1. Introduction
Since its inception in the early 20th century, the air transport sector has undergone a historical evolution in response to the economic, political, and social circumstances of the time. Originally a prohibitively expensive enterprise with a primary focus on military operations, the aviation industry has transformed into the ubiquitous and popular activity we recognize today, albeit with numerous boom-and-bust cycles. However, significant global events such as wars, economic crises, epidemics, or terrorist attacks have had substantial impacts on the aviation sector [
1]. At the beginning of 2020, the world was struck by the outbreak of the COVID-19 pandemic, the greatest challenge the aviation industry has ever faced, “making previous shocks such as the 1979 oil-price crisis, the Gulf War, 9/11, and the Global Financial Crisis look like minor incidents in comparison” [
2]. The ensuing global health crisis had devastating consequences for numerous industries and sectors, with the air transport industry arguably being one of the hardest hit, primarily due to the significant decline in travel demand [
3].
Confronted with an alarming surge in positive cases and the challenges of containment, governments worldwide implemented quarantines and travel restrictions, resulting in a severe disruption to commercial aviation due to a lack of passengers. According to both [
3,
4], global air traffic experienced a decline of nearly 70% in 2020 compared to the previous year, with a 98% reduction in international flights during the initial months of the pandemic.
Looking back, there are legitimate doubts regarding the optimal management of the situation, particularly during the initial months following the declaration of the pandemic. The aviation industry learned that relying solely on air traffic restriction policies as the primary driver of pandemic control—without methodologies or tools that enable decision-making based on data and models—was one of the main factors responsible for the worldwide halt in economic activity.
Now, four years have passed since the initial outbreak of COVID-19, and for most individuals, it seems to have become a thing of the past. However, this does not imply that the scientific community, as well as society at large, should dismiss the necessity of preparedness in the event of similar situations arising in the future. According to [
5], the impacts of climate change are projected to lead to the emergence of numerous new viruses among animal species by 2070.
Our aim in this paper is to demonstrate that traveling within the cabin of a commercial aircraft carries an acceptable level of risk, particularly when passengers are required to provide a negative PCR test prior to boarding and/or when they are vaccinated or adhere to mask usage policy, among other mitigation measures.
For this purpose, we build an air transport network (ATN) that represents the global airport system, with nodes corresponding to airports and links denoting routes. The network incorporates data from publicly available sources regarding the number of infected individuals and the number of flights and travelers. Using that information, we devise a Bayesian probabilistic model that assesses the likelihood of infection within the aircraft cabin, taking into account multiple factors such as the incidence rate in the origin region or the flight duration. We also evaluate the transmission of infectious diseases within the ATN, allowing us to estimate the imported risks associated with a given network airport or route.
We applied our methodology to the European ATN, analyzing the impact of infectious diseases originating from other regions of the world on major European hubs. We modeled the network performance using discrete event simulation (DES) [
6], a powerful computational framework that facilitates the modeling of individual events and their effects on the system, step-by-step over time.
This approach enables us to simulate the spread of a virus or its variants across Europe, allowing us to make predictions such as estimating the arrival time of a specific variant in a country after the first cases are detected in another region of the world. Additionally, our model would help decision-makers in the eventual implementation of preventive measures designed to safeguard the various affected regions while adhering to the safety regulations set forth by local authorities. The effectiveness of such measures are evaluated by analyzing their potential impact on curbing the spread of the infectious disease.
The paper is structured as follows.
Section 2 provides an overview of ATNs. In
Section 3, we present the Bayesian probabilistic model, which we use to forecast the expected number of infected passengers arriving at a specific airport.
Section 4 analyzes the transmission of infectious diseases throughout the ATN. In
Section 5, we apply our methodology to a real-case study of various significant European airport hubs, illustrating our approach. Finally, we conclude with a discussion.
2. Characterizing the Air Transport Network
ATNs are an example of transport and spatial networks [
7] that play a vital role in connecting people, goods, and ideas across the globe. ATNs are characterized by intricate interactions between airports, flights, and passengers. Traditional static network models fail to capture the time-dependent nature of these systems, limiting their ability to provide accurate representations of real-world scenarios. Therefore, we adopt in our work a dynamic network modeling approach that accounts for temporal changes and events occurring within the ATN. Figure 1 in [
8] presents an example of a dynamic network, built from data corresponding to commercial flights between European airports on a given day.
In a dynamic network, airports represent nodes whose features may evolve over time, and routes act as the edges connecting them. Each flight occurrence along a given route is a discrete event, creating a network structure that adapts to real-time changes, such as weather disruptions, flight delays, or passenger behavior. Such adaptability allows us to simulate various scenarios and explore how the network would respond to different contingencies. Specifically, we are interested in studying the spread of infectious diseases within the ATN and assess potential mitigation strategies that could minimize their impact.
In particular, we consider a scenario where an infectious disease first appears in a specific (origin) geographical area, denoted as . We aim to investigate how this new virus/variant could spread to a sufficiently distant (destination) area . We use and to refer to the sets of airports lying in the geographical areas and , respectively. Within the latter, we are particularly interested in assessing the impact of the infectious disease on a subset of target airports , which could be of particular relevance to local or national authorities or stakeholders.
For practical purposes, in our study, we only consider those routes that connect one airport in with one airport in within the same day after, at most, two stopovers. To that end, we define as the sets of airports corresponding to the first or second stopover, respectively. Once the set of suitable routes (potentially carrying infected passengers to the target airports) has been identified, we are further interested in determining which routes or intermediate airports could pose higher risks as potential vectors for the transmission of the infectious disease.
To address these issues, and given that the sequence of arrivals and departures at different airports in the network constitutes a discrete series of events over time, it is natural to employ DES as our fundamental modeling tool. Every event is scheduled to occur at a specific time, and once it transpires, the system’s status is updated accordingly. The system remains idle between successive events, enabling us to proceed directly to the scheduled time of the subsequent event. By simulating the impact of each event on the network, we can scrutinize the system’s behavior over time, discern emerging patterns, and conduct sensitivity analyses.
The network model, along with its underlying DES mechanism, is implemented using
R [
9]. This enables us to adeptly represent different epidemiological scenarios by adjusting the relevant parameters, eventually incorporating new input data as they arrive. Once our network model is trained and refined, it will empower us to forecast the progression and potential dissemination of epidemic outbreaks, akin to the global experiences of early 2020.
4. Estimating Imported Risks Using DES
Once we have specified probability models for the number of infected passengers at departure and arrival, we now use them to assess the propagation of such infectious disease across an ATN during a given time period.
For each day considered in our study, we monitor inbound flights departing from an airport that arrive at an airport between 00:00 h and 23:59 h coordinated universal time (UCT) of the current day and that will eventually connect to one of the target airports after a maximum of two stopovers. We aim to evaluate the influx of infected passengers arriving at the target airports by the end of any given day.
In
Section 3.1, we introduced the incidence rate
, which refers to the newly diagnosed cases of an infectious disease occurring or being recorded in the catchment area of the origin airport
i over a specified period of time. Incidence has an impact on the airsides of the different airports that form the network nodes, influencing the number of infected passengers
boarding flight
k, as described by (
1) and (
2). In
Section 3.2, we also defined the flight’s final epidemiological status,
, for which we provided a sampling procedure in (
8).
For each connection, we assume now that a proportion
of the arriving passengers (either infected or non-infected) leave the terminal, while the remaining passengers make a connection to another airport in the network. We model
as a beta random variable with mean
and precision
. Based on expert opinion and the available data, we assess
and a relatively high precision
. Based on that, we define the
individual imported risk
as the number of infected passengers who stay in the catchment area. Similarly, we define the
individual exported risk
as the number of infected passengers who make a connection to another flight. Another relevant quantity, which we need later on, is
representing the number of non-infected passengers who make a connection to another flight.
To determine the daily imported risk for each airport i in the ATN, we simply add the individual imported risks of all the flights arriving at that airport on the incumbent day. By assessing , we are able to compare its relative contribution to the current incidence at the corresponding catchment area.
Once we have defined the relevant quantities, we initialize our ATN from a suitable “starting point”, considering that the infectious disease is only present in those airports where the virus/variant originated. Therefore, we can assume that the initial incidence of the catchment areas around the destination airports is zero. In this hypothetical “absolute first flight” scenario, passengers coming from the catchment area of any airport would not have been affected by imported risks from other airports yet.
One further assumption of our model is that an incoming flight only impacts the airside of the destination airport in the first three hours after its arrival time. From a purely theoretical standpoint, the effect of an arriving flight, in terms of potentially spreading an infectious disease through the ATN, could extend for much longer than that. However, for the purpose of our model, we must set an upper bound on the maximum time a flight can affect the airport airside after arrival, and we believe three hours is a well-grounded choice. After that period, we assume that all passengers will have either left the airport or connected to another flight departing within one to three hours of their arrival time (We set one hour as the minimum time needed to make a connection in an international airport). As for the possible destinations when connecting to another flight, we explicitly rule out the possibility of flying back to the origin airport for domestic flights (and, additionally, back to the country of origin for international flights) since such connections would be highly unlikely.
As mentioned in
Section 2, we model the ATN performance using DES, which assumes that the system remains idle unless a new arrival or a new departure occurs. We keep track of those flights that are part of a suitable route connecting one of the origin airports
to one of the target airports
. We assume that the probability of two events (departure and/or arrival) occurring at the exact same time is zero. If, due to the time discretization (in minutes), two or more events are assigned the same timestamp in the database, we sort them in an arbitrary manner.
We now specify the main events we must consider in our simulation for a given day. For all the events in our database, we sort their departure and arrival times (in UTC) and address them in chronological order.
Algorithm 1 outlines the pseudocode we use in our simulations. Given that we are examining those routes
that connect one airport in
with one airport in
within the same day after, at most, two stopovers, this entails approximately
operations, where n represents the number of airports within the ATN.
| Algorithm 1: DES for the ATN performance |
| Data: Flights connecting airports in and plus internal connections in |
| Result: Daily imported risk at the network nodes’ airsides |
| Initialization: |
| for all flights in the database do |
| | if departure then |
| | | if flights arrived between 1 and 3 h before then |
| | | | Fill partially aircraft with passengers connecting from other flights |
| | | | Fill rest of aircraft from catchment area |
| | | else |
| | | | Fill aircraft from catchment area |
| | else |
| | | if arrival not final event then |
| | | | Prop. of passengers leave airport, of which are infected |
| | | | The rest ( and ) connect with other flights |
| | | else |
| | | | 100% passengers leave airport, of which are infected |
| | | Update |
5. The Impact of the Indian Outbreak in Europe
Our case study aims to investigate the spread of infectious diseases across the European ATN under various hypothetical scenarios. Given its undeniable impact in the recent past, and the fact that it still remains a global threat, we focus our analysis on the transmission of the Delta variant of COVID-19, a particularly contagious strain that originated in India around March 2021 [
44], a year and a half after the global pandemic sprang up in Wuhan, China, From that date, Indian authorities began reporting a highly aggressive outbreak in several regions across the country. According to data from the Johns Hopkins Coronavirus Resource Center
https://coronavirus.jhu.edu/map.html (accessed on 28 February 2024), the epidemic reached its peak on 6 May 2021, reporting a total of 414,000 new cases. This incident sparked international tension, as many countries feared a swift increase in the number of infected and deceased individuals. Given that air travel is the fastest mode of transportation, capable of quickly moving large numbers of passengers from India to other parts of the world in just a few hours, such an outbreak led to renewed restrictions on air travel worldwide, similar to those imposed during the initial months of the pandemic.
Our focus is on analyzing the extent to which the ATN may have facilitated the spread of the Delta variant to different European countries through their airport connections with India. By comparing our results with actual data recorded by European health authorities, we are confident that our network propagation model could adequately predict the effects of similar events in the future, thereby enabling governments to implement appropriate mitigation measures in advance. Considering our aim is to assess the impact of the new Delta variant in India, distinguishing its effects from other potential sources of infection, we regard the remaining incidences in Europe as negligible. This approach allows us to track the spread of the disease as if it originated exclusively from passengers boarding at Indian airports and traveling to Europe.
To achieve this, we simulate the propagation of such a variant across European soil, aiming to reproduce “when the Delta variant is first detected” in each European city after its appearance in India. Specifically, we are interested in assessing the impact of the Delta variant on the two main Spanish airports: Adolfo Suárez Madrid-Barajas (MAD) and Josep Tarradellas Barcelona-El Prat (BCN). These airports faced significant criticism during the first stages of the pandemic due to the controversial measures implemented around them, which potentially facilitated the entry of new virus strains or sizable groups of infected individuals. Once we have captured the propagation dynamics with our model, addressing both imported and onboard cases, we are able to identify the ‘hotspots’ (either airports or routes) in the ATN that affect MAD/BCN the most. This enables us to incorporate mitigation measures—such as reducing occupancy in aircraft or conducting PCR tests—based on the extent of the variant spread and document strategies for containing it, by intervening at the riskiest airports/routes.
For this purpose, we have access to a publicly available database from Eurocontrol
https://www.eurocontrol.int/ (accessed on 28 February 2024), comprising over 340,000 operations conducted between 1 March and 30 April 2021. These operations include direct flights originating in India and landing at European airports, along with all intra-European connections. We selected the period between March and April 2021 because it was during this time that the first reports about the new Delta variant in India emerged. We also gather disease information about cumulative incidences within the catchment areas associated with the considered airports in India from the Johns Hopkins database. These datasets serve as inputs for the probability and simulation models detailed in
Section 3 and
Section 4, respectively, facilitating the computation of the daily imported risks
.
The information contained in the flight database included the origin and destination airports, departure and arrival dates and times, and the aircraft capacity. Departure and arrival times were recorded in local times, as is standard practice. Therefore, to calculate flight duration, we needed to convert these local times into UTC. This necessitated augmenting the database with additional pertinent geographical details about the origin and destination countries, locations, and most importantly, time zones.
Managing local and UTC times, together with time zones, is not a trivial task, especially considering that the period analyzed included the forward daylight-savings time in many European countries, during the night of 27 to 28 March 2021. Despite our careful efforts in handling departure and arrival times, we encountered errors and inconsistencies in several routes—primarily involving operations to/from Turkey, Russia, and Ukraine—that could not be rectified and were, therefore, removed from the database.
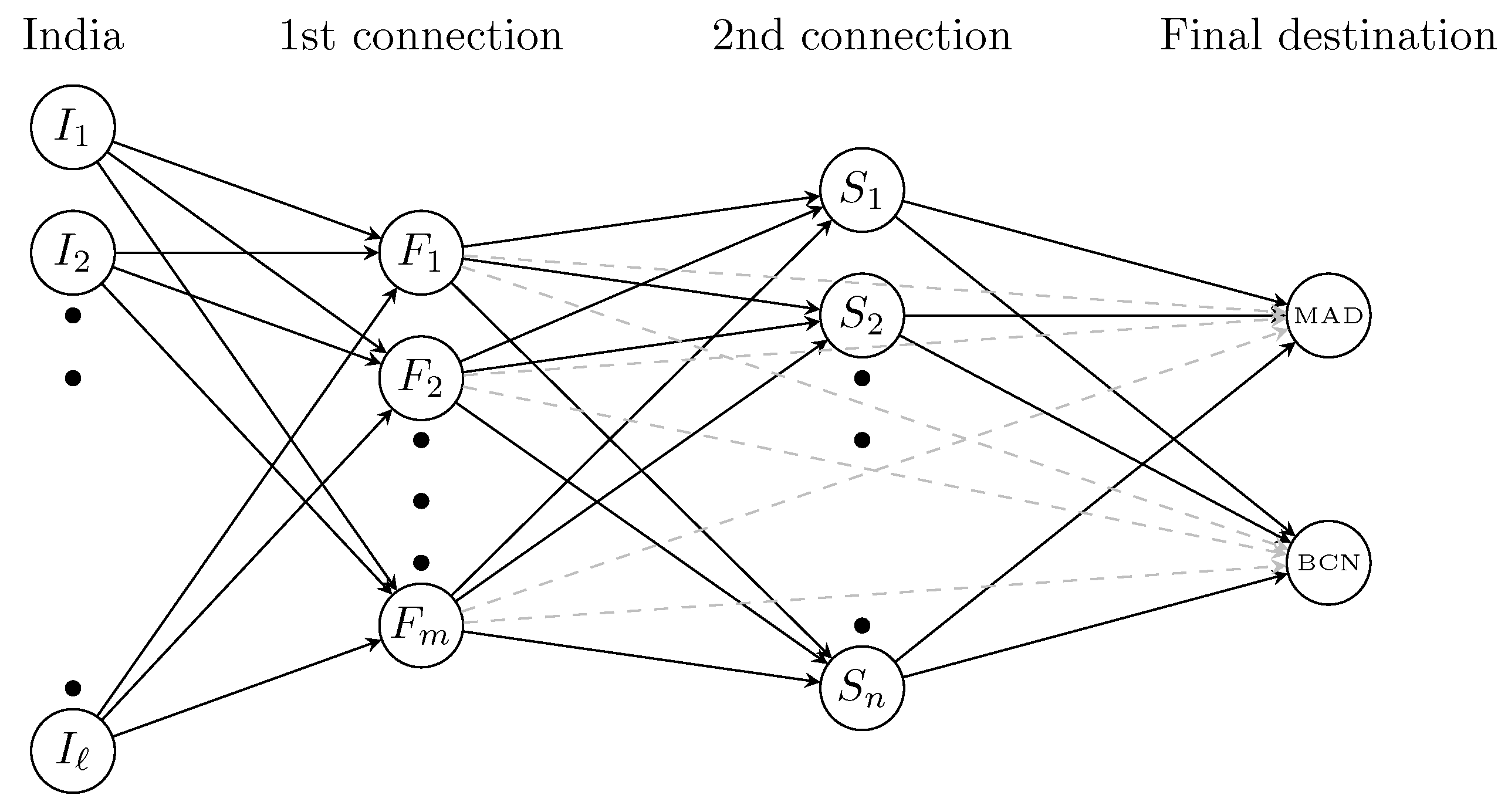
Once the database was sanitized, we were interested in monitoring flights originally coming from India and arriving at MAD or BCN after one or two connections on European soil, as illustrated in
Figure 4. As mentioned in
Section 4, we assume that for each of these connections, the time difference between arrival and departure must fall within one to three hours. Subsequently, for each day within the March–April 2021 period, we identify flights directly connecting an Indian airport
to a European destination
. These “seed flights”
–
are the origin for disease spread across the European network. We then monitor each of these seed flights, selecting only those that eventually lead to MAD or BCN, either directly or after a second stopover at another European airport
. We refer to these sequences of flights
or
as the set of suitable routes
.
In total, there were 665 flights in our database directly connecting a total of 10 Indian airports to another 11 European airports, as illustrated in
Table 1 and
Table 2.
Regarding the incidence database, we have access to data on the 7-day cumulative incidence in India from 1 March to 30 April 2021. These data allow us to estimate the expected number of infected passengers boarding each flight departing from the airports listed in
Table 1 using (
1). Then, employing our propagation model (
8), we can estimate the expected number of infected passengers upon the landing of these flights in European territory, assuming zero cumulative incidence of the Delta variant in all European countries on 1 March 2021.
Next, we consider all suitable routes
. For instance, for the first day in the database, 1 March 2021, a total of 8 direct flights departed from India to a European destination, and a further 140 intra-European flights served as 1- or 2-connection routes to MAD or BCN, where 13 and 3 flights arrived throughout the day, respectively, see
Figure 5. At the end of each day, we calculate the total expected number of infected passengers arriving in either MAD or BCN. This provides us with a rolling estimation of the evolution of the cumulative incidence between 1 March and 30 April 2021 that could help health authorities in their decision-making.
In a subsequent stage, we will analyze on which airports or routes might be advisable to establish control access considering their COVID-19 impact and potential passenger losses. We will also evaluate the effectiveness of several mitigation measures.
In a subsequent stage, we will analyze which airports or routes might be advisable to restrict, considering their impact from COVID-19 and potential passenger losses. Additionally, we will evaluate the effectiveness of certain mitigation measures.
5.1. Simulations of the Baseline Scenario
We run our simulations for the period spanning from 1 March to 30 April 2021 when all suitable routes in
are considered. We replicate our experiment
times to account for inherent uncertainty. Executing our algorithm took several minutes on a standard laptop running Windows.
Figure 6 shows the cumulative number of infected people who arrived at MAD/BCN airport after the 2-month period. As we can observe, there is a significant—and increasing, as days pass by—variance around the expected value, reflecting the great volatility of this scenario. As we can see, the initial infections are anticipated to reach MAD/BCN approximately one week after the first flights carrying infected passengers departed from India. This aligns with the information published regarding the detection of the first cases of the Delta variant in those cities.
The previous calculation only accounts for imported cases at MAD or BCN airports. However, to assess the true impact of the spread of the Delta variant in the catchment areas of both airports, we should also consider community transmission. Although a detailed estimation of such a phenomenon is beyond the scope of this paper, we use a straightforward propagation mechanism in which the number of infected people in a given catchment area increases by 5% from one day to the next. While we are well aware that this is a very rudimentary and unrealistic model for high numbers of infections and/or when applied over many consecutive days, it works reasonably well for our data. If we consider the augmented cases, where infected passengers arriving at MAD/BCN could potentially infect other inhabitants within the corresponding catchment area, the total number of infected people could potentially get out of control, as shown in
Figure 7.
5.2. Influence of High Occupancy
Our database contains information about the aircraft capacity. However, we lack details about the number of seats occupied. In the baseline scenario, and based on expert opinion, we assume an occupancy rate of 80–85% and apply a rule of thumb to determine the aircraft capacity and distribution: (i) two rows of two seats each (2-2) for capacities smaller than 100; (ii) 3-3 for capacities between 100 and 220; (iii) 3-3-3 for capacities between 220 and 300; and (iv) 3-4-3 for capacities bigger than 300.
We aim to compare the disease impact when authorities implement a policy where 1 out of 2 seats is required to remain empty in small aircraft (with capacities less than 100), and 1 out of 3 seats in larger aircraft. To achieve this, we rerun our simulations, reducing the number of passengers to half (two-thirds) of their actual value in the database for short- (long-) haul flights. We then distribute them according to the corresponding safety rules related to interpersonal distance. Focusing on the last day of the two-month period, the results obtained show an average reduction of 18% and 25% in the cumulative number of infected passengers compared to the baseline scenario in MAD and BCN, respectively. Such accomplishment brings to light the potential benefits of implementing a middle-row-empty policy in aircraft during a pandemic, particularly in terms of a reduced risk of infection. This is crucial for the airlines and their public image. By proving that flying with empty middle seats is no more dangerous than other day-to-day activities, airlines may gain public trust and encourage more people to fly even during uncertain times. Furthermore, implementing such policies contributes to overall efforts in managing pandemics and protecting public health.
5.3. Closing Airports/Routes
We aim to assess the impact of restricting access to the ATN for infected passengers from areas with a high incidence. Our goal is to evaluate the relative impact of each European airport/route on the spread of the delta variant. This allows us to observe how certain airports/routes contribute more significantly to its transmission, possibly due to a higher number of connections or more frequent flights, among other secondary factors. The most efficient way to implement such a policy would be by conducting PCR tests prior to boarding and denying access to those who test positive. While other measures such as masks and vaccines could be investigated (see
Section 3.2), for brevity reasons, we limit our study to the realization of PCR tests. For the purpose of our analysis—which is to provide a rough estimate of the benefit of implementing such a restrictive measure—we assume 100% effectiveness of the PCR test. With this configuration, we will rerun our simulations, setting to zero the values
in (
1) and
in (
18) for airports that are either identified as high-risk themselves or are part of a high-risk route.
We now identify those airports/routes with the most infected passengers in the previous simulation in
Section 5.1. Apart from MAD and BCN, the airports receiving the largest numbers of infected passengers during the 2-month period are displayed in
Figure 8, where we show boxplots for the different airports, ordered in decreasing order of their mean value (indicated with a black circle). As we can observe, some of the most important European airports act as major distribution centers in the sense that they receive/send significant numbers of infected passengers from/to other airports in the network.
As for the routes,
Figure 9 presents boxplots for those routes transporting the highest number of infected passengers at the end of the 2-month period. The boxplots are ordered in descending order of their mean value. As we can observe, route ARN-BCN stands out as the one with the highest traffic of infected passengers. Several other routes arriving at MAD or BCN serve also as conveying vectors on the propagation of the virus. As is already apparent from
Figure 8, most routes have one of the main European hubs as their origin or destination.
We now analyze the impact of restricting access to certain airports or routes for passengers testing positive. Specifically, we compare the total number of infected passengers arriving at MAD/BCN by the end of the period from 1 March to 30 April 2021, with the results obtained in the baseline situation analyzed in
Section 5.1.
For instance, let us assume that the Spanish authorities have decided to restrict flights departing from the five airports posing the highest risk of importing infected passengers: FRA, LHR, CDG, AMS, and FCO. The expected impact of banning flights from those airports results in a notable reduction of approximately 37% and 43% in the expected numbers of infected individuals arriving at MAD or BCN, respectively. With this measure, the impact of a country’s high incidence could be mitigated while allowing the free movement of non-infected passengers from that country. However, we still need to address the uncertainty that some passengers making a connection may not have been asked for a PCR test at the origin airport.
Similarly, the Spanish authorities could consider banning certain routes because they are known to be particularly hazardous in terms of their contagious potential. The number of infected individuals arriving in a country can be influenced by various factors. Thus, it is important to acknowledge that a higher count of infected individuals might not solely stem from epidemiological concerns but could also be associated with an extensive network of connections between destinations. Hence, we calculate the average number of infected passengers for all flights along a specific route. This approach provides a more accurate assessment of the most potentially hazardous routes, irrespective of the volume of flights on that particular route. This approach would provide decision-makers with more targeted options, aiming to disrupt air traffic as minimally as possible.
Figure 9 highlights that ARN-BCN stands out as a particularly risky route, even though ARN airport does not appear in the top-ten list of dangerous airports. This situation may arise due to a particularly intricate network of connections between major European hubs and BCN airport, with ARN airport serving as an intermediate stopover. Restricting access to the ARN-BCN route for passengers testing positive prior to boarding would result in a reduction of 5% and 7% in the expected numbers of infected individuals arriving at MAD and BCN, respectively. These results emphasize the importance of considering specific routes in addition to individual airports when implementing preventive measures. If each European country were to adopt similar measures, a dynamic network would be created. This network would remain operational but with a controlled percentage of routes. Thanks to these targeted interventions upon arrival, the overall ATN would be significantly safer while still operational.
5.4. Limitations of Our Model
Some data related to the virus’ virulence or mortality could be only gathered after the outbreak of a certain viral disease. Furthermore, it is typically not easy to access these data, which may limit the implication of the findings. It is also important to note that due to inadequate reporting, reporting delays, or limitations in the accuracy of data collection, any available data may only offer indicative insights, consequently impacting the forecasts obtained. Currently, our model lacks the ability to estimate the potential inaccuracies in the forecasts.
As we have mentioned throughout our paper, there might be instances where the data are unavailable for any of the proposed inference methods. Should that be the case, expert judgment could be used to determine the appropriate parameter values. Expert elicitation is notoriously challenging and subject to inaccuracies, as well as cognitive and motivational biases [
11]. In cases where expert elicitation is used to determine certain parameter values, the resultant forecasts may be sensitive to any inaccuracies in these elicitation processes.
While it is true that inaccuracies in data and expert elicitation can impact the accuracy of forecasts, the Bayesian approach we have opted for provides two crucial avenues to tackle this issue. First, as additional information regarding a new outbreak of a virus/variant becomes available, we can readily integrate this into our model, enabling updated results and enhanced decision-making. Second, the established state-of-the-art methodologies for examining the sensitivity of the model forecasts to inaccuracies in both prior elicitation and data uncertainty can be employed to gauge the potential variation in forecasts. We briefly discuss this in
Section 6.
Finally, although our study has been conducted retrospectively, we could also feed our algorithm with the new incidence data emerging daily to ‘simulate’ what is expected to happen in the next days and draw valuable conclusions that could eventually help decision-makers in their tasks.
6. Conclusions and Future Work
The impact of a pandemic extends beyond mere medical consequences and significantly affects various economic aspects, including the commercial aviation sector. Therefore, it is crucial to identify the epicenters of disease spread within ATNs to enable effective control measures, rather than relying solely on industry-wide shutdowns as the primary solution.
The European airspace is not uniform, as not all connections and destinations carry equal weight in passenger transportation. Even if a route is significant in terms of its impact, decision-making can be swayed by its effect on the destination’s epidemiological situation. Our interest was to explore the influence of individual routes and airports on potential disease transmission on a real crisis scenario.
In this paper, we enhance the understanding of ATNs by leveraging dynamic network modeling and discrete event simulation, identifying critical factors that affect network performance and implementable strategies to improve overall efficiency and safety. Using Bayesian methodology enables probabilistic forecasts of the number of passengers who may be infected during commercial flights. Using a stochastic approach that is validated using empirical data, we are able to account for the various sources of uncertainty. Thus, our work contributes to public health efforts by assessing the transmission risk of infectious diseases during air travel and supporting decision-making for pandemic preparedness. Through our innovative approach, we hope to pave the way for a more resilient and adaptive air transport system.
We first simulated the ATN performance in the baseline scenario without any mitigation measures. Then, we considered two alternative scenarios, reducing the aircraft occupancy or restricting access to those passengers testing positive on a PCR test. The results obtained demonstrate a significant reduction in the number of infected individuals moving through the ATN. Since these measures are neither expensive nor difficult to implement, they could be applied not only at the main hub airports but also, potentially, at every airport in the network. Our results show that by doing so, the risk of disease propagation could be minimized without restricting the people’s ability to travel to the same extent and duration that it was during the pandemic.
A sensitivity analysis was conducted on our model parameters, and it showed that the obtained results were not overly dependent on specific assumptions. However, it is inevitable that significant inaccuracies in expert elicitation could lead to inaccurate forecasts. The further research could consider performing a prior robustness analysis to quantify the effects that imprecisely defined prior distributions could have on the findings of our model. This analysis can be efficiently and relatively straightforwardly conducted using the distorted band class of priors [
45]. Recently, a novel approach using the ABC class of priors was proposed to explore the sensitivity of Bayesian posterior inference to data uncertainty [
46]. The further research could also investigate the applicability of the ABC class of priors to our model for analyzing the effects of data inaccuracy. This analysis can yield both the most optimistic and the most pessimistic forecasts, thereby enhancing the utility of our model.
The further research could also investigate risk assessment models that consider not only the spread of infectious diseases but also economic and operational risks. Such models should develop strategies to mitigate the impact of future pandemics on the aviation industry and explore adaptive risk management approaches that can be quickly implemented during crises to minimize losses.
Finally, our approach is ideally suited to be incorporated in methods such as the approximate Bayesian computation (ABC, [
47]), which enables a more accurate inference on parameters using the reported incidence data. Furthermore, this process can be implemented daily (if need be) to produce the most accurate inference using the latest data to ensure the most up-to-date and accurate forecasts possible.


 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}