Low-Circulating Homoarginine is Associated with Dilatation and Decreased Function of the Left Ventricle in the General Population

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Interview, Medical, and Laboratory Examination
2.3. Ultrasound Measurements
2.4. Statistics
3. Results
3.1. Population Description
3.2. Association of hArg with Left Ventricular Structural Parameters
3.3. Association of hArg with Left Ventricular Functional Parameters
3.4. Assocation of hArg with Right Ventricular Parameters
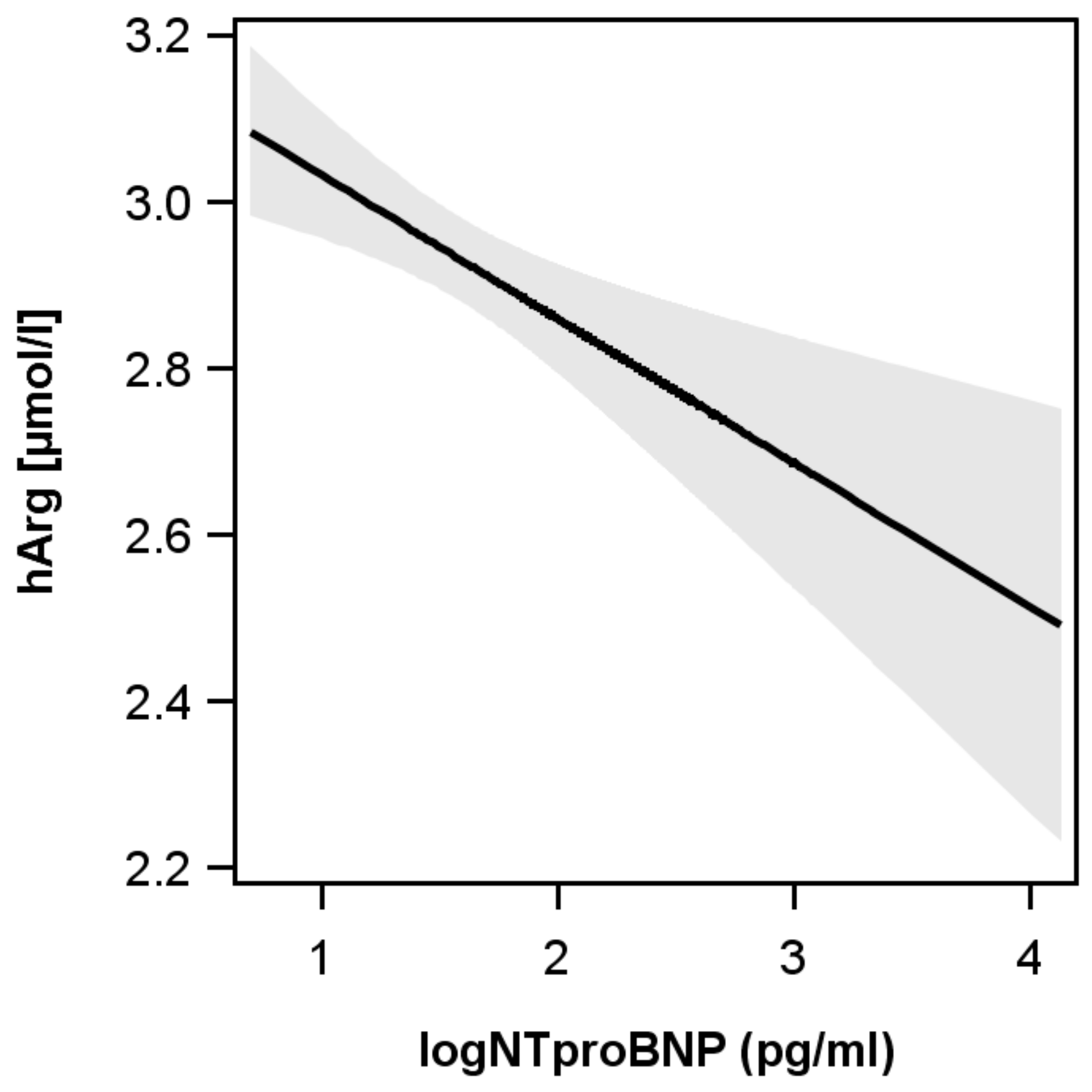
3.5. Association of hARG with Biochemical Parameters (NTproBNP)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Morris, S.M., Jr. Arginine Metabolism Revisited. J. Nutr. 2016, 146, 2579S–2586S. [Google Scholar] [PubMed]
- Davids, M.; Ndika, J.D.; Salomons, G.S.; Blom, H.J.; Teerlink, T. Promiscuous activity of arginine: Glycine amidinotransferase is responsible for the synthesis of the novel cardiovascular risk factor homoarginine. FEBS Lett. 2012, 586, 3653–3657. [Google Scholar] [PubMed]
- Moali, C.; Boucher, J.L.; Sari, M.A.; Stuehr, D.J.; Mansuy, D. Substrate specificity of NO synthases: Detailed comparison of l-arginine, homo-l-arginine, their N omega-hydroxy derivatives, and N omega-hydroxynor-l-arginine. Biochemistry 1998, 37, 10453–10460. [Google Scholar] [CrossRef] [PubMed]
- Tommasi, S.; Elliot, D.J.; Da Boit, M.; Gray, S.R.; Lewis, B.C.; Mangoni, A.A. Homoarginine and inhibition of human arginase activity: Kinetic characterization and biological relevance. Sci. Rep. 2018, 8, 3697. [Google Scholar] [CrossRef] [PubMed]
- Marz, W.; Meinitzer, A.; Drechsler, C.; Pilz, S.; Krane, V.; Kleber, M.E.; Fischer, J.; Winkelmann, B.R.; Böhm, B.O.; Ritz, E.; et al. Homoarginine, cardiovascular risk, and mortality. Circulation 2010, 122, 967–975. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Edelmann, F.; Meinitzer, A.; Gelbrich, G.; Doner, U.; Dungen, H.D.; Tomaschitz, A.; Kienreich, K.; Gaksch, M.; Duvinage, A.; et al. Associations of methylarginines and homoarginine with diastolic dysfunction and cardiovascular risk factors in patients with preserved left ventricular ejection fraction. J. Card. Fail. 2014, 20, 923–930. [Google Scholar] [PubMed]
- Faller, K.M.E.; Atzler, D.; McAndrew, D.J.; Zervou, S.; Whittington, H.J.; Simon, J.N.; Tomaschitz, A.; Kienreich, K.; Gaksch, M.; Duvinage, A.; et al. Impaired cardiac contractile function in arginine: Glycine amidinotransferase knockout mice devoid of creatine is rescued by homoarginine but not creatine. Cardiovasc. Res. 2018, 114, 417–430. [Google Scholar] [PubMed]
- Choe, C.U.; Atzler, D.; Wild, P.S.; Carter, A.M.; Boger, R.H.; Ojeda, F.; Simova, O.; Stockebrand, M.; Lackner, K.; Nabuurs, C.; et al. Homoarginine levels are regulated by l-arginine: Glycine amidinotransferase and affect stroke outcome: Results from human and murine studies. Circulation 2013, 128, 1451–1461. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Meinitzer, A.; Tomaschitz, A.; Drechsler, C.; Ritz, E.; Krane, V.; Wanner, C.; Boehm, B.O.; März, W. Low homoarginine concentration is a novel risk factor for heart disease. Heart 2011, 97, 1222–1227. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Teerlink, T.; Scheffer, P.G.; Meinitzer, A.; Rutters, F.; Tomaschitz, A.; Drechsler, C.; Kienreich, K.; Nijpels, G.; Stehouwer, C.D.; et al. Homoarginine and mortality in an older population: The Hoorn study. Eur. J. Clin. Investig. 2014, 44, 200–208. [Google Scholar]
- Drechsler, C.; Meinitzer, A.; Pilz, S.; Krane, V.; Tomaschitz, A.; Ritz, E.; März, W.; Wanner, C. Homoarginine, heart failure, and sudden cardiac death in haemodialysis patients. Eur. J. Heart Fail. 2011, 13, 852–859. [Google Scholar] [PubMed] [Green Version]
- Atzler, D.; Rosenberg, M.; Anderssohn, M.; Choe, C.U.; Lutz, M.; Zugck, C.; Böger, R.H.; Frey, N.; Schwedhelm, E. Homoarginine—An independent marker of mortality in heart failure. Int. J. Cardiol. 2013, 168, 4907–4909. [Google Scholar] [CrossRef] [PubMed]
- Volzke, H.; Alte, D.; Schmidt, C.O.; Radke, D.; Lorbeer, R.; Friedrich, N.; Aumann, N.; Lau, K.; Piontek, M.; Born, G.; et al. Cohort profile: The study of health in Pomerania. Int. J. Epidemiol. 2011, 40, 294–307. [Google Scholar] [PubMed]
- World Health Organization. Physical Status: The Use and Interpretation of Anthropometry; Report of a WHO Expert Committee; World Health Organization Technical Report Series; World Health Organization: Geneva, Switzerland, 1995; Volume 854, pp. 1–452. [Google Scholar]
- Levey, A.S.; Coresh, J.; Greene, T.; Marsh, J.; Stevens, L.A.; Kusek, J.W.; Van Lente, F. Chronic Kidney Disease Epidemiology Collaboration. Expressing the Modification of Diet in Renal Disease Study equation for estimating glomerular filtration rate with standardized serum creatinine values. Clin. Chem. 2007, 53, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Atzler, D.; Schwedhelm, E.; Nauck, M.; Ittermann, T.; Böger, R.H.; Friedrich, N. Serum reference intervals of homoarginine, ADMA, and SDMA in the Study of Health in Pomerania. Clin. Chem. Lab. Med. 2014, 52, 1835–1842. [Google Scholar] [CrossRef] [PubMed]
- Volzke, H.; Haring, R.; Lorbeer, R.; Wallaschofski, H.; Reffelmann, T.; Empen, K.; Rettig, R.; John, U.; Felix, S.B.; Dörr, M. Heart valve sclerosis predicts all-cause and cardiovascular mortality. Atherosclerosis 2010, 209, 606–610. [Google Scholar] [PubMed]
- Schiller, N.B.; Shah, P.M.; Crawford, M.; DeMaria, A.; Devereux, R.; Feigenbaum, H.; Gutgesell, H.; Reichek, N.; Sahn, D.; Schnittger, I.; et al. Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. American Society of Echocardiography Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms. J. Am. Soc. Echocardiogr. 1989, 2, 358–367. [Google Scholar] [CrossRef]
- Reichek, N.; Devereux, R.B. Left ventricular hypertrophy: Relationship of anatomic, echocardiographic and electrocardiographic findings. Circulation 1981, 63, 1391–1398. [Google Scholar] [CrossRef] [PubMed]
- Devereux, R.B.; Alonso, D.R.; Lutas, E.M.; Gottlieb, G.J.; Campo, E.; Sachs, I.; Reichek, N. Echocardiographic assessment of left ventricular hypertrophy: Comparison to necropsy findings. Am. J. Cardiol. 1986, 57, 450–458. [Google Scholar] [CrossRef]
- Verbraecken, J.; Van de Heyning, P.; De Backer, W.; Van Gaal, L. Body surface area in normal-weight, overweight, and obese adults. A. comparison study. Metabolism 2006, 55, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [PubMed]
- Stone, C.J.; Koo, C.-Y. Additive splines in statistics. Proc. Stat. Comput. Sect. Am. Stat. Assoc. 1985, 27, 45–48. [Google Scholar]
- Atzler, D.; Schwedhelm, E.; Choe, C.U. l-homoarginine and cardiovascular disease. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Lygate, C.A.; Schneider, J.E.; Neubauer, S. Investigating cardiac energetics in heart failure. Exp. Physiol. 2013, 98, 601–605. [Google Scholar] [PubMed]
- Cullen, M.E.; Yuen, A.H.; Felkin, L.E.; Smolenski, R.T.; Hall, J.L.; Grindle, S.; Miller, L.W.; Birks, E.J.; Yacoub, M.H.; Barton, P.J. Myocardial expression of the arginine: Glycine amidinotransferase gene is elevated in heart failure and normalized after recovery: Potential implications for local creatine synthesis. Circulation 2006, 114 (Suppl. 1), I16–I20. [Google Scholar] [CrossRef] [PubMed]
- Seppala, I.; Oksala, N.; Jula, A.; Kangas, A.J.; Soininen, P.; Hutri-Kahonen, N.; März, W.; Meinitzer, A.; Juonala, M.; Kähönen, M.; et al. The biomarker and causal roles of homoarginine in the development of cardiometabolic diseases: An observational and Mendelian randomization analysis. Sci. Rep. 2017, 7, 1130. [Google Scholar] [CrossRef] [PubMed]
- Atzler, D.; McAndrew, D.J.; Cordts, K.; Schneider, J.E.; Zervou, S.; Schwedhelm, E.; Neubauer, S.; Lygate, C.A. Dietary Supplementation with Homoarginine Preserves Cardiac Function in a Murine Model of Post-Myocardial Infarction Heart Failure. Circulation 2017, 135, 400–402. [Google Scholar] [CrossRef] [PubMed]
- Atzler, D.; Schönhoff, M.; Cordts, K.; Ortland, I.; Hoppe, J.; Hummel, F.C.; Gerloff, C.; Jaehde, U.; Jagodzinski, A.; Böger, R.H.; et al. Oral supplementation with l-homoarginine in young volunteers. Br. J. Clin. Pharmacol. 2016, 82, 1477–1485. [Google Scholar] [PubMed]


{kind=link}
| Parameter | Median (25th and 75th Percentile) or % |
|---|---|
| Age (years) | 48 (37, 60) |
| Sex (% male) | 45.5 |
| Systolic blood pressure (mmHg) | 125 (113, 137) |
| Body mass index (BMI) (kg/m2) | 26.7 (23.9, 30.1) |
| Height (cm) | 170 (163, 177) |
| Weight (kg) | 77.9 (67.6, 89.2) |
| Smoking (%) | |
| Nonsmoker | 37.4 |
| Exsmoker | 34.7 |
| Smoker | 27.9 |
| Diabetes mellitus type 2 (%) | 7.4 |
| Hypertension (%) | 40.5 |
| Metabolic syndrome (%) | 23.4 |
| Estimated glomerular filtration rate (eGFR) (mL/min/1.73 m2) | 88.5 (76.5, 102.4) |
| Left ventricle (LV) structural echocardiographic parameters | |
| Left ventricular mass (LVM) (g) | 172.4 (138.4, 211.7) |
| LVM index (LVMI) (g/m2) | 90.5 (76.9, 106.5) |
| LV diameter during diastole (LVD) (cm) | 4.9 (4.5, 5.2) |
| LV diameter during systole (LVS) (cm) | 2.9 (2.6, 3.2) |
| Posterior wall diameter (PWD) (cm) | 1.0 (0.9, 1.1) |
| Relative wall thickness (RWT) | 0.4 (0.3, 0.4) |
| Left atrium (cm) | 3.8 (3.5, 4.2) |
| Aorta (cm) | 2.8 (2.5, 3.1) |
| LV systolic functional echocardiographic parameters | |
| LV ejection fraction (LVEF) (%) | 72 (66, 78) |
| Fractional shortening (%) | 41 (36, 46) |
| LV diastolic functional echocardiographic parameters | |
| Mitral valve (MV) E-wave (cm/s) | 0.7 (0.6, 0.8) |
| MV A-wave (cm/s) | 0.6 (0.5, 0.7) |
| MV duration A-wave (ms) | 133 (121, 147) |
| MV deceleration (dec.) Time (ms) | 179 (157, 203) |
| E/e ratio | 5.9 (4.9, 7.1) |
| RV structural echocardiographic parameters | |
| Right ventricle (RV) (cm) | 2.4 (2.1, 2.8) |
| Right ventricular outflow tract (RVOT) (cm) | 3.4 (3.0, 3.7) |
| RV systolic functional echocardiographic parameters | |
| Tricuspid annular plane systolic excursion (TAPSE) (cm) | 2.4 (2.1, 2.6) |
| Pulmonary valve (PV) acc. time (ms) | 134 (115, 152) |
| PV acc. slope | 5.8 (4.9, 7.1) |
| hArg (µmol/L) | |
| β for 1 SD Decrease of hArg (95% CI) | p | |
|---|---|---|
| LV structural echocardiographic parameters | ||
| LVM (g) | 1.29 | 0.0677 |
| (0.09, 2.67) | ||
| LVMI (g/m2) | 0.63 | 0.0703 |
| (0.05, 1.31) | ||
| LVD (mm) | 0.34 | <0.0001 |
| (0.19, 0.50) | ||
| LVS (mm) | 0.38 | <0.0001 |
| (−0.22, 0.54) | ||
| PWD (mm) | −0.01 | 0.5514 |
| (−0.06, 0.03) | ||
| RWT | −0.003 | 0.011 |
| (−0.006, −0.001) | ||
| Left atrium (mm) | −0.07 | 0.3795 |
| (0.09, 0.24) | ||
| Aorta (mm) | 0.07 | 0.2396 |
| (−0.05, −0.19) | ||
| LV systolic functional echocardiographic parameters | ||
| LVEF (%) | −0.47 | 0.0043 |
| (−0.79, −0.15) | ||
| Fractional shortening (%) | −0.35 | 0.0141 |
| (−0.62, −0.07) | ||
| LV diastolic functional echocardiographic parameters | ||
| MV E-wave (mm/s) | −0.002 | 0.2607 |
| (−0.008, 0.002) | ||
| MV A-wave (mm/s) | −0.003 | 0.1708 |
| (−0.008, 0.001) | ||
| MV duration A-wave (ms) | 0.41 | 0.2844 |
| (−0.34, 1.17) | ||
| MV dec. time (ms) | 0.24 | 0.7166 |
| (−1.08, 1.57) | ||
| E/e ratio | −0.02 | 0.4205 |
| (−0.08, 0.04) | ||
| RV structural echocardiographic parameters | ||
| RV (mm) | −0.0006 | 0.9422 |
| (−0.02, 0.02) | ||
| RVOT (cm) | 0.01 | 0.07 |
| (−0.001, 0.03) | ||
| RV systolic functional echocardiographic parameters | ||
| TAPSE (cm) | −0.009 | 0.1772 |
| (−0.023, 0.004) | ||
| PV acc. time (ms) | 0.39 | 0.3755 |
| (−0.48, 1.26) | ||
| PV acc. slope | −0.04 | 0.1977 |
| (−0.12, 0.02) | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bahls, M.; Atzler, D.; Markus, M.R.P.; Friedrich, N.; Böger, R.H.; Völzke, H.; Felix, S.B.; Schwedhelm, E.; Dörr, M. Low-Circulating Homoarginine is Associated with Dilatation and Decreased Function of the Left Ventricle in the General Population. Biomolecules 2018, 8, 63. https://doi.org/10.3390/biom8030063
Bahls M, Atzler D, Markus MRP, Friedrich N, Böger RH, Völzke H, Felix SB, Schwedhelm E, Dörr M. Low-Circulating Homoarginine is Associated with Dilatation and Decreased Function of the Left Ventricle in the General Population. Biomolecules. 2018; 8(3):63. https://doi.org/10.3390/biom8030063
Chicago/Turabian StyleBahls, Martin, Dorothee Atzler, Marcello R.P. Markus, Nele Friedrich, Rainer H. Böger, Henry Völzke, Stephan B. Felix, Edzard Schwedhelm, and Marcus Dörr. 2018. "Low-Circulating Homoarginine is Associated with Dilatation and Decreased Function of the Left Ventricle in the General Population" Biomolecules 8, no. 3: 63. https://doi.org/10.3390/biom8030063