
Is Antimicrobial Photodynamic Therapy Effective as an Adjunct to Scaling and Root Planing in Patients with Chronic Periodontitis? A Systematic Review



Abstract
:1. Introduction
2. Methodology
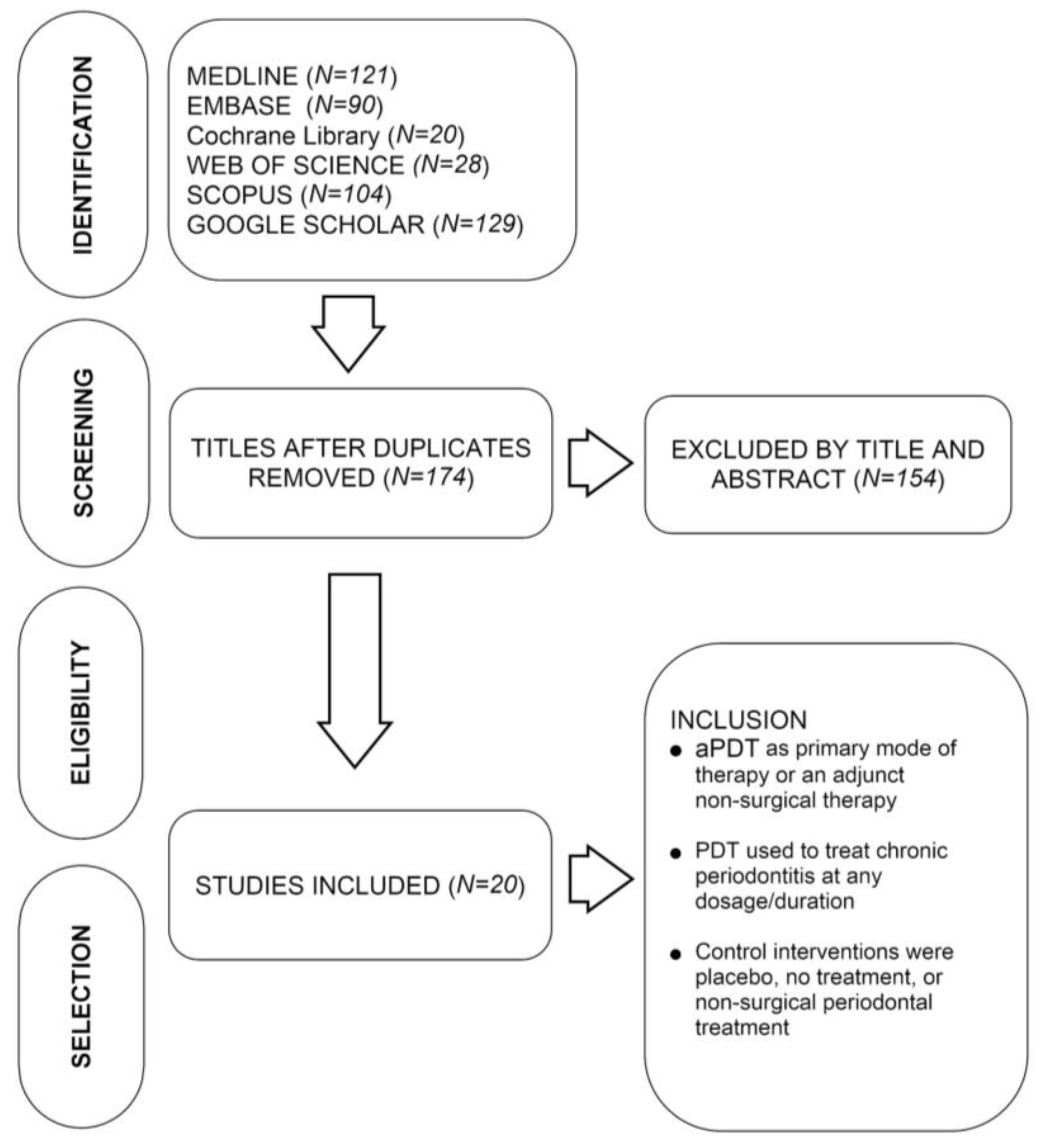
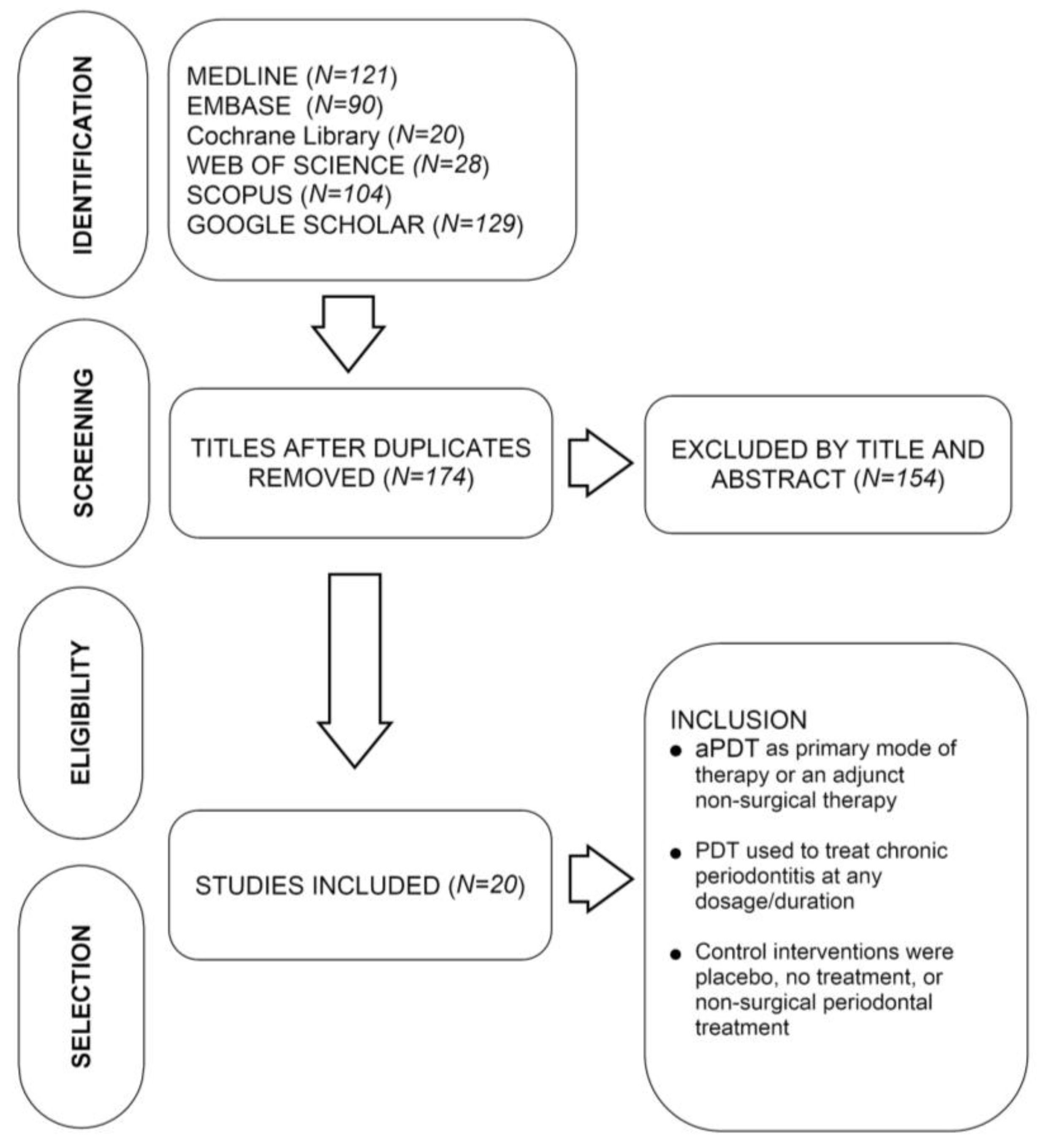
2.1. Search Strategy
2.2. Eligibility and Information Sources
2.3. Study Selection and Data Collection
3. Results
3.1. Study Characteristics
3.2. Study Design
3.3. Sample Size and Calculation
3.4. Blinding
3.5. Smokers
3.6. Photosensitizing Agents and Wavelengths Used in aPDT
3.7. Frequency of aPDT Application
3.8. Effect of aPDT on Clinical Parameters
3.9. Antimicrobial Effect of aPDT in Chronic Periodontitis
3.10. Effect of Immunological Parameters Following aPDT
3.11. Patient-Based Outcome Measures Reported in the Studies
4. Conclusions
Author Contributions
Conflicts of Interest
References
- Adriaens, P.A.; Adriaens, L.M. Effects of nonsurgical periodontal therapy on hard and soft tissues. Periodontology 2000 2004, 36, 121–145. [Google Scholar] [CrossRef] [PubMed]
- Umeda, M.; Takeuchi, Y.; Noguchi, K.; Huang, Y.; Koshy, G.; Ishikawa, I. Effects of nonsurgical periodontal therapy on the microbiota. Periodontology 2000 2004, 36, 98–120. [Google Scholar] [CrossRef] [PubMed]
- Hanes, P.J.; Purvis, J.P. Local anti-infective therapy: Pharmacological agents. A systematic review. Ann. Periodontol. 2003, 8, 79–98. [Google Scholar] [CrossRef] [PubMed]
- Assem, N.Z.; Alves, M.L.F.; Lopes, A.B.; Gualberto, E.C.J.; Garcia, V.G.; Theodoro, L.H. Antibiotic therapy as an adjunct to scaling and root planing in smokers: A systematic review and meta-analysis. Braz. Oral Res. 2017, 31, e67. [Google Scholar] [CrossRef] [PubMed]
- Dobson, J.; Wilson, M. Sensitization of oral bacteria in biofilms to killing by light from a low-power laser. Arch. Oral Biol. 1992, 37, 883–887. [Google Scholar] [CrossRef]
- Komerik, N.; Nakanishi, H.; MacRobert, A.J.; Henderson, B.; Speight, P.; Wilson, M. In vivo killing of porphyromonas gingivalis by toluidine blue-mediated photosensitization in an animal model. Antimicrob. Agents Chemother. 2003, 47, 932–940. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.A.; Pearson, G.J.; Colles, M.J.; Wilson, M. The photo-activated antibacterial action of toluidine blue o in a collagen matrix and in carious dentine. Caries Res. 2004, 38, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.A.; Pearson, G.J.; Colles, M.J.; Wilson, M. The effect of variable energy input from a novel light source on the photoactivated bactericidal action of toluidine blue o on streptococcus mutans. Caries Res. 2003, 37, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.; Burns, T.; Pratten, J.; Pearson, G.J. Bacteria in supragingival plaque samples can be killed by low-power laser light in the presence of a photosensitizer. J. Appl. Bacteriol. 1995, 78, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Azarpazhooh, A.; Shah, P.S.; Tenenbaum, H.C.; Goldberg, M.B. The effect of photodynamic therapy for periodontitis: A systematic review and meta-analysis. J. Periodontol. 2010, 81, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Braun, A.; Dehn, C.; Krause, F.; Jepsen, S. Short-term clinical effects of adjunctive antimicrobial photodynamic therapy in periodontal treatment: A randomized clinical trial. J. Clin. Periodontol. 2008, 35, 877–884. [Google Scholar] [CrossRef] [PubMed]
- Christodoulides, N.; Nikolidakis, D.; Chondros, P.; Becker, J.; Schwarz, F.; Rossler, R.; Sculean, A. Photodynamic therapy as an adjunct to non-surgical periodontal treatment: A randomized, controlled clinical trial. J. Periodontol. 2008, 79, 1638–1644. [Google Scholar] [CrossRef] [PubMed]
- Chondros, P.; Nikolidakis, D.; Christodoulides, N.; Rössler, R.; Gutknecht, N.; Sculean, A. Photodynamic therapy as adjunct to non-surgical periodontal treatment in patients on periodontal maintenance: A randomized controlled clinical trial. Lasers Med. Sci. 2009, 24, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Lulic, M.; Leiggener Gorog, I.; Salvi, G.E.; Ramseier, C.A.; Mattheos, N.; Lang, N.P. One-year outcomes of repeated adjunctive photodynamic therapy during periodontal maintenance: A proof-of-principle randomized-controlled clinical trial. J. Clin. Periodontol. 2009, 36, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Atieh, M.A. Photodynamic therapy as an adjunctive treatment for chronic periodontitis: A meta-analysis. Lasers Med. Sci. 2010, 25, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Sgolastra, F.; Petrucci, A.; Gatto, R.; Marzo, G.; Monaco, A. Photodynamic therapy in the treatment of chronic periodontitis: A systematic review and meta-analysis. Lasers Med. Sci. 2013, 28, 669–682. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.A.; Forrest, J.L. Enhancing your practice through evidence-based decision making: Pico, learning how to ask good questions. J. Evid. Based Dent. Pract. 2001, 1, 136–141. [Google Scholar] [CrossRef]
- Balata, M.L.; Andrade, L.P.; Santos, D.B.; Cavalcanti, A.N.; Tunes Uda, R.; Ribeiro Edel, P.; Bittencourt, S. Photodynamic therapy associated with full-mouth ultrasonic debridement in the treatment of severe chronic periodontitis: A randomized-controlled clinical trial. J. Appl. Oral Sci. 2013, 21, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Luchesi, V.H.; Pimentel, S.P.; Kolbe, M.F.; Ribeiro, F.V.; Casarin, R.C.; Nociti, F.H., Jr.; Sallum, E.A.; Casati, M.Z. Photodynamic therapy in the treatment of class ii furcation: A randomized controlled clinical trial. J. Clin. Periodontol. 2013, 40, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Dilsiz, A.; Canakci, V.; Aydin, T. Clinical effects of potassium-titanyl-phosphate laser and photodynamic therapy on outcomes of treatment of chronic periodontitis: A randomized controlled clinical trial. J. Periodontol. 2013, 84, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Berakdar, M.; Callaway, A.; Eddin, M.F.; Ross, A.; Willershausen, B. Comparison between scaling-root-planing (srp) and srp/photodynamic therapy: Six-month study. Head Face Med. 2012, 8, 12. [Google Scholar] [CrossRef] [PubMed]
- Lui, J.; Corbet, E.F.; Jin, L. Combined photodynamic and low-level laser therapies as an adjunct to nonsurgical treatment of chronic periodontitis. J. Periodontal. Res. 2011, 46, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Betsy, J.; Prasanth, C.S.; Baiju, K.V.; Prasanthila, J.; Subhash, N. Efficacy of antimicrobial photodynamic therapy in the management of chronic periodontitis: A randomized controlled clinical trial. J. Clin. Periodontol. 2014, 41, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Bassir, S.H.; Moslemi, N.; Jamali, R.; Mashmouly, S.; Fekrazad, R.; Chiniforush, N.; Shamshiri, A.R.; Nowzari, H. Photoactivated disinfection using light-emitting diode as an adjunct in the management of chronic periodontitis: A pilot double-blind split-mouth randomized clinical trial. J. Clin. Periodontol. 2013, 40, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Theodoro, L.H.; Silva, S.P.; Pires, J.R.; Soares, G.H.; Pontes, A.E.; Zuza, E.P.; Spolidorio, D.M.; de Toledo, B.E.; Garcia, V.G. Clinical and microbiological effects of photodynamic therapy associated with nonsurgical periodontal treatment. A 6-month follow-up. Lasers Med. Sci. 2012, 27, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Kolbe, M.F.; Ribeiro, F.V.; Luchesi, V.H.; Casarin, R.C.; Sallum, E.A.; Nociti, F.H., Jr.; Ambrosano, G.M.; Cirano, F.R.; Pimentel, S.P.; Casati, M.Z. Photodynamic therapy during supportive periodontal care: Clinical, microbiologic, immunoinflammatory, and patient-centered performance in a split-mouth randomized clinical trial. J. Periodontol. 2014, 85, e277–e286. [Google Scholar] [CrossRef] [PubMed]
- Campanile, V.S.M.; Giannopoulou, C.; Campanile, G.; Cancela, J.A.; Mombelli, A. Single or repeated antimicrobial photodynamic therapy as adjunct to ultrasonic debridement in residual periodontal pockets: Clinical, microbiological, and local biological effects. Lasers Med. Sci. 2013, 30, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Giannopoulou, C.; Cappuyns, I.; Cancela, J.; Cionca, N.; Mombelli, A. Effect of photodynamic therapy, diode laser, and deep scaling on cytokine and acute-phase protein levels in gingival crevicular fluid of residual periodontal pockets. J. Periodontol. 2012, 83, 1018–1027. [Google Scholar] [CrossRef] [PubMed]
- Cappuyns, I.; Cionca, N.; Wick, P.; Giannopoulou, C.; Mombelli, A. Treatment of residual pockets with photodynamic therapy, diode laser, or deep scaling. A randomized, split-mouth controlled clinical trial. Lasers Med. Sci. 2012, 27, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Ruhling, A.; Fanghanel, J.; Houshmand, M.; Kuhr, A.; Meisel, P.; Schwahn, C.; Kocher, T. Photodynamic therapy of persistent pockets in maintenance patients-a clinical study. Clin. Oral Investig. 2010, 14, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Sigusch, B.W.; Engelbrecht, M.; Volpel, A.; Holletschke, A.; Pfister, W.; Schutze, J. Full-mouth antimicrobial photodynamic therapy in fusobacterium nucleatum-infected periodontitis patients. J. Periodontol. 2010, 81, 975–981. [Google Scholar] [CrossRef] [PubMed]
- Alwaeli, H.A.; Al-Khateeb, S.N.; Al-Sadi, A. Long-term clinical effect of adjunctive antimicrobial photodynamic therapy in periodontal treatment: A randomized clinical trial. Lasers Med. Sci. 2015, 30, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, V.F.; Andrade, P.V.; Rodrigues, M.F.; Hirata, M.H.; Hirata, R.D.; Pannuti, C.M.; De Micheli, G.; Conde, M.C. Antimicrobial photodynamic effect to treat residual pockets in periodontal patients: A randomized controlled clinical trial. J. Clin. Periodontol. 2015, 42, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Campos, G.N.; Pimentel, S.P.; Ribeiro, F.V.; Casarin, R.C.; Cirano, F.R.; Saraceni, C.H.; Casati, M.Z. The adjunctive effect of photodynamic therapy for residual pockets in single-rooted teeth: A randomized controlled clinical trial. Lasers Med. Sci. 2013, 28, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Smail-Faugeron, V.; Fron-Chabouis, H.; Courson, F.; Durieux, P. Comparison of intervention effects in split-mouth and parallel-arm randomized controlled trials: A meta-epidemiological study. BMC Med. Res. Methodol. 2014, 14, 64. [Google Scholar] [CrossRef] [PubMed]
- Donner, A.; Eliasziw, M. Application of matched pair procedures to site-specific data in periodontal research. J. Clin. Periodontol. 1991, 18, 755–759. [Google Scholar] [CrossRef] [PubMed]
- Gomer, C.J. Preclinical examination of first and second generation photosensitizers used in photodynamic therapy. Photochem. Photobiol. 1991, 54, 1093–1107. [Google Scholar] [CrossRef] [PubMed]
- Olsen, C.E.; Weyergang, A.; Edwards, V.T.; Berg, K.; Brech, A.; Weisheit, S.; Hogset, A.; Selbo, P.K. Development of resistance to photodynamic therapy (pdt) in human breast cancer cells is photosensitizer-dependent: Possible mechanisms and approaches for overcoming pdt-resistance. Biochem. Pharmacol. 2017, 144, 63–77. [Google Scholar] [CrossRef] [PubMed]
- Giannelli, M.; Formigli, L.; Lorenzini, L.; Bani, D. Combined photoablative and photodynamic diode laser therapy as an adjunct to non-surgical periodontal treatment: A randomized split-mouth clinical trial. J. Clin. Periodontol. 2012, 39, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.; Lai, C.H. Bactericidal effects of different laser wavelengths on periodontopathic germs in photodynamic therapy. Lasers Med. Sci. 2003, 18, 51–55. [Google Scholar] [CrossRef] [PubMed]
- de Paula Eduardo, C.; de Freitas, P.M.; Esteves-Oliveira, M.; Aranha, A.C.; Ramalho, K.M.; Simoes, A.; Bello-Silva, M.S.; Tuner, J. Laser phototherapy in the treatment of periodontal disease. A review. Lasers Med. Sci. 2010, 25, 781–792. [Google Scholar] [CrossRef] [PubMed]
- Soukos, N.S.; Goodson, J.M. Photodynamic therapy in the control of oral biofilms. Periodontology 2000 2011, 55, 143–166. [Google Scholar] [CrossRef] [PubMed]
- Bunaes, D.F.; Lie, S.A.; Enersen, M.; Aastrom, A.N.; Mustafa, K.; Leknes, K.N. Site-specific treatment outcome in smokers following non-surgical and surgical periodontal therapy. J. Clin. Periodontol. 2015, 42, 933–942. [Google Scholar] [CrossRef] [PubMed]
- Garcia Canas, P.; Khouly, I.; Sanz, J.; Loomer, P.M. Effectiveness of systemic antimicrobial therapy in combination with scaling and root planing in the treatment of periodontitis: A systematic review. J. Am. Dent. Assoc. 2015, 146, 150–163. [Google Scholar] [CrossRef] [PubMed]
- Preus, H.R.; Dahlen, G.; Gjermo, P.; Baelum, V. Microbiologic observations after four treatment strategies among patients with periodontitis maintaining a high standard of oral hygiene: Secondary analysis of a randomized controlled clinical trial. J. Periodontol. 2015, 86, 856–865. [Google Scholar] [CrossRef] [PubMed]
- Correa, M.G.; Oliveira, D.H.; Saraceni, C.H.; Ribeiro, F.V.; Pimentel, S.P.; Cirano, F.R.; Casarin, R.C. Short-term microbiological effects of photodynamic therapy in non-surgical periodontal treatment of residual pockets: A split-mouth rct. Lasers Surg. Med. 2016, 48, 944–950. [Google Scholar] [CrossRef] [PubMed]
- Maisch, T. Anti-microbial photodynamic therapy: Useful in the future? Lasers Med. Sci. 2007, 22, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Fourmousis, I.; Suvan, J.; Cortellini, P.; Bragger, U.; Lang, N.P.; European Research Group on Periodontology (ERGOPERIO). Healing, post-operative morbidity and patient perception of outcomes following regenerative therapy of deep intrabony defects. J. Clin. Periodontol. 2004, 31, 1092–1098. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Aoki, A.; Romanos, G.; Schwarz, F.; Miron, R.J.; Cosgarea, R. Is photodynamic therapy an effective treatment for periodontal and peri-implant infections? Dent. Clin. N. Am. 2015, 59, 831–858. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Author Country | Sample Size (Male/Female) and Mean Age | Study design; Power of Study; Case Allotment | Outcome Measured | Treatment Arms | Conclusion |
|---|---|---|---|---|---|
| Kolbe et al. [26] Brazil | 22 (10/12) 48.52 y | Split-mouth 83% (CAL) Computer-generated | Clinical, Microbiology (polymerase chain reaction(PCR)); Pain perception (Visual Analogue Scale (VAS)) | Scaling and Root Planing (SRP) aPDT Photosensitizer | All therapies promoted similar improvements in clinical parameters. The aPDT protocol presented inferior frequency of Porphyromonas gingivalis at three months when compared with the other therapies. aPDT as an exclusive therapy may be considered a non-invasive alternative for treating residual pockets and offers advantages in the modulation of cytokines. |
| Carvalho et al. [33] Brazil | 34 (21/13) 48 y | Parallel | Pocket probing depth (PPD), CAL, bleeding on probing (BoP) and plaque index (PI) | SRP aPDT | Both treatments resulted in significant clinical improvement in patients with residual periodontal pockets. We did not find any additional significant benefit of PDT in terms of PPD, CAL, BoP, or pathogen level reduction. |
| Betsy et al. [23] India | 90 (39/51) 39.6 y | Parallel 80% (PD) Tippet’s 2-digit number table | Clinical and halitosis as perceived by patient | SRP SRP + aPDT | PD improved after three months and halitosis after one month. Statistically significant improvements in the gingival index and gingival bleeding index were observed for the test group after two weeks and one month of aPDT, respectively. aPDT is a beneficial adjunct to SRP in the non-surgical treatment and management of chronic periodontitis in the short term. |
| Luchesi et al. [19] Brazil | 37 50.5 y | Parallel 86% (CAL) Computer-generated | Clinical, Microbiology (PCR); Immunology (granulocyte-macrophage colony-stimulating factor (GM-CSF), interferon (IFN), Interleukin (IL)-6 and Interleukin-8 levels) | SRP + aPDT SRP + non-activated light (only PS) | Clinical parameters improved after both therapies. Did not promote clinical benefits for class II furcations; however, there were advantages in terms of the local levels of cytokines and periodontopathogens reduction. |
| Dilsiz et al. [20] Turkey | 24 (10/14) 40.7 y | Split-mouth Computer-generated | SRP SRP + aPDT SRP + KTP | Improvement in PD and CAL gain following treatment. Additional use of potassium titanyl phosphate (KTP) laser was found to be better in improving clinical parameters than conventional periodontal therapy of deeper pockets. | |
| Alwaeli et al. [32] Malaysia | 21 (7/14) 40.9 y | Split-mouth Computer-generated | SRP SRP + aPDT | Significant improvement in all evaluated clinical parameters for at least one year. There were significantly greater reductions and gains for SRP + aPDT than for SRP at all three-time points. aPDT as an adjunctive therapy to SRP represents a promising therapeutic concept for persistent periodontitis. | |
| Campanile et al. [27] Switzerland | 27 (14/13) 62.8 y | Parallel Smokers included 80% (PD) Computer-generated | Clinical, Microbiology (PCR); Pain perception (VAS); Immunology (C-reactive protein, Serum amyloid A, fibrinogen, procalcitonin, and α-2 macroglobulin) | aPDT twice in one week aPDT once Sham without active light | Significant PD and BoP reduction after three months when aPDT was administered twice a week. C-reactive protein was significantly lower only when the laser had been activated twice. |
| Bassir et al. [24] USA | 16 (8/8) 50.3 y | Split-mouth 80% (CAL) Computer-generated | Clinical | LED PS aPDT SRP | No additional benefit was noticed with administration of photoactivated disinfection (PAD) using LED in patients with moderate to severe chronic periodontitis. |
| Campos et al. [34] Brazil | 15 (8/7) 48.1 y | Split-mouth 80% (PD) Computer-generated | Clinical | SRP SRP + aPDT | aPDT as an adjunctive to mechanical debridement demonstrated additional clinical benefits for residual pockets in single-rooted teeth and may be an alternative therapeutic strategy in supportive periodontal maintenance. |
| Balata et al. [18] Brazil | 22 (8/14) 43.18 y | Split-mouth 80% (CAL) Coin toss | Clinical | SRP SRP + aPDT | Both approaches resulted in significant clinical improvement in the treatment of severe chronic periodontitis. aPDT did not provide any additional benefit. |
| Barekdar et al. [21] Germany | 22 (12/10) 59.3 y | Split-mouth | Clinical | SRP SRP + aPDT | A greater reduction of the PD was achieved by a combination of SRP/aPDT; therefore, aPDT is suitable as an adjuvant therapy. |
| Giannopoulou et al. [28] Switzerland | 32 (23/9) 52 y | Split-mouth Smokers included 80% (PD) Computer-generated | Clinical, Immunology (IL-17, basic fibroblast growth factor, granulocyte-macrophage colony-stimulating factor (GCSF), macrophage inflammatory protein (MIP)) | SRP Diode laser aPDT | No significant differences were observed among the three treatment modalities at any time point for any biochemical parameter or enhanced expression of inflammatory mediators. |
| Cappuyns et al. [29] Switzerland | 32 (23/9) 52 y | Split-mouth Smokers included 80% (PD) Computer-generated | Clinical, Microbiology (RNA probes); Pain perception (VAS) | SRP Diode laser aPDT | At the end of six months, statistically significant PD and BoP reductions were recorded. Frequencies of three periodontal pathogens were significantly lower in groups with aPDT- and SRP-treated than in diode soft laser-treated quadrants after 14 days. However, the same was not noticed at the end of two and six months. aPDT resulted in a reduction in the number of pockets after six months. |
| Lui et al. [22] Hong Kong | 24 (10/14) 50 y | Split-mouth | Clinical, Immunology (IL-1b levels in gingival crevicular fluid) | SRP SRP + one course of low level laser therapy (LLT) and aPDT within 5 days | The test teeth achieved greater reductions in the percentage of sites with bleeding on probing and in mean probing depth at one month compared with the control teeth and also greater reduction of interleukin (IL)-1b levels in gingival crevicular fluid at 1 week than did the control sites. No significant differences in periodontal parameters were found between the test and control teeth at three months. |
| Theodoro et al. [25] Brazil | 33 (12/21) 43.12 y | Split-mouth 81% (CAL) Computer-generated | Clinical, Microbiology (PCR) | SRP SRP + Toluidine Blue O (TBO) SRP + aPDT | All treatment groups showed an improvement in all clinical parameters and a significant reduction in the proportion of sites positive for periodontopathogens at 60, 90, and 180 days compared to baseline. None of the periodontal parameters showed a significant difference among the groups. At 180 days, aPDT treatment led to a significant reduction in the percentage of sites positive for all bacteria compared to SRP alone. |
| Sigush et al. [31] Germany | 24 (7/17) 42.7 y | Parallel Drawing lots | Clinical, Microbiology (PCR) | SRP + PS SRP + aPDT | Significant reductions in reddening, BoP, and mean PD and CAL were observed during the observation period and with respect to controls. Appropriate to reduce periodontal inflammation and to successfully treat infection with Fusobacterium nucleatum. |
| Ruhling et al. [30] Germany | 60 48 y | Parallel 80% (PD) Computer-generated | SRP aPDT | aPDT was not found to be better than routine mechanical debridement in the management of persistent pockets, but still maybe considered a valuable therapeutic option. | |
| Christodoulides et al. [12] Germany | 24 (13/11) 45 y | Parallel 80% (PD) Coin toss | SRP SRP + aPDT | Additional application of a single episode of aPDT to SRP failed to result in an additional improvement in terms of PD reduction and CAL gain, but resulted in a significantly higher reduction in bleeding scores compared to SRP alone. | |
| Braun et al. [11] Germany | 20 (9/11) 46.6 y | Split-mouth | SRP SRP + aPDT | Improvement in clinical parameters with the use of adjunctive aPDT as compared to subgingival debridement. | |
| Chondros et al. [13] Germany | 24 (10/14) 49.3 y | Parallel 80% (PD) Coin toss | Clinical, Microbiology (PCR) | SRP SRP + aPDT | Additional application of a single episode of aPDT to SRP failed to result in additional improvement. Significantly higher reduction of bleeding scores in test group. At three months and six months, a statistically significantly higher improvement of BoP was found in the test group. At three months after therapy, the microbiological analysis showed a statistically significant reduction of F.nucleatum and Eubacterium nodatum in the test group. |
| Author Country | Sample Size (Male/Female) | Power of the Study | Type of Randomization | Type of Blinding | Case Allotment | Whether Intention-to-Treat (ITT) Analysis Done |
|---|---|---|---|---|---|---|
| Kolbe et al. [26] Brazil | 22 (10/12) | 83% (CAL) | Not mentioned | Double-blinded | Computer-generated | Yes |
| Carvalho et al. [33] Brazil | 34 (21/13) | 90% (CAL) | Block randomization (size = 4) | Double -blinded | Computer-generated | Yes |
| Betsy et al. [23] India | 90 (39/51) | 80% (PD) | Block randomization (size = 4) | Double-blinded | Tippet’s 2-digit number table | Yes |
| Luchesi et al. [19] Brazil | 37 | 86% (CAL) | Not mentioned | Double-blinded | Computer-generated | Yes |
| Dilsiz et al. [20] Turkey | 24 (10/14) | Not given | Not mentioned | Double-blinded | Computer-generated | Yes |
| Alwaeli et al. [32] Malaysia | 21 (7/14) | Not given | Not mentioned | Double-blinded | Computer-generated | No |
| Campanile et al. [27] Switzerland | 27 (14/13) | 80% (PD) | Not mentioned | Single-blinded | Computer-generated | No |
| Bassir et al. [24] USA | 16 (8/8) | 80% (PD) | Block randomization (size = 1) | Double-blinded | Computer-generated | Not mentioned |
| Campos et al. [34] Brazil | 15 | 80% (PD) | Not mentioned | Double-blinded | Computer-generated | Not mentioned |
| Balata et al. [18] Brazil | 22 (8/14) | 80% (CAL) | Not mentioned | Not given | Coin toss | Yes |
| Barekdar et al. [21] Germany | 22 (12/10) | Not mentioned | Not mentioned | Single-blinded | Not mentioned | Yes |
| Giannopoulou et al. [28] Switzerland | 32 (23/9) | 80% (PD) | Not mentioned | Not mentioned | Computer-generated | No |
| Cappuyns et al. [29] Switzerland | 32 (23/9) | 80% (PD) | Not mentioned | Single-blinded | Computer-generated | No |
| Lui et al. [22] Hong Kong | 24 (10/14) | Not mentioned | Not mentioned | Single-blinded | Not mentioned | Yes |
| Theodoro et al. [25] Brazil | 33 (12/21) | 81% (CAL) | Not mentioned | Single-blinded | Computer-generated | Yes |
| Sigush et al. [31] Germany | 24 (7/17) | Not mentioned | Not mentioned | Not given | Drawing lots | Not mentioned |
| Ruhing et al. [30] Germany | 60 | 80% (PD) | Not mentioned | Single-blinded | Computer-generated | No |
| Christodoulides et al. [12] Germany | 24 (13/11) | 80% (PD) | Not mentioned | Not given | Coin toss | Yes |
| Braun et al. [11] Germany | 20 (9/11) | Not mentioned | Not mentioned | Single-blinded | Not mentioned | Yes |
| Chondros et al. [13] Germany | 24 (10/14) | 80% (PD) | Not mentioned | Single-blinded | Coin toss | Yes |
| Author Country | Photosensitizer Concentration | Resident Time of Photosensitizer | Laser Application Time | Laser Wavelength | Laser Output | Fiber Optic Tip Diameter | Laser Energy |
|---|---|---|---|---|---|---|---|
| Kolbe et al. [26] Brazil | Methylene blue 10 mg/mL | 1 min | 1 min | 660 nm | 60 mw/cm2 | Not mentioned | 129 J |
| Carvalho et al. [33] Brazil | Methylene blue 0.01% | 5 min | 1 min | 660 nm | 40 mw/cm2 | Not mentioned | 90 J |
| Betsy et al. [23] India | Methylene blue 10 mg/mL | 3 min | 1 min | 655 nm | 1 W/cm2 | 200 μm | Not mentioned |
| Luchesi et al. [19] Brazil | Methylene blue 10 mg/mL | 1 min | 1 min | 660 nm | 60 mw/cm2 | 600 μm | 129 J |
| Dilsiz et al. [20] Turkey | Methylene blue (25 g) 1% | 3 min | 1 min | 808 nm | 100 mw/cm2 | 300 μm | 6 J |
| Alwaeli et al. [32] Malaysia | Phenothiazine chloride | 1 min | 1 min | 660 nm | 100 mw/cm2 | Not mentioned | Not mentioned |
| Campanile et al. [27] Switzerland | Methylene blue | 1 min | 1 min | 670 nm | 280 mw/cm2 | Not mentioned | Not mentioned |
| Balata et al. [18] Brazil | Methylene blue 0.01% | 2 min | 1 min | 660 nm | 100 mw/cm2 | Not mentioned | 320 J |
| Bassir et al. [24] USA | Toluidine blue O 0.1 mg/mL | 3 min | 1 min | 635 nm | 2 W/cm2 | Not mentioned | Not mentioned |
| Barekdar et al. [21] Germany | Methylene blue 0.01% | 2 min | 1 min | 670 nm | 150 mw/cm2 | 600 μm | Not mentioned |
| Giannelli et al. [39] Italy | Methylene blue 0.03% | 5 min | 1 min | 635 nm | 100 mw/cm2 | 600 μm | 3.8 J |
| Giannopoulou et al. [28] Switzerland | Phenothiazine chloride; 100 μg/mL | 3 min | 1 min | 660 nm | 100 mw/cm2 | 750 μm | 3 J |
| Cappuyns et al. [29] Switzerland | Phenothiazine chloride; 100 μg/mL | 1 min | 1 min | 660 nm | 40 mw/cm2 | Not mentioned | Not mentioned |
| Lui et al. [22] Hong Kong | Methylene blue 1% | 3 min | 30 s | 940 nm | 1.5 W/cm2 | Not mentioned | 4 J |
| Theodoro et al. [25] Brazil | Toluidine blue O 100 μg/mL | 1 min | 150 s | 660 nm | 400 mw/cm2 | Not mentioned | Not mentioned |
| Sigush et al. [31] Germany | Phenothiazine | 1 min | 1 min | 660 nm | 60 mw/cm2 | 0.6 mm | Not mentioned |
| Ruhing et al. [30] Germany | Tolonium chloride 5% | Not mentioned | 1 min | 635 nm | 100 mw/cm2 | Not mentioned | Not mentioned |
| Christodoulides et al. [12] Germany | Phenothiazine | 3 min | 1 min | 670 nm | 75 mw/cm2 | Not mentioned | Not mentioned |
| Braun et al. [11] Germany | Phenothiazine | 3 min | 1 min | 660 nm | 100 mw/cm2 | Not mentioned | Not mentioned |
| Chondros et al. [13] Germany | Phenothiazine | Not mentioned | 1 min | 670 nm | 75 mw/cm2 | Not mentioned | Not mentioned |
| Author Country | Sample Size | Outcome Measured | Conclusions |
|---|---|---|---|
| Kolbe et al. [26] Brazil | 22 | Microbiology(PCR); Pain perception (VAS) | Similar improvements noticed in clinical parameters with all treatments. PDT protocol presented inferior frequency of P. gingivalis at three months when compared with the other therapies. aPDT as an exclusive therapy may be considered a non-invasive alternative for treating residual pockets, offering advantages in the modulation of cytokines. |
| Carvalho et al. [33] Brazil | 34 | Microbiology(PCR); Pocket probing depth (PPD), CAL, BoP and PI | All treatments resulted in significant clinical improvement in patients with residual periodontal pockets. PDT failed to show superior clinical results and pathogen load reduction in persistent pockets, compared to supragingival plaque control. |
| Betsy et al. [23] India | 90 | Halitosis as perceived by patient | Changes in PD after three months and halitosis after one month. Gingival index and gingival bleeding index improved significantly in the test group after two weeks and one month of aPDT. As an adjunct to SRP, aPDT shows effectiveness in the short term for managing chronic periodontitis. |
| Luchesi et al. [19] Brazil | 37 | Microbiology (PCR); Immunology (GM-CSF, IFN-c, IL-6 and IL-8 levels) | Clinical parameters improved after both therapies. At six months, real-time PCR evaluation showed a decrease in P. gingivalis and Tannerella forsythia only in the PDT group, with no inter-group differences. IL-4 and IL-10 levels increased in both groups at six months. GM-CSF, IL-8, IL-1b and IL-6 levels decreased only in the PDT group after three months. At three months, inter-group analyses showed that GM-CSF, IFN-c, IL-6 and IL-8 levels were lower in the PDT group. At six months, lower IL-1b levels were also observed in the PDT group. Did not promote clinical benefits for class II furcations. |
| Campanile et al. [27] Switzerland | 27 | Microbiology (PCR); Pain perception (VAS); Immunology (C-reactive protein, Serum amyloid A, fibrinogen, procalcitonin, and α-2 macroglobulin) | Detection frequencies of the studied microorganisms at >1000 and >100,000 cells/mL did not change significantly from baseline to months 3 or 6 in any group. Significant PD and BoP reduction after three months when aPDT given twice a week. C-reactive protein was significantly lower only if the laser had been activated twice. |
| Cappuyns et al. [29] Switzerland | 32 | Microbiology (RNA probes); Pain perception (VAS) | Statistically significant PD and BoP reduction was seen at six months. Frequencies of three microorganisms were significantly lower in aPDT- and SRP-treated than in diode soft laser-treated quadrants after 14 days, but not at months 2 and 6. aPDT resulted in fewer residual pockets after six months. |
| Giannopoulou et al. [28] Switzerland | 32 | Immunology (IL-17, basic fibroblast growth factor, granulocyte colony-stimulating factor, and macrophage inflammatory protein 1-a) | No significant differences were observed among the three treatment modalities at any time point for any biochemical parameter or enhanced expression of inflammatory mediators. |
| Theodoro et al. [25] Brazil | 33 | Microbiology (PCR) | All treatment groups showed an improvement in all clinical parameters, and a significant reduction in the proportion of sites positive for periodontopathogens at 60, 90, and 180 d compared to the baseline. None of the periodontal parameters showed a significant difference among the groups. At 180 days, PDT treatment led to a significant reduction in the percentage of sites positive for all bacteria compared to SRP alone. |
| Lui et al. [22] Hong Kong | 24 | Immunology (IL-1b levels in gingival crevicular fluid) | A significant decrease in gingival crevicular fluid volume was observed in both groups at one week, with a further decrease at one month in the test sites. The test sites showed a greater reduction of IL-1b levels in gingival crevicular fluid at one week than the control sites. No significant differences in periodontal parameters were found between the test and control teeth at three months. |
| Sigush et al. [31] Germany | 24 | Microbiology (PCR) | BoP, mean PD, and mean CAL showed improvement in the test group as compared to controls. aPDT may be used to manage periodontal inflammation and infection with F. nucleatum. |
| Chondros et al. [13] Germany | 24 | Microbiology (PCR) | Application of a single episode of aPDT to SRP failed to result in an additional improvement. Significantly higher reduction of bleeding scores in test group. At three and six months, a statistically significantly higher improvement of BoP was found in the test group. At three months after therapy, the microbiological analysis showed a statistically significant reduction of F. nucleatum and E. nodatum in the test group. |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joseph, B.; Janam, P.; Narayanan, S.; Anil, S. Is Antimicrobial Photodynamic Therapy Effective as an Adjunct to Scaling and Root Planing in Patients with Chronic Periodontitis? A Systematic Review. Biomolecules 2017, 7, 79. https://doi.org/10.3390/biom7040079
Joseph B, Janam P, Narayanan S, Anil S. Is Antimicrobial Photodynamic Therapy Effective as an Adjunct to Scaling and Root Planing in Patients with Chronic Periodontitis? A Systematic Review. Biomolecules. 2017; 7(4):79. https://doi.org/10.3390/biom7040079
Chicago/Turabian StyleJoseph, Betsy, Presanthila Janam, Subhash Narayanan, and Sukumaran Anil. 2017. "Is Antimicrobial Photodynamic Therapy Effective as an Adjunct to Scaling and Root Planing in Patients with Chronic Periodontitis? A Systematic Review" Biomolecules 7, no. 4: 79. https://doi.org/10.3390/biom7040079
APA StyleJoseph, B., Janam, P., Narayanan, S., & Anil, S. (2017). Is Antimicrobial Photodynamic Therapy Effective as an Adjunct to Scaling and Root Planing in Patients with Chronic Periodontitis? A Systematic Review. Biomolecules, 7(4), 79. https://doi.org/10.3390/biom7040079