
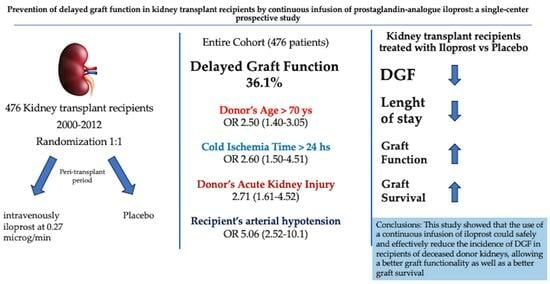
Prevention of Delayed Graft Function in Kidney Transplant Recipients through a Continuous Infusion of the Prostaglandin Analogue Iloprost: A Single-Center Prospective Study

 , , and
, , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meier-Kriesche, H.U.; Schold, J.D.; Srinivas, T.R.; Kaplan, B. Lack of improvement in renal allograft survival despite a marked decrease in acute rejection rates over the most recent era. Am. J. Transplant. 2004, 4, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Stratta, R.J.; Rohr, M.S.; Sundberg, A.K.; Armstrong, G.; Hairston, G.; Hartmenn, E.; Farney, A.C.; Roskopf, J.; Iskandar, S.S.; Adams, P.L. Increased kidney transplantation utilizing expanded criteria deceased organ donors with results comparable to standard criteria donor transplant. Ann. Surg. 2004, 239, 688–695. [Google Scholar] [CrossRef] [PubMed]
- Remuzzi, G.; Cravedi, P.; Perna, A.; Dimitrov, B.; Turturro, M.; Locatelli, G.; Rigotti, P.; Baldan, N.; Betaini, M.; Valente, U.; et al. Long-term outcome of renal transplantation from older donors. N. Engl. J. Med. 2006, 354, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Veroux, P.; Veroux, M.; Puliatti, C.; Valastro, M.; Di Mare, M.; Gagliano, M.; Macarone, M.; Cappello, D.; Spataro, M.; Giuffrida, G. Kidney transplantation from cadaveric donors unsuitable for other centers and older than 60 years of age. Transplant. Proc. 2005, 37, 2451–2453. [Google Scholar] [CrossRef] [PubMed]
- Mesnard, B.; Territo, A.; Campi, R.; Hevia, V.; Andras, I.; Piana, A.; Pecoraro, A.; Boissier, R.; Prudhomme, T. EAU-Young Academic Urologist (YAU) group of Kidney Transplantation. Kidney transplantation from elderly donors (>70 years): A systematic review. World J. Urol. 2023, 41, 695–707. [Google Scholar] [CrossRef] [PubMed]
- Corona, D.; Ekser, B.; Gioco, R.; Caruso, M.; Schipa, C.; Veroux, P.; Giaquinta, A.; Granata, A.; Veroux, M. Heme-Oxygenase and Kidney Transplantation: A Potential for Target Therapy? Biomolecules 2020, 10, 840. [Google Scholar] [CrossRef] [PubMed]
- Cooper, M.; Wiseman, A.C.; Doshi, M.D.; Hall, I.E.; Parsons, R.F.; Pastan, S.; Reddy, K.S.; Schold, J.D.; Mohan, S.; Hippen, B.E. Understanding Delayed Graft Function to Improve Organ Utilization and Patient Outcomes: Report of a Scientific Workshop Sponsored by the National Kidney Foundation. Am. J. Kidney Dis. 2023, S0272-638600860-0. [Google Scholar] [CrossRef]
- Schrezenmeier, E.; Müller, M.; Friedersdorff, F.; Khadzhynov, D.; Halleck, F.; Staeck, O.; Dürr, M.; Zhang, K.; Eckardt, K.U.; Budde, K.; et al. Evaluation of severity of delayed graft function in kidney transplant recipients. Nephrol. Dial. Transplant. 2022, 37, 973–981. [Google Scholar] [CrossRef]
- Lapointe, I.; Lachance, J.G.; Noël, R.; Côté, I.; Caumartin, Y.; Agharazii, M.; Houde, I.; Rousseau-Gagnon, M.; Kim, S.J.; De Serres, S.A. Impact of donor age on long-term outcomes after delayed graft function: 10-year follow-up. Transpl. Int. 2013, 26, 162–169. [Google Scholar] [CrossRef]
- Li, M.T.; Ramakrishnan, A.; Yu, M.; Daniel, E.; Sandra, V.; Sanichar, N.; King, K.L.; Stevens, J.S.; Husain, S.A.; Mohan, S. Effects of Delayed Graft Function on Transplant Outcomes: A Meta-analysis. Transplant. Direct. 2023, 9, e1433. [Google Scholar] [CrossRef]
- Swanson, K.J.; Bhattarai, M.; Parajuli, S. Delayed graft function: Current status and future directions. Curr. Opin. Organ. Transplant. 2023, 28, 1–7. [Google Scholar] [CrossRef]
- Feldman, H.I.; Gayner, R.; Berlin, J.A.; Roth, D.A.; Silibovsky, R.; Kushner, S.; Brayman, K.L.; Burns, J.E.; Kobrin, S.M.; Friedman, A.L.; et al. Delayed graft function reduces renal allograft survival independent of acute rejection. Nephrol. Dial. Transplant. 1996, 11, 1306–1313. [Google Scholar] [CrossRef] [PubMed]
- Heylen, L.; Pirenne, J.; Naesens, M.; Sprangers, B.; Jochmans, I. “Time is tissue”-A minireview on the importance of donor nephrectomy, donor hepatectomy, and implantation times in kidney and liver transplantation. Am. J. Transplant. 2021, 21, 2653–2661. [Google Scholar] [CrossRef] [PubMed]
- Quiroga, I.; Mcshane, P.; Koo, D.D.; Gray, D.; Friend, P.J.; Fuggle, S.; Darby, C. Major effects of delayed graft function and cold ischemia time on renal allograft survival. Nephrol. Dial. Transplant. 2006, 21, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Perico, N.; Cattaneo, D.; Sayegh, M.H.; Remuzzi, G. Delayed graft function in kidney transplantation. Lancet 2004, 364, 1814–1827. [Google Scholar] [CrossRef] [PubMed]
- Ponticelli, C.; Reggiani, F.; Moroni, G. Delayed Graft Function in Kidney Transplant: Risk Factors, Consequences and Prevention Strategies. J. Pers. Med. 2022, 12, 1557. [Google Scholar] [CrossRef] [PubMed]
- Salguero, J.; Chamorro, L.; Gómez-Gómez, E.; de Benito, P.; Robles, J.E.; Campos, J.P. Kidney Survival Impact of Delayed Graft Function Depends on Kidney Donor Risk Index: A Single-Center Cohort Study. J. Clin. Med. 2023, 12, 6397. [Google Scholar] [CrossRef] [PubMed]
- Dahmane, D.; Audard, V.; Hiesse, C.; Pessione, F.; Bentaarit, B.; Barrou, B.; Rondeau, E.; Cohen, S.; Lang, P.; Grimbert, P. Retrospective follow-up of transplantation of kidney from marginal donors. Kidney Int. 2006, 69, 532–546. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.T.; Chan, S.; Roberts, J.P.; Feng, S. Expanded criteria donor kidney allocation: Marked decrease in cold ischemia and delayed graft function at a single center. Am. J. Transplant. 2005, 5, 2745–2753. [Google Scholar] [CrossRef]
- Vacher-Coponat, H.; Purgus, R.; Indreis, M.; Moal, V.; Luciani, H.; Lechevallier, E.; Delaporte, V.; Luccioni, A.; Julian, H.; Reviron, D.; et al. Cold ischemia time in renal transplantation is reduced by a timesheet in a French transplant center. Transplantation 2007, 83, 555–561. [Google Scholar] [CrossRef]
- Hollenbeck, M.; Dinter, K.; Torsello, G.; Kock, M.; Willers, R.; Sandmann, W.; Grabensee, B. Prostaglandin E1 reduces the risk of delayed graft function after cadaveric renal transplantation. Nephrol. Dial. Transplant. 1999, 14 (Suppl. S4), 32–33. [Google Scholar] [CrossRef]
- Veroux, P.; Veroux, M.; Macarone, M.; Bonanno, M.G.; Tumminelli, M.G. Efficacy of a novel method of intravenous infusion of the prostaglandin analogue iloprost for the treatment of lower-limb critical ischemia:an open-label, nonrandomized study in two cohorts. Curr. Ther. Res. 2004, 65, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Port, F.K.; Bragg-Gresham, J.L.; Metzger, R.A.; Dykstra, D.M.; Gillespie, B.W.; Young, E.W.; Delmonico, F.L.; Wynn, J.J.; Merion, R.M.; Wolfe, R.A.; et al. Donor characteristics associated with reduced graft survival: An approach to expanding the pool of kidney donors. Transplantation 2002, 74, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Veroux, M.; Zerbo, D.; Basile, G.; Gozzo, C.; Sinagra, N.; Giaquinta, A.; Sanfiorenzo, A.; Veroux, P. Simultaneous Native Nephrectomy and Kidney Transplantation in Patients with Autosomal Dominant Polycystic Kidney Disease. PLoS ONE 2016, 11, e0155481. [Google Scholar] [CrossRef] [PubMed]
- Cavaleri, M.; Veroux, M.; Palermo, F.; Vasile, F.; Mineri, M.; Palumbo, J.; Salemi, L.; Astuto, M.; Murabito, P. Perioperative Goal-Directed Therapy during Kidney Transplantation: An Impact Evaluation on the Major Postoperative Complications. J. Clin. Med. 2019, 8, 80. [Google Scholar] [CrossRef] [PubMed]
- Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- Nita, G.E.; Gopal, J.P.; Khambalia, H.A.; Moinuddin, Z.; van Dellen, D. Kidney Transplantation from Donors With Acute Kidney Injury: Are the Concerns Justified? A Systematic Review and Meta-Analysis. Transpl. Int. 2023, 36, 11232. [Google Scholar] [CrossRef] [PubMed]
- Haas, M.; Loupy, A.; Lefaucheur, C.; Roufosse, C.; Glotz, D.; Seron, D.; Nankivell, B.J.; Halloran, P.F.; Colvin, R.B.; Akalin, E.; et al. The Banff 2017 Kidney Meeting Report: Revised diagnostic criteria for chronic active T cell-mediated rejection, antibody-mediated rejection, and prospects for integrative end points for next-generation clinical trials. Am. J. Transplant. 2018, 18, 293–307. [Google Scholar] [CrossRef]
- Fernández, A.R.; Sánchez-Tarjuelo, R.; Cravedi, P.; Ochando, J.; López-Hoyos, M. Review: Ischemia Reperfusion Injury-A Translational Perspective in Organ Transplantation. Int. J. Mol. Sci. 2020, 21, 8549. [Google Scholar] [CrossRef]
- Browne, B.J.; Holt, C.O.; Emovon, O.E. Delayed graft function may not adversely affect short-term renal allograft outcome. Clin. Transplant. 2003, 17 (Suppl. S9), 35–38. [Google Scholar] [CrossRef]
- Hauet, T.; Goujon, J.M.; Vandewalle, A.; Baumert, H.; Lacoste, L.; Tillement, J.P.; Eugene, M.; Carretier, M. Trimetazidine reduces renal dysfunction by limiting the cold ischemia/reperfusion injury in autotransplanted pig kidneys. J. Am. Soc. Nephrol. 2000, 11, 138–148. [Google Scholar] [CrossRef]
- Emrecan, B.; Tulukoglu, E.; Bozok, S.; Kestelli, M.; Onem, G.; Küpelioglu, A.; Yagdi, S.; Gürbüz, A. Effects of iloprost and pentoxifylline in renal ischemia reperfusion in rabbit model. Eur. J. Med. Res. 2006, 11, 295–299. [Google Scholar] [PubMed]
- Aytacoglu, B.N.; Sucu, N.; Tamer, L.; Polat, A.; Gul, A.; Degirmenci, U.; Mavioglu, I.; Dikmengil, M. Iloprost for the attenuation of ischaemia/reperfusion injury in a distant organ. Cell Biochem. Funct. 2006, 24, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Neumayer, H.H.; Schreiber, M.; Wagner, K. Prevention of delayed graft function in cadaveric kidney transplants by the calcium antagonist diltiazem and the prostacyclin-analogue iloprost. Outcome of a prospective randomized clinical trial. Prog. Clin. Biol. Res. 1989, 301, 289–295. [Google Scholar] [PubMed]
- Kassis, H.M.; Minsinger, K.D.; McCullough, P.A.; Block, C.A.; Sidhu, M.S.; Brown, J.R. A Review of the Use of Iloprost, A Synthetic Prostacyclin, in the Prevention of Radiocontrast Nephropathy in Patients Undergoing Coronary Angiography and Intervention. Clin. Cardiol. 2015, 38, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Hansen, J.M.; Christensen, N.J.; Fogh-Andersen, N.; Strandgaard, S. Effects of the prostacyclin analogue iloprost on cyclosporine-induced renal hypoperfusion in stable renal transplant recipients. Nephrol. Dial. Transplant. 1996, 11, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Corona, D.; Mistretta, A.; Zerbo, D.; Sinagra, N.; Giaquinta, A.; Cimino, S.; Ekser, B.; Giuffrida, G.; Leonardi, A.; et al. Delayed graft function and long-term outcome in kidney transplantation. Transplant. Proc. 2012, 44, 1879–1883. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| DGF (n = 172) | No DGF (n = 304) | p Value | |
|---|---|---|---|
| Mean Donor’s age (year) | 57.2 ± 15.8 | 47.1 ± 18.8 | <0.001 |
| Donor’s age | |||
| <55 years | 76 (44.1) | 191 (62.8) | 0.032 |
| 66–70 years | 49 (28.4) | 77 (25.3) | 0.543 |
| >70 years | 47 (27.3) | 36 (11.8) | <0.001 |
| Donors with AKI | 41 (23.8) | 38 (12.5) | 0.001 |
| Female Donor | 75 (43.6) | 155 (50.9) | 0.121 |
| Use of vasopressors | 165(95.9) | 285 (93.7) | 0.744 |
| Stay in ICU | 5.4 ± 4.0 | 4.9 ± 3.9 | 0.251 |
| Mean Cold Ischemia time (min) | 1070 ± 450 | 882 ± 331 | <0.001 |
| Cold ischemia time | |||
| <24 h | 132 (76.7) | 270 (88.9) | 0.635 |
| >24 h | 40 (23.3) | 34 (11.1) | <0.001 |
| i | 52.9 ± 11.4 | 46.0 ± 11.9 | <0.001 |
| Male recipients (%) | 110 (63.9) | 193 (63.4) | 0.884 |
| Recipient’s Hypotension | 30 (17.4) | 12 (3.9) | <0.001 |
| Waiting list (months) | 24.4 ± 21.2 | 16.5 ± 14.4 | 0.001 |
| Time on dialysis (months) | 65.0 ± 50.8 | 39.9 ± 32.7 | <0.001 |
| Characteristics | OR | 95% CI | p Value |
|---|---|---|---|
| Donor age | |||
| Donor age < 70 years | reference | ||
| Donors age > 70 years | 2.50 | 1.40–3.05 | <0.001 |
| Cold ischemia time | |||
| <24 h | reference | ||
| >24 h | 2.60 | 1.50–4.51 | <0.001 |
| Donors with AKI | 2.71 | 1.61–4.52 | 0.021 |
| Time on dialysis | |||
| <12 months | reference | ||
| 12–24 months | 1.01 | 0.66–1.56 | 0.908 |
| >24 months | 2.87 | 1.91–4.33 | <0.001 |
| Recipient age > 60 years | 3.39 | 2.14–5.38 | <0.001 |
| Recipient’s hypotension | 5.06 | 2.52–10.1 | <0.001 |
| Group and Characteristics | Treatment Group (n = 238) | Control Group (n = 238) | p Value |
|---|---|---|---|
| Donor | |||
| Age (year) | 50.9 ± 20.4 | 50.7± 19.8 | 0.845 |
| Male Sex (%) | 91 (38.2) | 69 (28.9) | 0.032 |
| Terminal Serum Creatinine (mg/dL) | 1.13 ± 0.3 | 1.11 ± 0.3 | 0.532 |
| Use of vasoactive amines (%) | 200 (84%) | 203 (85.2) | 0.624 |
| Diabetes (%) | 18 (7.5) | 13 (5.4) | 0.223 |
| Arterial Hypertension > 10 years (%) | 95 (39.9) | 92 (38.6) | 0.498 |
| Cold Ischemia Time (h) | 17.3 ± 7.4 | 13.8 ± 6.2 | <0.001 |
| Cerebral hemorrhage/ischemia brain death (%) | 141 (59.2) | 158 (66.3) | 0.147 |
| Non-traumatic brain death (%) | 93 (39) | 78 (32.7) | 0.122 |
| Other cause of brain death | 4 (1.6) | 2 (0.8) | 0.554 |
| Use of vasoamine drugs | 225 (94.5) | 228 (95.7) | 0.922 |
| Stay in ICU | 4.9 ± 3.8 | 5.3 ± 4.2 | 0.279 |
| Recipient | |||
| Age (year) | 49 ± 11.1 | 47.9 ± 12 | 0.324 |
| Male sex (%) | 159 (66.8) | 142 (59.6) | 0.424 |
| Pre-transplant Panel-Reactive Antibody (%) | 25 ± 10.2 | 21 ± 9.7 | 0.723 |
| Time on Dialysis (mo) | 50 ± 23.4 | 47.1 ± 26.2 | 0.113 |
| Time on waiting list (mo) | 23.9 ± 33 | 15 ± 16 | <0.001 |
| Peritoneal dialysis (%) | 5 (2.1) | 9 (3.7) | 0.433 |
| Dual transplant (%) | 17 (7.1) | 11 (4.6) | 0.115 |
| HCV seropositivity | 36 (15.1) | 11(4.6) | <0.05 |
| Delayed graft function (%) | 51 (21.4) | 121 (50.9) | <0.001 |
| Discontinuation of dialysis (day) | 10.5 ± 8.3 | 13.4 ± 6.7 | 0.016 |
| Primary Non-Function (%) | 6 (2.5%) | 6(2.5%) | 1 |
| Acute rejection | 16 (6.7) | 25 (10.5) | 0.141 |
| Immunosuppression | |||
| Induction (basiliximab) | 68 (28.5) | 55 (23.1) | 0.753 |
| Induction (thymoglobuline) | 22 (9.2) | 24 (10) | 0.883 |
| Tacrolimus | 150 (63) | 164 (68.9) | 0.214 |
| MMF | 205 (86.1) | 185 (77.7) | 0.301 |
| Sirolimus | 36 (15.1) | 26 (10.9) | 0.112 |
| Cyclosporine | 29 (12.1) | 55 (23.1) | 0.108 |
| Everolimus | 14 (5.8) | 19 (7.9) | 0.323 |
| Hospital stay | 10.5 ± 4.4 | 13.3 ± 6.4 | <0.05 |
| 30-day acute rejection | 22 (9.2) | 25 (10.5) | 0.212 |
| Postoperative Death (30-day) | 3 (1.2) | 4 (0.8) | 0.823 |
| 1 year Serum Creatinine (mg/dL) | 1.41 ± 0.61 | 1.60 ± 0.65 | 0.008 |
| 5 years Serum Creatinine (mg/dL) | 1.50 ± 0.62 | 1.66 ± 0.81 | 0.045 |
| 10 years Serum Creatinine (mg/dL) | 1.54 ± 0.76 | 1.64 ± 0.55 | 0.525 |
| 1-year eGlomerular Filtration Rate (mL/min per 1.73 m2) | 67 ± 15.8 | 59 ± 12.4 | 0.012 |
| 5-year eGlomerular Filtration Rate (mL/min per 1.73 m2) | 63 ± 13.4 | 56 ± 11.8 | 0.048 |
| 10-year eGlomerular Filtration Rate (mL/min per 1.73 m2) | 61 ± 18.4 | 55 ± 12.4 | 0.633 |
| 1 year Graft Survival | 93.3% | 92% | <0.05 |
| 5 years Graft Survival | 83% | 83.7% | <0.05 |
| 10 years Graft Survival | 75% | 74% | 0.183 |
| 1 year Patient Survival | 96.7% | 92.1% | 0.185 |
| 5 years Patient Survival | 96.3% | 93.7% | 0.211 |
| 10 years patient Survival | 80% | 77% | 0.172 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veroux, M.; Sanfilippo, F.; Roscitano, G.; Giambra, M.; Giaquinta, A.; Riccioli, G.; Zerbo, D.; Corona, D.; Sorbello, M.; Veroux, P. Prevention of Delayed Graft Function in Kidney Transplant Recipients through a Continuous Infusion of the Prostaglandin Analogue Iloprost: A Single-Center Prospective Study. Biomedicines 2024, 12, 290. https://doi.org/10.3390/biomedicines12020290
Veroux M, Sanfilippo F, Roscitano G, Giambra M, Giaquinta A, Riccioli G, Zerbo D, Corona D, Sorbello M, Veroux P. Prevention of Delayed Graft Function in Kidney Transplant Recipients through a Continuous Infusion of the Prostaglandin Analogue Iloprost: A Single-Center Prospective Study. Biomedicines. 2024; 12(2):290. https://doi.org/10.3390/biomedicines12020290
Chicago/Turabian StyleVeroux, Massimiliano, Floriana Sanfilippo, Giuseppe Roscitano, Martina Giambra, Alessia Giaquinta, Giordana Riccioli, Domenico Zerbo, Daniela Corona, Massimiliano Sorbello, and Pierfrancesco Veroux. 2024. "Prevention of Delayed Graft Function in Kidney Transplant Recipients through a Continuous Infusion of the Prostaglandin Analogue Iloprost: A Single-Center Prospective Study" Biomedicines 12, no. 2: 290. https://doi.org/10.3390/biomedicines12020290