
Current Status and Prospect of Diabetes Diagnosis and Treatment Based on Biosensing Technology


State Key Laboratory of Digital Medical Engineering, School of Biological Science and Medical Engineering, Southeast University, Nanjing 210096, China
*
Author to whom correspondence should be addressed.
Chemosensors 2023, 11(7), 391; https://doi.org/10.3390/chemosensors11070391
Submission received: 9 June 2023
/
Revised: 5 July 2023
/
Accepted: 11 July 2023
/
Published: 13 July 2023
(This article belongs to the Special Issue Bionic Recognition and Biosensors: A Theme Issue in Honor of Professor Hong-Yuan Chen)
Abstract
:Diabetes mellitus has increasingly become a threat to health all over the world. This review focuses on the promoting effect of biosensing technology on the diagnosis and treatment of diabetes mellitus. Types of diabetes and their corresponding pathogeneses are first introduced, followed by the diabetes prevalence and research progress at home and abroad. To emphasize the importance of diabetes diagnosis and treatment, we secondly summarize the breakthrough technology in this field based on biosensing technology at the present stage. In terms of diagnosis, diversified ways of blood glucose detection and multiple combinations of diabetes biomarkers are discussed, while a variety of insulin administration routes and non-drug treatment means are presented in the aspect of treatment. In conclusion, the prospect of the future development of diabetes diagnosis and treatment is put forward at the end of the review.
1. A General Overview of Diabetes Mellitus
1.1. Types and Pathogenesis of Diabetes Mellitus
Diabetes Mellitus (DM) is a chronic metabolic disease, manifesting as metabolic disorders of glucose, protein, lipid, and other substances within the body and persistent hyperglycemia externally. It is caused by the lack of insulin secretion and/or insulin resistance, which results from the combined effects of various factors.
Most DMs can be classified as type 1 diabetes mellitus (T1DM) and type 2 diabetes mellitus (T2DM). In addition, there are monogenic diabetes mellitus, secondary diabetes mellitus, gestational diabetes mellitus, and unresolved diabetes mellitus as a more refined distinction. The classification of T1DM and T2DM is based on classic characteristics of early understanding of DM, including the age of onset, degree of loss of β-cell function, degree of insulin resistance, presence of diabetes-related autoantibodies, and insulin therapy required for survival, etc. [1]. The World Health Organization has updated the classification standard of DM by issuing guidelines regularly since 1965. However, with the increasing prevalence of obesity in the young generation, the phenotypes of T1DM and T2DM are less obvious, on the basis of which more types of diabetes subtypes are produced [2]. The combined influence of multiple genes and factors has become a typical feature of contemporary DMs, which makes it difficult for people to understand the whole spectrum of diabetes phenotypes. Based on the classical diabetes model, only the known pathogenesis of classic T1DM and T2DM is elaborated here.
T1DM is a kind of organ-specific autoimmune disease, the pathogenesis of which is that the necrosis of pancreatic β cells in the autoimmune environment leads to the decrease in insulin secretion in the body, resulting in metabolic disorders. At present, T1DM accounts for about 5–10% of the total DM cases [3]. As early as 1974, the association between T1DM and genetic factors was discovered by scientists, showing a pattern of multi-gene inheritance. Further analyses conducted recently, locations of important, relevant alleles have been identified, and the mechanism of many cytokines directly related to T1DM has been successfully explored, such as interleukin-1 (IL-1), interferon-γ (IFN-γ), tumor necrosis factor (TNF), etc. [4]. In addition to cytokines, the formation of T1DM participates more in the process of human immunity; therefore, polypeptides and proteins result in the typical biomarkers, such as C-peptide, urinary haptoglobin [5] and zinc transporter 8 autoantibody (ZnT8A) [6].
T2DM accounts for about 90% of the total DM cases. The course of T2DM is characterized by the co-existence of β-cell secretion dysfunction and insulin resistance. The initial factors of the onset of T2DM are still controversial; however, it can be concluded that the former is a necessary condition for the onset, while the latter is throughout the course of T2DM. Both glucotoxicity and lipid toxicity can cause damage to pancreatic β cells; therefore, long-term acquired high-carbohydrate and high-fat diet can promote the onset of T2DM [7]. Further, related pathogenic genes (CDKAL1, CDKN2A, CDKN2B, etc.) have also been found. Due to the high proportion of T2DM in diabetics and the complexity of its causes, the biomarkers related to T2DM are diverse and involve various parts of physiological processes. For example, glycation markers (such as albumin and cystatin C), oxidation markers (such as apolipoprotein CI), and truncation markers (such as chemokine CCL5) all have considerable reference values in the detection of T2DM.
1.2. Development Status of Diabetes Mellitus Worldwide
According to the 10th edition of the Global Diabetes Map [8] released by the International Diabetes Federation (IDF) in 2021, about 537 million adults worldwide were living with DM. The prevalence rate reached 10.5%, indicating the fact that 1 in 10 people was living with the disease (Figure 1a). The age range of diabetics is wide, covering people aged 20–79 years. Prevalence increases with age, and a similar trend is expected to continue till 2045. Further, the report estimates that for every 20 percent increase in the world population, the number of diabetics increases by about 46 percent, which is expected to rise to 643 million by 2030 and rise to 783 million by 2045. Excluding acute deaths due to COVID-19, approximately 6.7 million people died from DM or its complications in 2021, representing 12.2% of all deaths. Moreover, one-third (32.6%) of diabetes deaths occurred in people younger than 60 years of age.
In such a global situation, the number of diabetics in China increased from 90 million to 140 million in the past 10 years, ranking first in the total number of diabetics. The number of undiagnosed diabetics and the number of diabetes-related deaths (Figure 1b) also showed a rapid growth trend which simultaneously took the first place in the world. Both the treatment conditions for diagnosed diabetes patients and the screening measures for potential diabetes patients bring great pressure on the existing medical system [9]. Therefore, China is faced with a severe situation of DM prevention and control.
The data display that the number of research on DM is gradually increasing in the world (Figure 1c). In recent 5 years, the number of articles published worldwide has been on the rise, with the United States taking the leading position. Although the number of articles published in Asian countries has been on the rise [10], it reveals the lack of influence of articles published and the necessity to improve the article quality. In addition, comparing the research emphases worldwide, it can be seen that, with diabetes complications as the central axis, researchers abroad focus on effective correlation indicators such as blood glucose detection and all-cause mortality, and more attention is paid to female patients. In China, the research is more based on DM core mechanics, including blood glucose treatment and intervention, self-health management, disease management, health education, etc., showing no obvious group research preference. Similar research directions exhibit in DM information intervention and the emphasis of intelligent health management guided by disease [11].
1.3. Importance of Diabetes Mellitus Diagnosis and Treatment
Complications developed in the late stage of DM will cause great harm to the human body. Affected by excessive blood glucose environment, large, medium, small, and micro blood vessels in the whole body could be injured, leading to various cardiovascular and cerebrovascular diseases. The respiratory system and urinary system are also common areas that suffer from complications, including tuberculosis and kidney failure. In addition, DM has a great impact on patients’ eyes and feet. The complications in eyes often reflect in diabetic fundus diseases, cataracts, and retinopathy, while diabetic foot shows infection, diabetic foot ulcer (DFU), and gangrene as typical symptoms [12], which is the most well-known complication in the public view [13]. Diabetic foot is one of the most serious complications of DM, as well as the most common reason for hospitalization of diabetics and one of the leading causes of amputation worldwide. For female diabetics, various risks during pregnancy will be increased to some extent, followed by the increasing probability of birth defects in the next generation [14].
According to the recovery situation of COVID-19 in the past two years, COVID-19 patients with underlying diseases often face more severe symptoms or deterioration of the existing underlying diseases [15,16], most commonly seen in patients with cardiovascular and diabetes diseases. This discovery indicates that DM undoubtedly interferes and hinders the treatment and intervention of COVID-19 patients, and the complicated factors that doctors need to consider in the treatment process have increased. The facts above confirm the high proportion of deaths from DM and its complications mentioned in Section 1.2. Therefore, reasonable prevention, diagnosis, and treatment of DM are significant for national health. What is noteworthy is that some data speculate that COVID-19 survivors may be at an increased risk of developing new-onset DM, identified as a kind of post-acute sequelae of COVID-19 (PASC) [17].
In order to deal with the current situation of diabetics with multiple subtypes and phenotypes mentioned in Section 1.1, researchers have constantly emphasized the importance of DM reclassification. With the support of the “palette model” theory [18], reclassification was carried out based on topology-based analysis [19] and Bayesian non-negative matrix factorization clustering method [20] to achieve personalized treatment at the level of precise diabetology from pathogenesis [21] as much as possible (Figure 2). On the one hand, effective prevention of the formation of DM through genetic testing and lifestyle management can improve the quality of life of the people, fitting right in the concept of “preventive treatment of disease”, which is expected to achieve if further research and development of early diagnosis technology of DM make great progress. On the other hand, for patients already suffering from DM, small portable wearable devices helping in diabetes diagnosis, multi-target and multi-channel diabetes treatment will effectively extend lives and improve patients’ motivation facing the disease.
2. Diagnosis of Diabetes Based on Electrochemical Biosensing Technology
According to the distribution and total number of DM patients, the demand in the global market for diabetes diagnostic equipment increased quickly, while the demand for cost-effective, convenient, highly portable, and responsive medical equipment has also increased year by year in the past decade. Both the rapid development of biochemical technology and the increasing demand for a higher standard of living have contributed to this scene.
The diagnosis of DM is inseparable from blood glucose detection, its original feature. The earliest detection for blood glucose was developed in the early 1900’s by Canadian surgeon Frederick Banting and his assistant Charles Best to measure glucose in blood and urine. Clark and Lyons proposed the initial concept of a glucose sensor in 1962 [22] on the basis of it, which explored the approach for people to study glucose detection technology. After that, electrochemical technologies were introduced into the invention of sensors, and electrochemical sensing components such as enzymes and electrodes [23] were added to the detection chain to optimize the whole process. It was not until 1971 that Clemens in the United States developed the first regular glucose monitor [24] (the Ames Reflectance meter), which was a milestone in DM detection technology. Although the device was expensive and cumbersome from the point of now, it undoubtedly brought together the best technologies and efforts of numerous scientists at the time. During the evolution of the structure and mechanism of glucose meters, the successful application of screen-printing technology [25], invented in 2004, made the mass production of electrochemical glucose sensors possible and brought great efficiency improvement in the preparation of glucose sensing strips for electrochemical devices. With the development of electrochemical technology, Abbott launched the first electrochemical glucose monitor named ExacTech [26]. The clunky meters have evolved into lighter and more sensitive combinations of strips and reagents.
Nowadays, electrochemical biosensors have been widely used in glucose detection due to their high sensitivity and specificity, accounting for about 85% of the global biosensor market [27]. They are iterating into more sophisticated instruments that can be adapted to a wide range of needs.
2.1. Diverse Blood Glucose Detection
DM, as an endocrine disease, is characterized by hyperglycemia, indicating that its most direct biomarker is blood glucose. During the development history of the glucose meter mentioned, the glucose analyzer (known as Model 23A YSI analyzer) proposed by Yellow Springs Instrument Company in the United States for the amperometric detection of hydrogen peroxide was still used as a clinical diagnostic standard until the 21st century [28]. Although the model of glucose analysis has been changing, its basic chemical reaction mechanism has not changed. Among them, the redox chemical chains based on glucose oxidase (GOx) and glucose dehydrogenase (GDHs) are the most classic, which are still the basis of many current glucose biosensors [29] (Figure 3a). These typical methods are highly selective to glucose targets, and their disadvantages of oxygen dependence and electroactivity interference have also been further overcome by the breakthrough of the electrochemical biosensing technology. So far, three generations of electrochemical glucose analyzers have been developed, including enzymatic and non-enzymatic electrochemical glucose sensing methods for applications in different fields according to the different electron transfer mechanisms (Figure 3b). Enzymatic sensors are constructed by the combination of the immobilized enzyme and electrodes, in which the enzyme is acted as the sensitive element of the biosensor to realize the concentration monitoring of biomolecules. The first-generation glucose-enzyme biosensors use oxygen molecules as electron acceptors. The catalytic reaction of the enzyme will reduce oxygen in the solution and generate hydrogen peroxide, which can measure the concentration of glucose indirectly through the detection of the amount of oxygen reduction or the amount of hydrogen peroxide generated. The second-generation biosensors make use of electron transport medium instead of oxygen as the electron acceptor, overcoming the disadvantages of the first-generation biosensors which are limited by oxygen. The electron transport medium refers to small volume of soluble redox active molecules, such as ferrocene derivatives, ferrocyanide, conductive organic salts and quinones, which are able to carry out a rapid reversible redox reaction to increase the rate of enzymatic reaction. However, this kind of medium can be easily diffused from the enzyme layer into the substrate solution, contributing to the instability of the whole biosensor. Compared with previous two generations, the third-generation biosensors avoid the need of oxygen molecules or electron transfer mediators as electron acceptors, but fix the enzyme directly on the modified electrode. This change of environmental conditions of catalytic reactions makes the active site of the enzyme close to the electrode, which can directly carry out the electron transfer, improving the sensitivity and selectivity of the glucose-enzyme biosensor. The materials used to fix enzymes are often organic conductive composite films, metal or non-metallic nanoparticles. In addition to the enzymatic catalysis, various technologies were applied to develop the non-enzymatic methods [30] to detect glucose and corresponding mechanism has been found in the years of research. Chen and his co-workers have demonstrated the electrochemical detection of glucose using nonenzyme mode, such as plasmon-accelerated electrochemical reaction [31], or on Cu2O/Au nano-composite modified surface [32]. Further, the nanopipette confinement effect is used to investigate the reaction in volume-confined glucose oxidase-based detection [33].
Blood is the most available body fluid for measuring glucose; therefore, most electrochemical glucose analyzers rely on detecting glucose directly in the blood. Although the electrochemical glucose analyzer has made a breakthrough in functionality, achieving great success in the commercialization process, it still has limitations. On the one hand, it is inconvenient that such methods have to pick the finger for sampling. On the other hand, some drugs, metabolites and other blood components may interfere with the glucose sensor [34]. Researchers began to explore wearable non-invasive technology, considering the need for health and cleaning. These non-invasive methods mainly concern the physical and chemical properties of internal and external biological fluids. A typical case of internal fluids is the detection of metabolites in interstitial fluid (ISF). In daily life, the self-regulation of physical and chemical components in ISF contributes to the homeostasis of glucose, Na+, and K+ in the blood, which provides a new approach for people to measure blood glucose. The emergence of flexible electronic devices, like microneedle patches [35], inspired researchers who tried to use them to detect blood glucose through ISF. For example, a kind of biosensor was designed to measure blood glucose which can change the osmotic pressure of ISF by changing the electric field to induce glucose in blood vessels to seep into the skin’s surface [36]. It completed the whole process by means of an electrochemical dual channel generated by a paper battery under the skin, using blood glucose seepage and glucose reverse ion electroosmosis, which showed a high correlation with the clinically measured blood glucose level (>0.9). This kind of flexible electronic device removes interference from the external environment to some extent and is one of the main directions of non-invasive real-time glucose detection in the future.
In addition to the study of internal biological fluids, the measurement methods of glucose in external biological fluids (tears, sweat, saliva, etc.) have also been developed. These fluids are used as samples of glucose, whose specific component concentration is determined by its association with the amount of glucose in the body (Figure 4); thus, glucose concentration can be calculated through the information from these fluids. Saliva contains biomarkers of clinical significance and is easy to obtain, which is of great importance for monitoring physiological and metabolic status. Laura et al. [37] proposed an integrated pacifier sensor (Figure 4b) for non-invasive chemical detection of newborn saliva, whose results achieved a relative standard deviation of about 9%. Integrated disposable PB electrodes by screen printing, which is modified with chitosan and GOx, were used for in vitro analysis of glucose in saliva. It not only breaks through the traditional thought of integrated physical parameters sensors but also avoids piercing the skin to obtain tissue fluids, commonly used in neonatal care units, making the newborn in a safer environment. The sweat can present a timely concentration tracking in various parameters with the change of blood glucose concentration, including sweat glucose concentration and pH value, although its concentration is much smaller than the glucose concentration in the blood [38]. In a typical contribution, Lee et al. [39] developed a wearable sensor for detecting glucose in sweat. When the glucose concentration of sweat was fed back, the statistics of pH value, temperature, and humidity of sweat can assist in correcting the result of it in real-time, forming a multi-mode accurate glucose concentration detection (Figure 4d). This self-checking working system allowed it to measure blood glucose concentration with low sweat volume (4 μL) in non-extreme environments, which showed almost no significant deviation compared with direct blood detection. Further, glucose and lactate contained in tears can also reflect blood glucose concentration to a certain extent [40], and contact lenses equipped with integrated lactate sensors have been invented. In terms of the newly proposed contact lens that detected glucose in tears [41], the researchers realized the detection accuracy of a wide range of concentrations, from the extremely low concentration of 0.05 mM to the high concentration of 0.9 mM, which had a good reproducibility of the results with a standard deviation of only about 4.5%.
Although the composition of biological fluids can indicate the blood glucose concentration, considering the uncertainties of human activities (such as uncontrollable sweat production and pollution risk of the unpredictable mix of new and old sweat in collection pipelines [42]) and the effects of environmental changes (such as changes in ambient temperature and humidity), biological fluids will inevitably be affected by the surrounding parameters, which may not accurately reflect the data. Therefore, how to tackle these extra problems becomes a further research topic. It is one of the development directions in the future to integrate multiple detection technologies of biological fluid components for multi-dimensional detection and calibration, which appears as multi-channel and multi-substrate biosensors. Correspondingly, with the increase in biological fluid technologies for collection and detection, researchers also need to overcome the barriers in computer science of the stable algorithm [43] to predict the level of blood metabolites through various kinds of data.
How to collect multiple types of external fluids simultaneously has great difficulty in technology. For example, sweat and ISF can share the same sampling sites on the skin surface; however, the methods used to collect them are different. When the method of sweat stimulation is used, the perspiration production area cannot be controlled, which may result in the mix of the two collection fluids and interference with the signals. As shown in Kim’s work [44], positive and reverse iontophoresis (IP) was proposed to deal with the problem. The two external fluids were obtained in parallel through the reverse IP of ISF in the cathode chamber and the IP of transdermal pilocarpine delivery in the anode chamber. Under the effect of electric repulsion, the anode delivered the pilocarpine with a positive charge and caused the delivery area to produce sweat, which was located in the pilocarpine-loaded gel in the anode compartment. At the same time, because of the negative charge of the human skin, a convective ionic electroosmotic flow to the cathode resulted in the migration of positive ions and neutral molecules (such as glucose), excluding the interference of proteins, other biomolecules, and some electroactive substances. Therefore, this system allowed selective, simultaneous, and localized sampling to be performed on different electrodes, avoiding mixing between samples (Figure 4e). The cathode side of the system is a biosensor based on glucose oxidase (GOx), and the anode side is a biosensor based on an alcohol oxidation reaction. The alcohol level (anode) and glucose level (cathode) of the blood can be effectively detected, which can be used for the blood glucose diagnosis of DM and the monitoring of the diabetic glucose curve after drinking, by completing the following reactions (1) and (2), respectively on the biosensor. Thus, it may provide a facile strategy to design a non-invasive epidermal sampling and analysis platform for effective evaluation of physiological status.
2.2. Diverse Selections of Biomarkers for Diabetes
The diversity of the synergistic redox reactions makes it possible to detect various biomarkers. On the one hand, there are many other biomarkers useful to indicate the occurrence of DM, just like blood glucose can do, because the endocrine disorder is a complex process. In traditional detections, biomarkers such as urine glucose, glycosylated hemoglobin, serum insulin, and insulin antibody have been used to indicate DM [47]. Studies on metabolomics markers start from the direction of lipid and glucose metabolism and have been reported that amino acids and their derivatives are significantly associated with DM [48,49], such as glycine and glutamine, the content of which is negatively correlated with the disease. In order to overcome the shortcoming that a single biomarker cannot accurately indicate diseases, Borges et al. proposed an integrative method on the basis of principal component analysis (PCA). Through the evaluation of the reliability of different biomarkers for the diagnosis in patients, different combinations of diabetes biomarkers were associated, and specific biomarker combinations, such as glycation markers and oxidation markers, were obtained. The detection of a single biomarker was expanded into the detection of a combination of biomarkers, which greatly improved the accuracy of DM detection [50].
The study of molecular markers has also been developed since most types of DM have been linked to genes. These markers are mainly microRNAs (miRNAs). For example, miRNA-375 will be highly expressed during the onset of DM, while miRNA-23a will be significantly reduced in the plasma of patients with T2DM. Recent studies have confirmed that circRNA is another reliable molecular marker to indicate the occurrence of DM and its related complications [51], which have been shown to be related to insulin regulation and disease development in patients with T2DM [52]. Furthermore, these kinds of markers suggest the occurrence of complications such as diabetic retinopathy and diabetic nephropathy, more specifically [53], which provide a more effective way to predict complications for the long-term treatment of DM patients and a new guiding basis for the comprehensive early diagnosis of DM.
On the other hand, the evolution of electrochemical techniques would bring about the way of biomarker detection updates. With researchers experimenting with new substrates and electrochemical reaction chains, the quest for biosensors has never stopped. Newfound reaction chains continuously improve the electrochemical detection scheme of various biomarkers and simplify the reaction steps, which further increases the accuracy of results and improves detection efficiency. For example, Esokkiya et al. reported an acetaldehyde (AcH) ultra-trace detection sensor based on electrochemically activated copper nitroprusside (CuNPr) in 2022 [54]. This method is expected to overcome the difficulty and high cost of traditional breathalyzers with fuel cells for the accurate measurement of acetaldehyde. Therefore, based on technological development, people will have more feasible sections about biomarker detection objects and methods for DM in the future.
With the development of non-invasive detection, researchers found that reasonable capture and analysis of volatile organic compounds (VOCs) in human breath can obtain associated blood indicators, combined with the biochemical indicators of DM in body fluids and current breath detection methods. The ease of access to breath samples is one of the huge advantages of expiratory biochemical sensors. Acetone, acetaldehyde, carbon monoxide, alkane, methyl nitrate, and other compounds in respiration have been proven to have abnormal concentrations in patients with DM [55]. According to the method of PCA, researchers further classified VOCs into different clusters (Table 1) to indicate the occurrence of DM accurately [56]. On account of non-invasive breath testing, some researchers have tried to develop a self-powered wearable breath biosensor based on the electrochemical determination of acetone for non-invasive blood glucose monitoring. Su et al. [57] proposed an electrochemical respiratory biochemical sensor based on a triboelectric nanogenerator (TENG) (Figure 5). The periodic vertical contact and separation of the PTFE film and nylon film acted as a self-powered device in the upper chamber. Patients’ breath entered the lower reaction chamber, and then the acetone in the airflow reacted with the sensitive film at the bottom of the chamber to produce electron exchange which changed the dielectric constant of the gas so that the voltage generated by the upper self-powered chamber, which would conduct to the copper electrode in the lower chamber, occurred different degrees of attenuation. From the analysis of the final load voltage displayed by the device, the acetone concentration in the breath and the breath state of the patients can be detected simultaneously. In addition to the sensors of a single biochemical indicator, Wang et al. [58] prepared a self-powered respiratory biosensor based on the transverse sliding mode of a TENG for the multi-channel detection of gas molecules synchronously. The sensor set up the sensing unit and the self-powered unit in a piece of the electronic sticker, which could complete the whole sensing process through the displacement current caused by the breakdown discharge. In a further study, researchers successfully adjusted the amplitude and spectrum of the signal, making this self-powered wireless sensing e-sticker (SWISE) realize the multi-point sensing behavior of gas sensing.
3. Novel Treatment of Diabetes Based on Electrochemical Biosensing Technology
Over the years, a variety of technologies have been applied in the treatment of DM, aiming to inhibit the progression of DM based on blood glucose control and insulin regulation. Hypoglycemic drugs have the longest history. Metformin was first reported in 1922 [59] and is currently the most classic hypoglycemic drug ingredient. From the 1920s to the 1960s, people gradually discovered the hypoglycemic ability of metformin in animals [60] and humans [61]. It is surprising that the process of hypoglycemia is harmless to the body, both in animals and humans. With the development of drug extraction technology, researchers discovered and prepared more components with hypoglycemic effects, such as the genus Aloe [62] and tetrahydrocarbazole derivatives [63]. At the same time, the discovery of insulin marked a major breakthrough in medicine and treatment for DM. The deepening knowledge of the human body and physiology made people aware of insulin [64] and its close association with DM. Therefore, in addition to controlling DM by reducing blood glucose, researchers also shifted their attention to insulin levels, including the improvement in insulin sensitivity [65], external insulin delivery, and the development of insulin analogs [66]. Combination therapies with hypoglycemic drugs and insulin control were also being perfected. The variety of means of controlling the progression of DM led to an increase in the life expectancy and the frequency of diabetes complications of most people with DM. At present, the prevention and cure of diabetic complications have become an important issue in improving the quality of life of DM patients. Researchers are still struggling at the forefront of DM treatment, seeking the well-being of patients, while patients’ demand for DM treatment has changed from blood glucose reduction and regulation simply to diversified requirements such as portability, autonomy, and safety.
3.1. Insulin Administration Regimen
Oral hypoglycemic drugs and insulin administration are traditional methods of DM treatment; however, both of them lack intelligent regulation of blood glucose levels, often leading to poor blood glucose control and the risk of hypoglycemia. If the oral drug administration schedule is fixed, it cannot be adjusted in time in the long-term development of DM, which will result in problems such as a potential mismatch between the severity of the disease and the schedule. Insulin administration is mostly limited to subcutaneous and intravenous injections. Frequent injections may cause pain, and the injection site is prone to inflammation, increasing the risk of infection [67].
The study of the microneedle patch greatly reduces the risk of infection during insulin administration, and the environmental stimulus-responsive microneedle patch is more efficient in regulating blood glucose levels. Glucose-responsive compounds with different mechanisms (such as glucose oxidase (GOx), glucose-binding protein (GBP), etc.) are used to construct biochemical cascade reactions with glucose in vivo so as to effectively stimulate polymer dissociation in microneedles to release insulin and other glucose-regulating agents when blood glucose concentration rises. At the same time, when the content is released by the change of glucose, the internal environmental feedback can regulate the amount of the content released. For example, the pH-responsive micellar complex developed by Zhang [68] has a cascade reaction behavior triggered by changes in the pH of the environment. In the condition of hyperglycemia, the oxidation of the polymer and the reduction in the negative charge of insulin occur successively, which leads to the dissociation of the complex on the microneedle and the subsequent release of insulin. This two-step cascade of insulin release avoids the failure release of drugs in single acid environments and increases the safety of drug delivery (Figure 6a). Similarly, oxidation-responsive polymer microneedle patches were developed. Chen et al. [69] reported an intelligent insulin delivery device based on dual mineralized particles containing exendin-4 (Ex4) and glucose oxidase (GOx). While sensitive to blood glucose concentration, the patch device can achieve the transformation of glucose signal to H signal when blood glucose concentration rises, releasing drugs specifically. After the blood glucose concentration gradually returns to normal level, the release rate of drugs slows down, forming a long-term closed-loop regulation. Some studies have proposed that glucose-responsive copolymers, which can be self-assembled into nanocarriers, can decompose and release insulin in a high-glucose environment in the body [70]. The researcher used polymer vesicles, a kind of carrier with a strong hollow structure and a large loading capacity of hydrophilic drugs, to improve the efficiency of insulin use and its own biocompatibility to a certain extent. The carrier was self-assembled from an amphiphilic triblock copolymer, poly(ethylene glycol)-b-poly(3-acrylamidophenylboronic acid)-b-poly(4-(4,4,5,5-tetramethyl-1,3,2-dioxaborolan-2-yl)benzyl acrylate) (PEG-b-PPBA-b-PPBEM). The polymer vesicles have both functional groups of phenylboronic acid (PBA) sensitive to glucose and phenylboronic acid pinacol ester (PBEM) sensitive to H2O2, which have a dual cascade response to glucose after being coated with insulin and GOx. For the selection of patch microneedles, researchers prepared soluble microneedles based on poly(vinylpyrrolidone) (PVP) and (poly(vinyl alcohol)) (PVA), which can be inserted into the skin cuticle to deliver internal reagents to the skin barrier not only noninvasively but also safely dissolve in the skin tissue after the use. It had a practical significance that insulin can release from vesicles in an incomplete state under normal glucose concentration, while it is able to release a large amount of insulin promptly under high glucose concentration according to the results of animal experiments, which better fulfilled the goal of rapid response and long-term painless drug administration (Figure 6b). As described in Section 2.1, with the improvement in glucose-related reaction chains, adjustable means of insulin administration are gradually developed.
Insulin administration sources include external and internal routes. The external routes, including oral medication, subcutaneous injection, and microneedle administration, are discussed previously. Internally, the artificial pancreas (closed-loop glucose controller) is created to deliver insulin as an implantable pump. The drugs in closed-loop control show better blood glucose control compared to traditional insulin therapy (open-loop control). In general, the closed-loop system includes an insulin pump, a continuous glucose monitor, and a control algorithm [71] designed to measure and regulate blood glucose concentration in vivo in real time. PID algorithm [72], model predictive control (MPC) [73], controller based on pancreatic physiology (BiAP) [74], and other algorithms iteratively improve the drug delivery scheme of an artificial pancreas. Through the integration of bioelectronics, information engineering, and other disciplines, human identity as an important controller of the external open loop is liberated, which is expected to achieve long-term operation by self-help drug delivery depending on the changes of the organism’s environment. At present, many varieties of closed-loop control systems have completed commercial applications. Medtronic MiniMed 670 G (Minimed Medtronic, Northridge, California) [75] is the first commercial hybrid closed-loop system. Although T1DM is treated by artificial pancreas far more than T2DM and the algorithm is more mature, the plasticity of an artificial pancreas is stronger than other open-loop controls when facing both T1DM and T2DM simultaneously.
3.2. Bioelectronic Medicine Based on Nervous System Regulation
Despite the widespread success of the drug approach in treating DM, many problems remain, such as side effects, drug resistance, and patient compliance. The increase in treatment resistance in many chronic diseases will further limit the use of drug therapies. Therefore, people begin to explore alternative treatment strategies for chronic metabolic diseases.
Recent studies in the field of glucose homeostasis show that the nervous system is greatly involved in the control of dietary intake (such as appetite) as well as the regulation of hormone pancreatic secretion and insulin sensitivity [76], providing brand new thoughts toward the treatment of DM. In the past, this type of electrostimulation therapy focused on treating inflammatory diseases by interfering with the neuroimmune reflex and has successfully improved the treatment of rheumatoid arthritis and colitis in clinical trials.
The success of electrical nerve stimulation has given researchers confidence that the use of electrical stimulation in conjunction with nervous system therapy is expected to be the non-drug treatment option. People try to abandon the traditional thinking of drug therapy and look for ways to regulate the repair from the inside out: (1) Whether they can record the electrical activity of peripheral nerves to extract metabolic information; (2) Whether blood glucose fluctuations can be improved by regulating electrical activity. This therapeutic approach, which alleviates metabolic dysfunction by stimulating relevant nerves and silences or activating nerves to control organ and tissue function, is called bioelectronic medicine [77].
Studies of the nervous system are gradually unraveling the question of how neural circuits regulate blood glucose in the human body. On the one hand, pancreatic β-cells have been found to be electrochemically active cells that are able to depolarize and release insulin in response to glucose activation. Since adjacent pancreatic β-cells are connected through the interstice, depolarization will spread throughout the network and islets. On the other hand, the activity of pancreatic β-cell is also regulated by direct innervation. Acetylcholine (ACh) released from nerve endings of efferent fibers in the vagus nerve increases insulin release in response to glucose stimulation [78]. However, the complexity of the nervous system also has resulted in its characteristics of multi-pathway, multi-target, and multi-synergistic glucose regulation circuits. In addition to the neural pathways found around the pancreatic β-cells, the central nervous system also plays a role in glucose homeostasis and numerous peripheral nerves, which directly control the endocrine function of the pancreas.
To date, researchers have only a sketchy understanding of the physiological mechanisms behind this neurometabolic interaction, while multicellular biological circuits are expected to be properly designed to replace and restore the lost function, which diseased tissues operate to complete the body’s autonomous response in metabolic diseases. In terms of DM, activation or inhibition of neural activity in specific groups of neurons can be used to achieve glucose homeostasis. Over the past few years, new treatment strategies for T2DM have been developed based on electrical stimulation of peripheral nerve fibers. These studies focus on the effects of neural stimulation on food intake and insulin sensitivity recovery [79]. Joana et al. used kilohertz frequency alternating current (KHFAC) modulation to electrically stimulate the carotid sinus nerve (CSN). The glucose tolerance and insulin sensitivity of mice were improved to a certain extent under the appropriate KHFAC pulse frequency, which was designed in the form of rectangular pulses, with several clinical experiments showing good responses. Therefore, bioelectronic medicine based on nervous system regulation is expected to provide more entry points for DM treatment.
4. Summary and Prospect
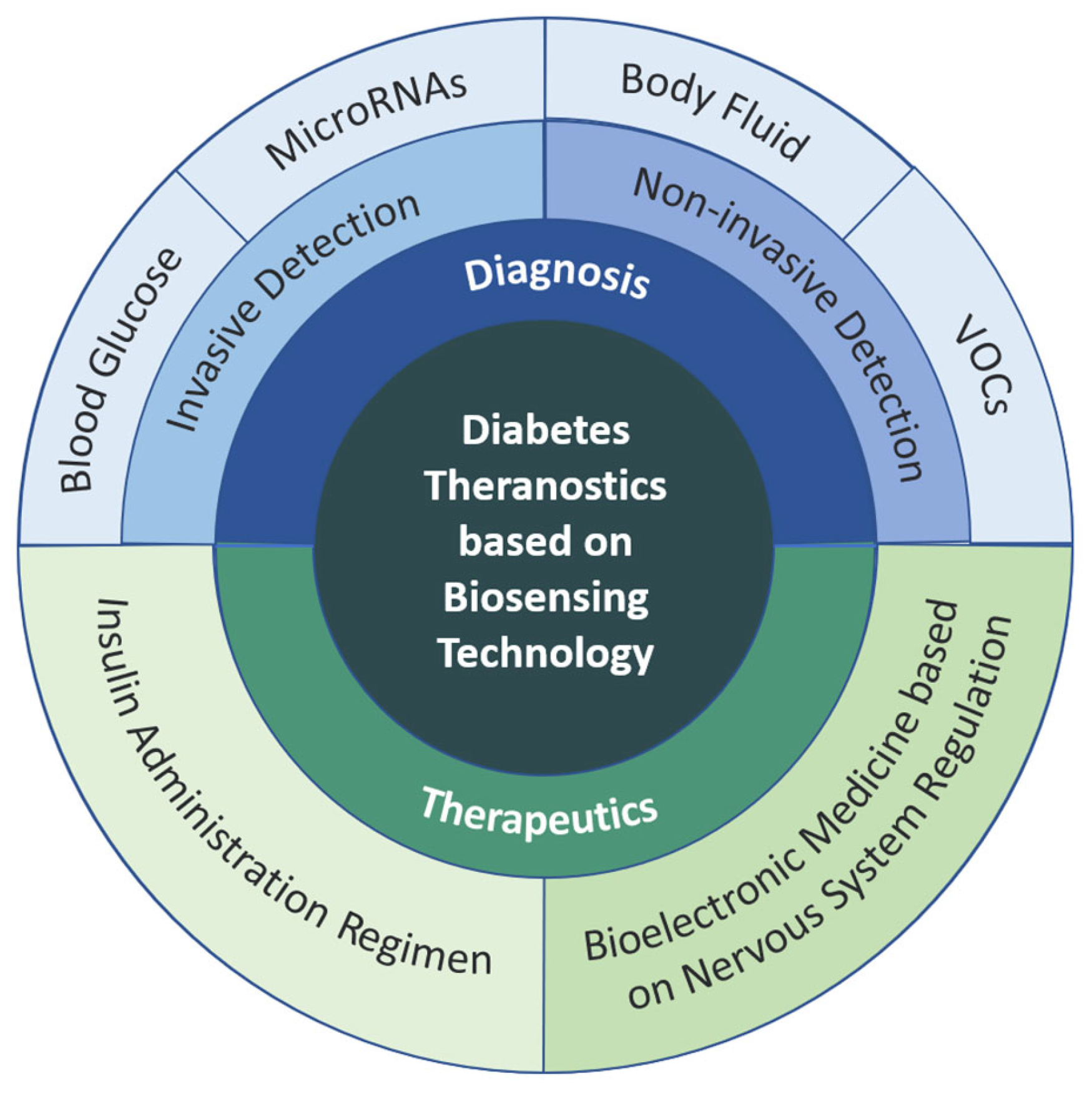
The correlation between electrochemical biosensing technology and existing diagnosis and treatment technology for DM indicates that electrochemistry plays an important role in such processes, including reaction principle at the biochemical level in diagnosis and treatment technology, signal transduction at the electronic level, or the construction of dynamic models. It connects various technologies together to construct biological signal transduction pathways with different functions and application scenes, making contributions to the improvement in the efficiency, portability, timeliness, and safety of DM diagnosis and treatment (Figure 7). This is of great significance at a time when the global diabetes situation is becoming increasingly serious.
4.1. Diagnosis of Diabetes
For diagnosis of diabetes, firstly, the diversified detection methods of blood glucose and the relevant principles of mainstream blood glucose measurements (enzymatic and non-enzymatic glucose electrochemical sensors) are introduced, including direct blood collection and indirect analyses of external body fluids (tears, saliva, sweat, tissue fluid, etc.). Followed by the proposal of unreliability and non-uniqueness of single indicators, some biochemical indicators (metabolomics markers, molecular markers, etc.) that have been proved to be associated with diabetes are listed on the basis of the principal ponent analysis. Further, breath measurement methods are mentioned in detail as an application of VOCs.
The development of glucose detection technology based on electrochemistry has made great progress in the perspective of diabetes diagnosis. Researchers have expanded more diversified diagnostic ideas based on traditional glucose-related electrochemical reactions, including but not limited to the joint application of new nanomaterial reaction chains and enzyme electrodes, the integration of non-invasive/minimally invasive electrochemical sensor platforms and wearable bioelectronics and self-powered biosensors. Although there are some problems with the development of advanced material technology and computational models, such as accuracy, reliability, and environmental impact in the realization process, it is expected to develop the sensor system with the more accurate functions required. In addition, as the limitations of single biomarker detection are gradually realized, multi-biomarker analysis technology has come to the stage. Recently, the convergence of technologies has become a trend that advance the integration of different surface chemical compositions and detection principles in a single device. In virtue of methods for simplification of the complexity in high-dimensional data, such as principal component analysis, the detection techniques of different combinations of biochemical indexes become more and more mature, preventing conflicting indicators from influencing results. Future diabetes-related sensing strategies tend to focus on the improvement in cost performance, accuracy, precision, selectivity, and stability, providing more comfortable and safe conditions for patients. Advances with the concept of miniaturization and portability, better software, and hardware facilities can be provided in booming electrochemical biosensing technology.
4.2. Treatment of Diabetes
Considering the demand for the treatment of diabetes, the advantages and disadvantages of different drug delivery methods are introduced in Section 3, drawing forth the typical cases of current controlled drug delivery methods (microneedle patch, artificial pancreas, etc.) and their general principles. For non-drug treatment methods, we have summarized the theoretical studies and empirical studies on the use of the nervous system to regulate insulin secretion in DM.
The hygiene and regulation of dosage is very important in terms of the treatment of diabetes. In view of the shortcomings of traditional oral drugs and subcutaneous injection, glucose and its Gox-related reactions show the possibility of controlled insulin release, which starts to build a long-term independent and sustained-release insulin delivery channel. Researchers have paid more attention to microneedle patches recently due to their low risk of infection and portable characteristics, promoting the progress of modified polymer micelles/vesicles in controlled slow-release insulin delivery.
Generally, the emergence of resistance to the treatment of chronic metabolic diseases prompts the urgent demand for new non-drug alternative therapies. Drawing inspiration from the successful application of spinal cord electrical stimulation to treat chronic pain, researchers turn their attention to electrotherapy based on continuous in-depth research on human metabolic neural pathways. However, on account of the high complexity of the human nervous system, the relevant neural pathways of blood glucose regulation have not been sorted out until now. While neurotherapy is promising, there are still a lot of research depths and hurdles to overcome. It is worth mentioning that the combination of existing neural pathways and the closed-loop control of the artificial pancreas has become a new direction, which is expected to simultaneously instruct the artificial pancreas to acquire information and repair the body damage to reduce the amount of insulin administration to a certain extent.
Funding
This research was funded by the National Natural Science Foundation of China (21974019, 82027806).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No research data are available.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Leslie, R.D.; Palmer, J.; Schloot, N.C.; Lernmark, A. Diabetes at the crossroads: Relevance of disease classification to pathophysiology and treatment. Diabetologia 2016, 59, 13–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adler, A.; Bennett, P.; Chair, S.C.; Gregg, E.; Narayan, K.M.V.; Schmidt, M.I.; Sobngwi, E.; Tajima, N.; Tandon, N.; Unwin, N.; et al. Reprint of: Classification of diabetes mellitus. Diabetes Res. Clin. Pract. 2021, 108972. [Google Scholar] [CrossRef] [PubMed]
- Burahmah, J.; Zheng, D.; Leslie, R.D. Adult-onset type 1 diabetes: A changing perspective. Eur. J. Intern. Med. 2022, 104, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.W.; Ruan, M.H.; Liu, J.L.; He, C.H.; Yu, J.R. Progress on research and development in diabetes mellitus. Yi Chuan = Hered. 2022, 44, 824–839. [Google Scholar]
- Bezen, D.; Vurgun, E.; Dursun, H. Evaluation of urinary haptoglobin level as a biomarker of diabetic nephropathy in children with type 1 diabetes. Pediatr. Nephrol. 2023. [Google Scholar] [CrossRef]
- Bhatty, A.; Baig, S.; Fawwad, A.; Rubab, Z.E.; Shahid, M.A.; Waris, N. Association of zinc transporter-8 autoantibody (ZnT8A) with type 1 diabetes mellitus. Cureus 2020, 12, e7263. [Google Scholar] [CrossRef] [Green Version]
- Liang, W. Type 2 Diabetes Pathogenesis and Treatment. Smart Healthc. 2021, 7, 43–45. [Google Scholar]
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar]
- Wang, L.; Gao, P.; Zhang, M.; Huang, Z.; Zhang, D.; Deng, Q.; Li, Y.; Zhao, Z.; Qin, X.; Jin, D.; et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA 2017, 317, 2515–2523. [Google Scholar] [CrossRef]
- Ramachandran, A.; Ma, R.C.W.; Snehalatha, C. Diabetes in asia. Lancet 2010, 375, 408–418. [Google Scholar] [CrossRef]
- Sun, X.R.; Yong, Q.M.; Peng, T.; Gao, W.J.; Yang, L. A visual analysis of the research progress in information technology-enabled diabetes management in China and abroad. Chin. J. Clin. Healthc. 2022, 25, 662–666. [Google Scholar]
- Kalish, J.; Hamdan, A. Management of diabetic foot problems. J. Vasc. Surg. 2010, 51, 476–486. [Google Scholar] [CrossRef] [Green Version]
- Matijević, T.; Talapko, J.; Meštrović, T.; Matijević, M.; Erić, S.; Erić, I.; Škrlec, I. Understanding the multifaceted etiopathogenesis of foot complications in individuals with diabetes. World J. Clin. Cases 2023, 11, 1669–1683. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.W.; Hoffstad, O.J.; Sullivan, M.O.; Margolis, D.J. Association of diabetic foot ulcer and death in a population-based cohort from the United Kingdom. Diabet. Med. 2016, 33, 1493–1498. [Google Scholar] [CrossRef] [PubMed]
- Mansueto, G.; Niola, M.; Napoli, C. Can COVID 2019 induce a specific cardiovascular damage or it exacerbates pre-existing cardiovascular diseases? Pathol.-Res. Pract. 2020, 216, 153086. [Google Scholar] [CrossRef]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Harding, J.L.; Oviedo, S.A.; Ali, M.K.; Ofotokun, I.; Gander, J.C.; Patel, S.A.; Magliano, D.J.; Patzer, R.E. The bidirectional association between diabetes and long-COVID-19–A systematic review. Diabetes Res. Clin. Pract. 2022, 195, 110202. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, M.I. Painting a new picture of personalized medicine for diabetes. Diabetologia 2017, 60, 793–799. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Cheng, W.Y.; Glicksberg, B.S.; Gottesman, O.; Tamler, R.; Chen, R.; Bottinger, E.P.; Dudley, J.T. Identification of type 2 diabetes subgroups through topological analysis of patient similarity. Sci. Transl. Med. 2015, 7, 311ra174. [Google Scholar] [CrossRef] [Green Version]
- Udler, M.S.; Kim, J.; von Grotthuss, M.; Bonàs-Guarch, S.; Cole, J.B.; Chiou, J.; Boehnke, M.; Laakso, M.; Atzmon, G.; Glaser, B.; et al. Type 2 diabetes genetic loci informed by multi-trait associations point to disease mechanisms and subtypes: A soft clustering analysis. PLoS Med. 2018, 15, e1002654. [Google Scholar] [CrossRef] [Green Version]
- Herder, C.; Roden, M. A novel diabetes typology: Towards precision diabetology from pathogenesis to treatment. Diabetologia 2022, 65, 1770–1781. [Google Scholar] [CrossRef]
- Clark, L.C., Jr.; Lyons, C. Electrode systems for continuous monitoring in cardiovascular surgery. Ann. N. Y. Acad. Sci. 1962, 102, 29–45. [Google Scholar] [CrossRef] [PubMed]
- Updike, S.J.; Hicks, G.P. The enzyme electrode. Nature 1967, 214, 986–988. [Google Scholar] [CrossRef] [PubMed]
- Newman, J.D.; Turner, A.P.F. Home blood glucose biosensors: A commercial perspective. Biosens. Bioelectron. 2005, 20, 2435–2453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.E. Screen-printing methods for biosensor production. In Biosensors: A Practical Approach, 2nd ed.; Cooper, J.M., Cass, A.E.G., Eds.; Oxford University Press: New York, NY, USA, 2004; pp. 41–58. [Google Scholar]
- Kyvik, K.O.; Traulsen, J.; Reinholdt, B.; Frøland, A. The ExacTech blood glucose testing system. Diabetes Res. Clin. Pract. 1990, 10, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Shoaib, A.; Darraj, A.; Khan, M.E.; Azmi, L.; Alalwan, A.; Alamri, O.; Tabish, M.; Khan, A.U. A Nanotechnology-Based Approach to Biosensor Application in Current Diabetes Management Practices. Nanomaterials 2023, 13, 867. [Google Scholar] [CrossRef] [PubMed]
- Vashist, S.K.; Zheng, D.; Al-Rubeaan, K.; Luong, J.H.T.; Sheu, F.S. Technology behind commercial devices for blood glucose monitoring in diabetes management: A review. Anal. Chim. Acta 2011, 703, 124–136. [Google Scholar] [CrossRef]
- Teymourian, H.; Barfidokht, A.; Wang, J. Electrochemical glucose sensors in diabetes management: An updated review (2010–2020). Chem. Soc. Rev. 2020, 49, 7671–7709. [Google Scholar] [CrossRef]
- Scandurra, A.; Censabella, M.; Boscarino, S.; Condorelli, G.G.; Grimaldi, M.G.; Ruffino, F. Fabrication of Cu(II)oxide-hydroxide nanostructures onto graphene paper by laser and thermal processes for sensitive nano-electrochemical sensing of glucose. Nanotechnology 2021, 33, 045501. [Google Scholar] [CrossRef]
- Wang, C.; Nie, X.G.; Shi, Y.; Zhou, Y.; Xu, J.J.; Xia, X.H.; Chen, H.Y. Direct plasmon-accelerated electrochemical reaction on gold nanoparticles. ACS Nano 2017, 11, 5897–5905. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhao, W.; Chen, H.Y.; Xu, J.J. Dark-field microscopic real-time monitoring the growth of Au on Cu2O nanocubes for ultra-sensitive glucose detection. Anal. Chim. Acta 2021, 1162, 338503. [Google Scholar] [CrossRef]
- Wang, Y.; Pan, R.; Jiang, D.; Jiang, D.C.; Chen, H.Y. Nanopipettes for the electrochemical study of enhanced enzymatic activity in a femtoliter space. Anal. Chem. 2021, 93, 14521–14526. [Google Scholar] [CrossRef] [PubMed]
- Tang, Z.; Du, X.; Louie, R.F.; Kost, G.J. Effects of drugs on glucose measurements with handheld glucose meters and a portable glucose analyzer. Am. J. Clin. Pathol. 2000, 113, 75–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, D.D.; Tan, Y.R.; Zheng, L.W.; Lao, J.Z.; Liu, J.Y.; Yu, J.; Chen, P. Microneedle-Coupled Epidermal Sensors for In-Situ-Multiplexed Ion Detection in Interstitial Fluids. ACS Appl. Mater. Interfaces 2023, 15, 14146–14154. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Lu, S.; Zhang, S.; Li, Y.; Qu, Z.; Chen, Y.; Lu, B.W.; Wang, X.Y.; Feng, X. Skin-like biosensor system via electrochemical channels for noninvasive blood glucose monitoring. Sci. Adv. 2017, 3, e1701629. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Carmona, L.; Martin, A.; Sempionatto, J.R.; Moreto, J.R.; Gonzalez, M.C.; Wang, J.; Escarpa, A. Pacifier biosensor: Toward noninvasive saliva biomarker monitoring. Anal. Chem. 2019, 91, 13883–13891. [Google Scholar] [CrossRef]
- Gao, W.; Emaminejad, S.; Nyein, H.Y.Y.; Challa, S.; Chen, K.; Peck, A.; Fahad, H.M.; Ota, H.; Shiraki, H.; Kiriya, D.; et al. Fully integrated wearable sensor arrays for multiplexed in situ perspiration analysis. Nature 2016, 529, 509–514. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Song, C.; Hong, Y.S.; Kim, M.S.; Cho, H.R.; Kang, T.; Shin, K.; Choi, S.H.; Hyeon, T.; Kim, D.H. Wearable/disposable sweat-based glucose monitoring device with multistage transdermal drug delivery module. Sci. Adv. 2017, 3, e1601314. [Google Scholar] [CrossRef] [Green Version]
- Gao, W.; Brooks, G.A.; Klonoff, D.C. Wearable physiological systems and technologies for metabolic monitoring. J. Appl. Physiol. 2018, 124, 548–556. [Google Scholar] [CrossRef]
- Li, Z.; Yun, J.; Li, X.; Kim, M.; Li, J.; Lee, D.H.; Wu, A.Y.; Lee, S.W. Power-Free Contact Lens for Glucose Sensing. Adv. Funct. Mater. 2023, 2304647. [Google Scholar] [CrossRef]
- Son, J.; Bae, G.Y.; Lee, S.; Lee, G.; Kim, S.W.; Kim, D.; Chung, S.; Cho, K. Cactus-Spine-Inspired Sweat-Collecting Patch for Fast and Continuous Monitoring of Sweat. Adv. Mater. 2021, 33, 2102740. [Google Scholar] [CrossRef]
- Anwar, F.; Ejaz, M.Y.; Mosavi, A. A comparative analysis on diagnosis of diabetes mellitus using different approaches–A survey. Inform. Med. Unlocked 2020, 21, 100482. [Google Scholar] [CrossRef]
- Kim, J.; Sempionatto, J.R.; Imani, S.; Hartel, M.C.; Barfidokht, A.; Tang, G.D.; Campbell, A.S.; Mercier, P.P.; Wang, J. Simultaneous monitoring of sweat and interstitial fluid using a single wearable biosensor platform. Adv. Sci. 2018, 5, 1800880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandodkar, A.J.; Jia, W.; Yardımcı, C.; Wang, X.; Ramirez, J.; Wang, J. Tattoo-based noninvasive glucose monitoring: A proof-of-concept study. Anal. Chem. 2015, 87, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Kownacka, A.E.; Vegelyte, D.; Joosse, M.; Anton, N.; Toebes, B.J.; Lauko, J.; Buzzacchera, I.; Lipinska, K.; Wilson, D.A.; Geelhoed-Duijvestijn, N.; et al. Clinical evidence for use of a noninvasive biosensor for tear glucose as an alternative to painful finger-prick for diabetes management utilizing a biopolymer coating. Biomacromolecules 2018, 19, 4504–4511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogurtsova, K.; da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Ashoori, M.R.; Rahmati-Yamchi, M.; Ostadrahimi, A.; Aval, S.F.; Zarghami, N. MicroRNAs and adipocytokines: Promising biomarkers for pharmacological targets in diabetes mellitus and its complications. Biomed. Pharmacother. 2017, 93, 1326–1336. [Google Scholar] [CrossRef]
- Lees, T.; Nassif, N.; Simpson, A.; Shad-Kaneez, F.; Martiniello-Wilks, R.; Lin, Y.G.; Jones, A.; Qu, X.Q.; Lal, S. Recent advances in molecular biomarkers for diabetes mellitus: A systematic review. Biomarkers 2017, 22, 604–613. [Google Scholar] [CrossRef]
- Cao, Y.M. Advances in biomarkers of type 2 diabetes mellitus. J. Med. Theory Pract. 2021, 34, 2. [Google Scholar]
- Dehghanbanadaki, H.; Asili, P.; Haji Ghadery, A.; Mirahmad, M.; Dehnavi, A.Z.; Parsaei, A.; Baradaran, H.R.; Azami, M.; Jose Justo da Silva, G.; Parvan, R.; et al. Diagnostic accuracy of circular RNA for diabetes Mellitus: A systematic review and diagnostic Meta-analysis. BMC Med. Genom. 2023, 16, 48. [Google Scholar] [CrossRef]
- Zhang, Z.; Yang, T.; Xiao, J. Circular RNAs: Promising biomarkers for human diseases. EBioMedicine 2018, 34, 267–274. [Google Scholar] [CrossRef] [Green Version]
- Fan, W.; Pang, H.; Xie, Z.; Huang, G.; Zhou, Z.G. Circular RNAs in diabetes mellitus and its complications. Front. Endocrinol. 2022, 13, 885650. [Google Scholar] [CrossRef] [PubMed]
- Esokkiya, A.; Murugasenapathi, N.K.; Kumar, S.; Sudalaimani, S.; Santhosh, B.; Tamilarasan, P.; Sivakumar, C.; Giribabu, K. Electrochemically activated copper nitroprusside as a catalyst for sensing of carcinogenic acetaldehyde in red wine. Sens. Actuators B Chem. 2022, 363, 131798. [Google Scholar] [CrossRef]
- Yan, K.; Zhang, D.; Wu, D.; Wei, H.; Lu, G.M. Design of a breath analysis system for diabetes screening and blood glucose level prediction. IEEE Trans. Biomed. Eng. 2014, 61, 2787–2795. [Google Scholar] [CrossRef] [PubMed]
- Dixit, K.; Fardindoost, S.; Ravishankara, A.; Tasnim, N.; Hoorfar, M. Exhaled breath analysis for diabetes diagnosis and monitoring: Relevance, challenges and possibilities. Biosensors 2021, 11, 476. [Google Scholar] [CrossRef]
- Su, Y.; Yang, T.; Zhao, X.; Cai, Z. A wireless energy transmission enabled wearable active acetone biosensor for non-invasive prediabetes diagnosis. Nano Energy 2020, 74, 104941. [Google Scholar] [CrossRef]
- Wang, H.; Wang, J.; Yao, K.; Fu, J.; Xia, X.; Zhang, R.; Li, J.; Xu, G.; Wang, L.; Yang, J.; et al. A paradigm shift fully self-powered long-distance wireless sensing solution enabled by discharge-induced displacement current. Sci. Adv. 2021, 7, eabi6751. [Google Scholar] [CrossRef]
- Werner, E.A.; Bell, J. CCXIV.—The preparation of methylguanidine, and of ββ-dimethylguanidine by the interaction of dicyanodiamide, and methylammonium and dimethylammonium chlorides respectively. J. Chem. Soc. Trans. 1922, 121, 1790–1794. [Google Scholar] [CrossRef]
- Slotta, K.H.; Tschesche, R. Über Biguanide, II.: Die blutzucker-senkende Wirkung der Biguanide. Berichte Der Dtsch. Chem. Ges. (A B Ser.) 1929, 62, 1398–1405. [Google Scholar] [CrossRef]
- Bailey, C.J.; Day, C. Metformin: Its botanical background. Pract. Diabetes Int. 2004, 21, 115–117. [Google Scholar] [CrossRef]
- Kazeem, M.I.; Bankole, H.A.; Fatai, A.A.; Saibu, G.M.; Wusu, A.D. Genus Aloe as sources of antidiabetic, antihyperglycemic and hypoglycemic agents: A review. S. Afr. J. Bot. 2022, 147, 1070–1077. [Google Scholar] [CrossRef]
- Wang, L.L.; Du, Y.; Li, S.M.; Cheng, F.; Zhang, N.-N.; Chen, R.; Cui, X.; Yang, S.-G.; Fan, L.-L.; Wang, J.-T.; et al. Design, synthesis and evaluation of tetrahydrocarbazole derivatives as potential hypoglycemic agents. Bioorganic Chem. 2021, 115, 105172. [Google Scholar] [CrossRef]
- Rydén, L.; Lindsten, J. The history of the Nobel prize for the discovery of insulin. Diabetes Res. Clin. Pract. 2021, 175, 108819. [Google Scholar] [CrossRef]
- Ye, J. Commentary: Inhibitors of mitochondrial respiratory chain in the treatment of type 2 diabetes. Acta Pharm. Sin. B 2023, 13, 2807–2808. [Google Scholar] [CrossRef]
- Sebastian, S.A.; Co, E.L.; Mehendale, M.; Hameed, M. Insulin analogs in the treatment of type II diabetes and future perspectives. Dis. -A-Mon. 2023, 69, 101417. [Google Scholar] [CrossRef]
- Zheng, J.; Wu, X.H. Research progress of microneedle patch as insulin delivery device. Chin. J. Diabetes 2022, 30, 3. [Google Scholar]
- Zhang, Y.; Wang, J.; Yu, J.; Wen, D.; Kahkoska, A.R.; Lu, Y.; Zhang, X.D.; Buse, J.B.; Gu, Z. Bioresponsive microneedles with a sheath structure for H2O2 and pH cascade-triggered insulin delivery. Small 2018, 14, 1704181. [Google Scholar] [CrossRef]
- Chen, W.; Tian, R.; Xu, C.; Yung, B.C.; Wang, G.; Liu, Y.; Ni, Q.; Zhang, F.; Zhou, Z.; Wang, J.; et al. Microneedle-array patches loaded with dual mineralized protein/peptide particles for type 2 diabetes therapy. Nat. Commun. 2017, 8, 1777. [Google Scholar] [CrossRef] [Green Version]
- Tong, Z.; Zhou, J.; Zhong, J.; Tang, Q.; Lei, Z.; Luo, H.; Ma, P.; Liu, X. Glucose-and H2O2-responsive polymeric vesicles integrated with microneedle patches for glucose-sensitive transcutaneous delivery of insulin in diabetic rats. ACS Appl. Mater. Interfaces 2018, 10, 20014–20024. [Google Scholar] [CrossRef]
- Nwokolo, M.; Hovorka, R. The artificial pancreas and type 1 diabetes. J. Clin. Endocrinol. Metab. 2023, 108, 1614–1623. [Google Scholar] [CrossRef]
- Mahmud, F.; Isse, N.H.; Daud, N.A.M.; Morsin, M. Evaluation of PD/PID controller for insulin control on blood glucose regulation in a Type-I diabetes. In AIP Conference Proceedings; AIP Publisher: College Park, MD, USA, 2017; Volume 1788, p. 030072. [Google Scholar]
- Magni, L.; Raimondo, D.M.; Dalla Man, C.; De Nicolao, G.; Kovatchev, B.; Cobelli, C. Model predictive control of glucose concentration in subjects with type 1 diabetes: An in silico trial. IFAC Proc. Vol. 2008, 41, 4246–4251. [Google Scholar] [CrossRef] [Green Version]
- Herrero, P.; Georgiou, P.; Oliver, N.; Reddy, M.; Johnston, D.; Toumazou, C. A composite model of glucagon-glucose dynamics for in silico testing of bihormonal glucose controllers. J. Diabetes Sci. Technol. 2013, 7, 941–951. [Google Scholar] [CrossRef] [Green Version]
- Bergenstal, R.M.; Garg, S.; Weinzimer, S.A.; Buckingham, B.A.; Bode, B.W.; Tamborlane, W.V.; Kaufman, F.R. Safety of a hybrid closed-loop insulin delivery system in patients with type 1 diabetes. JAMA 2016, 316, 1407–1408. [Google Scholar] [CrossRef]
- Güemes, A.; Herrero, P.; Georgiou, P. A novel glucose controller using insulin sensitivity modulation for management of type 1 diabetes. In Proceedings of the 2019 IEEE International Symposium on Circuits and Systems (ISCAS), Hokkaido, Japan, 26–29 May 2019; pp. 1–5. [Google Scholar]
- Güemes Gonzalez, A.; Etienne-Cummings, R.; Georgiou, P. Closed-loop bioelectronic medicine for diabetes management. Bioelectron. Med. 2020, 6, 1–7. [Google Scholar] [CrossRef]
- Seicol, B.J.; Bejarano, S.; Behnke, N.; Guo, L. Neuromodulation of metabolic functions: From pharmaceuticals to bioelectronics to biocircuits. J. Biol. Eng. 2019, 13, 11. [Google Scholar] [CrossRef] [Green Version]
- Sacramento, J.F.; Chew, D.J.; Melo, B.F.; Donegá, M.; Dopson, W.; Guarino, M.P.; Robinson, A.; Prieto-Lloret, J.; Patel, S.; Holinski, B.J.; et al. Bioelectronic modulation of carotid sinus nerve activity in the rat: A potential therapeutic approach for type 2 diabetes. Diabetologia 2018, 61, 700–710. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Status of diabetes mellitus worldwide. (a) The estimated total number and global distribution of diabetics in 2021 [8]. (b) Top 10 countries or territories with the highest number of diabetics in 2021 [8]. (c) Visualization analysis of the output of DM information literature in China3National Knowledge Network (CNKI) database and Web of Science Core Collection database by country or region [11]. All figures are licensed under an open-access Creative Commons CC BY license.
Figure 1.
Status of diabetes mellitus worldwide. (a) The estimated total number and global distribution of diabetics in 2021 [8]. (b) Top 10 countries or territories with the highest number of diabetics in 2021 [8]. (c) Visualization analysis of the output of DM information literature in China3National Knowledge Network (CNKI) database and Web of Science Core Collection database by country or region [11]. All figures are licensed under an open-access Creative Commons CC BY license.

Figure 2.
Future implications of precision diabetology based on novel diabetes subgroups [21]. SAID: Severe autoimmune diabetes. SIDD: Severe insulin-deficient diabetes. SIRD: Severe insulin-resistant diabetes. MOD: Mild obesity-related diabetes. MARD: Mild age-related diabetes. All figures are licensed under an open-access Creative Commons CC BY license.
Figure 2.
Future implications of precision diabetology based on novel diabetes subgroups [21]. SAID: Severe autoimmune diabetes. SIDD: Severe insulin-deficient diabetes. SIRD: Severe insulin-resistant diabetes. MOD: Mild obesity-related diabetes. MARD: Mild age-related diabetes. All figures are licensed under an open-access Creative Commons CC BY license.
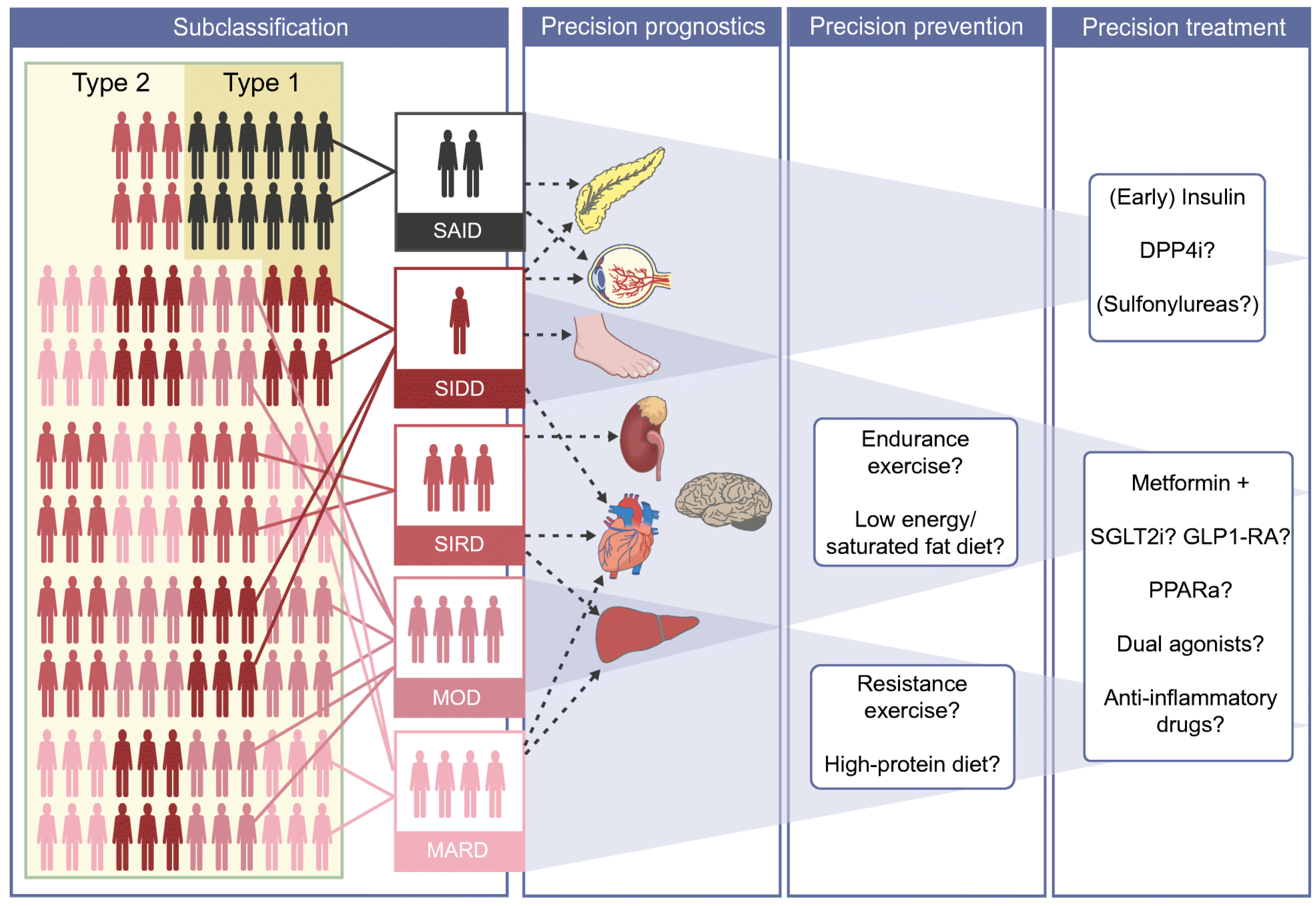
Figure 3.
Schematic diagrams of principle of (a) enzymatic and (b) non-enzymatic electrochemical glucose sensors [29]. Reprint permission was requested from [29].

Figure 4.
Some wearable non-invasive glucose sensor. (a) Tattoo glucose sensor based on ISF [45]. (b) Wireless glucose pacifier sensor [37]. (c) Electrochemical tear glucose sensor [46]. (d) Sensor arrays for sweat glucose monitoring [39]. (e) Wearable biosensor device for wireless real-time detection of the ISF glucose and sweat alcohol [44]. All figures are licensed under an open-access Creative Commons CC BY license.
Figure 4.
Some wearable non-invasive glucose sensor. (a) Tattoo glucose sensor based on ISF [45]. (b) Wireless glucose pacifier sensor [37]. (c) Electrochemical tear glucose sensor [46]. (d) Sensor arrays for sweat glucose monitoring [39]. (e) Wearable biosensor device for wireless real-time detection of the ISF glucose and sweat alcohol [44]. All figures are licensed under an open-access Creative Commons CC BY license.

Figure 5.
Schematic diagram of self-powered wearable acetone breath biosensor [57]. Reprint permission was requested from [57].
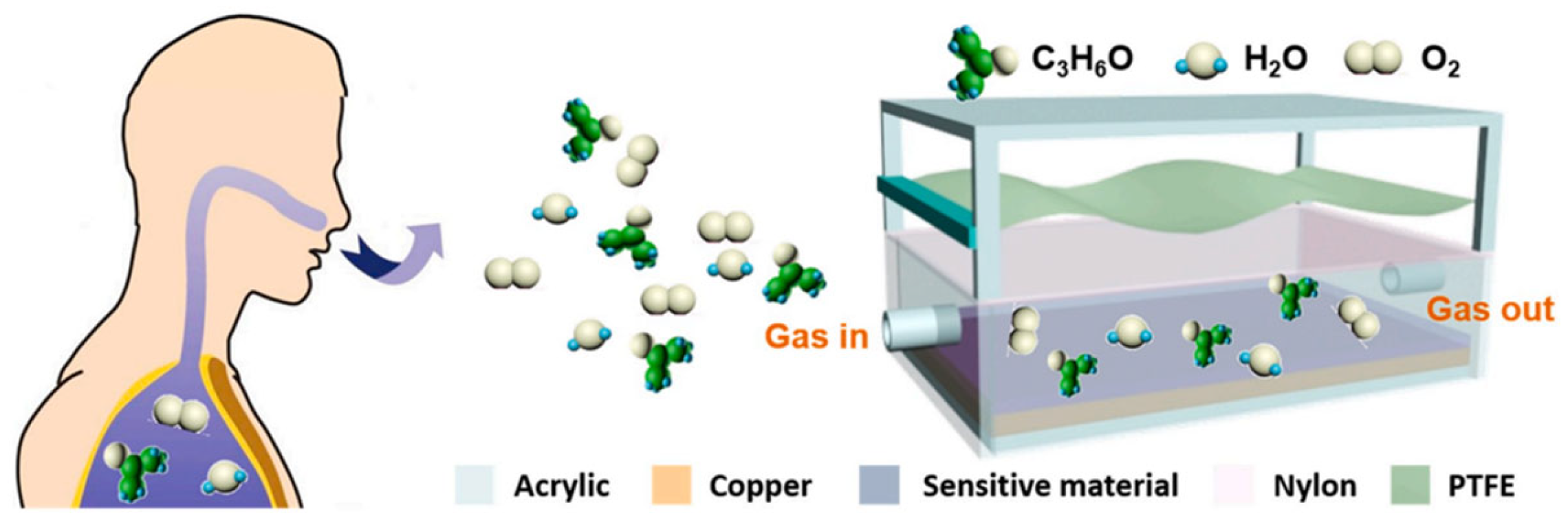
Figure 6.
Schematic diagrams of glucose-responsive insulin delivery systems. (a) A nanoarray transdermal microneedle patch with cascade reaction of H2O2 and pH [68]. Reprint permission was requested from [68]. (b) Synthesis route of PEG-b-PPBA-b-PPBEM and its transdermal drug delivery approach [70]. All figures are licensed under an open-access Creative Commons CC BY license.
Figure 6.
Schematic diagrams of glucose-responsive insulin delivery systems. (a) A nanoarray transdermal microneedle patch with cascade reaction of H2O2 and pH [68]. Reprint permission was requested from [68]. (b) Synthesis route of PEG-b-PPBA-b-PPBEM and its transdermal drug delivery approach [70]. All figures are licensed under an open-access Creative Commons CC BY license.
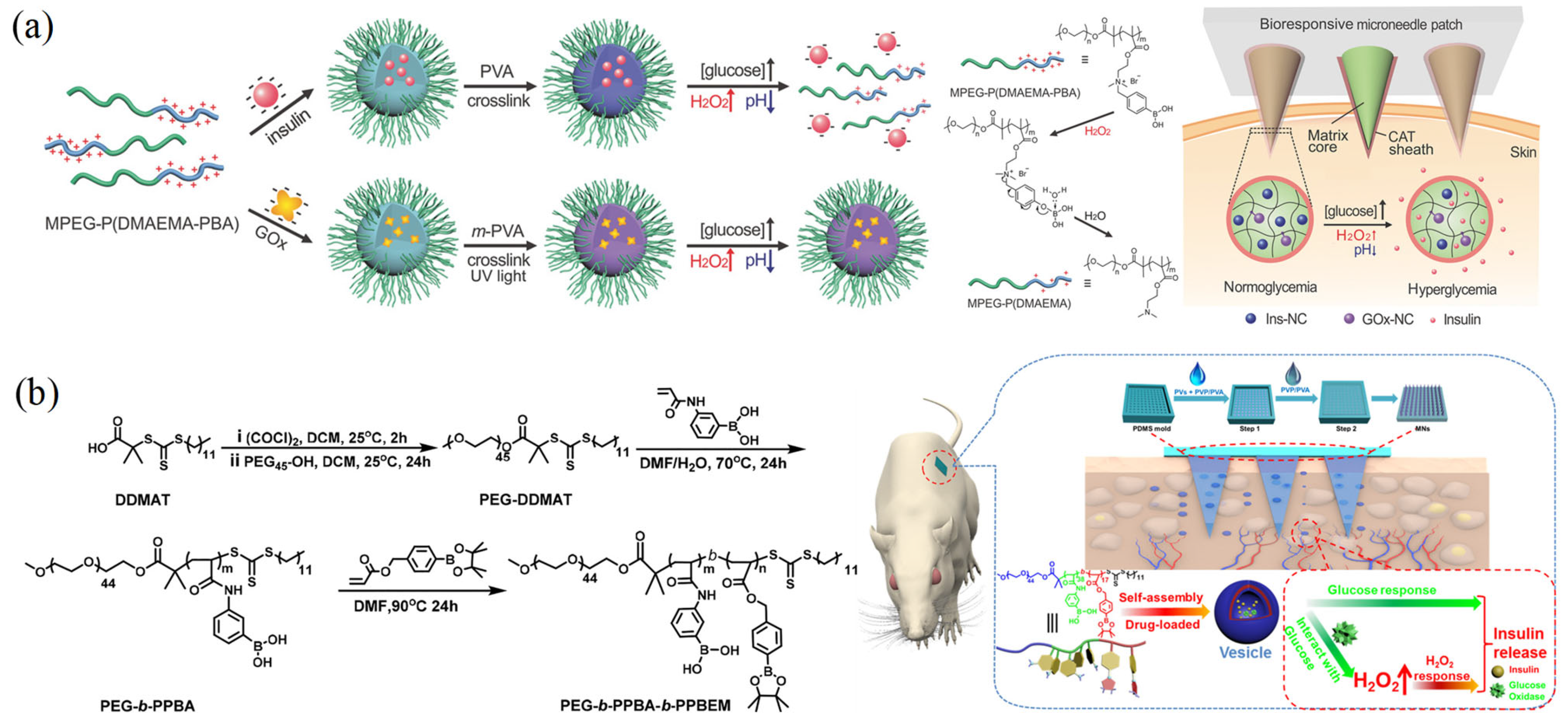
Figure 7.
Diabetes theranostics based on biosensing technology.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
VOC clusters for diabetes diagnosis *.
| Biomarker Clusters | Healthy/T1DM/T2DM Subjects | Method Used | Research Outcome |
|---|---|---|---|
| Acetone, methyl nitrate, ethanol, and ethylbenzene | 17 healthy, 8 T1DM subjects | Gas Chromatograpy | Mean Correlation Coefficients All = 0.883 Healthy Subjects = 0.836 T1DM Subjects = 0.950 |
| 2-pentyl nitrate, propane, methanol, and acetone | 17 healthy, 8 T1DM subjects | Gas Chromatograpy | Mean Correlation Coefficients All = 0.869 Healthy Subjects = 0.829 T1DM Subjects = 0.990 |
| Acetone, ethanol, and propane | 130 healthy, 70 subjects with diabetes | Analog Semiconductor Sensors | Mean Correlation Coefficients All = 0.25 Healthy Subjects = 0.97 Subjects with diabetes = 0.35 |
| Isopropanol, 2,3,4-trimethylhexane, 2,6,8-trimethyldecane, tridecane, and undecane | 39 healthy, 48 T2DM subjects | Gas Chromatograpy—Mass Spectrometry | Sensitivity = 97.9% Specificity = 100% |
* Data adapted from [56].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Xu, X.; Wang, X.; Jiang, H. Current Status and Prospect of Diabetes Diagnosis and Treatment Based on Biosensing Technology. Chemosensors 2023, 11, 391. https://doi.org/10.3390/chemosensors11070391
AMA Style
Xu X, Wang X, Jiang H. Current Status and Prospect of Diabetes Diagnosis and Treatment Based on Biosensing Technology. Chemosensors. 2023; 11(7):391. https://doi.org/10.3390/chemosensors11070391
Chicago/Turabian StyleXu, Xinyi, Xuemei Wang, and Hui Jiang. 2023. "Current Status and Prospect of Diabetes Diagnosis and Treatment Based on Biosensing Technology" Chemosensors 11, no. 7: 391. https://doi.org/10.3390/chemosensors11070391
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.