Emerging Therapeutic Targets and Experimental Drugs for the Treatment of NAFLD

 , and
, and
Abstract
1. Introduction
2. Pathophysiology and Pathogenesis of NAFLD
3. Treatment Guidelines
4. Potential Drug Targets for the Treatment of NAFLD
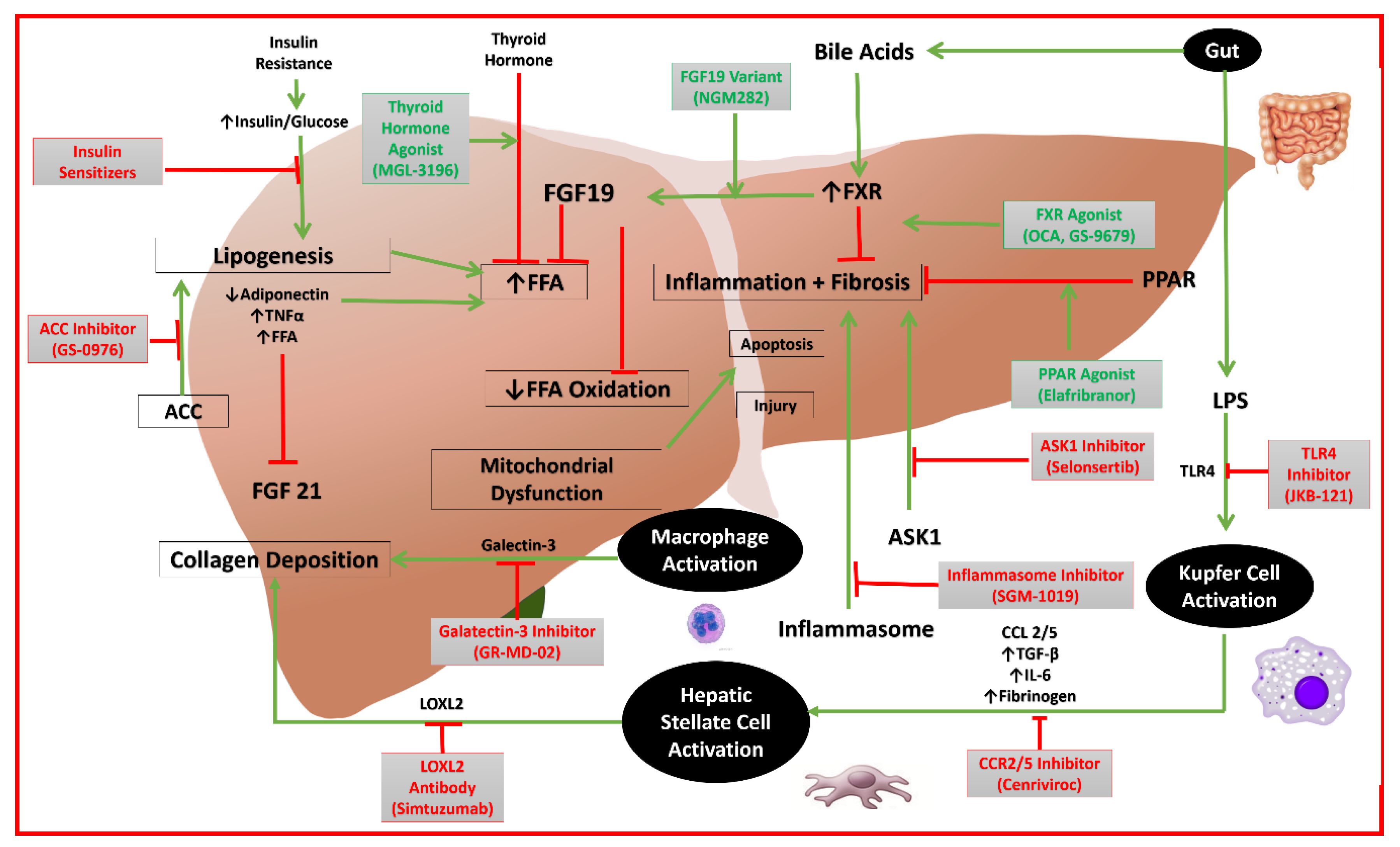
4.1. Obeticholic Acid and GS-9674—Farnesoid X Receptor Agonists
4.2. Elafibranor: A Dual Peroxisome Proliferator-Activated Receptor (PPAR) Alpha/Delta Agonist
4.3. Cencriviroc: CCR2/CCR5 Dual Antagonist
4.4. GR-MD-02: Galectin-3 Protein Inhibitor
4.5. NGM282: Variant of FGF19
4.6. MGL-3196: Selective Thyroid Hormone Receptor-Beta Agonist
4.7. Selonsertib: Apoptosis Signal-Regulating Kinase 1 Inhibitor
4.8. GS-0976: Acentyl-Coenzyme A Carboxylase Inhibitor
4.9. SGM-1019: Inflammasome Inhibitor
4.10. Simtuzumab: Anti-LOXL2 Antibody
4.11. JKB-121: TLR4 Antagonism
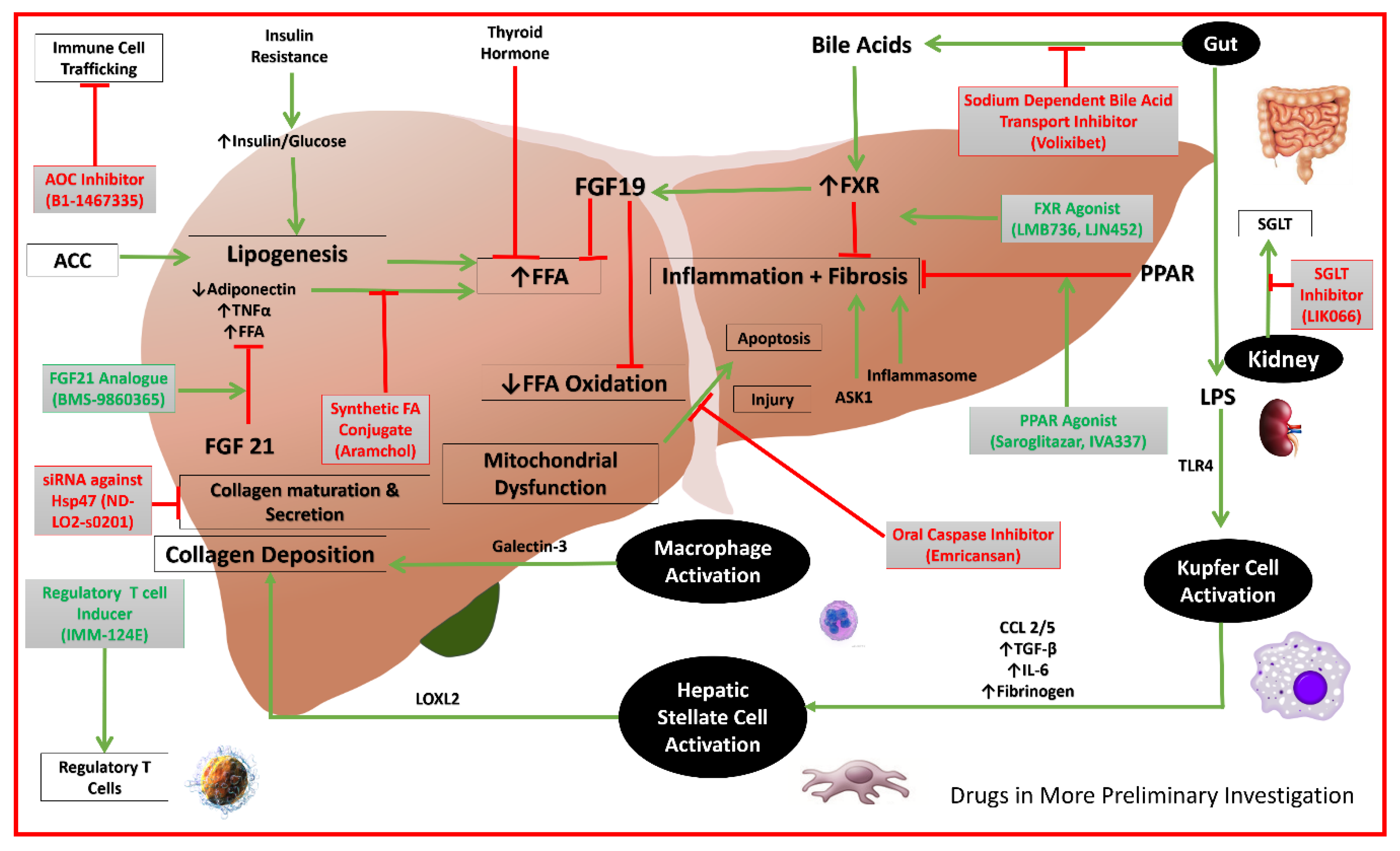
4.12. Additional Drugs in Phase 2a
5. Future Directions
6. Conclusions
Funding
Conflicts of Interest
References
- European Association for the Study of the Liver, & European Association for the Study of Diabetes. EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. Obes. Facts 2016, 9, 65–90. [Google Scholar] [CrossRef] [PubMed]
- Chitturi, S.; Wong, V.W.S.; Chan, W.K.; Wong, G.L.H.; Wong, S.K.H.; Sollano, J.; Ni, Y.H.; Liu, C.J.; Lesmana, L.A.; Kim, S.U. The Asia-pacific Working Party on Non-alcoholic Fatty Liver Disease guidelines 2017—Part 2: Management and special groups. J. Gastroenterol. Hepatol. 2018, 33, 86–98. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.L.; Ratziu, V.; Harrison, S.A.; Abdelmalek, M.F.; Aithal, G.P.; Caballeria, J.; Francque, S.; Farrell, G.; Kowdley, K.V.; Craxi, A.; et al. A randomized, placebo-controlled trial of cenicriviroc for treatment of nonalcoholic steatohepatitis with fibrosis. Hepatology 2018, 67, 1754–1767. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.A.; Rinella, M.E.; Abdelmalek, M.F.; Trotter, J.F.; Paredes, A.H.; Arnold, H.L.; Kugelmas, M.; Bashir, M.R.; Jaros, M.J.; Ling, L.; et al. NGM282 for treatment of non-alcoholic steatohepatitis: A multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet 2018, 391, 1174–1185. [Google Scholar] [CrossRef]
- Harrison, S.; Moussa, S.; Bashir, M.; Alkhouri, N.; Frias, J.; Baum, S.; Tetri, B.; Bansal, M.; Taub, R. MGL-3196, a selective thyroid hormone receptor-beta agonist significantly decreases hepatic fat in NASH patients at 12 weeks, the primary endpoint in a 36-week serial liver biopsy study. J. Hepatol. 2018, 68, S38. [Google Scholar] [CrossRef]
- Loomba, R.; Lawitz, E.; Mantry, P.S.; Jayakumar, S.; Caldwell, S.H.; Arnold, H.; Deihl, A.M.; Djedjos, C.S.; Han, L.; Myers, R.P.; et al. The ASK1 inhibitor selonsertib in patients with nonalcoholic steatohepatitis: A randomized, phase 2 trial. Hepatology 2018, 67, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Nelson, C.H.; Kirby, B.J.; Lu, N.; McColgan, B.; Djedjos, C.S.; Myers, R.P.; Cuvin, J.; Qin, A.; Mathias, A. Pharmacokinetics of selonsertib, GS-9674, and/or GS-0976 in combination in healthy subjects. J. Hepatol. 2017, 66, S151–S152. [Google Scholar] [CrossRef]
- Dabbagh, K.; Dodson, G.S.; Yamamoto, L.; Baeza-Raja, B.; Goodyear, A.W. Preclinical and first-in human development of SGM-1019, a first-in-class novel small molecule modulator of inflammasome activity for the treatment of nonalcoholic steatohepatitis (NASH). J. Hepatol. 2018, 68, S60. [Google Scholar] [CrossRef]
- Sanyal, A.; Abdelmalek, M.F.; Diehl, A.M.; Caldwell, S.; Shiffman, M.L.; Ghalib, R.; Lawitz, E.; Rockey, D.C.; Schall, R.A.; Jia, C.; et al. Efficacy and safety of simtuzumab for the treatment of nonalcoholic steatohepatitis with bridging fibrosis or cirrhosis: Results of two phase 2b, dose-ranging, randomized, placebo-controlled trials. J. Hepatol. 2017, 66, S54. [Google Scholar] [CrossRef]
- Machado, M.V.; Diehl, A.M. Pathogenesis of Nonalcoholic Steatohepatitis. Gastroenterology 2016, 150, 1769–1777. [Google Scholar] [CrossRef] [PubMed]
- Federico, A.; Zulli, C.; de Sio, I.; Del Prete, A.; Dallio, M.; Masarone, M.; Loguercio, C. Focus on emerging drugs for the treatment of patients with non-alcoholic fatty liver disease. World J. Gastroenterol. 2014, 20, 16841–16857. [Google Scholar] [CrossRef] [PubMed]
- Liles, J.T.; Karnik, S.; Hambruch, E.; Kremoser, C.; Birkel, M.; Watkins, W.J.; Tumas, D.; Breckenridge, D.; French, D. FXR agonism by GS-9674 decreases steatosis and fibrosis in a murine model of NASH. J. Hepatol. 2016, 64, S169. [Google Scholar] [CrossRef]
- Adorini, L.; Pruzanski, M.; Shapiro, D. Farnesoid X receptor targeting to treat nonalcoholic steatohepatitis. Drug Discov. Today 2012, 17, 988–997. [Google Scholar] [CrossRef] [PubMed]
- Kong, B.; Luyendyk, J.P.; Tawfik, O.; Guo, G.L. Farnesoid X receptor deficiency induces nonalcoholic steatohepatitis in low-density lipoprotein receptor-knockout mice fed a high-fat diet. J. Pharmacol. Exp. Ther. 2009, 328, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Mudaliar, S.; Henry, R.R.; Sanyal, A.J.; Morrow, L.; Marschall, H.U.; Kipnes, M.; Adorini, L.; Sciacca, C.I.; Clopton, P.; Castelloe, E.; et al. Efficacy and safety of the farnesoid X receptor agonist obeticholic acid in patients with type 2 diabetes and nonalcoholic fatty liver disease. Gastroenterology 2013, 145, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Neuschwander-Tetri, B.A.; Loomba, R.; Sanyal, A.J.; Lavine, J.E.; Van Natta, M.L.; Abdelmalek, M.F.; Abdelmalek, M.; Chalasani, N.; Dasarthy, S.; Diehl, A.M.; et al. Farnesoid X nuclear receptor ligand obeticholic acid for non-cirrhotic, non-alcoholic steatohepatitis (FLINT): A multicentre, randomised, placebo-controlled trial. Lancet 2015, 385, 956–965. [Google Scholar] [CrossRef]
- Hameed, B.; Terrault, N.A.; Gill, R.M.; Loomba, R.; Chalasani, N.; Hoofnagle, J.H.; Van Natta, M.L.; McCullough, A.J. Clinical and metabolic effects associated with weight changes and obeticholic acid in non-alcoholic steatohepatitis. Aliment. Pharmacol. Ther. 2018, 47, 645–656. [Google Scholar] [CrossRef] [PubMed]
- Ratziu, V.; Sanyal, A.J.; MacConell, L.; Shringarpure, R.; Marmon, T.; Shapiro, D.; Younossi, Z.M. Regenerate: A phase 3, double-blind, randomized, placebo-controlled multicenter study of obeticholic acid therapy for nonalcoholic steatohepatitis. J. Hepatol. 2016, 64, S294–S295. [Google Scholar] [CrossRef]
- Randomized Global Phase 3 Study to Evaluate the Impact on NASH with Fibrosis of Obeticholic Acid Treatment. 28 May 2018. Available online: https://clinicaltrials.gov/ct2/show/NCT02548351 (accessed on 18 June 2018).
- Myers, R.P.; Djedjos, C.; Kirby, B.; Bilin, A.; Khan, M.; Gosink, J.; Song, Q.; Srihari, R. A198 pharmacodynamic effects of the oral, non-steroidal farnesoid X receptor agonist GS-9674 in healthy volunteers. J. Can. Assoc. Gastroenterol. 2018, 1 (Suppl. S1), 346. [Google Scholar] [CrossRef]
- Evaluating the Safety, Tolerability, and Efficacy of GS-9674 in Participants with Nonalcoholic Steatohepatitis (NASH). 17 January 2018. Available online: https://clinicaltrials.gov/ct2/show/NCT02854605 (accessed on 14 June 2018).
- Pawlak, M.; Lefebvre, P.; Staels, B. Molecular mechanism of PPARα action and its impact on lipid metabolism, inflammation and fibrosis in non-alcoholic fatty liver disease. J. Hepatol. 2015, 62, 720–733. [Google Scholar] [CrossRef] [PubMed]
- Ratziu, V.; Harrison, S.A.; Francque, S.; Bedossa, P.; Lehert, P.; Serfaty, L.; Romero-Gomez, M.; Boursier, J.; Abdelmalek, M.; Caldwell, S.; et al. Elafibranor, an agonist of the peroxisome proliferator-activated receptor−α and−δ, induces resolution of nonalcoholic steatohepatitis without fibrosis worsening. Gastroenterology 2016, 150, 1147–1159. [Google Scholar] [CrossRef] [PubMed]
- Phase IIb Study to Evaluate the Efficacy and Safety of GFT505 Versus Placebo in Patients with Non-Alcoholic Steatohepatitis (NASH). 14 January 2016. Available online: https://clinicaltrials.gov/ct2/show/NCT01694849 (accessed on 16 June 2018).
- Satsangi, S.; Duseja, A. NASH: Do We Really Have an Effective Treatment? Available online: https://pdfs.semanticscholar.org/8b8b/c9600b3da4ec12ff759fa169f22b686c4e98.pdf (accessed on 16 June 2018).
- Phase 3 Study to Evaluate the Efficacy and Safety of Elafibranor Versus Placebo in Patients with Nonalcoholic Steatohepatitis (NASH). 14 May 2018. Available online: https://clinicaltrials.gov/ct2/show/NCT02704403 (accessed on 16 June 2018).
- Visseaux, B.; Charpentier, C.; Collin, G.; Bertine, M.; Peytavin, G.; Damond, F.; Matheron, S.; Lefebvre, E.; Brun-Vezinet, F.; Descamps, D.; et al. Cenicriviroc, a novel CCR5 (R5) and CCR2 antagonist, shows in vitro activity against R5 tropic HIV-2 clinical isolates. PLoS ONE 2015, 10, e0134904. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.; Sanyal, A.; Goodman, Z.; Lefebvre, E.; Gottwald, M.; Fischer, L.; Ratziu, V. Efficacy and safety study of cenicriviroc for the treatment of non-alcoholic steatohepatitis in adult subjects with liver fibrosis: CENTAUR Phase 2b study design. Contemp. Clin. Trials 2016, 47, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Seki, E.; De Minicis, S.; Inokuchi, S.; Taura, K.; Miyai, K.; Van Rooijen, N.; Schwabe, R.; Brenner, D.A. CCR2 promotes hepatic fibrosis in mice. Hepatology 2009, 50, 185–197. [Google Scholar] [CrossRef] [PubMed]
- Lefebvre, E.; Moyle, G.; Reshef, R.; Richman, L.P.; Thompson, M.; Hong, F.; Chou, H.; Hashiguchi, T.; Plato, C.; Poulin, D.; et al. Antifibrotic effects of the dual CCR2/CCR5 antagonist cenicriviroc in animal models of liver and kidney fibrosis. PLoS ONE 2016, 11, e0158156. [Google Scholar] [CrossRef] [PubMed]
- Miura, K.; Yang, L.; van Rooijen, N.; Ohnishi, H.; Seki, E. Hepatic recruitment of macrophages promotes nonalcoholic steatohepatitis through CCR2. Am. J. Physiol.-Gastrointest. Liver Physiol. 2012, 302, G1310–G1321. [Google Scholar] [CrossRef] [PubMed]
- Sanyal, A.J.; Chalasani, N.; Kowdley, K.V.; McCullough, A.; Diehl, A.M.; Bass, N.M.; Neuschwander-Tetri, B.; Lavine, J.E.; Tonascia, J.; Unalp, A.; et al. Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. N. Engl. J. Med. 2010, 362, 1675–1685. [Google Scholar] [CrossRef] [PubMed]
- Kruger, A.J.; Fuchs, B.C.; Masia, R.; Holmes, J.A.; Salloum, S.; Sojoodi, M.; Ferreira, D.S.; Rutledge, S.M.; Caravan, P.; Alatrakchi, N.; et al. Prolonged cenicriviroc therapy reduces hepatic fibrosis despite steatohepatitis in a diet-induced mouse model of nonalcoholic steatohepatitis. Hepatol. Commun. 2018, 2, 529–545. [Google Scholar] [CrossRef] [PubMed]
- Tacke, F. Cenicriviroc for the treatment of non-alcoholic steatohepatitis and liver fibrosis. Expert Opin. Investig. Drugs 2018, 27, 301–311. [Google Scholar] [CrossRef] [PubMed]
- AURORA: Phase 3 Study for the Efficacy and Safety of CVC for the Treatment of Liver Fibrosis in Adults with NASH. 13 February 2018. Available online: https://clinicaltrials.gov/ct2/show/NCT03028740 (accessed on 13 June 2018).
- Sumida, Y.; Yoneda, M. Current and future pharmacological therapies for NAFLD/NASH. J. Gastroenterol. 2018, 53, 362–376. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.A.; Marri, S.R.; Chalasani, N.; Kohli, R.; Aronstein, W.; Thompson, G.A.; Irish, W.; Miles, M.V.; Xanthakos, S.A.; Lawitz, E.; et al. Randomised clinical study: GR-MD-02, a galectin-3 inhibitor, vs. placebo in patients having non-alcoholic steatohepatitis with advanced fibrosis. Aliment. Pharmacol. Ther. 2016, 44, 1183–1198. [Google Scholar] [CrossRef] [PubMed]
- Traber, P.G.; Zomer, E. Therapy of Experimental NASH and Fibrosis with Galectin Inhibitors. PLoS ONE 2013, 8, e83481. [Google Scholar] [CrossRef] [PubMed]
- Banini, B.A.; Sanyal, A.J. Current and future pharmacologic treatment of nonalcoholic steatohepatitis. Curr. Opin. Gastroenterol. 2017, 33, 134. [Google Scholar] [CrossRef] [PubMed]
- Clinical Trial to Evaluation the Safety and Efficacy of GR-MD-02 for the Treatment of Liver Fibrosis and Resultant Portal Hypertension in Patients with Nash Cirrhosis. 14 February 2018. Available online: https://clinicaltrials.gov/ct2/show/NCT02462967 (accessed on 13 June 2018).
- Chlasani, N.; Garcia-Tsao, G.; Goodman, Z.; Abdelmalek, M.; Rinella, M.; Ryan, M.; Noureddin, M.; Jue, C.; Pyko, M.; Allgood, A.; et al. A Multicenter, Randomized, Double-Bind, Placebo-Controlled Trial of Galectin-3 Inhibitor (GR-MD-02) For One Year in Patients with NASH Cirrhosis and Portal Hypertension. 2018. Available online: http://investor.galectintherapeutics.com/static-files/a877f30d-b0b3-4db3-83eb-6840ccc5335b (accessed on 16 June 2018).
- Galectin Therapeutics Proceeds to Phase 3 Development of GR-MD-02 for NASH Cirrhosis Following FDA Meeting. 14 May 2018. Available online: https://www.nasdaq.com/press-release/galectin-therapeutics-proceeds-to-phase-3-development-of-grmd02-for-nash-cirrhosis-following-fda-20180514-00670 (accessed on 13 June 2018).
- Repana, D.; Ross, P. Targeting FGF19/FGFR4 Pathway: A Novel Therapeutic Strategy for Hepatocellular Carcinoma. Diseases 2015, 3, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, E.; Fu, L.; John, L.; Hultgren, B.; Huang, X.; Renz, M.; Stewart, T.A.; Stephan, J.P.; Tsai, S.P.; Powell-Braxton, L.; et al. Transgenic mice expressing human fibroblast growth factor-19 display increased metabolic rate and decreased adiposity. Endocrinology 2002, 143, 1741–1747. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, W.; Doughtie, A.; Cui, G.; Li, X.; Pandit, H.; Yang, Y.; Li, S.; Martin, R. Up-regulation of fibroblast growth factor 19 and its receptor associates with progression from fatty liver to hepatocellular carcinoma. Oncotarget 2016, 7, 52329–52339. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Learned, R.M.; Rossi, S.J.; DePaoli, A.M.; Tian, H.; Ling, L. Engineered FGF19 eliminates bile acid toxicity and lipotoxicity leading to resolution of steatohepatitis and fibrosis in mice. Hepatol. Commun. 2017, 1, 1024–1042. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Ko, B.; To, C.; Ling, L.; Rossi, S.; DePaoli, A.; Tian, H. P0932: Treatment with NGM282 significantly improves liver histopathology in a mouse model of non-alcoholic steatohepatitis (NASH). J. Hepatol. 2015, 62, S694. [Google Scholar] [CrossRef]
- Study of NGM282 in Patients with Nonalcoholic Steatohepatitis (NASH). 5 June 2018. Available online: https://clinicaltrials.gov/ct2/show/NCT02443116 (accessed on 16 June 2018).
- Dickson, I. NASH: Successful phase II trial of FGF19 analogue. Nat. Rev. Gastroenterol. Hepatol. 2018. [Google Scholar] [CrossRef] [PubMed]
- NGM Bio Reports Positive Results from Phase II Trial of NGM282. 16 April 2018. Available online: https://www.drugdevelopment-technology.com/news/ngm-bio-reports-positive-results-phase-ii-trial-ngm282/ (accessed on 13 June 2018).
- Brierley, R. The International Liver Congress 2018. Gastreonterol. Hepatol. 2018, 3, 379. [Google Scholar] [CrossRef]
- Kelly, M.J.; Pietranico-Cole, S.; Larigan, J.D.; Haynes, N.E.; Reynolds, C.H.; Scott, N.; Vermeulen, J.; Dvorozniak, M.; Conde-Knape, K.; Huang, K.; et al. Discovery of 2-[3,5-dichloro-4-(5-isopropyl-6-oxo-1, 6-dihydropyridazin-3-yloxy) phenyl]-3, 5-dioxo-2, 3, 4, 5-tetrahydro [1,2,4] triazine-6-carbonitrile (MGL-3196), a highly selective thyroid hormone receptor β agonist in clinical trials for the treatment of dyslipidemia. J. Med. Chem. 2014, 57, 3912–3923. [Google Scholar] [PubMed]
- Taub, R.; Chiang, E.; Chabot-Blanchet, M.; Kelly, M.J.; Reeves, R.A.; Guertin, M.C.; Tardif, J.C. Lipid lowering in healthy volunteers treated with multiple doses of MGL-3196, a liver-targeted thyroid hormone receptor-β agonist. Atherosclerosis 2013, 230, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Phase 2 Study of MGL-3196 in Patients with Non-Alcoholic Steatohepatitis (NASH). 19 December 2017. Available online: https://clinicaltrials.gov/ct2/show/NCT02912260 (accessed on 13 June 2018).
- Terry, M. Madrigal Pharma’s NASH Drug Has Positive Results in Phase II. 31 May 2018. Available online: https://www.biospace.com/article/madrigal-pharma-s-nash-drug-has-positive-results-in-phase-ii/ (accessed on 11 June 2018).
- Madrigal’s MGL-3196 Achieves Liver Biopsy Endpoints in Patients with Non-Alcoholic Steatohepatitis (NASH) at 36 Weeks in Phase 2 Clinical Trial. 31 May 2018. Available online: http://ir.madrigalpharma.com/news-releases/news-release-details/madrigals-mgl-3196-achieves-liver-biopsy-endpoints-patients-non (accessed on 13 June 2018).
- Wang, P.X.; Ji, Y.X.; Zhang, X.J.; Zhao, L.P.; Yan, Z.Z.; Zhang, P.; Shen, L.; Yang, X.; Fang, J.; Tian, S.; et al. Targeting CASP8 and FADD-like apoptosis regulator ameliorates nonalcoholic steatohepatitis in mice and nonhuman primates. Nat. Med. 2017, 23, 439. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, E.; Dong, Y.F.; Kataoka, K.; Yamashita, T.; Tokutomi, Y.; Matsuba, S.; Ichijo, H.; Ogawa, H.; Kim-Mitsuyama, S. Olmesartan prevents cardiovascular injury and hepatic steatosis in obesity and diabetes, accompanied by apoptosis signal regulating kinase-1 inhibition. Hypertension 2008, 52, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Budas, G.; Karnik, S.; Jonnson, T.; Shafizadeh, T.; Watkins, S.; Breckenridge, D.; Tumas, D. Reduction of liver steatosis and fibrosis with an Ask1 inhibitor in a murine model of nash is accompanied by improvements in cholesterol, bile acid and lipid metabolism. J. Hepatol. 2016, 64, S170. [Google Scholar] [CrossRef]
- Safety, Tolerability, and Efficacy of GS-4997 Alone or in Combination with Simtuzumab (SIM) in Adults with Nonalcoholic Steatohepatitis (NASH) and Fibrosis Stages F2–F3. 27 February 2017. Available online: https://clinicaltrials.gov/ct2/show/NCT02466516 (accessed on 16 June 2018).
- Younossi, Z.M.; Stepanova, M.; Lawitz, E.; Charlton, M.; Loomba, R.; Myers, R.P.; Subramanian, M.; McHutchinson, J.G.; Goodman, Z. Improvement of hepatic fibrosis and patient-reported outcomes in non-alcoholic steatohepatitis treated with selonsertib. Liver Int. 2018. [Google Scholar] [CrossRef] [PubMed]
- Safety and Efficacy of Selonsertib, GS-0976, GS-9674, and Combinations in Participants with Bridging Fibrosis or Compensated Cirrhosis Due to Nonalcoholic Steatohepatitis (NASH). 11 June 2018. Available online: https://clinicaltrials.gov/ct2/show/NCT03449446 (accessed on 13 June 2018).
- Lawitz, E.; Herring, R.; Younes, Z.H.; Gane, E.; Ruane, P.; Schall, R.A.; Jia, C.; Xu, R.; Mccolgan, B.; Djedjos, S.; et al. Proof of concept study of an apoptosis-signal regulating kinase (ASK1) inhibitor (selonsertib) in combination with an acetyl-CoA carboxylase inhibitor (GS-0976) or a farnesoid X receptor agonist (GS-9674) in NASH. J. Hepatol. 2018, 68, S57. [Google Scholar] [CrossRef]
- Gilead Sciences, Inc., Investors. Gilead Presents Data on Multiple Investigational Regimens for the Treatment of Patients with Nonalcoholic Steatohepatitis (NASH) and Advanced Fibrosis at The International Liver Congress™ 2018. 13 April 2018. Available online: http://markets.on.nytimes.com/research/stocks/news/press_release.asp?docTag=201804131015BIZWIRE_USPRX____BW5160&feedID=600&press_symbol=138551 (accessed on 16 June 2018).
- Harrison, S.; Noureddin, M.; Herring, R.; Ruane, P.; Mccolgan, B.; Kirby, B.; Nelson, C.; Schall, R.A.; Jia, C.; Subramanian, M.; et al. Preliminary efficacy and safety of acetyl-CoA carboxylase inhibitor GS-0976 in patients with compensated cirrhosis due to NASH. J. Hepatol. 2018, 68, S583. [Google Scholar] [CrossRef]
- Lawitz, E.J.; Poordad, F.; Coste, A.; Loo, N.; Djedjos, C.S.; McColgan, B.; Jia, C.; Myers, R.P.; Subramanian, G.M.; McHutchison, J.G.; et al. Acetyl-CoA carboxylase (ACC) inhibitor GS-0976 leads to suppression of hepatic de novo lipogenesis and significant improvements in MRI-PDFF, MRE, and markers of fibrosis after 12 weeks of therapy in patients with NASH. J. Hepatol. 2017, 66, S34. [Google Scholar] [CrossRef]
- Lawitz, E.J.; Coste, A.; Poordad, F.; Alkhouri, N.; Loo, N.; McColgan, B.J.; Tarrant, J.M.; Nguyen, T.; Han, L.; Chung, C.; et al. Acetyl-CoA Carboxylase Inhibitor GS-0976 for 12 Weeks Reduces Hepatic De Novo Lipogenesis and Steatosis in Patients with Nonalcoholic Steatohepatitis. Clin. Gastroenterol. Hepatol. 2018. [Google Scholar] [CrossRef] [PubMed]
- GS-0976 in Adults with Nonalcoholic Steatohepatitis. 4 August 2017. Available online: https://clinicaltrials.gov/ct2/show/NCT02856555 (accessed on 16 June 2018).
- Carotti, S.; Guarino, M.P.L.; Vespasiani-Gentilucci, U.; Morini, S. Starring role of toll-like receptor-4 activation in the gut-liver axis. World J. Gastrointest. Pathophysiol. 2015, 6, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Deihl, A.M.; Harrison, S.; Caldwell, S.; Rinella, M.; Paredes, A.; Moylan, C.; Guy, C.; Bashir, M.R.; Wang, Y.; Miller, L.; et al. A Randomized, Double-Blind, Placebo Controlled, Parallel-Group, Phase II Trial of JKB-121 for the Treatment of Nonalcoholic Steatohepatitis (NASH). 2018. Available online: http://www.natap.org/2018/EASL/EASL_50.htm (accessed on 16 June 2018).
- JKB-121 for the Treatment of Nonalcoholic Steatohepatitis. 30 January 2018. Available online: https://clinicaltrials.gov/ct2/show/NCT02442687 (accessed on 16 June 2018).
- Walker, M. TLR-4 Antagonist for NASH Flops in Phase IIa Trial. 16 April 2018. Available online: https://www.medpagetoday.com/meetingcoverage/easl/72362 (accessed on 13 June 2018).
- Younossi, Z.M.; Loomba, R.; Rinella, M.E.; Bugianesi, E.; Marchesini, G.; Neuschwander-Tetri, B.; Serfaty, L.; Negro, F.; Caldwell, S.H.; Ratziu, V.; et al. Current and Future Therapeutic Regimens for Non-alcoholic Fatty Liver Disease (NAFLD) and Non-alcoholic Steatohepatitis (NASH). Hepatology 2017. [Google Scholar] [CrossRef]
- Konerman, M.A.; Jones, J.C.; Harrison, S.A. Pharmacotherapy for NASH: Current and emerging. J. Hepatol. 2017, 68, 362–375. [Google Scholar] [CrossRef] [PubMed]
- Teschke, R.; Xuan, T.D. A Contributory Role of Shell Ginger (Alpinia zerumbet) for Human Longevity in Okinawa, Japan? Nutrients 2018, 10, 166. [Google Scholar] [CrossRef] [PubMed]
- Teschke, R.; Danan, G. Prospective Indian study of DILI with confirmed causality using the roussel uclaf causality assessment method (RUCAM): A report of excellence. Ann. Hepatol. 2017, 16, 324–325. [Google Scholar] [CrossRef] [PubMed]
- Teschke, R.; Schulze, J.; Eickhoff, A.; Danan, G. Drug induced liver injury: Can biomarkers assist RUCAM in causality assessment? Int. J. Mol. Sci. 2017, 18, 803. [Google Scholar] [CrossRef] [PubMed]
- Cholankeril, G.; Wong, R.J.; Hu, M.; Perumpail, R.B.; Yoo, E.R.; Puri, P.; Younossi, Z.; Harrison, S.; Ahmed, A. Liver transplantation for nonalcoholic steatohepatitis in the US: Temporal trends and outcomes. Dig. Dis. Sci. 2017, 62, 2915–2922. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Drug Therapy | Current Clinical Trial Name | Phase | Mechanism of Action | |
|---|---|---|---|---|
| 1 | Obeticholic Acid | REGENERATE; NCT02548351 [21] | 3 | FXR agonist |
| 2 | GS-9674 | NCT02854605 [23] | 2 | FXR agonist |
| 3 | Elafibranor | RESOLVE-IT, NCT02704403 [28] | 3 | Dual PPAR α/δ agonist |
| 4 | Cencriviroc | AURORA; NCT03028740 [36,37] | 3 | CCR2 and CCR5 dual antagonist |
| 5 | GR-MD-02 | NASH-CX [42,43] | 2b | Galectin-3 inhibitor |
| 6 | NGM282 | NCT02443116 [50] | 2 | Variant of FGF19 |
| 7 | MGL-3196 | NDT02912260 [53] | 2 | Selective thyroid hormone receptor-beta agonist |
| 8 | Selonsertib | STELLAR-3; NCT03053050 [8] and STELLAR-4; NCT03053063 [8] | 3 | Apoptosis signal-regulating kinase 1 inhibitor |
| 9 | Simtuzumab | NCT02466516 [62] and NCT01672879 [11] | 2, 2b | Monoclonal antibody against LOXL2 |
| 10 | Selonsertib + Simtuzumab | NCT02466516 [62] | 2 | |
| 11 | GS-0976 | NCT 02856555 [70] | 2 | Acetyl-coenzyme A carboxylase (ACC) inhibitor |
| 12 | Selonsertib + GS-9674 | ATLAS, NCT03449446 [64] | 2 | |
| 13 | Selonsertib + GS-0976 | ATLAS, NCT03449446 [64] | 2 | |
| 14 | JKB-121 | NCT02442687 [71] | 2a | TLR-4 antagonist |
| 15 | SGM-1019 | NCT | 2a | Inflammasome inhibitor |
| 16 | BMS-986036 | 2a | Pegylated fibroblast growth factor 21 (FGF21) analogue [76,77] | |
| 17 | Aramchol | 2b | Synthetic fatty acid/bile acid conjugate [76,77] | |
| 18 | Volixibet | 2a | Apical sodium dependent bile acid transporter inhibitor [76,77] | |
| 19 | LMB763 | 2a | FXR agonist [76,77] | |
| 20 | LJN452 | 2a | FXR agonist [76,77] | |
| 21 | Emricasan | 2b | Oral caspase inhibitor [76,77] | |
| 22 | Saroglitazar | 2a | PPAR α/δ agonist [76,77] | |
| 23 | IVA337 | 2a | Pan-PPAR agonist [76,77] | |
| 24 | IMM-124E-Hyperimmune bovine colostrum | 2a | Induction of regulatory T-cells [76,77] | |
| 25 | BI-1467335 | 2a | Amino-oxidase copper (AOC) containing-3 inhibitor [76,77] | |
| 26 | LIK066 | 2a | Sodium glucose cotransporter inhibitor (SGLT) [77] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dibba, P.; Li, A.A.; Perumpail, B.J.; John, N.; Sallam, S.; Shah, N.D.; Kwong, W.; Cholankeril, G.; Kim, D.; Ahmed, A. Emerging Therapeutic Targets and Experimental Drugs for the Treatment of NAFLD. Diseases 2018, 6, 83. https://doi.org/10.3390/diseases6030083
Dibba P, Li AA, Perumpail BJ, John N, Sallam S, Shah ND, Kwong W, Cholankeril G, Kim D, Ahmed A. Emerging Therapeutic Targets and Experimental Drugs for the Treatment of NAFLD. Diseases. 2018; 6(3):83. https://doi.org/10.3390/diseases6030083
Chicago/Turabian StyleDibba, Pratima, Andrew A. Li, Brandon J. Perumpail, Nimy John, Sandy Sallam, Neha D. Shah, Waiyee Kwong, George Cholankeril, Donghee Kim, and Aijaz Ahmed. 2018. "Emerging Therapeutic Targets and Experimental Drugs for the Treatment of NAFLD" Diseases 6, no. 3: 83. https://doi.org/10.3390/diseases6030083
APA StyleDibba, P., Li, A. A., Perumpail, B. J., John, N., Sallam, S., Shah, N. D., Kwong, W., Cholankeril, G., Kim, D., & Ahmed, A. (2018). Emerging Therapeutic Targets and Experimental Drugs for the Treatment of NAFLD. Diseases, 6(3), 83. https://doi.org/10.3390/diseases6030083