1. Introduction
Cancer is a health condition that is characterized by the unregulated growth of abnormal cells that can develop in any tissue or organ inside the body. The World Health Organization says that it was the second most common cause of death in the world in 2020, with about 10 million deaths [
1]. Compared to other cancer types, colorectal cancer accounts for 1.80 million new cases and 783 thousand fatalities, whereas lung cancer contributes to 1.76 million new cases and 1.76 million fatalities. The two varieties of lung cancer that spread and grow quickly are small-cell lung cancer (SCLC) and non-small-cell lung cancer (NSCLC) [
2,
3]. Cells with neuroendocrine characteristics cause SCLC, which accounts for 15% of all instances of lung cancer and remains a hazardous form of the disease. The three pathologic types of NSCLC, including immense cell carcinoma, adenocarcinoma, and squamous cell carcinoma, account for 85% of all cases [
4]. The most common cause of death is colorectal cancer, which accounts for 10.7% of all instances [
1].
To examine the therapy possibilities in the early stages of the disease, a more precise diagnosis of various cancer subtypes is required. For lung cancer, radiography, computed tomography (CT) imaging, flexible sigmoidoscopy, and CT colonoscopy are among the non-invasive diagnostic techniques [
4]. Histopathology is one simple test that can be required to effectively diagnose the disease and improve the quality of treatment. However, non-invasive techniques may not always produce effective classifications of these cancers. Additionally, pathologists may grow exhausted from manually grading histological images. Additionally, expert pathologists are required for the precise classification of lung and colon cancer (LCC) subtypes; manual grading may be prone to mistakes. To lessen the workload on pathologists, automated image processing techniques for LCC subtype screening are necessary [
5].
There are a lot of different methods for diagnosing cancer symptoms. The amount of data kept in archives is increasing daily because of technical improvements [
5]. The rising accessibility of healthcare data offers researchers opportunities to enhance current methods for more in-depth clinical analysis [
6]. Artificial intelligence (AI) techniques like machine learning (ML) and DL are the foundation of automatic diagnosis approaches. Researchers have solved numerous health challenges and applications using a variety of traditional machine learning techniques [
7,
8]. The traditional method for utilizing ML to retrieve and categorize photos in the medical area is solely dependent on manually constructed features created through the feature engineering process. All kinds of characteristics must be used to automatically classify LCC. Filtering and segmentation algorithms can retrieve intensity values and texture descriptors, which are examples of low-level features that are important aspects of an image. Additionally, low-level characteristics can be extracted automatically from LCC images using feature extraction methods, including Haralick characteristics and local binary patterns (LBPs). They function as a base for representations of higher-level features [
9].
The characteristics of the surrounding tissue, as well as the tumor’s location, size, and shape, are important classification criteria for LCC. Both low-level and high-level features must be considered for automatic tumor categorization to be accurate and reliable. The basic characteristics of images are captured by low-level features, while high-level features offer general and meaningful data [
10]. Thus, due to its capacity to deal with these drawbacks and its powerful discrimination capabilities, DL has gained popularity for use in medical testing [
11]. These features can be automatically extracted using DL techniques, and they are necessary to organize treatments and make correct diagnoses. Combining these features is required to obtain high accuracy. Convolutional neural network (CNN) is a well-known DL architecture that is frequently employed in this context [
12]. Through their numerous deep layers, CNN models may identify high-level features in raw data. In this manner, CNNs can successfully analyze complicated and challenging data. These models have an increasing number of parameters, along with substantial complexity [
13]. The complexity and depth of the CNN architecture are what make the models so successful.
Based on the CNN model, explainable artificial intelligence (XAI) is a useful tool in the medical industry that increases the transparency of automatically generated prediction models. It speeds up the creation of predictive models, utilizing expertise in the field and helping to produce results that are understandable to humans [
14,
15]. There are several ways to show the most active areas and to make a model more explicable. A few examples of these techniques include utilizing XAI algorithms, Shapley Additive Explanation (SHAP), and gradient-weighted class activation mapping (Grad-CAM) [
16] for the model’s explanatory categorization [
17].
It is not easy to process LCC datasets using conventional methods as there are various challenges, such as the following:
- ▪
Most of these techniques have substantial computing costs and require a lot of labeled training data.
- ▪
Overfitting can happen when the model works well with training data but poorly with new, untested data.
- ▪
Risk of poor performance brought on by inaccurate or biased training data.
- ▪
DL models’ decision-making process is not explainable.
To avoid overfitting or inaccurate diagnosis, it is essential to use DL models that have been thoroughly tested and proven on large, diverse datasets. It is also critical to use techniques like cross-validation (CV) to account for any possible biases in the data used for training to guarantee the model’s wider applicability. The overall objective of the proposed method is to be improved by offering precise and early diagnoses that allow for quick and efficient treatment. This paper focuses on categorizing lung and colon cancer subtypes using histopathological images from a dataset named LC25000, which is publicly available on Kaggle. There are a total of five classes in the dataset, which are benign lung tissue, lung adenocarcinomas, lung squamous cell carcinoma, benign colon tissue, and colon adenocarcinomas.
Compared to DL models, the suggested model is less complex and very lightweight, with only eight layers, which makes it appropriate for real-time applications and mobile applications. The originality of the proposed work can be summed up as follows:
A novel lightweight multi-scale (LW-MS) end-to-end CNN model for the identification of LCC is introduced. The proposed model has 1.1 million trainable parameters and is superior to other models in this field, which need deeper layers to achieve acceptable detection accuracy. This reduces processing time and model complexity, making the system suitable for real-time applications.
To increase the accuracy and efficiency of multi-class predictions, predictions from multiple layers are concatenated to produce a range of feature maps that function at different resolutions.
XAI techniques have been integrated into the proposed LW-MS CNN model with its performance metrics analysis. This aspect has frequently been neglected in prior studies.
A web application system has been developed with the purpose of aiding pathologists and doctors in the diagnosis of histological pictures and offering substantiation for their scientific findings.
The remainder of the article is organized as follows.
Section 2 includes a review of the literature on the most current DL advancements related to LCC detection.
Section 3 discusses the proposed method in detail.
Section 4 presents and thoroughly discusses the experimental setup and achieved results.
Section 5 summarizes the proposed model’s findings and discusses the model. Finally,
Section 6 concludes the research and suggests potential future research directions.
2. Related Works
To classify images of lung tissues from histopathology, a computer-aided system (CAD) method was developed by Nishio et al. [
18]. They extracted visual characteristics from two datasets using homology-based processing of images (HI) and traditional texture analysis (TA), and then they assessed the effectiveness of eight ML algorithms. In both datasets, the HI-equipped CAD system outperformed the TA system. They concluded that for CAD systems, HI was significantly more advantageous than TA and that this could lead to the development of an accurate CAD system. Similarly, Mangal et al. [
19] developed a CAD system by looking at digital pathology images and using CNN to identify lung and colon cancer. In comparison to deep CNN models that employ TL trained on a similar collection and classical ML models, their experimental results on the LC25000 showed a decent accuracy of 96.61% for the colon and 97.89% for the lung, which were acquired by the CNN using the most recent feature descriptions. Shandilya et al. [
20] have created a CAD technique to categorize lung tissue histology pictures. They employed a dataset of histological pictures of lung tissue that was made publicly available for the development and validation of CAD. Multi-scale processing was used to extract image features. Seven CNN models that had been hyper-tuned before were used in a comparative analysis to predict lung cancer, with ResNet101 achieving the greatest overall accuracy at 98.67%. Masud et al. [
21] used DL on histopathology pictures to present a categorization system for five different types of lung and colon tissues. First, image sharpening was applied to pathological example images. A CNN model that was manually tweaked was trained using these features. This model’s accuracy performance was reported to be 96.33%.
Similarly, Hatuwal et al. [
22] stated a CNN-based technique for classifying histological images to diagnose cancer. They built and trained a neural network with a specific shape. The accuracy in training and validation were reported to be 96.11% and 97.20%, respectively. Similar to this, three CNN models were introduced by Tasnim et al. [
23] to assess colon cell imaging data. To calculate the learning rate, the models were developed and put to the test at various epochs. It was demonstrated that the maximum pooling layer has an accuracy of 97.49%, while the average pooling layer has an accuracy of 95.48%. MobileNetV2 outperforms the previous two versions, with a 99.67% accuracy rate and a 1.24% loss rate. However, Sikder et al. [
24] have suggested a novel technique for separating, recognizing, classifying, and spotting various malignant cell types in RGB and MRI images. They merged a CNN model with a SegNet method that employs anatomical changes that were better than the regular SegNet model to shorten training times and enhance segmentation results. The proposed method identified cancer cells from several cancer datasets with an average accuracy rate of 93%. They were able to overcome the drawbacks of using different cancer detection methods for MRI and histopathology data.
A CNN model for predicting colon cancer developed by Qasim et al. [
25] is notable for its speed and accuracy, with few parameters. They used two separate strategies in their model and then 256 feature maps were created by each. By increasing the number of features at different levels, they were able to increase the accuracy and sensitivity. The same dataset was used to develop and train the VGG16, which was used to evaluate the effectiveness of the suggested strategy. The proposed model’s achieved accuracy is 99.6%, while the VGG16’s is 96.2%. The results suggest that it was effective in detecting colon cancer. To classify different forms of lung and colon cancer, Talukder et al. [
1] have introduced a combination of ensemble attribute-obtaining techniques. Ensemble learning for image filtering and the deep feature extraction method were combined. The proposed hybrid model reportedly had a 99.05% accuracy rate in identifying the possibility of cancer. Hanan et al. [
26] have presented the Marine Predator Algorithm with DL (MPADL-LC3) method for classifying lung and colon cancer. This method leveraged MobileNet to generate feature vectors and used CLAHE-based contrast enhancement as a preprocessing step. They introduced MPA as a hyper-parameter optimizer, and a deep belief network was applied for classification. With a maximum accuracy of 99.27%, the comparison research emphasized the improved results of the MPADL-LC3 approach.
Attallah et al. [
27] have created a lightweight DL method. To achieve feature reduction and provide a more comprehensive representation of the data, the architecture uses various transformation techniques. In that sense, the SqueezeNet, ShuffleNet, and MobileNet algorithms are fed with HSI. Thus, the features extracted from the model are decreased by using PCA models and the fast Walsh–Hadamard transform (FHWT). It obtained 99.6% accuracy. Al-Jabbar et al. [
28] have suggested a method that combines ANN with fusion features and CNN models. The ANN achieved an accuracy of 99.64% with VGG-19 fusion features and handcrafted features. By analyzing the LC2500 dataset, Sameh et al. [
29] have built a unique deep network for LCC fine-tuning using pre-trained ResNet101. Hyper-parameter optimizations were used to make these improvements. They obtained 99.84%, 99.85%, 99.84%, 99.96%, and 99.94% scores for their model’s precision, recall, F1-score, specificity, and accuracy, respectively. Imran et al. [
30] have proposed a deep CNN model for the automated detection and characterization of colon cancer, in which textured images are trained in high resolution without being converted into low-resolution images by changing the classification of binary data in the resultant activation layer to the sigmoid function. They achieved 99.80% recall, 99.87% F1-score, 99.80% accuracy, and 100% precision. Two methods were presented by Kumar et al. [
3]. Six approaches for extracting handcrafted aspects based on color, texture, shape, and structure are provided in one method. They also employed seven frameworks for DL that extract features from deep data from histopathology pictures, with the idea of transfer learning. However, compared to manually created features, deep CNN network features show a considerable boost in classifier performance. The LCC tissue was recognized by the Random Forest classifier, with DenseNet-121 retrieving deep features with an accuracy and recall of 98.60%, precision of 98.63%, F1 score of 0.985, and receiver operating characteristic curve (ROC)—area under the ROC Curve (AUC) of 1.
Even though numerous research works show the outstanding accuracy in limited-class and binary classification scenarios, their performance steadily deteriorates as the number of classes rises. This phenomenon results from the growing difficulty of differentiating between many diseases with precisely various characteristics. This restriction makes the models less useful in actual clinical settings where patients may present with a range of lung diseases. Consequently, to perform a multi-class classification of lung and colon diseases with high accuracy and confidence for real-life scenarios, a customized and reliable deep learning framework is needed. In this study, a LW-MS CNN with 1.1 million parameters has been proposed to produce a more promising outcome than the state-of-the-art (SOTA) models. Nevertheless, Grad-CAM and SHAP have been used for showing the effectiveness of the model by detecting ROI despite all the challenges. Also, to the best of the authors’ knowledge, only a small number of studies have so far demonstrated these explainable AI methods to show interpretability.
4. Result Analysis
In this section, all the experimental setups and results of this research will be described in detail.
4.1. Experimental Setup
The experimental setup of the proposed system is described in this subsection.
Table 4 accommodates the system specifications upon which the proposed work has been based. All coding operations have been performed in Google Colab, which has a backend of Keras with TensorFlow, and the disk space for it is 78.2 GB. The GPU used was a Nvidia Tesla T4 with a RAM size of 15 GB. In this study, the operating system was Windows 11, and for visualization in web environments, Gradio Library was used.
4.2. Performance Metrics of the Proposed Framework
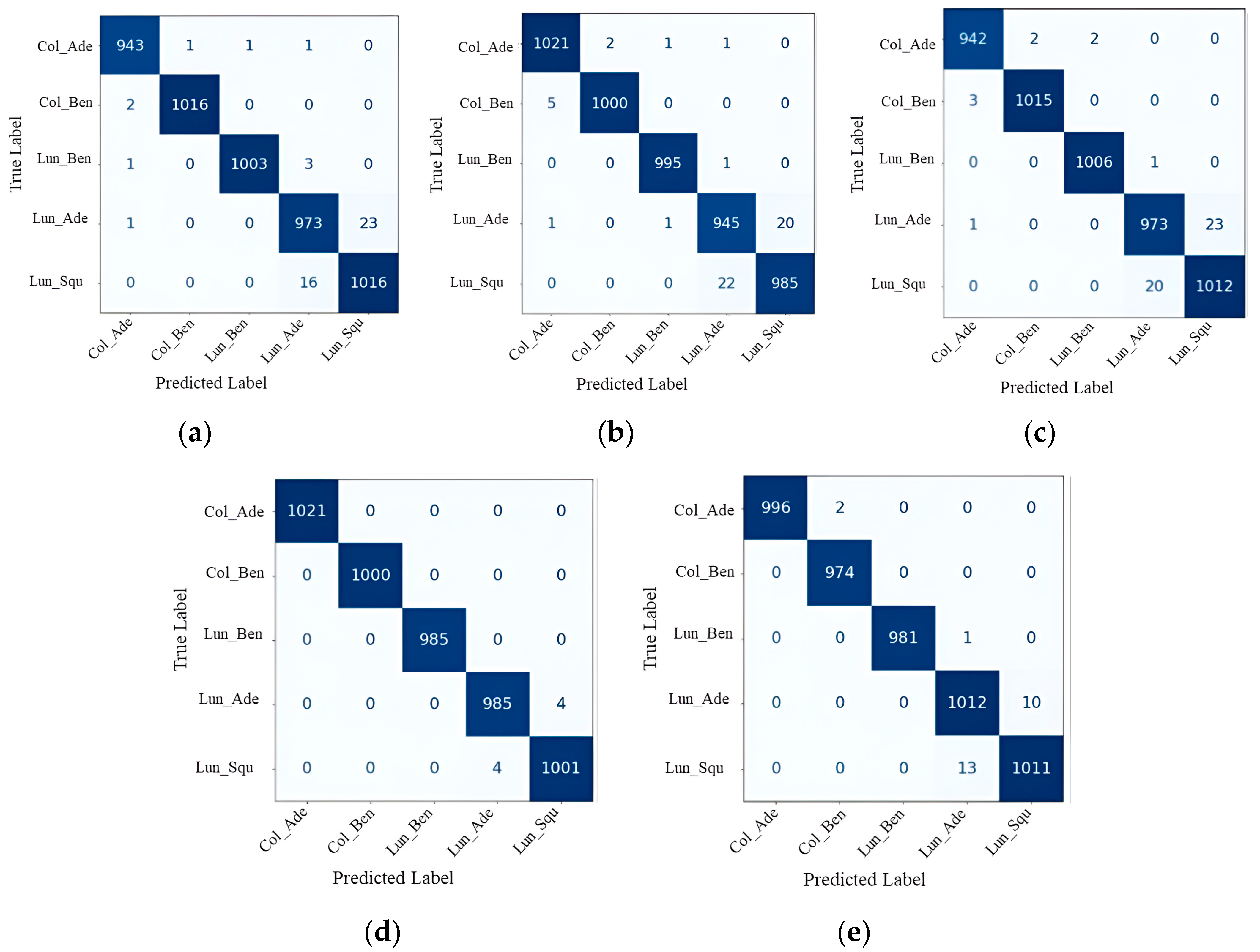
The confusion matrix is a technique for assessing how well ML categorization works. The terms TP (true positive) and TN (true negative) accurately reflect expected positive values. TP represents a correctly predicted positive value, FP (false positive) represents a false positive value, and FN (false negative) represents a false negative value. They are highly helpful in determining the ROC curve, F1-score, accuracy, recall, and precision.
The most obvious performance statistic is accuracy, which is directly proportional to the number of properly predicted observations over the total number of observations [
40,
41].
Precision is defined as the proportion of accurately anticipated positive values to all positively predicted values. It is shown as follows:
Recall [
42] is defined as the ratio of all the actual values to the values that were positively predicted and successfully made. It is demonstrated as follows:
The harmonic mean of a classification problem’s precision and recall scores is known as the F1-score [
43]. The F1-score is shown as follows:
ROC curves are two-dimensional graphs that are used for evaluating and understanding classifier performance [
44]. Classifiers are graded and chosen according to particular user requirements, which are often associated with changeable error costs and accuracy expectations [
45,
46]. The sensitivity or specificity interchanges in a classifier for all possible classification thresholds are displayed in detail on the ROC graphs. The AUC measures the degree of distinction, whereas the ROC is a likelihood curve. It demonstrates a model’s ability to discriminate across various groups. Plotting the false positive rate on the
x-axis corresponds to the genuine positive rate on the
y-axis. An AUC near 1 suggests that the expected model performs well in terms of class label separability, whereas an AUC near 0 denotes a poorly anticipated model. Actually, the word “lousy” means that the effect is being reflected [
47]. It is a method for demonstrating the effectiveness of a classification [
48]. The best classifiers are those with greater ROC curves [
49].
Specificity is a metric that evaluates the ability of a model to correctly detect true negatives within each available class. The mathematical expression can be expressed as follows [
48].
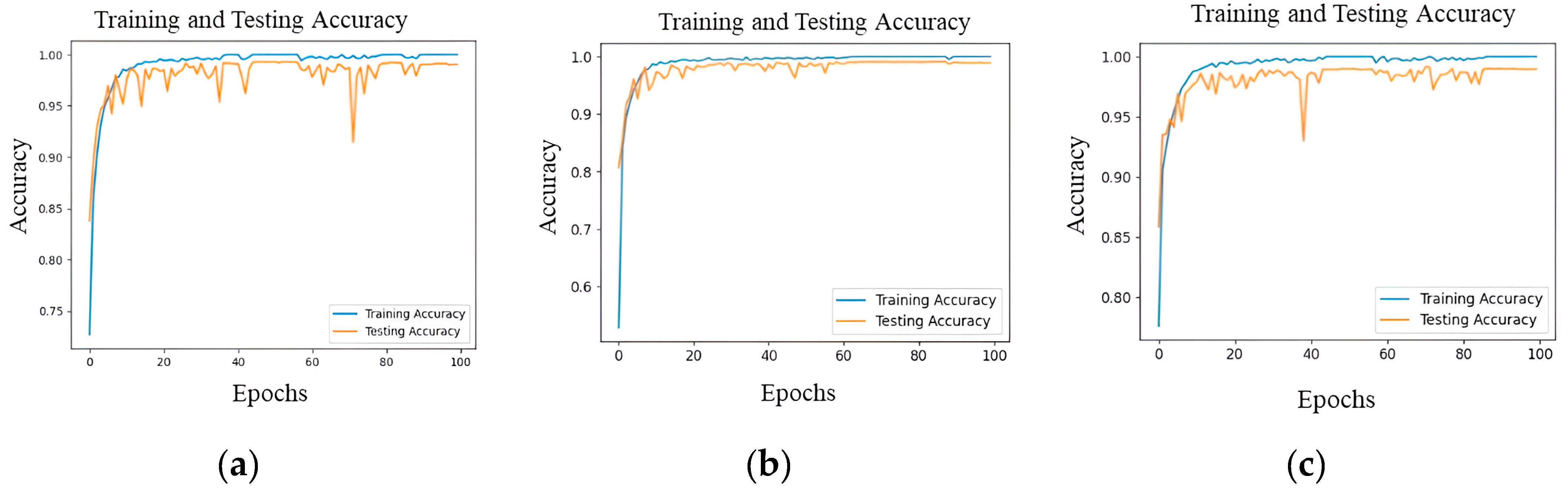
The XAI performance metrics include normalized root mean square error (nRMSE), which is a standardized form of the root mean square error (RMSE). The metric calculates the mean size of the discrepancies between projected and actual values, which is then adjusted based on the data’s range. It offers a standardized way to quantify errors, allowing for meaningful comparisons across diverse datasets. The structural similarity index (SSIM) is a perceptual model that takes into account brightness, contrast, and structure. The normalized index quantifies the degree of structural similarity between two images. The values go from −1 to 1, with a value of 1 denoting photo that are identical. The multi-scale structural similarity index (MS-SSIM) is an extension of SSIM that takes into account changes in image resolution by using multiple scales. It offers a more adaptable assessment of structural similarity by taking into account variations in image viewing conditions. Using the k-fold CV technique, k, smaller sets are created from a training set. The plan is to train a model on each of the k “folds” and then validate it using the remaining data. Using k-fold CV, the average of the values computed in the loop is then included as an evaluation metric. For LCC detection experiments, k-fold CV with a value of k = 5 has been used. Five distinct folds are created from the dataset, and each is used as a testing component while the dataset is being folded. The dataset is divided into 80% for training and the remaining 20% for testing in a k-fold.
4.3. Performance Evaluations
In this section, the performance of the proposed model on the LC25000 dataset is demonstrated. The performance is evaluated with different performance metrics as well as by using XAI like Grad-CAM and SHAP to evaluate the proposed model based on which portion of the image the decision is made on and what predicting the class is.
4.4. XAI Visualization
The applied explainable DL algorithm Grad-CAM, which is explained in previous sections, can be observed to retrieve the information after the final convolution and transform it into a heatmap. This map displays the regions in which the verdict was concentrated to reach its decision. This heatmap is superimposed on the original image to help the medical practitioner recognize the regions that affect the outcome. Before using the softmax technique (activating the class with the greatest value and inhibiting the others), the numerical result of the classifier is also taken from the system’s final layer.
The size of the original image is 180 × 180 pixels, whereas the resolution of the heatmap is 5 × 5 pixels (because of the final convolution layer before maximum pooling). As a result, the heatmap image needs to be over scaled before being overlaid on the original. This results in some portions of the heatmap not fitting completely with the original due to the decimals produced during this process of resolution improvement; nevertheless, when observing them, it is clear which parts of the image it refers to. When it comes to model prediction in
Figure 7, the red color on the maps denotes greater attention paid to those locations, while the blue color denotes that less attention was paid to those regions. Each image belongs to a different class, so the red color as well as the blue color heatmap in each image are situated in different positions of that image.
This not only aids in model interpretability but also empowers healthcare practitioners to make informed decisions with additional information based on XAI-assisted analysis. By providing visual justification for the model’s predictions, trust in the explainability and accuracy of the proposed model is the aim, ultimately facilitating its integration into clinical workflows for improved patient care.
Grad-CAM focuses on identifying the “class-discriminative” regions in the image, which are the areas that are most relevant to the predicted class. The visualization produced by Grad-CAM is specific to the model’s prediction for a particular class. The SHAP results for each group explanation are set against a clear gray background. Here, the Shapley value represents the contribution of that feature to the model’s prediction. SHAP provides a comprehensive explanation for individual predictions by quantifying the impact of each feature on the output.
In order for the model to determine the SHAP values for a particular set of instances, a SHAP explanation has to be first created. A customized SHAP partition explainer specifically made for deep learning models was made by using the SHAP—partition explainer function. For each instance in the dataset, the SHAP values show how much each pixel contributes to the model’s output. The SHAP data are arranged in matrices, where columns stand for features and rows for instances. The features that push the prediction towards the positive class are shown by positive values, and those that push towards the negative class are indicated by negative values.
Figure 8 shows an image plot of all five classes, generated by using the SHAP values. The plot shows the original image, with blue and red highlights in specific areas. Positive contributions to the class prediction are indicated by red areas, and negative contributions are indicated by blue areas. Blue zones reduce the likelihood of guessing a class, but red regions increase it. In
Figure 8, a lower SHAP value to the left indicates a lower prediction value, while a higher SHAP value to the right indicates a greater prediction value. It can be seen in
Figure 8 that for the Colon_Adenocarcinoma class, the prominence of red areas (positive SHAP values) in the plot signifies a tendency toward the prediction of the Colon_Adenocarcinoma class, indicating the correct prediction. In the second row, it has red pixels both in the Colon_Adenocarcinoma and the Colon_Bengin_Tissue classes, which is confusing. For Colon_Bengin_Tissue, all the pixels are red, whereas in Colon_Adenocarcinoma there are still some negative SHAP value. So, it is clear that the second row is Colon_Bengin_Tissue. The last row does not properly explain this, which is a limitation of the model.
Table 6 shows a full breakdown of how well the three explainability methods, Grad-CAM, and SHAP perform compared to a standard measure. The reference (Ref.) value column shows the optimal score for each parameter. This score is used to generate heatmaps that provide a clear and balanced representation of the data. It can be highlighted that a smaller value of nRMSE is preferable, and that higher values for SSIM and MS-SSIM indicate better similarity, with a value of 1 representing perfect similarity. Lower nRMSE values mean that the model is more accurate, and SHAP has the lowest number at 0.0678 ± 0.0245. Higher SSIM and MS-SSIM numbers indicate better structural similarity, and SHAP does very well in both, showing that it is good at capturing image features and is better than other methods.
4.5. Web Application
In the context of LCC detection, the interpretability of the DL model is crucial for both medical professionals and patients. Gradio provides an intuitive and interactive platform that allows users, including non-technical stakeholders in the medical field, to comprehend and trust the predictions of the model. Gradio’s user-friendly interfaces make it possible for oncologists, radiologists, and other healthcare professionals to interact with and understand the model without needing extensive technical expertise. Gradio simplifies the communication process between the model and the web interface. When a user interacts with the Gradio interface, the input data, the LCC image, are sent to the model. The model processes the input and generates predictions. Gradio receives the model’s output and updates the web interface to display the results in a user-friendly format, which here is in text format, showing the predicted class. Utilizing Gradio’s image input components allows for users to upload medical images for analysis, displaying the model’s output and indicating the predicted class or probabilities for different cancer types.
In
Figure 9, the web-application visualization can be seen, wherein the input images are classified correctly by the proposed model. So, in this way, from a user point of view, real-time prediction can be realized by the proposed model. The web application visualization demonstrates the accurate classification of input images by the proposed model, providing real-time predictions for different classes. Specifically:
- (a)
For colon adenocarcinomas, the proposed model correctly identifies and predicts this category.
- (b)
In the case of benign colon tissue, the proposed model accurately classifies the input images as such.
- (c)
Similarly, for benign lung tissue, the proposed model correctly predicts and categorizes the images.
- (d)
When it comes to lung adenocarcinomas, the proposed model reliably classifies the input images with precision.
- (e)
Finally, for lung squamous cell carcinoma, the proposed model consistently provides accurate real-time predictions.
This web application, aided by Gradio, showcases the effectiveness of the proposed model from the user’s perspective, ensuring reliable and precise predictions across various classes.
5. Discussion
To produce both quantitative as well as qualitative analyses, the suggested model was contrasted with other methods found in the literature.
Table 7 indicates how well the proposed method performed on the lung and colon disease datasets.
Hasan et al. [
3] have used custom CNN and PCA, and they achieved 99.80% accuracy for colon cancer only. XAI and end-to-end solutions were not used by the authors. On the other hand, this research paper provides the best solution for multi-class classification, provides an end-to-end pipeline solution, and uses explainable AI for visualization. Kumar et al. [
30] have used DenseNet121 for feature extraction and an RF ML classifier to predict the actual class techniques. Mehmood S. et al. [
50] have performed image enhancement and used AlexNet for training the data, achieving 98.40% accuracy. They used too many parameters. On the contrary, this research used 0.9 million parameters, which reduced the computational complexity. Masud M. et al. [
21] have used traditional ML classifiers and achieved 96.33% accuracy, which is relatively low compared to other SOTA methods, whereas 99.20% accuracy was achieved in this paper. Hatuwal B. K. et al. [
22] have also used a custom CNN, but it was only used for lung cancer. They achieved an accuracy of 97.20%. The hybrid ensemble learning technique was used by Talukder M. A. et al. [
1], and it achieved 99.30% accuracy. Bukhari et al. [
51] have used the pre-trained model ResNet50, which indicates that having more parameters also increases the computational complexity. The accuracy is also very low, at 93.13%. Balasundaram et al. [
38] have made AdenoCanNet and AdenoCanSVM. They achieved 99% accuracy. The above-mentioned methods require different algorithms to detect ROI, but the model in this research article can detect ROI with the help of XAI. In comparison to [
52], the proposed LW-MS CNN demonstrates superior efficiency with a parameter count of only 1.1 million, a substantial reduction from the 4.1 million parameters in the reference model. A model with fewer parameters requires less computational resources during training and inference. By incorporating convolutional layers with varying receptive field sizes, the model can capture both local and global features present in the input data. This multi-scale approach facilitates the detection of subtle abnormalities and distinctive characteristics across different scales, enhancing the model’s sensitivity and discriminative power. Consequently, the model can provide a more comprehensive representation of the underlying pathology, leading to improved accuracy in cancer detection. This is especially beneficial for scenarios with limited computational power, such as edge devices or mobile applications. Training a model with fewer parameters is generally faster than training a larger model. This allows for quicker experimentation, faster model iteration, and reduced training time. Models with fewer parameters are less prone to overfitting, especially when dealing with limited data. The reduced parameter count makes the proposed model more suitable for deployment in resource-constrained environments, where memory and computation resources are limited.
Table 7.
Comparison between the proposed model and other previous models.
Table 7.
Comparison between the proposed model and other previous models.
| References | Cancer Type | Methods | XAI | Accuracy | Precision | Recall | F1-Score |
|---|
| [34] | Lung and colon | Feature extraction | Yes | 95.60% | 95.8% | 96.00% | 95.90% |
| [21] | Lung and colon | CNN | No | 96.33% | 96.39% | 96.37% | 96.38% |
| [22] | Lung | CNN | No | 97.20% | 97.33% | 97.33% | 97.33% |
| [19] | Lung | CNN | No | 97.89% | - | - | - |
| [19] | Colon | CNN | No | 96.61% | - | - | - |
| [52] | Colon | CNN | No | 99.50% | 99.00% | 100% | 99.49% |
| [38] | Lung and colon | CNN | No | 99.00% | - | - | - |
| [53] | Colon | CNN | No | 99.21% | 99.18% | 98.23% | 98.70% |
| [53] | Lung | CNN | No | 98.30% | 97.84% | 98.16% | 97.99% |
| Proposed | Lung and colon | LW-MS-CCN | Yes | 99.20% | 99.16% | 99.36% | 99.16% |
The achievements and limitations of the proposed model can be highlighted as follows:
The proposed model achieved an accuracy of 99.20% for the overall LCC class classification (five classes), indicating that it can detect LCC with greater accuracy than similar DL models.
The suggested model is more appropriate for real-time applications, such as mobile or Internet of Medical Things (IoMT) devices, because it has fewer computationally expensive parameters (1.1 million) compared to existing DL models.
The multi-scale aspect of the proposed model plays a pivotal role in extracting features at different hierarchical levels, thereby enriching its ability to discern intricate patterns inherent in LCC images.
When compared to existing DL models, the suggested model is an end-to-end model since it can complete feature extraction and classification in a single pipeline. This reduces the system’s complexity.
The CV technique was employed to train and evaluate the suggested model, with the aim of reducing overfitting and enhancing the model’s generalizability by applying it to three combinations of the LC25000 dataset.
The integration of XAI algorithms, such as Grad-CAM and SHAP, enhances the model’s interpretability by providing diverse and complementary insights into feature importance, enabling a more comprehensive understanding of the model’s decision-making process.
Limitations:
- ▪
The proposed model has undergone testing on an LCC dataset using cross-validation methods. However, it has not yet undergone complete validation for application in real clinical scenarios. Additional clinical trials are necessary to validate the reliability and precision of the model in real-life scenarios.
- ▪
Despite the advancements in DL, the diagnosis of LCC still poses a difficult problem that requires a careful assessment of several parameters, such as the disease’s location, shape, size, and the improvements observed following contrast enhancement. The suggested model may not comprehensively consider all of these parameters, suggesting a requirement for more enhancements to improve its accuracy in identifying LCC.
- ▪
Future work will focus on enhancing the model to minimize the margin of error in XAI.
In the realm of medical image analysis, the LW-MS CNN presents several advantages worthy of discussion. Firstly, its ability to efficiently process and analyze medical images while maintaining a relatively low computational footprint makes it highly suitable for real-time applications, offering timely diagnoses critical for patient care. Additionally, the incorporation of multi-scale features enables the model to capture intricate details across various levels of granularity, enhancing its sensitivity to the subtle abnormalities characteristic of LCC. This multi-scale architecture facilitates a more holistic understanding of the pathology present in the images, thereby potentially improving diagnostic accuracy. Moreover, the lightweight design of the model, with a modest parameter count of 1.1 million, not only ensures rapid inference but also makes it more accessible for deployment on resource-constrained environments, such as edge devices or low-power computing platforms. These combined attributes render the lightweight multi-scale CNN an attractive solution for addressing the pressing need for early and accurate cancer detection, ultimately contributing to improved patient outcomes and healthcare delivery. Finally, the suggested approach has the potential to increase the effectiveness and precision of LCC identification, particularly in real-world applications where computational power and speed are crucial considerations as well as to analyze the region of interest areas.
6. Conclusions
A novel end-to-end DL-based lung and colon detection model that is interpretable is proposed in this research. The proposed model demonstrates a high degree of accuracy in identifying the most prevalent types of cancer in the five-class classification of both LCC subtypes. The LW-MS CNN design of the suggested model, with 1.1 million trainable parameters, enables real-time applications, cutting down on processing time and boosting system effectiveness. The proposed model has less trainable parameters than other SOTA models, which indicates that the training and testing time are also less than in other SOTA models. Additionally, the CV strategy was utilized to address the overfitting issue and guarantee the generalizability of the model, providing an accuracy of 99.20% for the classification of LCC. Medical practitioners can use an inventive end-to-end application that was created to make use of the proposed model, which will provide precise forecasts and support decision making. As a result, the proposed model’s capability to identify the type of LCC rapidly and accurately can help neurosurgeons and medical professionals make fast and correct clinical decisions about patients with LCC. In this study, interpretability approaches including Grad-CAM, and SHAP improve the understandability, dependability, and adaptability of lightweight CNN models to increase their efficacy. These methods assist users, developers, and data scientists in understanding model behavior, resolving problems, and improving the models’ effectiveness and fairness.
However, more research is required to properly comprehend the potential and limitations of DL in LCC detection in the IoMT and to overcome the challenges of practical application. To prevent overfitting or incorrect diagnosis, it is crucial to utilize strong and proven DL models that have been trained on substantial and varied datasets. To ensure the generalizability of the model, it is also crucial to consider potential biases in the training data and to apply methods like CV. The proposed model can be used in clinics for the automated diagnosis of LCC. The model could have improved performance with more advanced image pre-processing and dataset segmentation, even though the architecture provides greater accuracy. Additionally, segmentation techniques improve performance results, and the region of interest of segmentation methods can be compared with the use of interpretability methods. The datasets on LCC that were recently made public will be investigated in the future to conduct an ablation study of the suggested model, aiming to demonstrate its reliability. In further study endeavors, it is important to contemplate the inclusion of comparisons with vision transformers to provide a more thorough perspective on the progressions within this domain.






 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}










