
The Effects of Volatile Anesthetics on Renal Sympathetic and Phrenic Nerve Activity during Acute Intermittent Hypoxia in Rats

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
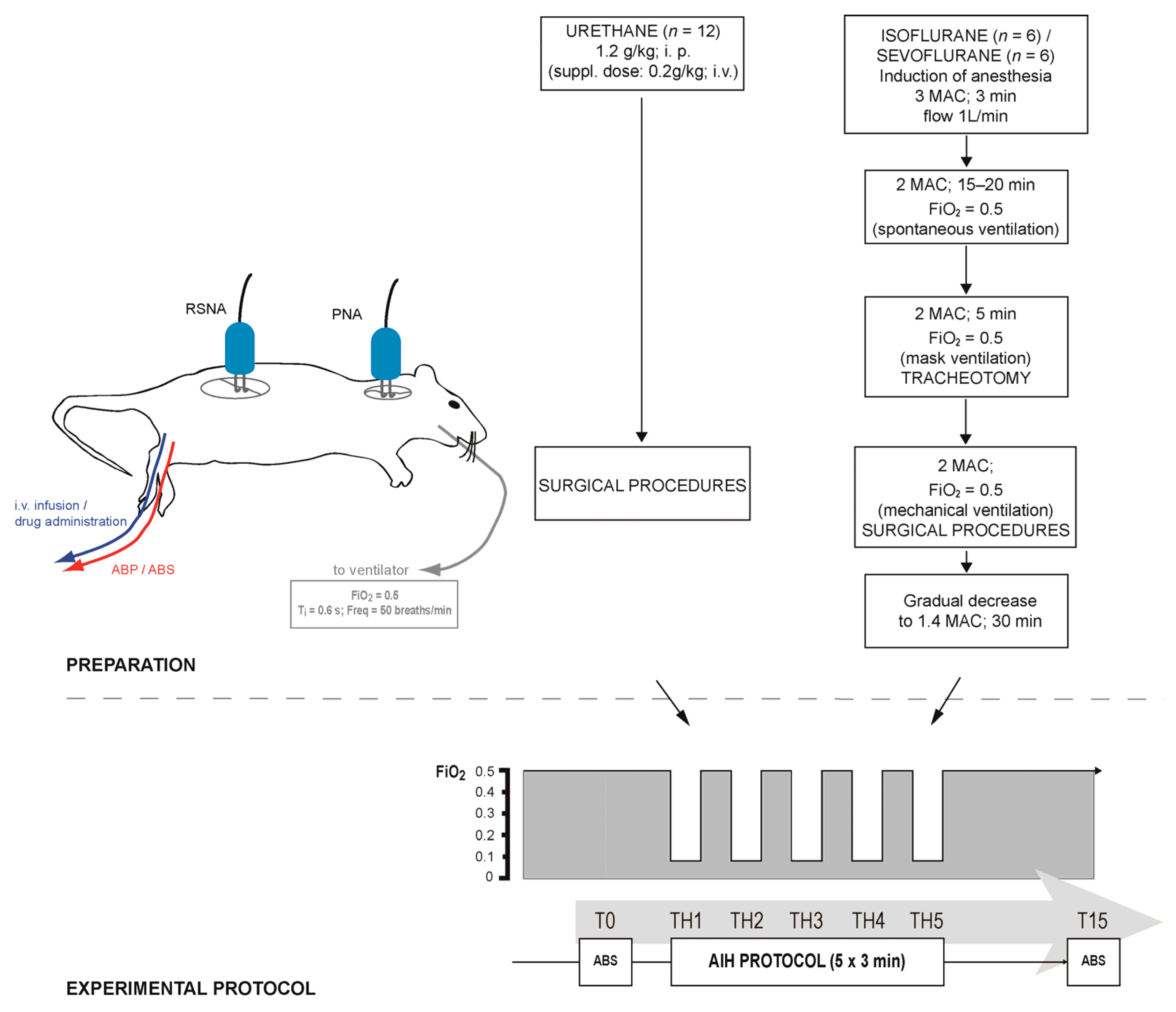
2.1. General Procedures
2.2. Recording Parameters
2.3. Acute Intermittent Hypoxia Protocol
2.4. Data Analysis
2.5. Statistical Analysis
3. Results
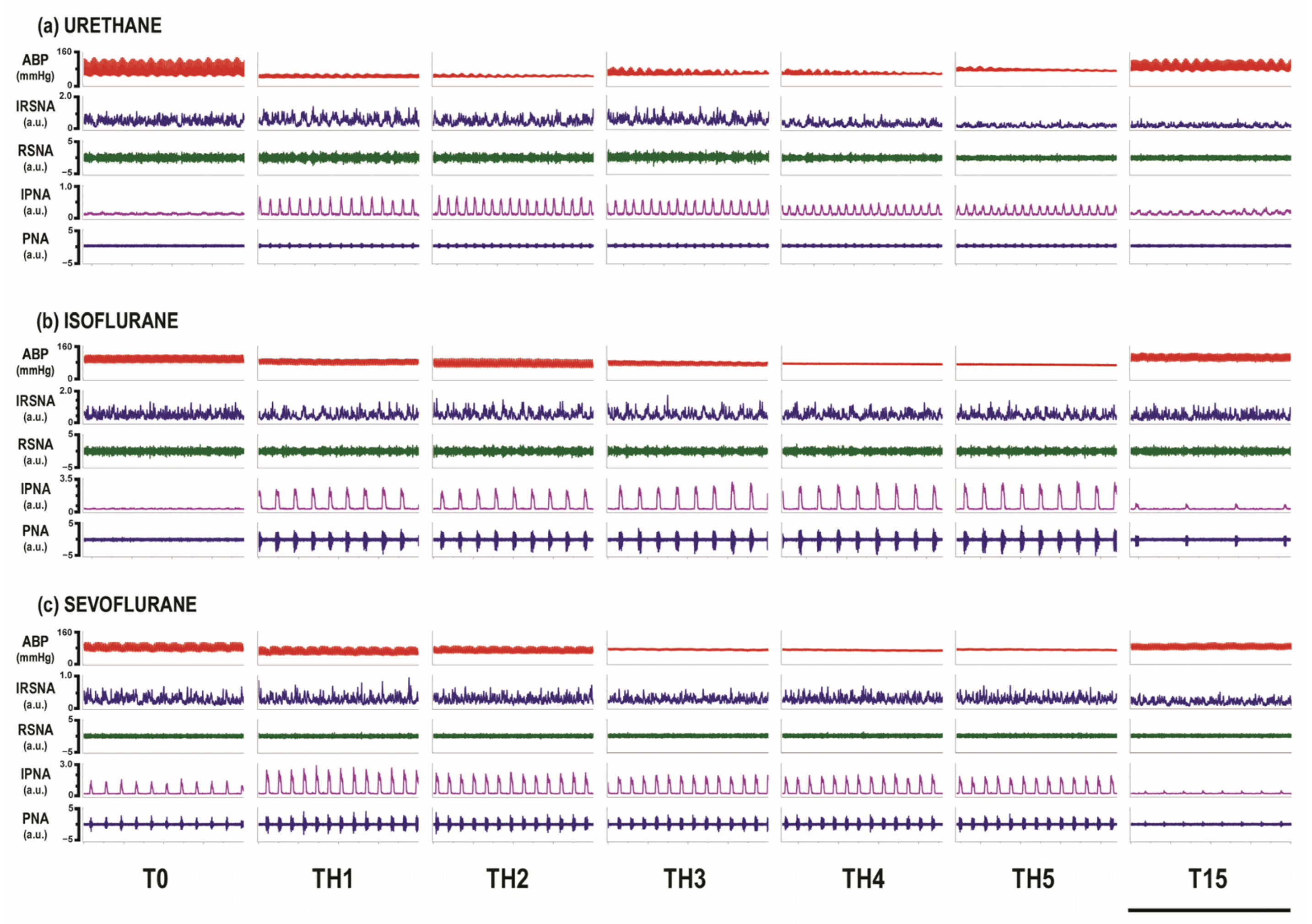
3.1. Overall Activity of Renal Sympathetic and Phrenic Nerves
3.2. Activity of RSNA and PNA at the Baseline and during the First Hypoxic Challenge
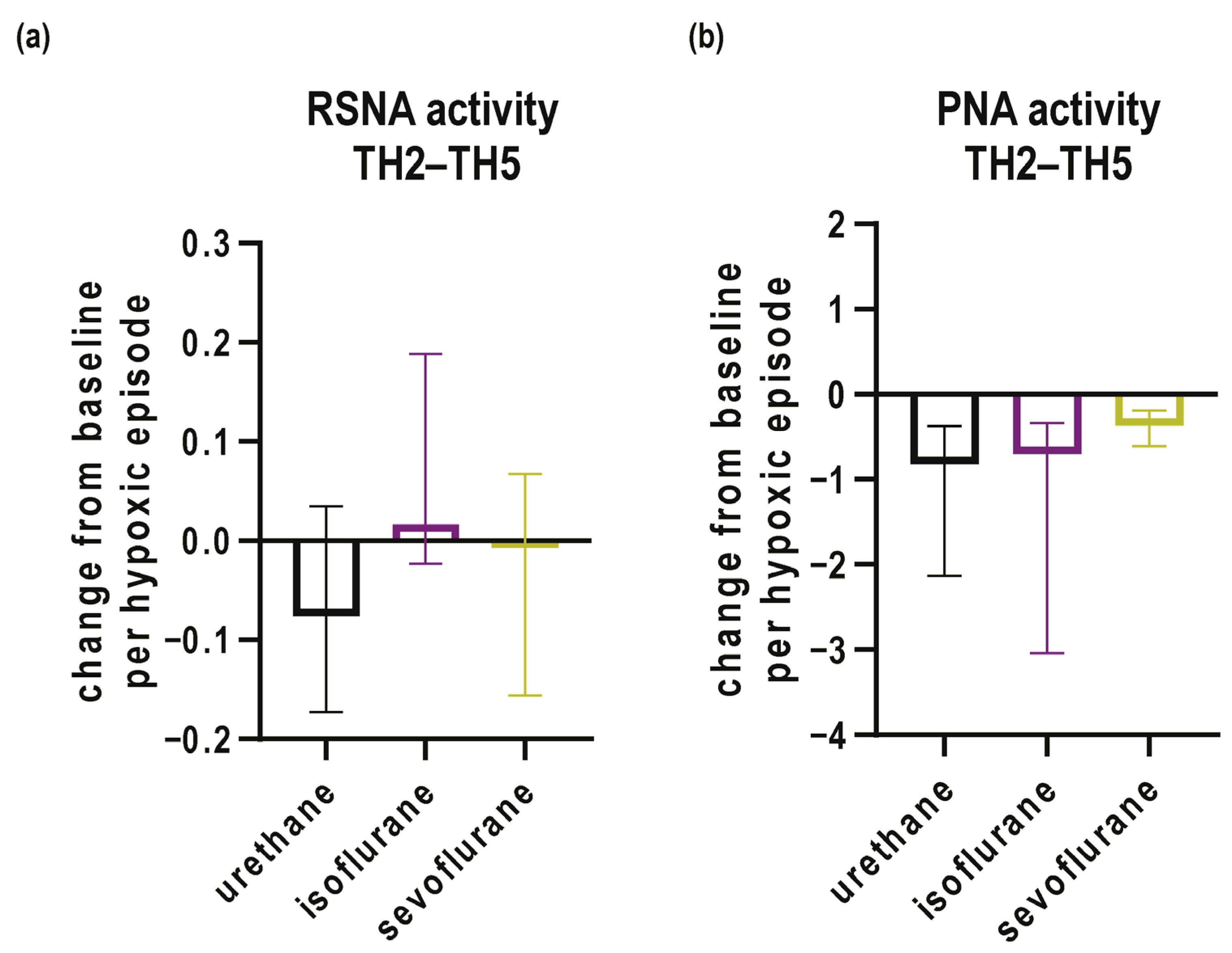
3.3. Activity of RSNA and PNA during Subsequent Episodes of Hypoxia and Recovery
3.4. Mean Arterial Pressure and Acid–Base Status
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gulyaeva, N.V. Molecular Mechanisms of Neuroplasticity: An Expanding Universe. Biochemistry 2017, 82, 237–242. [Google Scholar] [CrossRef]
- Mitchell, G.S.; Johnson, S.M. Neuroplasticity in respiratory motor control. J. Appl. Physiol. 2003, 94, 358–374. [Google Scholar] [CrossRef] [PubMed]
- Dick, T.E.; Hsieh, Y.H.; Dhingra, R.R.; Baekey, D.M.; Galan, R.F.; Wehrwein, E.; Morris, K.F. Cardiorespiratory coupling: Common rhythms in cardiac, sympathetic, and respiratory activities. Prog. Brain Res. 2014, 209, 191–205. [Google Scholar] [PubMed]
- Dick, T.E.; Hsieh, Y.H.; Wang, N.; Prabhakar, N. Acute intermittent hypoxia increases both phrenic and sympathetic nerve activities in the rat. Exp. Physiol. 2007, 92, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Molkov, Y.I.; Zoccal, D.B.; Baekey, D.M.; Abdala, A.P.; Machado, B.H.; Dick, T.E.; Paton, J.F.; Rybak, I.A. Physiological and pathophysiological interactions between the respiratory central pattern generator and the sympathetic nervous system. Prog. Brain Res. 2014, 212, 1–23. [Google Scholar] [PubMed]
- Puri, S.; Panza, G.; Mateika, J.H. A comprehensive review of respiratory, autonomic and cardiovascular responses to intermittent hypoxia in humans. Exp. Neurol. 2021, 341, 113709. [Google Scholar] [CrossRef] [PubMed]
- Baker, T.L.; Mitchell, G.S. Episodic but not continuous hypoxia elicits long-term facilitation of phrenic motor output in rats. J. Physiol. 2000, 529 Pt 1, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Docio, I.; Olea, E.; Prieto, L.J.; Gallego-Martin, T.; Obeso, A.; Gomez-Niño, A.; Rocher, A. Guinea Pig as a Model to Study the Carotid Body Mediated Chronic Intermittent Hypoxia Effects. Front. Physiol. 2018, 9, 694. [Google Scholar] [CrossRef] [PubMed]
- Lemes, E.V.; Aiko, S.; Orbem, C.B.; Formentin, C.; Bassi, M.; Colombari, E.; Zoccal, D.B. Long-term facilitation of expiratory and sympathetic activities following acute intermittent hypoxia in rats. Acta Physiol. 2016, 217, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Mifflin, S.; Cunningham, J.T.; Toney, G.M. Neurogenic mechanisms underlying the rapid onset of sympathetic responses to intermittent hypoxia. J. Appl. Physiol. 2015, 119, 1441–1448. [Google Scholar] [CrossRef] [PubMed]
- Xing, T.; Fong, A.Y.; Bautista, T.G.; Pilowsky, P.M. Acute intermittent hypoxia induced neural plasticity in respiratory motor control. Clin. Exp. Pharmacol. Physiol. 2013, 40, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, E.C.; Lesske, J.; Behm, R.; Miller, C.C., 3rd; Stauss, H.; Unger, T. Carotid chemoreceptors, systemic blood pressure, and chronic episodic hypoxia mimicking sleep apnea. J. Appl. Physiol. 1992, 72, 1978–1984. [Google Scholar] [CrossRef] [PubMed]
- Farre, R.; Almendros, I.; Martinez-Garcia, M.A.; Gozal, D. Experimental Models to Study End-Organ Morbidity in Sleep Apnea: Lessons Learned and Future Directions. Int. J. Mol. Sci. 2022, 23, 14430. [Google Scholar] [CrossRef] [PubMed]
- Zong, S.; Du, P.; Li, H.; Wang, M.; Xiao, H. Advances in animal models of obstructive sleep apnea. Front. Med. 2023, 10, 988752. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, G.S.; Baker, T.L. Respiratory neuroplasticity: Mechanisms and translational implications of phrenic motor plasticity. Handb. Clin. Neurol. 2022, 188, 409–432. [Google Scholar] [PubMed]
- Dick, T.E.; Hsieh, Y.H.; Morrison, S.; Coles, S.K.; Prabhakar, N. Entrainment pattern between sympathetic and phrenic nerve activities in the Sprague-Dawley rat: Hypoxia-evoked sympathetic activity during expiration. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2004, 286, R1121–R1128. [Google Scholar] [CrossRef] [PubMed]
- Moraes, D.J.; Machado, B.H.; Zoccal, D.B. Coupling of respiratory and sympathetic activities in rats submitted to chronic intermittent hypoxia. Prog. Brain Res. 2014, 212, 25–38. [Google Scholar] [PubMed]
- Brioni, J.D.; Varughese, S.; Ahmed, R.; Bein, B. A clinical review of inhalation anesthesia with sevoflurane: From early research to emerging topics. J. Anesth. 2017, 31, 764–778. [Google Scholar] [CrossRef] [PubMed]
- Dohoo, S.E. Isoflurane as an inhalational anesthetic agent in clinical practice. Can Vet. J. 1990, 31, 847–850. [Google Scholar] [PubMed]
- Ebert, T.J. Inhaled anesthetics. In Clinical Anesthesia, 6th ed.; Barash, P.G., Cullen, B.F., Stoelting, R.K., Cahalan, M.K., Stock, M.C., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2009; pp. 413–443. [Google Scholar]
- Dahan, A. General anesthesia and control of respiration. Semin. Anesth. Perioper. Med. Pain 1996, 15, 328–334. [Google Scholar] [CrossRef]
- Karanovic, N.; Pecotic, R.; Valic, M.; Jeroncic, A.; Carev, M.; Karanovic, S.; Ujevic, A.; Dogas, Z. The acute hypoxic ventilatory response under halothane, isoflurane, and sevoflurane anaesthesia in rats. Anaesthesia 2010, 65, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Marinov, V.; Valic, M.; Pecotic, R.; Karanovic, N.; Pavlinac Dodig, I.; Carev, M.; Valic, Z.; Dogas, Z. Sevoflurane and isoflurane monoanesthesia abolished the phrenic long-term facilitation in rats. Respir. Physiol. Neurobiol. 2013, 189, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Pandit, J.J. The variable effect of low-dose volatile anaesthetics on the acute ventilatory response to hypoxia in humans: A quantitative review. Anaesthesia 2002, 57, 632–643. [Google Scholar] [CrossRef]
- Sjogren, D.; Sollevi, A.; Ebberyd, A.; Lindahl, S.G. Isoflurane anaesthesia (0.6 MAC) and hypoxic ventilatory responses in humans. Acta Anaesthesiol. Scand. 1995, 39, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Ide, T.; Sakurai, Y.; Aono, M.; Nishino, T. Contribution of peripheral chemoreception to the depression of the hypoxic ventilatory response during halothane anesthesia in cats. Anesthesiology 1999, 90, 1084–1091. [Google Scholar] [CrossRef] [PubMed]
- Ebert, T.J.; Harkin, C.P.; Muzi, M. Cardiovascular responses to sevoflurane: A review. Anesth. Analg. 1995, 81, S11–S22. [Google Scholar] [CrossRef] [PubMed]
- Hao, X.; Ou, M.; Zhang, D.; Zhao, W.; Yang, Y.; Liu, J.; Yang, H.; Zhu, T.; Li, Y.; Zhou, C. The Effects of General Anesthetics on Synaptic Transmission. Curr. Neuropharmacol. 2020, 18, 936–965. [Google Scholar] [CrossRef] [PubMed]
- Kotani, N.; Akaike, N. The effects of volatile anesthetics on synaptic and extrasynaptic GABA-induced neurotransmission. Brain Res. Bull. 2013, 93, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Mapelli, J.; Gandolfi, D.; Giuliani, E.; Casali, S.; Congi, L.; Barbieri, A.; D’Angelo, E.; Bigiani, A. The effects of the general anesthetic sevoflurane on neurotransmission: An experimental and computational study. Sci. Rep. 2021, 11, 4335. [Google Scholar] [CrossRef] [PubMed]
- Iguchi, N.; Kosaka, J.; Booth, L.C.; Iguchi, Y.; Evans, R.G.; Bellomo, R.; May, C.N.; Lankadeva, Y.R. Renal perfusion, oxygenation, and sympathetic nerve activity during volatile or intravenous general anaesthesia in sheep. Br. J. Anaesth. 2019, 122, 342–349. [Google Scholar] [CrossRef]
- Ma, D.; Sapsed-Byrne, S.M.; Chakrabarti, M.K.; Whitwam, J.G. Effect of sevoflurane on spontaneous sympathetic activity and baroreflexes in rabbits. Br. J. Anaesth. 1998, 80, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Nagayama, T. Effects of sevoflurane anesthesia and baroreceptor function on renal sympathetic nerve activity in rats. Masui 1990, 39, 210–218. [Google Scholar] [PubMed]
- Okamoto, H.; Hoka, S.; Kawasaki, T.; Okuyama, T.; Takahashi, S. Dose-dependent increases in the renal sympathetic nerve activity during rapid increase in isoflurane concentration in intact, lower airway-deafferented, and baroreceptor-deafferented rabbits. Anesthesiology 1996, 84, 1196–1204. [Google Scholar] [CrossRef] [PubMed]
- Pac-Soo, C.K.; Wang, C.; Chakrabarti, M.K.; Whitwam, J.G. Comparison of the effects of inhalational anaesthetic agents on sympathetic activity in rabbits. Eur. J. Anaesthesiol. 2000, 17, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Seagard, J.L.; Hopp, F.A.; Bosnjak, Z.J.; Osborn, J.L.; Kampine, J.P. Sympathetic efferent nerve activity in conscious and isoflurane-anesthetized dogs. Anesthesiology 1984, 61, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Taavo, M.; Rundgren, M.; Frykholm, P.; Larsson, A.; Franzen, S.; Vargmar, K.; Valarcher, J.F.; DiBona, G.F.; Frithiof, R. Role of Renal Sympathetic Nerve Activity in Volatile Anesthesia’s Effect on Renal Excretory Function. Function 2021, 2, zqab042. [Google Scholar] [CrossRef] [PubMed]
- Taoda, M.; Hashimoto, K.; Karasawa, F.; Satoh, T. The effect of sevoflurane and enflurane on renal sympathetic nerve activity in sinoaortic denerved rabbits. Masui 2000, 49, 1328–1332. [Google Scholar] [PubMed]
- Kashimoto, S.; Furuya, A.; Nonaka, A.; Oguchi, T.; Koshimizu, M.; Kumazawa, T. The minimum alveolar concentration of sevoflurane in rats. Eur. J. Anaesthesiol. 1997, 14, 359–361. [Google Scholar] [CrossRef] [PubMed]
- Mazze, R.I.; Rice, S.A.; Baden, J.M. Halothane, isoflurane, and enflurane MAC in pregnant and nonpregnant female and male mice and rats. Anesthesiology 1985, 62, 339–341. [Google Scholar] [CrossRef] [PubMed]
- Madirazza, K.; Pecotic, R.; Pavlinac Dodig, I.; Valic, M.; Dogas, Z. Hyperoxia blunts renal sympathetic nerve activity response to acute intermittent hypercapnia in rats. J. Physiol. Pharmacol. 2019, 70, 737–746. [Google Scholar]
- Dempsey, J.A.; Veasey, S.C.; Morgan, B.J.; O’Donnell, C.P. Pathophysiology of sleep apnea. Physiol. Rev. 2010, 90, 47–112. [Google Scholar] [CrossRef] [PubMed]
- Iturriaga, R.; Del Rio, R.; Idiaquez, J.; Somers, V.K. Carotid body chemoreceptors, sympathetic neural activation, and cardiometabolic disease. Biol. Res. 2016, 49, 13. [Google Scholar] [CrossRef] [PubMed]
- Carev, M.; Valic, M.; Pecotic, R.; Karanovic, N.; Valic, Z.; Pavlinac, I.; Dogas, Z. Propofol abolished the phrenic long-term facilitation in rats. Respir. Physiol. Neurobiol. 2010, 170, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.H.; Jacono, F.J.; Siegel, R.E.; Dick, T.E. Respiratory modulation of sympathetic activity is attenuated in adult rats conditioned with chronic hypobaric hypoxia. Respir. Physiol. Neurobiol. 2015, 206, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Xing, T.; Pilowsky, P.M. Acute intermittent hypoxia in rat in vivo elicits a robust increase in tonic sympathetic nerve activity that is independent of respiratory drive. J. Physiol. 2010, 588, 3075–3088. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, K.; Lalley, P.; Mifflin, S. Acute intermittent optogenetic stimulation of nucleus tractus solitarius neurons induces sympathetic long-term facilitation. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2015, 308, R266–R275. [Google Scholar] [CrossRef] [PubMed]
- Franzen, S.; DiBona, G.; Frithiof, R. Anesthesia and the renal sympathetic nervous system in perioperative AKI. Semin. Nephrol. 2022, 42, 151283. [Google Scholar] [CrossRef] [PubMed]
- Zoccal, D.B.; Paton, J.F.; Machado, B.H. Do changes in the coupling between respiratory and sympathetic activities contribute to neurogenic hypertension? Clin. Exp. Pharmacol. Physiol. 2009, 36, 1188–1196. [Google Scholar] [CrossRef] [PubMed]
- Takeda, R.; Haji, A. Cellular effects of isoflurane on bulbar respiratory neurons in decerebrate cats. Jpn. J. Pharmacol. 1993, 62, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Takita, K.; Morimoto, Y. Effects of sevoflurane on respiratory rhythm oscillators in the medulla oblongata. Respir. Physiol. Neurobiol. 2010, 173, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Teppema, L.; Sarton, E.; Dahan, A.; Olievier, K. Selective depression of peripheral chemoreflex loop by sevoflurane in lightly anesthetized cats. Adv. Exp. Med. Biol. 1998, 450, 155–158. [Google Scholar] [PubMed]
- Mateika, J.H.; Sandhu, K.S. Experimental protocols and preparations to study respiratory long term facilitation. Respir. Physiol. Neurobiol. 2011, 176, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hara, K.; Harris, R.A. The anesthetic mechanism of urethane: The effects on neurotransmitter-gated ion channels. Anesth. Analg. 2002, 94, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Maggi, C.A.; Meli, A. Suitability of urethane anesthesia for physiopharmacological investigations in various systems. Part 1: General considerations. Experientia 1986, 42, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Morrison, S.F. RVLM and raphe differentially regulate sympathetic outflows to splanchnic and brown adipose tissue. Am. J. Physiol. 1999, 276, R962–R973. [Google Scholar] [CrossRef] [PubMed]
- Takakura, A.C.; Colombari, E.; Menani, J.V.; Moreira, T.S. Ventrolateral medulla mechanisms involved in cardiorespiratory responses to central chemoreceptor activation in rats. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2011, 300, R501–R510. [Google Scholar] [CrossRef]
- Baker, T.L.; Fuller, D.D.; Zabka, A.G.; Mitchell, G.S. Respiratory plasticity: Differential actions of continuous and episodic hypoxia and hypercapnia. Respir. Physiol. 2001, 129, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, C.B.; Cravo, S.L.; Stocker, S.D. Airway obstruction produces widespread sympathoexcitation: Role of hypoxia, carotid chemoreceptors, and NTS neurotransmission. Physiol. Rep. 2018, 6, e13536. [Google Scholar] [CrossRef] [PubMed]
- Stipica, I.; Pavlinac Dodig, I.; Pecotic, R.; Dogas, Z.; Valic, Z.; Valic, M. Periodicity during hypercapnic and hypoxic stimulus is crucial in distinct aspects of phrenic nerve plasticity. Physiol. Res. 2016, 65, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Fink, A.M.; Dean, C. Quantifying Acute Changes in Renal Sympathetic Nerve Activity in Response to Central Nervous System Manipulations in Anesthetized Rats. J. Vis. Exp. 2018, 139, e58205. [Google Scholar]
- Casey, D.P.; Joyner, M.J. Compensatory vasodilatation during hypoxic exercise: Mechanisms responsible for matching oxygen supply to demand. J. Physiol. 2012, 590, 6321–6326. [Google Scholar] [CrossRef] [PubMed]
- Cui, F.; Gao, L.; Yuan, F.; Dong, Z.F.; Zhou, Z.N.; Kline, D.D.; Zhang, Y.; Li, D.P. Hypobaric intermittent hypoxia attenuates hypoxia-induced depressor response. PLoS ONE 2012, 7, e41656. [Google Scholar] [CrossRef] [PubMed]
- Saeki, Y.; Hasegawa, Y.; Shibamoto, T.; Yamaguchi, Y.; Hayashi, T.; Tanaka, S.; Wang, H.G.; Koyama, S. The effects of sevoflurane, enflurane, and isoflurane on baroreceptor-sympathetic reflex in rabbits. Anesth. Analg. 1996, 82, 342–348. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline | AIH Protocol | Recovery | |||||
|---|---|---|---|---|---|---|---|
| Group | T0 | TH1 | TH2 | TH3 | TH4 | TH5 | T15 |
| Urethane | 98.5 ± 3.7 | 81.8 ± 6.8 † | 76.2 ± 6.4 † | 77.2 ± 5.2 *,† | 72.9 ± 5.1 *,† | 72.9 ± 5.6 *,† | 106.2 ± 4.7 |
| Isoflurane | 82.1 ± 5.0 ‡ | 62.3 ± 8.5 | 62.1 ± 7.7 | 61.5 ± 6.1 *,† | 60.5 ± 6.4 *,† | 61.7 ± 5.9 | 87.4 ± 6.4 |
| Sevoflurane | 90.5 ± 2.6 | 73.6 ± 8.9 | 76.5 ± 8.8 | 64.7 ± 10.0 | 69.1 ± 7.6 | 72.9 ± 9.2 | 89.1 ± 4.1 |
| Group | pH | PaCO2 | PaO2 | |||
|---|---|---|---|---|---|---|
| T0 | T15 | T0 | T15 | T0 | T15 | |
| Urethane | 7.300 ± 0.013 | 7.283 ± 0.015 | 52.0 ± 1.7 | 48.3 ± 2.0 * | 263.9 ± 5.9 | 261.6 ± 6.2 |
| Isoflurane | 7.301 ± 0.022 | 7.276 ± 0.025 | 51.4 ± 1.5 | 50.3 ± 1.4 | 277.7 ± 8.9 | 281.3 ± 3.6 |
| Sevoflurane | 7.357 ± 0.029 | 7.356 ± 0.021 | 51.8 ± 1.7 | 49.5 ± 2.6 | 267.4 ± 12.3 | 265.8 ± 13.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krnić, J.; Madirazza, K.; Pecotić, R.; Benzon, B.; Carev, M.; Đogaš, Z. The Effects of Volatile Anesthetics on Renal Sympathetic and Phrenic Nerve Activity during Acute Intermittent Hypoxia in Rats. Biomedicines 2024, 12, 910. https://doi.org/10.3390/biomedicines12040910
Krnić J, Madirazza K, Pecotić R, Benzon B, Carev M, Đogaš Z. The Effects of Volatile Anesthetics on Renal Sympathetic and Phrenic Nerve Activity during Acute Intermittent Hypoxia in Rats. Biomedicines. 2024; 12(4):910. https://doi.org/10.3390/biomedicines12040910
Chicago/Turabian StyleKrnić, Josip, Katarina Madirazza, Renata Pecotić, Benjamin Benzon, Mladen Carev, and Zoran Đogaš. 2024. "The Effects of Volatile Anesthetics on Renal Sympathetic and Phrenic Nerve Activity during Acute Intermittent Hypoxia in Rats" Biomedicines 12, no. 4: 910. https://doi.org/10.3390/biomedicines12040910