
Optimal Volume Assessment for Serous Fluid Cytology

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients’ Selection
2.2. Specimen Processing
2.3. Reports’ Categorization
- ND: Non-diagnostic specimen.
- NFM: Specimens with clearly benign characteristics.
- AUS: Specimens containing cells exhibiting some degree of atypia, lacking definitive features of malignancy, and often leaning towards benignity with atypia attributed to inflammation.
- SFM: Cases with atypical cells strongly resembling malignant ones, but without enough atypia or a sufficient number of atypical cells to warrant a malignant diagnosis.
- MAL: Specimens containing unequivocally malignant cells.
2.4. Statistical Analysis
3. Results
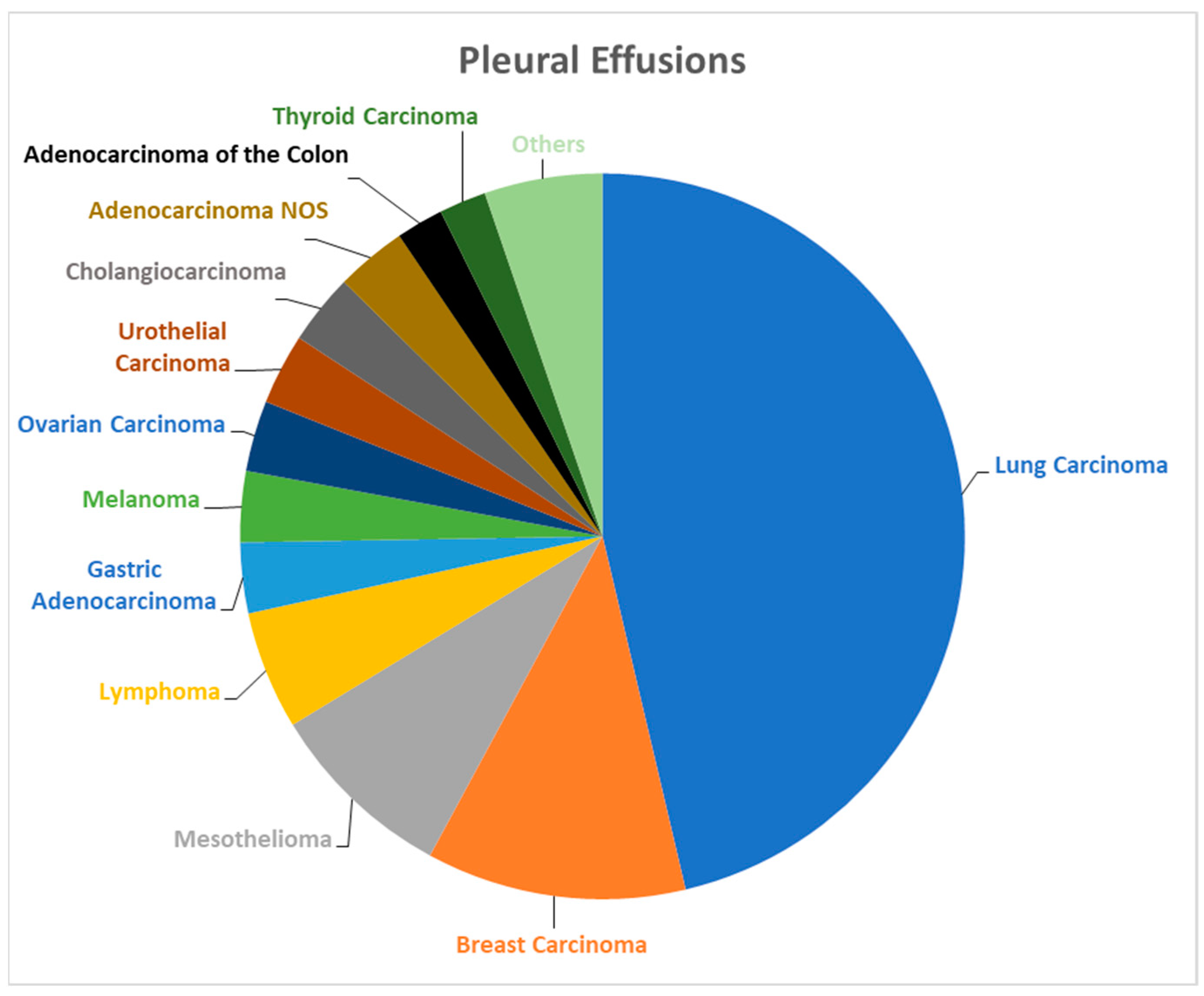
3.1. Pleural Effusions
3.2. Peritoneal Effusions
3.3. Pericardial Effusions
3.4. Optimal Volume Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Michael, C.W. Serous fluid cytopathology: Past, present, and future. Diagn. Cytopathol. 2021, 49, 577–581. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, E.F.; Pastorello, R.; Morris, P.; Saieg, M.; Chowsilpa, S.; Maleki, Z. Suspicious for Malignancy Diagnoses on Pleural Effusion Cytology. Am. J. Clin. Pathol. 2020, 154, 394–402. [Google Scholar] [CrossRef] [PubMed]
- Murali, R.; Park, K.; Leslie, K.O. The Pleura in Health and Disease. Semin. Respir. Crit. Care Med. 2010, 31, 649–673. [Google Scholar] [CrossRef] [PubMed]
- Porcel, J.M.; Light, R.W. Diagnostic approach to pleural effusion in adults. Am. Fam. Physician 2006, 73, 1211–1220. [Google Scholar] [PubMed]
- Siddiqui, M.T. Serous cavity fluids: Momentum, molecules, markers... and more! Cancer Cytopathol. 2020, 128, 381–383. [Google Scholar] [CrossRef]
- Al Shaikh, S.; Lapadat, R.; Do, M.K.A.; Mehrotra, S.; Barkan, G.A.; Wojcik, E.M.; Pambuccian, S.E. The utilization and utility of immunostains in body fluid cytology. Cancer Cytopathol. 2020, 128, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Nayar, R.; Wilbur, D.C. The Bethesda System for Reporting Cervical Cytology: A Historical Perspective. Acta Cytol. 2017, 61, 359–372. [Google Scholar] [CrossRef]
- Barkan, G.A.; Wojcik, E.M.; Nayar, R.; Savic-Prince, S.; Quek, M.L.; Kurtycz, D.F.; Rosenthal, D.L. The Paris System for Reporting Urinary Cytology: The quest to develop a standardized terminology. J. Am. Soc. Cytopathol. 2016, 5, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Cibas, E.S.; Ali, S.Z. The 2017 Bethesda System for Reporting Thyroid Cytopathology. Thyroid 2017, 27, 1341–1346. [Google Scholar] [CrossRef]
- Pitman, M.B.; Centeno, B.A.; Ali, S.Z.; Genevay, M.; Stelow, E.; Mino-Kenudson, M.; Castillo, C.F.; Schmidt, C.M.; Brugge, W.; Layfield, L. Standardized terminology and nomenclature for pancreatobiliary cytology: The Papanicolaou Society of Cytopathology guidelines. Diagn. Cytopathol. 2014, 42, 338–350. [Google Scholar] [CrossRef]
- Maleki, Z.; Baloch, Z.; Lu, R.; Shafique, K.; Song, S.J.; Viswanathan, K.; Rao, R.A.; Lefler, H.; Fatima, A.; Wiles, A.; et al. Application of the Milan System for Reporting Submandibular Gland Cytopathology: An international, multi-institutional study. Cancer Cytopathol. 2019, 127, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Field, A.S.; Raymond, W.A.; Rickard, M.; Arnold, L.; Brachtel, E.F.; Chaiwun, B.; Chen, L.; Di Bonito, L.; Kurtycz, D.F.; Lee, A.H.; et al. The International Academy of Cytology Yokohama System for Reporting Breast Fine-Needle Aspiration Biopsy Cytopathology. Acta Cytol. 2019, 63, 257–273. [Google Scholar] [CrossRef] [PubMed]
- Crothers, B.A.; Chandra, A. Proceedings of the American Society of Cytopathology Companion Session at the 2019 United States and Canadian Academy of Pathology Meeting Part 1: Towards an International System for Reporting Serous Fluid Cytopathology. J. Am. Soc. Cytopathol. 2019, 8, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Chandra, A.; Crothers, B.; Kurtycz, D.; Schmitt, F. Announcement: The International System for Reporting Serous Fluid Cytopathology. Acta Cytol. 2019, 63, 349–351. [Google Scholar] [CrossRef] [PubMed]
- Lobo, C.L.; Costa, J.; Petronilho, S.; Monteiro, P.; Leça, L.; Schmitt, F. Cytohistological correlation in serous effusions using the newly proposed International System for Reporting Serous Fluid Cytopathology: Experience of an oncological center. Diagn. Cytopathol. 2021, 49, 596–605. [Google Scholar] [CrossRef] [PubMed]
- Straccia, P.; Chiappetta, M.; Magnini, D.; Cancellieri, A. Application of the International System for Reporting Serous Fluid Cytopathology (TIS): A retrospective institutional study. Cytopathology 2022, 33, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.H.; Liu, C.Y.; Jhuang, J.Y.; Chen, C.C. Comprehensive evaluation of benign and malignant etiologies of different serous effusions with the International System for Reporting Serous Fluid Cytopathology: A multi-institutional study in Taiwan. Cancer Cytopathol. 2023, 132, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Pergaris, A.; Stefanou, D.; Keramari, P.; Sousouris, S.; Kavantzas, N.; Gogas, H.; Mikou, P. Application of the International System for Reporting Serous Fluid Cytopathology with Cytohistological Correlation and Risk of Malignancy Assessment. Diagnostics 2021, 11, 2223. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mikou, P.; Pergaris, A.; Engels, M.; Chandra, A. Review of the impact of the International System for Serous Fluid Cytopathology. Cytopathology 2024, 35, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Sallach, S.M.; Sallach, J.A.; Vasquez, E.; Schultz, L.; Kvale, P. Volume of pleural fluid required for diagnosis of pleural malignancy. Chest 2002, 122, 1913–1917. [Google Scholar] [CrossRef] [PubMed]
- Abouzgheib, W.; Bartter, T.; Dagher, H.; Pratter, M.; Klump, W. A prospective study of the volume of pleural fluid required for accurate diagnosis of malignant pleural effusion. Chest 2009, 135, 999–1001. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Khosla, R.; Rohatgi, P.K.; Chauhan, S.S.; Paal, E.; Chen, W. The minimum volume of pleural fluid required to diagnose malignant pleural effusion: A retrospective study. Lung India 2017, 34, 34–37. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Torous, V.F. How much is enough: Investigation of pleural fluid cytology findings related to sample volume. J. Am. Soc. Cytopathol. 2022, 11, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Coconubo, D.M.; Baskota, S.U.; Li, R.; Srivastava, P.; Cuda, J.; Khader, S. Reassessing the optimal volume for malignancy detection in serous fluid cytology. Cancer Cytopathol. 2022, 130, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Beg, S.; Zanettini, C.; Queiroz, L.; Marchionni, L.; Alperstein, S.A.; Siddiqui, M.T. Optimal fluid volume for detecting malignancy in serous effusions: A single institution experience. J. Am. Soc. Cytopathol. 2023, 12, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Rooper, L.M.; Ali, S.Z.; Olson, M.T. A minimum fluid volume of 75 mL is needed to ensure adequacy in a pleural effusion: A retrospective analysis of 2540 cases. Cancer Cytopathol. 2014, 122, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Jha, S.; Sethy, M.; Sharma, G.; Adhya, A.K. Adequacy in pleural effusion: What is the minimum volume required for detection of malignant cells? Diagn. Cytopathol. 2022, 50, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.C.; Davidson, L.R.; McKean, M.E. An investigation of adequate volume for the diagnosis of malignancy in pleural fluids. Cytopathology 2011, 22, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Swiderek, J.; Morcos, S.; Donthireddy, V.; Surapaneni, R.; Jackson-Thompson, V.; Schultz, L.; Kini, S.; Kvale, P. Prospective study to determine the volume of pleural fluid required to diagnose malignancy. Chest 2010, 137, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Feng, Z.; Zhang, Y.; Liu, Z.; Sun, X.; Jin, S. Determination of the optimal volume of ascitic fluid for the precise diagnosis of malignant ascites. Saudi J. Gastroenterol. 2019, 25, 327–332. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rooper, L.M.; Ali, S.Z.; Olson, M.T. A specimen volume of ≥80 mL improves cytologic sensitivity for malignant ascites: A retrospective analysis of 2665 cases. J. Am. Soc. Cytopathol. 2016, 5, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Rooper, L.M.; Ali, S.Z.; Olson, M.T. A Minimum Volume of More Than 60 mL Is Necessary for Adequate Cytologic Diagnosis of Malignant Pericardial Effusions. Am. J. Clin. Pathol. 2016, 145, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Dragoescu, E.A.; Liu, L. Pericardial fluid cytology: An analysis of 128 specimens over a 6-year period. Cancer Cytopathol. 2013, 121, 242–251. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ND | NFM | AUS | SFM | MAL | Total | |
|---|---|---|---|---|---|---|
| Peritoneal | 15 (2.14%) | 484 (69.14%) | 21 (3%) | 20 (2.86%) | 160 (22.86%) | 700 |
| Pleural | 66 (4.14%) | 1228 (77.04%) | 39 (2.45%) | 51 (3.2%) | 210 (13.17%) | 1594 |
| Pericardial | 5 (10.87%) | 27 (58.7%) | 0 (0%) | 1 (2.17%) | 13 (28.26%) | 46 |
| Diagnostic Category | Gender | Age (Years) | Volume (mL) | ICC | Histology Reports | |
|---|---|---|---|---|---|---|
| ND (n = 66) | M: 39 | F: 27 | Min: 11 | Min: 1 | 0 | 24 |
| Max: 91 | Max: 10 | |||||
| Ave: 72.4 | Ave: 5.33 | |||||
| NFM (n = 1228) | M: 712 | F: 516 | Min: 18 | Min: 0.5 | 28 | 525 |
| Max: 95 | Max: 1600 | |||||
| Ave: 69.37 | Ave: 182 | |||||
| AUS (n = 39) | M: 10 | F: 29 | Min: 60 | Min: 0.5 | 7 | 16 |
| Max: 83 | Max: 50 | |||||
| Ave: 75 | Ave: 19.38 | |||||
| SFM (n = 51) | M: 33 | F: 18 | Min: 55 | Min: 3 | 15 | 40 |
| Max: 91 | Max: 700 | |||||
| Ave: 70.2 | Ave: 125.57 | |||||
| MAL (n = 210) | M: 99 | F: 111 | Min: 45 | Min: 0.5 | 126 | 107 |
| Max: 95 | Max: 1400 | |||||
| Ave: 74.3 | Ave: 206.5 | |||||
| Total (n = 1594) | M: 893 | F: 701 | Min: 11 | Min: 0.5 | 176 | 712 |
| Max: 95 | Max: 1600 | |||||
| Ave: 70.92 | Ave: 173.75 | |||||
| Diagnostic Category | Gender | Age (Years) | Volume (mL) | ICC | Histology Reports | |
|---|---|---|---|---|---|---|
| ND (n = 15) | M: 10 | F: 5 | Min: 37 | Min: 3 | 0 | 4 |
| Max: 88 | Max: 20 | |||||
| Ave: 67.75 | Ave: 8.7 | |||||
| NFM (n = 484) | M: 262 | F: 222 | Min: 16 | Min: 0.5 | 28 | 240 |
| Max: 89 | Max: 2400 | |||||
| Ave: 66.47 | Ave: 230.44 | |||||
| AUS (n = 21) | M: 11 | F: 10 | Min: 42 | Min: 5 | 3 | 11 |
| Max: 85 | Max: 500 | |||||
| Ave: 64.6 | Ave: 133.2 | |||||
| SFM (n = 20) | M: 11 | F: 9 | Min: 55 | Min: 3 | 3 | 17 |
| Max: 87 | Max: 100 | |||||
| Ave: 70 | Ave: 36.5 | |||||
| MAL (n = 160) | M: 54 | F: 106 | Min: 35 | Min: 1 | 54 | 91 |
| Max: 93 | Max: 2000 | |||||
| Ave: 70.38 | Ave: 245.2 | |||||
| Total (n = 700) | M: 348 | F: 352 | Min: 16 | Min: 0.2 | 69 | 363 |
| Max: 93 | Max: 2400 | |||||
| Ave: 67.6 | Ave: 234.72 | |||||
| Diagnostic Category | Gender | Age (Years) | ICC | Histology Reports | |
|---|---|---|---|---|---|
| ND (n = 5) | M: 1 | F: 4 | Min: 54 | 0 | 0 |
| Max: 81 | |||||
| Ave: 71.2 | |||||
| NFM (n = 27) | M: 14 | F: 13 | Min: 25 | 0 | 14 |
| Max: 79 | |||||
| Ave: 55.4 | |||||
| AUS (n = 0) | M: - | F: - | Min: - | 0 | 0 |
| Max: - | |||||
| Ave: - | |||||
| SFM (n = 1) | M: 0 | F: 1 | Min: 78 | 0 | 0 |
| Max: 78 | |||||
| Ave: 78 | |||||
| MAL (n = 13) | M: 12 | F: 1 | Min: 50 | 12 | 5 |
| Max: 82 | |||||
| Ave: 66.61 | |||||
| Total (n = 46) | M: 27 | F: 19 | Min: 25 | 12 | 19 |
| Max: 82 | |||||
| Ave: 60.78 | |||||
| TIS | ND | NFM | AUS | SFM | MAL | Total |
|---|---|---|---|---|---|---|
| <10 mL | 4 (1.1%) | 298 (81.2%) | 9 (2.5%) | 14 (3.8%) | 42 (11.4%) | 367 |
| 10–500 mL | 2 (0.3%) | 563 (77.7%) | 11 (1.5%) | 21 (2.9%) | 128 (17.7%) | 725 |
| >500 mL | 0 (0%) | 68 (76.4%) | 3 (3.4%) | 2 (2.3%) | 16 (17.9%) | 89 |
| Total No. | 6 | 929 | 23 | 37 | 186 | 1181 |
| ND | NFM | AUS | SFM | MAL | Total |
|---|---|---|---|---|---|
| 6 (0.6%) | 773 (79.1%) | 17 (1.7%) | 30 (3.1%) | 151 (15.5%) | 977 |
| Comparison | Z | p.Unadj | p.Adj |
|---|---|---|---|
| 1 AUS–MAL | −1.39 | 0.16 | 1 |
| 2 AUS–ND | 1.51 | 0.13 | 1 |
| 3 MAL–ND | 2.46 | 0.01 | 0.14 |
| 4 AUS–NFM | −0.39 | 0.7 | 1 |
| 5 MAL–NFM | 2.9 | 0 | 0.04 |
| 6 ND–NFM | −1.92 | 0.06 | 0.55 |
| 7 AUS–SFM | −0.42 | 0.68 | 1 |
| 8 MAL–SFM | 1.15 | 0.25 | 1 |
| 9 ND–SFM | −1.85 | 0.06 | 0.65 |
| 10 NFM–SFM | −0.16 | 0.87 | 1 |
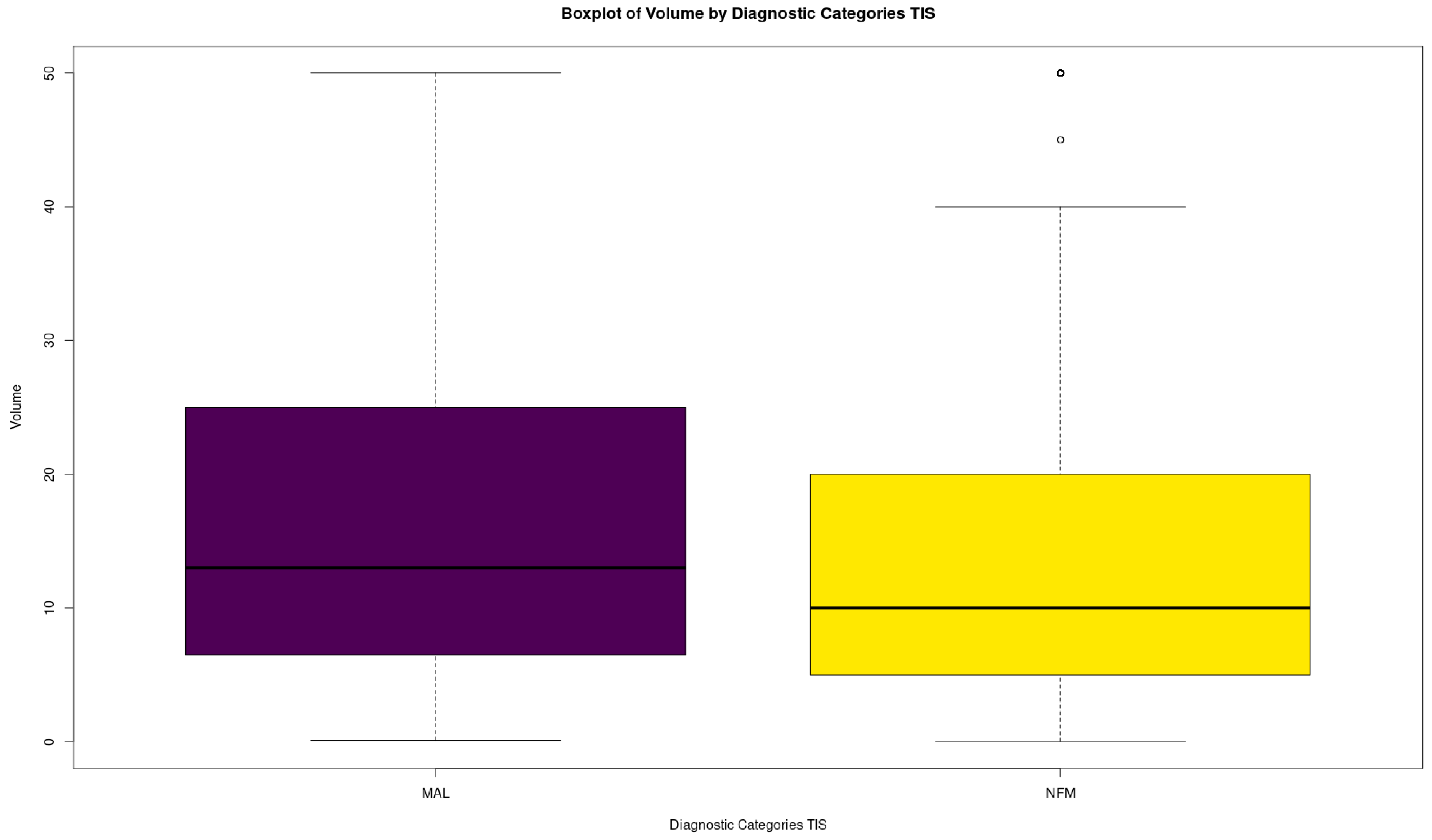
| Min. | 1st Qu. | Median | Mean | 3rd Qu. | Max. | |
|---|---|---|---|---|---|---|
| MAL | 0.10 | 6.50 | 13.00 | 18.94 | 25.00 | 50.00 |
| NFM | 0.01 | 5.00 | 10.00 | 14.60 | 20.00 | 50.00 |
| Comparison | Z | p.Unadj | p.Adj |
|---|---|---|---|
| 1 MAL–NFM | 3.055861 | 0 | 0.01 |
| 2 MAL–UNCERTAIN | 2.750022 | 0.01 | 0.02 |
| 3 NFM–UNCERTAIN | 1.177339 | 0.24 | 0.72 |
| Min. | 1st Qu. | Median | Mean | 3rd Qu. | Max. | |
|---|---|---|---|---|---|---|
| MAL | 0.10 | 6.50 | 13.00 | 18.94 | 25.00 | 50.00 |
| NFM | 0.01 | 5.00 | 10.00 | 14.60 | 20.00 | 50.00 |
| UNCERTAIN | 0.20 | 5.00 | 7.00 | 13.79 | 20.00 | 50.00 |
| Min. | 1st Qu. | Median | Mean | 3rd Qu. | Max. | |
|---|---|---|---|---|---|---|
| MAL | 0.10 | 6.50 | 13.00 | 18.94 | 25.00 | 50.00 |
| NOT MAL | 0.01 | 5.00 | 10.00 | 14.54 | 20.00 | 50.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Christofidis, K.; Theochari, M.; Mavropoulos Papoudas, S.; Kiohou, L.; Sousouris, S.; Dimitriadou, A.; Volakakis, N.; Maounis, N.; Mikou, P. Optimal Volume Assessment for Serous Fluid Cytology. Biomedicines 2024, 12, 899. https://doi.org/10.3390/biomedicines12040899
Christofidis K, Theochari M, Mavropoulos Papoudas S, Kiohou L, Sousouris S, Dimitriadou A, Volakakis N, Maounis N, Mikou P. Optimal Volume Assessment for Serous Fluid Cytology. Biomedicines. 2024; 12(4):899. https://doi.org/10.3390/biomedicines12040899
Chicago/Turabian StyleChristofidis, Konstantinos, Maria Theochari, Stylianos Mavropoulos Papoudas, Lamprini Kiohou, Stylianos Sousouris, Areti Dimitriadou, Nikolaos Volakakis, Nicoletta Maounis, and Panagiota Mikou. 2024. "Optimal Volume Assessment for Serous Fluid Cytology" Biomedicines 12, no. 4: 899. https://doi.org/10.3390/biomedicines12040899