f55e7a-cbd3-11e7-aa96-54417592cf72_story.html (accessed on 1 May 2018).
- Kloner, R.A.; Rezkalla, S.H. To drink or not to drink? That is the question. Circulation 2007, 116, 1306–1317. [Google Scholar] [CrossRef] [PubMed]
- Naimi, T.S.; Stockwell, T.; Zhao, J.; Xuan, Z.; Dangardt, F.; Saitz, R.; Liang, W.; Chikritzhs, T. Selection biases in observational studies affect associations between ‘moderate’ alcohol consumption and mortality. Addiction 2017, 112, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Bakhshi, S.; While, A.E. Health professionals’ alcohol-related professional practices and the relationship between their personal alcohol attitudes and behavior and professional practices: A systematic review. Int. J. Environ. Res. Public Health 2013, 11, 218–248. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.; Diehl, K.; Bock, C.; Herr, R.M.; Mayer, M.; Görig, T. Modifying health behavior to prevent cardiovascular diseases: A nationwide survey among German primary care physicians. Int. J. Environ. Res. Public Health 2014, 11, 4218–4232. [Google Scholar] [CrossRef] [PubMed]
- Tough, S.C.; Clarke, M.; Hicks, M.; Clarren, S. Variation in health care provider definitions of moderate consumption of alcohol as related to recommendations regarding alcohol consumption during pregnancy: Results from a Canadian survey. Ther. Drug Monit. 2005, 27, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Kalinowski, A.; Humphreys, K. Governmental standard drink definitions and low-risk alcohol consumption guidelines in 37 countries. Addiction 2016, 111, 1293–1298. [Google Scholar] [CrossRef] [PubMed]
- NMHRC Australian Guidelines to Reduce Health Risks from Drinking Alcohol. Available online: https://www. nhmrc.gov.au/health-topics/alcohol-guidelines (accessed on 15 July 2018).
- Connor, J.; Hall, W. Thresholds for safer alcohol use might need lowering. Lancet 2018, 391, 1460–1461. [Google Scholar] [CrossRef]
- Baranchuk, A.; Haseeb, S.; Alexander, B. Alcohol Consumption Guidelines: International Discrepancies and Variations. BMJ 2018. Available online: https://www.bmj.com/content/361/bmj.k1630/rr-1 (accessed on 20 July 2018).
- Wood, A.M.; Kaptoge, S.; Butterworth, A.S.; Willeit, P.; Warnakula, S.; Bolton, T.; Paige, E.; Paul, D.S.; Sweeting, M.; Burgess, S.; et al. Risk thresholds for alcohol consumption: Combined analysis of individual-participant data for 599 912 current drinkers in 83 prospective studies. Lancet 2018, 391, 1513–1523. [Google Scholar] [CrossRef]
- Wise, J. Study backs alcohol UK limit of six glasses of wine a week. BMJ 2018, 361, k1630. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health and Human Services Dietary Guidelines for Americans 2015–2020. Available online: https://health.gov/dietaryguidelines/2015/guidelines/appendix-9/ (accessed on 10 July 2018).
- Kerr, W.C.; Stockwell, T. Understanding standard drinks and drinking guidelines. Drug Alcohol. Rev. 2012, 31, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Babor, T.F.; Higgins-Biddle, J.C. Brief Intervention for Hazardous and Harmful Drinking: A Manual for Use in Primary Care. World Health Organization, 2001. Available online: http://apps.who.int/iris/handle/10665/67210 (accessed on 12 July 2018).
- Department of Health UK Chief Medical Officers’ Alcohol Guidelines Review: Summary of the Proposed New Guidelines. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/545739/GDG_report-Jan2016.pdf (accessed on 12 July 2018).
- Goldberg, I.J.; Mosca, L.; Piano, M.R.; Fisher, E.A. Wine and your heart. Circulation 2001, 103, 472–475. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, A.H.; Appel, L.J.; Brands, M.; Carnethon, M.; Daniels, S.; Franch, H.A.; Franklin, B.; Kris-Etherton, P.; Harris, W.S.; Howard, B.; et al. Diet and lifestyle recommendations revision 2006. Circulation 2006, 114, 82–96. [Google Scholar] [CrossRef] [PubMed]
- Furie, K.L.; Kasner, S.E.; Adams, R.J.; Albers, G.W.; Bush, R.L.; Fagan, S.C.; Halperin, J.L.; Johnston, S.C.; Katzan, I.; Kernan, W.N.; et al. Guidelines for the prevention of stroke in patients with stroke or transient ischemic attack: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2011, 42, 227–276. [Google Scholar] [CrossRef] [PubMed]
- Hypertension ASo My Blood Pressure Guide-HTN Risks. Available online: http://www.ashus. org/ASH-Patient-Portal/Get-Information/HTN-Risks.aspx (accessed on 20 July 2018).
- American Diabetes Association Food & Fitness-Alcohol. Available online: http://www.diabetes.org/food-and-fitness/food/what-can-i-eat/making-healthy-food-choices/alcohol.html (accessed on 20 July 2018).



{kind=link}
{kind=link}
| Variable | All Respondents 1 (n = 745) | Respondents Location 1 | p-Value | |
|---|---|---|---|---|
| Non-Producer Regions (n = 467) | Producer Regions (n = 278) | |||
| Age, n (%) | 0.068 | |||
| <35 years | 116 (16) | 63 (14) | 53 (19) | |
| 35–44 years | 199 (27) | 116 (25) | 83 (30) | |
| 45–54 years | 202 (27) | 134 (29) | 68 (25) | |
| 55–64 years | 145 (20) | 100 (22) | 45 (16) | |
| >65 years | 72 (10) | 46 (10) | 26 (10) | |
| Gender, n (%) | 0.492 | |||
| Male | 524 (71) | 324 (70) | 200 (72) | |
| Female | 217 (29) | 140 (30) | 77 (28) | |
| Clinical practice setting, n (%) | ||||
| Urban or rural | 0.721 | |||
| Urban | 712 (95) | 444 (95) | 268 (96) | |
| Rural | 2 (1) | 1 (1) | 1 (1) | |
| Both | 29 (4) | 20 (4) | 9 (3) | |
| Academic or non-academic | <0.001 | |||
| University hospital (A) | 194 (26) | 142 (31) | 52 (19) | |
| Private academic (A) | 12 (2) | 9 (2) | 3 (1) | |
| Private hospital (NA) | 238 (32) | 155 (33) | 83 (30) | |
| Private clinic (NA) | 224 (30) | 123 (27) | 101 (37) | |
| Community hospital (NA) | 63 (9) | 29 (6) | 34 (12) | |
| Other (NA) | 10 (1) | 6 (1) | 4 (1) | |
| Variable | All Respondents 1 (n = 745) | Gender 1 | p-Value | |
|---|---|---|---|---|
| Male (n = 524) | Female (n = 217) | |||
| Knowledge of drinking guidelines | ||||
| Satisfaction with own knowledge, mean ± SD 2 | 3.01 ± 2.73 | 3.25 ± 2.73 | 2.47 ± 2.50 | <0.001 |
| Satisfaction in guiding patients, mean ± SD 2 | 6.22 ± 3.20 | 6.39 ± 3.11 | 5.92 ± 3.34 | 0.071 |
| Knowledge of drinking metric units | ||||
| Aware of metric “standard drink”, n (%) | 0.099 | |||
| Yes | 301 (41) | 217 (42) | 83 (39) | |
| No | 351 (47) | 250 (48) | 98 (45) | |
| Maybe | 87 (12) | 53 (10) | 34 (16) | |
| Satisfaction with converting standard drinks to other metrics, mean ± SD 2 | 1.78 ± 2.52 | 1.90 ± 2.57 | 1.50 ± 2.38 | 0.052 |
| Respondents, n | |
|---|---|
| Lectures and conferences | 426 |
| Website | 349 |
| Interactive smartphone app | 322 |
| Media campaigns and workshops | 3 |
| No need for strategies | 18 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopez Santi, R.; Haseeb, S.; Alexander, B.; D′Ovidio, A.; Gimenez, S.; Secotaro, C.; Martinez Demaria, D.; Pupi, L.M.; Costantini, S.; Piskorz, D.; et al. Attitudes and Recommendations of Physicians towards Alcohol Consumption and Cardiovascular Health: A Perspective from Argentina. Diseases 2018, 6, 77. https://doi.org/10.3390/diseases6030077
Lopez Santi R, Haseeb S, Alexander B, D′Ovidio A, Gimenez S, Secotaro C, Martinez Demaria D, Pupi LM, Costantini S, Piskorz D, et al. Attitudes and Recommendations of Physicians towards Alcohol Consumption and Cardiovascular Health: A Perspective from Argentina. Diseases. 2018; 6(3):77. https://doi.org/10.3390/diseases6030077
Chicago/Turabian StyleLopez Santi, Ricardo, Sohaib Haseeb, Bryce Alexander, Adrian D′Ovidio, Sergio Gimenez, Carlos Secotaro, Diego Martinez Demaria, Luis Maria Pupi, Sonia Costantini, Daniel Piskorz, and et al. 2018. "Attitudes and Recommendations of Physicians towards Alcohol Consumption and Cardiovascular Health: A Perspective from Argentina" Diseases 6, no. 3: 77. https://doi.org/10.3390/diseases6030077
APA StyleLopez Santi, R., Haseeb, S., Alexander, B., D′Ovidio, A., Gimenez, S., Secotaro, C., Martinez Demaria, D., Pupi, L. M., Costantini, S., Piskorz, D., Amarilla, A., Lorenzatti, A., Gutierrez, N., Hopman, W., & Baranchuk, A. (2018). Attitudes and Recommendations of Physicians towards Alcohol Consumption and Cardiovascular Health: A Perspective from Argentina. Diseases, 6(3), 77. https://doi.org/10.3390/diseases6030077