
Association between Protein Intake and Diabetes Complications Risk Following Incident Type 2 Diabetes: The EPIC-Potsdam Study

Abstract
:1. Introduction
2. Methods
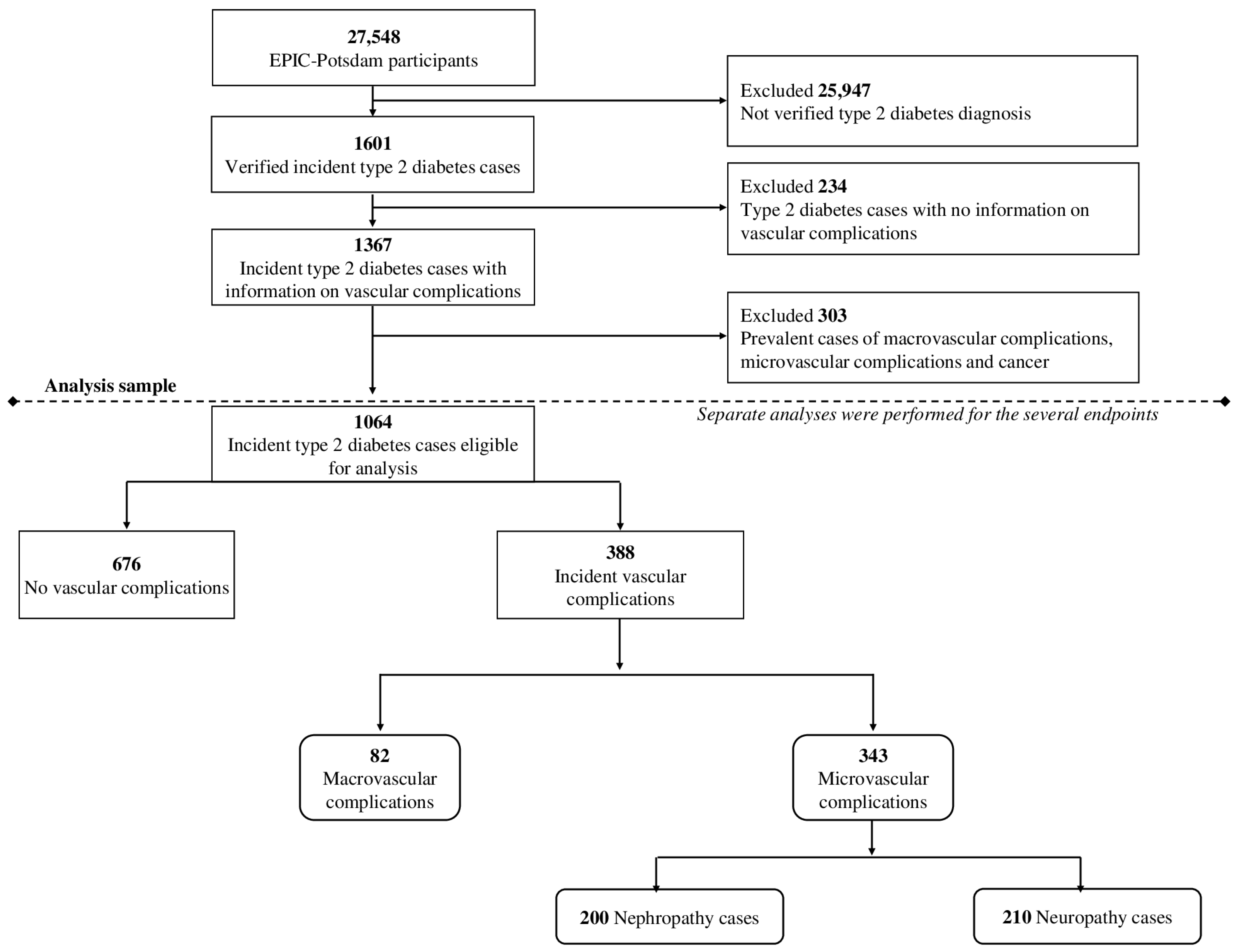
2.1. Study Population
2.2. Assessment of Protein Intake
2.3. Ascertainment of Type 2 Diabetes and Vascular Complications
2.4. Assessment of Covariates
2.5. Statistical Analyses
3. Results
3.1. Protein Intake Prior to Diagnosis and Diabetes-Related Complications
3.2. Change of Protein Intake from Pre to Post Diabetes Diagnosis and Risk of Complications
3.3. Protein Intake among Prevalent Diabetes Cases and Diabetes-Related Complications
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ye, J.; Yu, Q.; Mai, W.; Liang, P.; Liu, X.; Wang, Y. Dietary protein intake and subsequent risk of type 2 diabetes: A dose–response meta-analysis of prospective cohort studies. Acta Diabetol. 2019, 56, 851–870. [Google Scholar] [CrossRef]
- Kaptoge, S.; Seshasai, S.R.K.; Sun, L.; Walker, M.; Bolton, T.; Spackman, S.; Ataklte, F.; Willeit, P.; Bell, S.; Burgess, S.; et al. Life expectancy associated with different ages at diagnosis of type 2 diabetes in high-income countries: 23 million person-years of observation. Lancet Diabetes Endocrinol. 2023, 11, 731–742. [Google Scholar] [CrossRef] [PubMed]
- Nichols, G.A.; Glauber, H.S.; Brown, J.B. Type 2 diabetes: Incremental medical care costs during the 8 years preceding diagnosis. Diabetes Care 2000, 23, 1654–1659. [Google Scholar] [CrossRef] [PubMed]
- Tuomilehto, J.; Lindström, J.; Eriksson, J.G.; Valle, T.T.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M.; et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. NEJM 2001, 344, 1343–1350. [Google Scholar] [CrossRef]
- Pan, A.; Sun, Q.; Bernstein, A.M.; Schulze, M.B.; Manson, J.E.; Willett, W.C.; Hu, F.B. Red meat consumption and risk of type 2 diabetes: 3 cohorts of US adults and an updated meta-analysis. Am. J. Clin. Nutr. 2011, 94, 1088–1096. [Google Scholar] [CrossRef] [PubMed]
- InterAct Consortium. Association between dietary meat consumption and incident type 2 diabetes: The EPIC-InterAct study. Diabetologia 2013, 56, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Afshin, A.; Micha, R.; Khatibzadeh, S.; Mozaffarian, D. Consumption of nuts and legumes and risk of incident ischemic heart disease, stroke, and diabetes: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Nanri, A.; Mizoue, T.; Takahashi, Y.; Kirii, K.; Inoue, M.; Noda, M.; Tsugane, S. Soy product and isoflavone intakes are associated with a lower risk of type 2 diabetes in overweight Japanese women. J. Nutr. 2010, 140, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Schulze, M.B.; Schulz, M.; Heidemann, C.; Schienkiewitz, A.; Hoffmann, K.; Boeing, H. Carbohydrate intake and incidence of type 2 diabetes in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Potsdam Study. Br. J. Nutr. 2008, 99, 1107–1116. [Google Scholar] [CrossRef]
- Zhao, L.G.; Zhang, Q.L.; Liu, X.L.; Wu, H.; Zheng, J.L.; Xiang, Y.B. Dietary protein intake and risk of type 2 diabetes: A dose–response meta-analysis of prospective studies. Eur. J. Nutr. 2019, 58, 1351–1367. [Google Scholar] [CrossRef]
- Schulze, M.B.; Haardt, J.; Amini, A.M.; Kalotai, N.; Lehmann, A.; Schmidt, A.; Buyken, A.E.; Egert, S.; Ellinger, S.; Kroke, A.; et al. Protein intake and type 2 diabetes mellitus: An umbrella review of systematic reviews for the evidence-based guideline for protein intake of the German Nutrition Society. Eur. J. Nutr. 2023, 63, 33–50. [Google Scholar] [CrossRef]
- Fouque, D.; Laville, M.; Boissel, J.P. Low protein diets for chronic kidney disease in non diabetic adults. Cochrane Database Syst. Rev. 2006, 2, CD001892. [Google Scholar]
- Oosterwijk, M.M.; Soedamah-Muthu, S.S.; Geleijnse, J.M.; Bakker, S.J.; Navis, G.; Binnenmars, S.H.; Gant, C.M.; Laverman, G.D. High dietary intake of vegetable protein is associated with lower prevalence of renal function impairment: Results of the Dutch DIALECT-1 cohort. Kidney Int. Rep. 2019, 4, 710–719. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, R.; Lipworth, L.; Cavanaugh, K.L.; Young, B.A.; Tucker, K.L.; Carithers, T.C.; Kabagambe, E.K.; Ikizler, T.A. Protein intake and long-term change in glomerular filtration rate in the Jackson Heart Study. J. Ren. Nutr. 2018, 28, 245–250. [Google Scholar] [CrossRef]
- Lagiou, P.; Sandin, S.; Lof, M.; Trichopoulos, D.; Adami, H.O.; Weiderpass, E. Low carbohydrate-high protein diet and incidence of cardiovascular diseases in Swedish women: Prospective cohort study. BMJ 2012, 344, e4026. [Google Scholar] [CrossRef] [PubMed]
- Halton, T.L.; Willett, W.C.; Liu, S.; Manson, J.E.; Albert, C.M.; Rexrode, K.; Hu, F.B. Low-carbohydrate-diet score and the risk of coronary heart disease in women. NEJM 2006, 355, 1991–2002. [Google Scholar] [CrossRef] [PubMed]
- Feinman, R.D.; Pogozelski, W.K.; Astrup, A.; Bernstein, R.K.; Fine, E.J.; Westman, E.C.; Accurso, A.; Frassetto, L.; Gower, B.A.; McFarlane, S.I.; et al. Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base. Nutrition 2015, 31, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Nuttall, F.Q.; Gannon, M.C. Metabolic response of people with type 2 diabetes to a high protein diet. Nutr. Metab. 2004, 1, 6. [Google Scholar] [CrossRef] [PubMed]
- Ameer, F.; Scandiuzzi, L.; Hasnain, S.; Kalbacher, H.; Zaidi, N. De novo lipogenesis in health and disease. Metabolism 2014, 63, 895–902. [Google Scholar] [CrossRef]
- Oosterwijk, M.M.; Groothof, D.; Navis, G.; Bakker, S.J.; Laverman, G.D. High-normal protein intake is not associated with faster renal function deterioration in patients with type 2 diabetes: A prospective analysis in the DIALECT cohort. Diabetes Care 2022, 45, 35–41. [Google Scholar] [CrossRef]
- Campmans-Kuijpers, M.J.; Sluijs, I.; Nöthlings, U.; Freisling, H.; Overvad, K.; Weiderpass, E.; Fagherazzi, G.; Kühn, T.; Katzke, V.A.; Mattiello, A.; et al. Isocaloric substitution of carbohydrates with protein: The association with weight change and mortality among patients with type 2 diabetes. Cardiovasc. Diabetol. 2015, 14, 39. [Google Scholar] [CrossRef] [PubMed]
- Von Bibra, H.; Wulf, G.; Sutton, M.S.J.; Pfützner, A.; Schuster, T.; Heilmeyer, P. Low-carbohydrate/high-protein diet improves diastolic cardiac function and the metabolic syndrome in overweight-obese patients with type 2 diabetes. IJC Metab. Endocr. 2014, 2, 11–18. [Google Scholar] [CrossRef]
- Lin, C.C.; Liu, C.S.; Li, C.I.; Lin, C.H.; Lin, W.Y.; Wang, M.C.; Yang, S.Y.; Li, T.C. Dietary macronutrient intakes and mortality among patients with type 2 diabetes. Nutrients 2020, 12, 1665. [Google Scholar] [CrossRef]
- Böing, H.; Wahrendorf, J.; Becker, N. EPIC-Germany–a source for studies into diet and risk of chronic diseases. Ann. Nutr. Metab. 1999, 43, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, M.M.; Bussas, U.; Boeing, H. Follow-up procedures in EPIC-Germany–data quality aspects. Ann. Nutr. Metab. 1999, 43, 225–234. [Google Scholar] [CrossRef]
- Lotta, L.A.; Gulati, P.; Day, F.R.; Payne, F.; Ongen, H.; Van De Bunt, M.; Gaulton, K.J.; Eicher, J.D.; Sharp, S.J.; Luan, J.; et al. Integrative genomic analysis implicates limited peripheral adipose storage capacity in the pathogenesis of human insulin resistance. Nat. Genet. 2017, 49, 17–26. [Google Scholar] [CrossRef]
- Kroke, A.; Klipstein-Grobusch, K.; Voss, S.; Möseneder, J.; Thielecke, F.; Noack, R.; Boeing, H. Validation of a self-administered food-frequency questionnaire administered in the European Prospective Investigation into Cancer and Nutrition (EPIC) study: Comparison of energy, protein, and macronutrient intakes estimated with the doubly labeled water, urinary nitrogen, and repeated 24-h dietary recall methods. Am. J. Clin. Nutr. 1999, 70, 439–447. [Google Scholar] [PubMed]
- Dehne, L.I.; Klemm, C.; Henseler, G.; Hermann-Kunz, E. The German Food Code and Nutrient Data Base (BLS II.2). Eur. J. Epidemiol. 1999, 15, 355–359. [Google Scholar] [CrossRef]
- Kroke, A.; Bergmann, M.M.; Lotze, G.; Jeckel, A.; Klipstein-Grobusch, K.; Boeing, H. Measures of quality control in the German component of the EPIC study. European Prospective Investigation into Cancer and Nutrition. Ann. Nutr. Metab. 1999, 43, 216–224. [Google Scholar] [CrossRef]
- World Health Organization. A Healthy Lifestyle—WHO Recommendations. 2010. Available online: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations (accessed on 11 March 2024).
- Adeva-Andany, M.M.; Fernández-Fernández, C.; Carneiro-Freire, N.; Vila-Altesor, M.; Ameneiros-Rodríguez, E. The differential effect of animal versus vegetable dietary protein on the clinical manifestations of diabetic kidney disease in humans. Clin. Nutr. ESPEN 2022, 48, 21–35. [Google Scholar] [CrossRef]
- Kurella, M.; Lo, J.C.; Chertow, G.M. Metabolic syndrome and the risk for chronic kidney disease among nondiabetic adults. J. Am. Soc. Nephrol. 2005, 16, 2134–2140. [Google Scholar] [CrossRef]
- Mitch, W.E. Diets for Patients with Chronic Kidney Disease, Still Worth Prescribing. J. Am. Soc. Nephrol. 2004, 15, 234–237. [Google Scholar] [CrossRef]
- Johnson, D.W. Dietary protein restriction as a treatment for slowing chronic kidney disease progression: The case against. Nephrology 2006, 11, 58–62. [Google Scholar] [CrossRef]
- Mandayam, S.; Mitch, W.E. Dietary protein restriction benefits patients with chronic kidney disease. Nephrology 2006, 11, 53–57. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI clinical practice guideline for nutrition in CKD: 2020 update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Sohouli, M.H.; Mirmiran, P.; Seraj, S.S.; Kutbi, E.; Alkahmous, H.A.M.; Almuqayyid, F.; Arafah, O.A.; Barakeh, A.R.R.; Abu-Zaid, A. Impact of low-protein diet on cardiovascular risk factors and kidney function in diabetic nephropathy: A systematic review and meta-analysis of randomized-controlled trials. Diabetes Res. Clin. Pract. 2022, 191, 110068. [Google Scholar] [CrossRef]
- Beeharry, D.; Joseph, F.; Ewins, D.; Nair, S. Dietary management of diabetic chronic kidney disease. Curr. Nutr. Rep. 2014, 3, 333–339. [Google Scholar] [CrossRef]
- Pan, Y.; Guo, L.L.; Jin, H.M. Low-protein diet for diabetic nephropathy: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2008, 88, 660–666. [Google Scholar] [CrossRef]
- Nezu, U.; Kamiyama, H.; Kondo, Y.; Sakuma, M.; Morimoto, T.; Ueda, S. Effect of low-protein diet on kidney function in diabetic nephropathy: Meta-analysis of randomised controlled trials. BMJ Open 2013, 3, e002934. [Google Scholar] [CrossRef]
- Zhu, H.G.; Jiang, Z.S.; Gong, P.Y.; Zhang, D.M.; Zou, Z.W.; Ma, H.M.; Guo, Z.G.; Zhao, J.Y.; Dong, J.J. Efficacy of low-protein diet for diabetic nephropathy: A systematic review of randomized controlled trials. Lipids Health Dis. 2018, 17, 141. [Google Scholar] [CrossRef]
- Landgraf, R.; Kellerer, M.; Aberle, J.; Fach, E.; Gallwitz, B.; Hamann, A.; Joost, H.; Klein, H.; Müller-Wieland, D.; Nauck, M.A.; et al. Therapie des Typ-2-Diabetes. Diabetologe 2019, 15, 146–167. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Total (n = 1064) | Men (n = 577) | Women (n = 487) |
|---|---|---|---|
| Age at diabetes diagnosis (years) (median (Q1, Q3)) | 60 (53–65) | 60 (53–65) | 61 (54–66) |
| Education (n(%)) | |||
| No school degree or primary school | 481 (45.2) | 223 (38.7) | 258 (53.0) |
| Technical or professional school | 267 (25.1) | 117 (20.3) | 150 (30.8) |
| University degree | 316 (29.7) | 237 (41.0) | 79 (16.2) |
| Pre-diagnosis lifestyle | |||
| Physical activity (h/week) (median (Q1, Q3)) | 1 (0–3.3) | 1 (0–3) | 1 (0–3.5) |
| Smoking status (n (%)) | |||
| Never-smoker | 421 (39.6) | 134 (23.2) | 287 (59.1) |
| Former smoker | 464 (43.6) | 331 (57.3) | 133 (27.4) |
| Current smoker | 179 (16.8) | 112 (19.5) | 67 (13.5) |
| Smoking duration (years) (median (Q1, Q3)) | 10 (0, 28) | 19 (3, 31) | 0 (0–19) |
| Body mass index (kg/m2) (median (Q1, Q3)) | 29.9 (27.4–33.2) | 29.7 (27.5–32.5) | 30.2 (27.2–34.0) |
| Medical information | |||
| Diabetes duration (years) (median (Q1, Q3)) | 12.1 (9.4–14.9) | 12.5 (9.7, 15.1) | 11.5 (9–14.6) |
| Family history of myocardial infarction (n (%)) | 183 (17.0) | 84 (14.5) | 99 (20.3) |
| Family history of stroke (n (%)) | 219 (21.0) | 99 (17.1) | 120 (24.7) |
| Hypertension (n (%)) | 853 (80.0) | 466–467 (80.8) | 386 (79.3) |
| Dyslipidaemia (n (%)) | 779 (73.2) | 422–423 (73.2) | 356 (73.1) |
| Dietary intake (median (Q1, Q3)) | |||
| Energy intake (kJ) | 8767 (7070–10,661) | 9852 (8021–11,574) | 7544 (6371–9226) |
| Protein intake (g/day) | 75.7 (60.6–93.4) | 85.8 (69.3–101.5) | 66.1 (53.6–79.4) |
| Animal protein intake (g/day) | 49.0 (38.4–62.6) | 56.3 (43.0–69.5) | 43.3 (34.3–53.4) |
| Plant protein intake (g/day) | 25.2 (20.3–31.4) | 28.6 (23.5–34.5) | 21.8 (18.5–26.8) |
| Carbohydrate intake (g/day) | 222.5 (179.8–274.6) | 241.6 (198.4–291.0) | 201.8 (166.0–247.5) |
| Fat intake (g/day) | 81.7 (65.1–105.6) | 92.7 (71.8–116.8) | 72.4 (60.1–90.9) |
| Alcohol intake (g/day) | 9.1 (2.8–21.7) | 16.1 (7.5–33.3) | 4.2 (1.5–9.4) |
| Fibre intake (g/d) | 21.1 (17.3–26.3) | 22.3 (17.9–27.3) | 20.0 (16.8–24.0) |
| PUFA:SFA ratio | 0.5 (0.4–0.6) | 0.5 (0.4–0.6) | 0.5 (0.4–0.5) |
| Mg intake (mg/d) | 0.3 (0.2–0.4) | 0.4 (0.3–0.4) | 0.3 (0.2–0.3) |
| Cholesterol intake (mg/d) | 0.3 (0.2–0.4) | 0.3 (0.2–0.4) | 0.3 (0.2–0.3) |
| Vitamin E intake (mg/d) | 11.9 (9.5–14.8) | 12.5 (9.8–15.6) | 11.3 (9.2–14.0) |
| Complications | Total | |||
|---|---|---|---|---|
| Events (n) | Total Protein | Animal Protein | Plant Protein | |
| HR (95% CI) | HR (95% CI) | HR (95% CI) | ||
| Total complications | 388 | |||
| Model 1 | 1.01 (0.78, 1.32) | 1.01 (0.78, 1.31) | 1.20 (0.53, 2.70) | |
| Model 2 | 0.89 (0.68, 1.16) | 0.89 (0.68, 1.16) | 1.02 (0.43, 2.39) | |
| Model 3 | 0.83 (0.60, 1.14) | 0.82 (0.60, 1.13) | 1.62 (0.61, 4.27) | |
| Macrovascular complications | 82 | |||
| Model 1 | 0.76 (0.42, 1.38) | 0.76 (0.42, 1.38) | 3.11 (0.40, 16.98) | |
| Model 2 | 0.81 (0.45, 1.47) | 0.82 (0.44, 1.49) | 3.36 (0.53, 21.22) | |
| Model 3 | 0.81 (0.39, 1.68) | 0.77 (0.37, 1.61) | 3.25 (0.52, 20.01) | |
| Microvascular complications | 343 | |||
| Model 1 | 1.09 (0.82, 1.44) | 1.09 (0.82, 1.44) | 0.90 (0.39, 2.07) | |
| Model 2 | 0.90 (0.67, 1.21) | 0.90 (0.67, 1.22) | 0.74 (0.30, 1.79) | |
| Model 3 | 0.83 (0.58, 1.19) | 0.83 (0.58, 1.19) | 1.19 (0.41, 3.46) | |
| Nephropathy | 200 | |||
| Model 1 | 1.06 (0.72, 1.54) | 1.06 (0.72, 1.54) | 0.91 (0.34, 2.41) | |
| Model 2 | 0.85 (0.57, 1.27) | 0.85 (0.57, 1.27) | 0.84 (0.31, 2.33) | |
| Model 3 | 1.03 (0.64, 1.64) | 0.87 (0.43, 1.76) | 1.42 (0.36, 5.55) | |
| Neuropathy | 210 | |||
| Model 1 | 1.10 (0.77, 1.57) | 1.10 (0.77, 1.57) | 0.80 (0.26, 2.44) | |
| Model 2 | 0.93 (0.64, 1.36) | 0.94 (0.65, 1.36) | 0.64 (0.20, 2.02) | |
| Model 3 | 0.76 (0.49, 1.18) | 0.77 (0.50, 1.19) | 1.15 (0.27, 4.92) | |
| Complications | Total | Low Protein Intake | High Protein Intake | |||
|---|---|---|---|---|---|---|
| Events (n) | HR (95% CI) | Events (n) | HR (95% CI) | Events (n) | HR (95% CI) | |
| Total complications | 267 | 126 | 141 | |||
| Model 1 | 1.00 (0.95, 1.07) | 0.97 (0.88, 1.07) | 1.06 (0.98, 1.16) | |||
| Model 2 | 1.02 (0.94, 1.10) | 0.93 (0.82, 1.04) | 1.05 (0.92, 1.21) | |||
| Model 3 | 0.98 (0.89, 1.08) | 1.01 (0.82, 1.24) | 0.95 (0.80, 1.13) | |||
| Microvascular complications | 241 | 116 | 125 | |||
| Model 1 | 1.03 (0.97, 1.10) | 1.02 (0.92, 1.12) | 1.08 (0.98, 1.18) | |||
| Model 2 | 1.06 (0.98, 1.16) | 0.99 (0.87, 1.13) | 1.12 (0.96, 1.30) | |||
| Model 3 | 1.02 (0.92, 1.14) | 1.01 (0.81, 1.25) | 1.03 (0.86, 1.25) | |||
| Nephropathy | 148 | 69 | 79 | |||
| Model 1 | 1.01 (0.94, 1.09) | 0.97 (0.86, 1.09) | 1.13 (1.02, 1.26) | |||
| Model 2 | 1.03 (0.82, 1.14) | 0.80 (0.61, 1.05) | 1.18 (0.96, 1.44) | |||
| Model 3 | 0.93 (0.81, 1.06) | 0.75 (0.36, 1.54) | 0.92 (0.69, 1.23) | |||
| Neuropathy | 148 | 72 | 76 | |||
| Model 1 | 1.06 (0.97, 1.16) | 1.10 (0.94, 1.29) | 1.06 (0.95, 1.19) | |||
| Model 2 | 1.01 (0.90, 1.14) | 0.98 (0.74, 1.29) | 1.04 (0.82, 1.33) | |||
| Model 3 | 0.99 (0.83, 1.17) | 1.03 (0.66, 1.60) | 0.91 (0.54, 1.53) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inan-Eroglu, E.; Kuxhaus, O.; Jannasch, F.; Nickel, D.V.; Schulze, M.B. Association between Protein Intake and Diabetes Complications Risk Following Incident Type 2 Diabetes: The EPIC-Potsdam Study. Metabolites 2024, 14, 172. https://doi.org/10.3390/metabo14030172
Inan-Eroglu E, Kuxhaus O, Jannasch F, Nickel DV, Schulze MB. Association between Protein Intake and Diabetes Complications Risk Following Incident Type 2 Diabetes: The EPIC-Potsdam Study. Metabolites. 2024; 14(3):172. https://doi.org/10.3390/metabo14030172
Chicago/Turabian StyleInan-Eroglu, Elif, Olga Kuxhaus, Franziska Jannasch, Daniela V. Nickel, and Matthias B. Schulze. 2024. "Association between Protein Intake and Diabetes Complications Risk Following Incident Type 2 Diabetes: The EPIC-Potsdam Study" Metabolites 14, no. 3: 172. https://doi.org/10.3390/metabo14030172