
The Association of Chronic Periodontitis as a Potential Risk Factor with Rheumatoid Arthritis: A Nested Case-Control Study Using a Korean National Health Screening Cohort

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
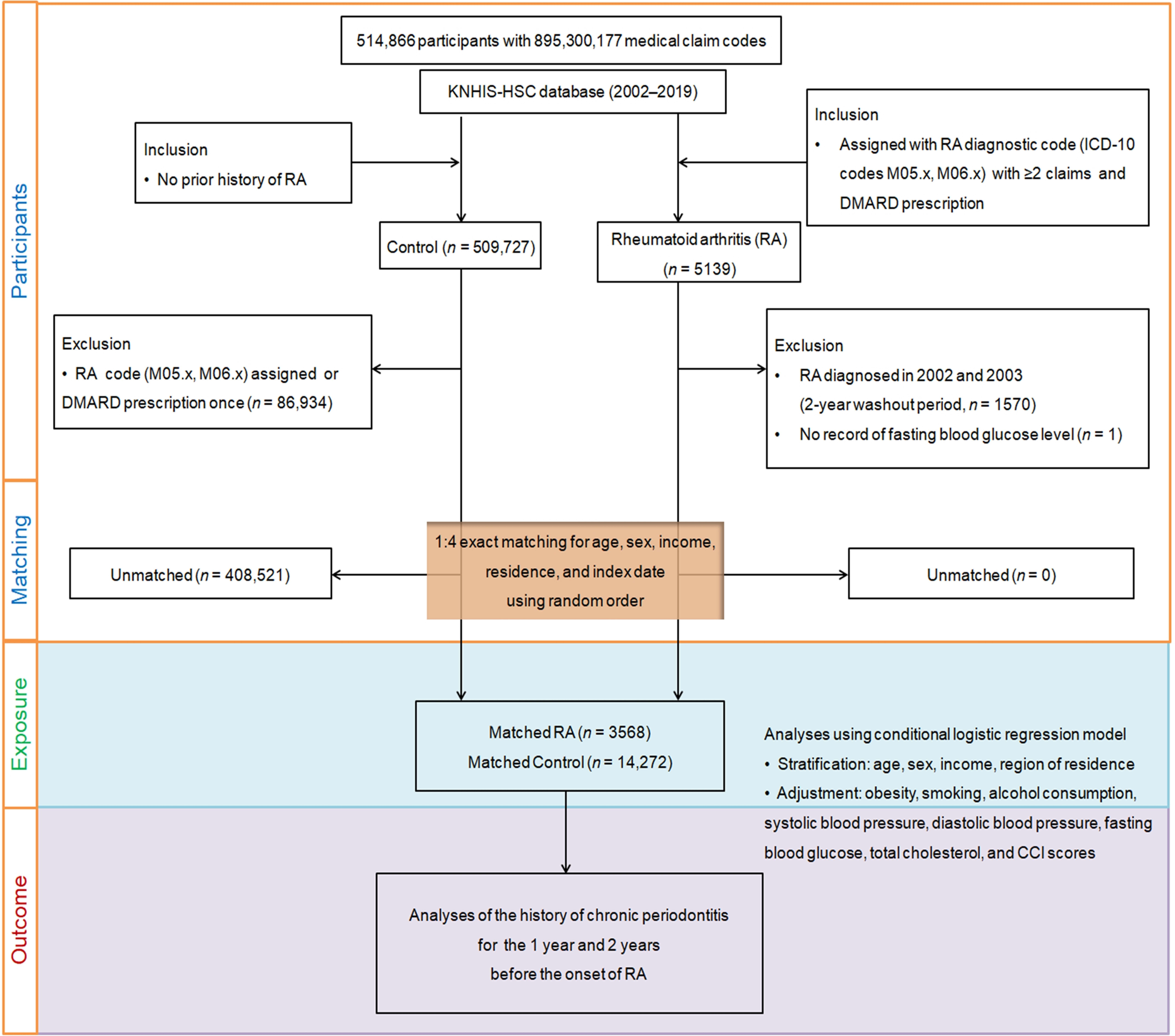
2.1. Research Methodology and Subjects
2.2. Rheumatoid Arthritis (Outcome)
2.3. Chronic Periodontitis (Exposure)
2.4. Covariates
2.5. Statistical Analyses
3. Results
3.1. Baseline Demographics
3.2. RA Odds Ratios in Relation to CP Histories
3.3. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, H.; Sung, Y.-K. Epidemiology of Rheumatoid Arthritis in Korea. J. Rheum. Dis. 2021, 28, 60–67. [Google Scholar] [CrossRef]
- Cross, M.; Smith, E.; Hoy, D.; Carmona, L.; Wolfe, F.; Vos, T.; Williams, B.; Gabriel, S.; Lassere, M.; Johns, N.; et al. The global burden of rheumatoid arthritis: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1316–1322. [Google Scholar] [CrossRef]
- Hur, N.W.; Choi, C.B.; Uhm, W.S.; Bae, S.C. The prevalence and trend of arthritis in Korea: Results from Korea National Health and Nutrition Examination Surveys. J. Korean Rheum. Assoc. 2008, 10, 151–157. [Google Scholar] [CrossRef]
- Safiri, S.; Kolahi, A.A.; Hoy, D.; Smith, E.; Bettampadi, D.; Mansournia, M.A.; Almasi-Hashiani, A.; Ashrafi-Asgarabad, A.; Moradi-Lakeh, M.; Qorbani, M.; et al. Global, regional and national burden of rheumatoid arthritis 1990-2017: A systematic analysis of the Global Burden of Disease study 2017. Ann. Rheum. Dis. 2019, 78, 1463–1471. [Google Scholar] [CrossRef]
- Choi, I.A.; Lee, J.S.; Song, Y.W.; Lee, E.Y. Mortality, disability, and healthcare expenditure of patients with seropositive rheumatoid arthritis in Korea: A nationwide population-based study. PLoS ONE 2019, 14, e0210471. [Google Scholar] [CrossRef]
- Wells, I.; Zemedikun, D.T.; Simons, G.; Stack, R.J.; Mallen, C.D.; Raza, K.; Falahee, M. Predictors of interest in predictive testing for rheumatoid arthritis amongst first degree relatives of rheumatoid arthritis patients. Rheumatology 2021, 61, 3223–3233. [Google Scholar] [CrossRef]
- Venetsanopoulou, A.I.; Alamanos, Y.; Voulgari, P.V.; Drosos, A.A. Epidemiology and Risk Factors for Rheumatoid Arthritis Development. Mediterr. J. Rheumatol. 2023, 34, 404–413. [Google Scholar] [CrossRef]
- Venetsanopoulou, A.I.; Alamanos, Y.; Voulgari, P.V.; Drosos, A.A. Epidemiology of rheumatoid arthritis: Genetic and environmental influences. Expert Rev. Clin. Immunol. 2022, 18, 923–931. [Google Scholar] [CrossRef]
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Jepsen, S.; Jin, L.; Otomo-Corgel, J. Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: A call for global action. J. Clin. Periodontol. 2017, 44, 456–462. [Google Scholar] [CrossRef]
- Yeun, Y.-R.; Kwak, Y.S.; Kim, H.-Y. Association Serum Lipid Levels with Periodontal Disease in Korean Adults Over the Age of 50: The Korea National Health and Nutrition Examination Survey, 2016–2018. Exerc. Sci. 2022, 31, 312–318. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Periodontol. 2018, 89 (Suppl. S1), S1–S8. [Google Scholar] [CrossRef]
- Qiao, Y.; Wang, Z.; Li, Y.; Han, Y.; Zhou, Y.; Cao, X. Rheumatoid arthritis risk in periodontitis patients: A systematic review and meta-analysis. Jt. Bone Spine 2020, 87, 556–564. [Google Scholar] [CrossRef]
- Kobayashi, T.; Bartold, P.M. Periodontitis and periodontopathic bacteria as risk factors for rheumatoid arthritis: A review of the last 10 years. Jpn. Dent. Sci. Rev. 2023, 59, 263–272. [Google Scholar] [CrossRef]
- Bae, S.C.; Lee, Y.H. Causal association between periodontitis and risk of rheumatoid arthritis and systemic lupus erythematosus: A Mendelian randomization. Z. Rheumatol. 2020, 79, 929–936. [Google Scholar] [CrossRef]
- Rajkarnikar, J.; Thomas, B.S.; Rao, S.K. Inter- relationship between rheumatoid arthritis and periodontitis. Kathmandu Univ. Med. J. (KUMJ) 2013, 11, 22–26. [Google Scholar] [CrossRef]
- Oates, T.W.; Graves, D.T.; Cochran, D.L. Clinical, radiographic and biochemical assessment of IL-1/TNF-alpha antagonist inhibition of bone loss in experimental periodontitis. J. Clin. Periodontol. 2002, 29, 137–143. [Google Scholar] [CrossRef]
- Tesser, J.; Fleischmann, R.; Dore, R.; Bennett, R.; Solinger, A.; Joh, T.; Modafferi, D.; Schechtman, J.; Study, G. Concomitant medication use in a large, international, multicenter, placebo controlled trial of anakinra, a recombinant interleukin 1 receptor antagonist, in patients with rheumatoid arthritis. J. Rheumatol. 2004, 31, 649–654. [Google Scholar]
- Mankia, K.; Cheng, Z.; Do, T.; Hunt, L.; Meade, J.; Kang, J.; Clerehugh, V.; Speirs, A.; Tugnait, A.; Hensor, E.M.A.; et al. Prevalence of Periodontal Disease and Periodontopathic Bacteria in Anti-Cyclic Citrullinated Protein Antibody-Positive At-Risk Adults Without Arthritis. JAMA Netw. Open 2019, 2, e195394. [Google Scholar] [CrossRef]
- Huang, Y.; Ni, S. Aggregatibacter Actinomycetemcomitans With Periodontitis and Rheumatoid Arthritis. Int. Dent. J. 2024, 74, 58–65. [Google Scholar] [CrossRef]
- Wu, K.J.; Tu, C.C.; Hu, J.X.; Chu, P.H.; Ma, K.S.; Chiu, H.Y.; Kuo, M.Y.; Tsai, T.F.; Chen, Y.W. Severity of periodontitis and salivary interleukin-1beta are associated with psoriasis involvement. J. Formos. Med. Assoc. 2022, 121, 1908–1916. [Google Scholar] [CrossRef]
- Ma, K.S.; Chiang, C.H.; Chen, Y.W.; Wang, L.T. Correspondence to ‘Bacterial citrullinated epitopes generated by Porphyromonas gingivalis infection-a missing link for ACPA production’. Ann. Rheum. Dis. 2023, 82, e216. [Google Scholar] [CrossRef]
- Svard, A.; Kastbom, A.; Ljungberg, K.R.; Potempa, B.; Potempa, J.; Persson, G.R.; Renvert, S.; Berglund, J.S.; Soderlin, M.K. Antibodies against Porphyromonas gingivalis in serum and saliva and their association with rheumatoid arthritis and periodontitis. Data from two rheumatoid arthritis cohorts in Sweden. Front. Immunol. 2023, 14, 1183194. [Google Scholar] [CrossRef]
- Soderlin, M.K.; Persson, G.R.; Renvert, S.; Sanmartin Berglund, J. Cytokines in gingival crevicular fluid in elderly rheumatoid arthritis patients in a population-based cross-sectional study: RANTES was associated with periodontitis. J. Periodontal Res. 2021, 56, 907–916. [Google Scholar] [CrossRef]
- Demmer, R.T.; Molitor, J.A.; Jacobs, D.R., Jr.; Michalowicz, B.S. Periodontal disease, tooth loss and incident rheumatoid arthritis: Results from the First National Health and Nutrition Examination Survey and its epidemiological follow-up study. J. Clin. Periodontol. 2011, 38, 998–1006. [Google Scholar] [CrossRef]
- Arkema, E.V.; Karlson, E.W.; Costenbader, K.H. A prospective study of periodontal disease and risk of rheumatoid arthritis. J. Rheumatol. 2010, 37, 1800–1804. [Google Scholar] [CrossRef]
- Chen, H.H.; Huang, N.; Chen, Y.M.; Chen, T.J.; Chou, P.; Lee, Y.L.; Chou, Y.J.; Lan, J.L.; Lai, K.L.; Lin, C.H.; et al. Association between a history of periodontitis and the risk of rheumatoid arthritis: A nationwide, population-based, case-control study. Ann. Rheum. Dis. 2013, 72, 1206–1211. [Google Scholar] [CrossRef]
- Chou, Y.Y.; Lai, K.L.; Chen, D.Y.; Lin, C.H.; Chen, H.H. Rheumatoid Arthritis Risk Associated with Periodontitis Exposure: A Nationwide, Population-Based Cohort Study. PLoS ONE 2015, 10, e0139693. [Google Scholar] [CrossRef]
- Chen, H.H.; Chen, D.Y.; Lin, S.Y.; Lai, K.L.; Chen, Y.M.; Chou, Y.J.; Chou, P.; Lin, C.H.; Huang, N. Periodontitis exposure within one year before anti-diabetic treatment and the risk of rheumatoid arthritis in diabetes mellitus patients: A population-based cohort study. Rev. Bras. Reum. 2014, 54, 124–130. [Google Scholar] [CrossRef]
- Choi, I.A.; Kim, J.H.; Kim, Y.M.; Lee, J.Y.; Kim, K.H.; Lee, E.Y.; Lee, E.B.; Lee, Y.M.; Song, Y.W. Periodontitis is associated with rheumatoid arthritis: A study with longstanding rheumatoid arthritis patients in Korea. Korean J. Intern. Med. 2016, 31, 977–986. [Google Scholar] [CrossRef]
- Kim, J.W.; Park, J.B.; Yim, H.W.; Lee, J.; Kwok, S.K.; Ju, J.H.; Kim, W.U.; Park, S.H. Rheumatoid arthritis is associated with early tooth loss: Results from Korea National Health and Nutrition Examination Survey V to VI. Korean J. Intern. Med. 2019, 34, 1381–1391. [Google Scholar] [CrossRef] [PubMed]
- Fuggle, N.R.; Smith, T.O.; Kaul, A.; Sofat, N. Hand to Mouth: A Systematic Review and Meta-Analysis of the Association between Rheumatoid Arthritis and Periodontitis. Front. Immunol. 2016, 7, 80. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Lozano, B.; Gonzalez-Febles, J.; Garnier-Rodriguez, J.L.; Dadlani, S.; Bustabad-Reyes, S.; Sanz, M.; Sanchez-Alonso, F.; Sanchez-Piedra, C.; Gonzalez-Davila, E.; Diaz-Gonzalez, F. Association between severity of periodontitis and clinical activity in rheumatoid arthritis patients: A case-control study. Arthritis Res. Ther. 2019, 21, 27. [Google Scholar] [CrossRef] [PubMed]
- Seong, S.C.; Kim, Y.Y.; Park, S.K.; Khang, Y.H.; Kim, H.C.; Park, J.H.; Kang, H.J.; Do, C.H.; Song, J.S.; Lee, E.J.; et al. Cohort profile: The National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) in Korea. BMJ Open 2017, 7, e016640. [Google Scholar] [CrossRef] [PubMed]
- Pratt, A.G.; Lendrem, D.; Hargreaves, B.; Aslam, O.; Galloway, J.B.; Isaacs, J.D. Components of treatment delay in rheumatoid arthritis differ according to autoantibody status: Validation of a single-centre observation using national audit data. Rheumatology 2016, 55, 1843–1848. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.G.; Kang, H.S.; Lim, H.; Kim, J.H.; Kim, J.H.; Cho, S.J.; Nam, E.S.; Min, K.W.; Park, H.Y.; Kim, N.Y.; et al. Potential Cancer Risk in Patients with Rheumatoid Arthritis: A Longitudinal Korean Population-Based Analysis. J. Pers. Med. 2022, 12, 965. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.K.; Sung, Y.K.; Choi, C.B.; Kwon, J.M.; Lee, E.K.; Bae, S.C. Development of an algorithm for identifying rheumatoid arthritis in the Korean National Health Insurance claims database. Rheumatol. Int. 2013, 33, 2985–2992. [Google Scholar] [CrossRef] [PubMed]
- Kwon, M.J.; Byun, S.H.; Kim, J.H.; Kim, J.H.; Kim, S.H.; Kim, N.Y.; Park, H.R.; Choi, H.G. Longitudinal follow-up study of the association between statin use and chronic periodontitis using national health screening cohort of Korean population. Sci. Rep. 2022, 12, 5504. [Google Scholar] [CrossRef] [PubMed]
- Kwon, M.J.; Kang, H.S.; Kim, M.J.; Kim, N.Y.; Choi, H.G.; Lim, H. Chronic Periodontitis and the Potential Likelihood of Gastric Cancer: A Nested Case-Control Study in the Korean Population Utilizing a National Health Sample Cohort. Cancers 2023, 15, 3974. [Google Scholar] [CrossRef]
- Kwon, M.J.; Kang, H.S.; Choi, H.G.; Kim, J.H.; Kim, J.H.; Bang, W.J.; Hong, S.K.; Kim, N.Y.; Hong, S.; Lee, H.K. Risk for Esophageal Cancer Based on Lifestyle Factors-Smoking, Alcohol Consumption, and Body Mass Index: Insight from a South Korean Population Study in a Low-Incidence Area. J. Clin. Med. 2023, 12, 7086. [Google Scholar] [CrossRef]
- WHO/IASO/IOTF. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia Pty Limited. 2000. Available online: https://iris.who.int/bitstream/handle/10665/206936/0957708211_eng.pdf (accessed on 12 December 2023).
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Dalton, J.E. A unified approach to measuring the effect size between two groups using SAS. SAS Global Forum 2012: Statistics and Data Analysis. 2012. Paper 335-2012. Available online: https://www.semanticscholar.org/paper/A-unified-approach-to-measuring-the-effect-size-two-Yang-Dalton/6cf4bd36ca4c90006a5d6563f646a391c255581b (accessed on 12 December 2023).
- de Pablo, P.; Dietrich, T.; McAlindon, T.E. Association of periodontal disease and tooth loss with rheumatoid arthritis in the US population. J. Rheumatol. 2008, 35, 70–76. [Google Scholar] [PubMed]
- Molitor, J.A.; Alonso, A.; Wener, M.H.; Michalowicz, B.S.; Beck, J.; Gersuk, V. Moderate to severe adult periodontitis increases risk of rheumatoid arthritis in non-smokers and is associated with elevated ACPA titers: The ARIC study. Arthritis Rheum. 2009, 60, S433. [Google Scholar]
- Kanakdande, V.; Patil, K.P.; Nayyar, A.S. Comparative Evaluation of Clinical, Hematological and Systemic Inflammatory Markers in Smokers and Non-Smokers with Chronic Periodontitis. Contemp. Clin. Dent. 2015, 6, 348–357. [Google Scholar] [CrossRef]
- Saxena, R.M.; Deepika, P.C. Comparison of glycosylated hemoglobin levels in periodontitis patients and healthy controls: A pilot study in Indian population. Indian J. Dent. Res. 2012, 23, 368–372. [Google Scholar] [CrossRef]
- Kang, H.S.; Kim, S.Y.; Choi, H.G.; Lim, H.; Kim, J.H.; Kim, J.H.; Cho, S.J.; Nam, E.S.; Min, K.W.; Park, H.Y.; et al. Comparison of the Concordance of Cardiometabolic Diseases and Physical and Laboratory Examination Findings between Monozygotic and Dizygotic Korean Adult Twins: A Cross-Sectional Study Using KoGES HTS Data. Nutrients 2022, 14, 4834. [Google Scholar] [CrossRef]
- Havemose-Poulsen, A.; Sorensen, L.K.; Bendtzen, K.; Holmstrup, P. Polymorphisms within the IL-1 gene cluster: Effects on cytokine profiles in peripheral blood and whole blood cell cultures of patients with aggressive periodontitis, juvenile idiopathic arthritis, and rheumatoid arthritis. J. Periodontol. 2007, 78, 475–492. [Google Scholar] [CrossRef]
- Cheng, Z.; Do, T.; Mankia, K.; Meade, J.; Hunt, L.; Clerehugh, V.; Speirs, A.; Tugnait, A.; Emery, P.; Devine, D. Dysbiosis in the oral microbiomes of anti-CCP positive individuals at risk of developing rheumatoid arthritis. Ann. Rheum. Dis. 2021, 80, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.; Meade, J.; Mankia, K.; Emery, P.; Devine, D.A. Periodontal disease and periodontal bacteria as triggers for rheumatoid arthritis. Best. Pract. Res. Clin. Rheumatol. 2017, 31, 19–30. [Google Scholar] [CrossRef]
- Liao, F.; Li, Z.; Wang, Y.; Shi, B.; Gong, Z.; Cheng, X. Porphyromonas gingivalis may play an important role in the pathogenesis of periodontitis-associated rheumatoid arthritis. Med. Hypotheses 2009, 72, 732–735. [Google Scholar] [CrossRef] [PubMed]
- Lucchese, A. Periodontal bacteria and the rheumatoid arthritis-related antigen RA-A47: The cross-reactivity potential. Curr. Opin. Rheumatol. 2019, 31, 542–545. [Google Scholar] [CrossRef] [PubMed]
- Azzi, L.; Rania, S.; Spadari, F.; Vinci, R.; Manfredini, M.; Croveri, F.; Boggio, A.; Tettamanti, L.; Tagliabue, A.; Silvestre-Rangil, J.; et al. Genetic correlation between rheumatoid arthritis and periodontal disease: The role of sex and IL-10. J. Biol. Regul. Homeost. Agents 2017, 31, 67–75. [Google Scholar] [PubMed]
- MacGregor, A.J.; Snieder, H.; Rigby, A.S.; Koskenvuo, M.; Kaprio, J.; Aho, K.; Silman, A.J. Characterizing the quantitative genetic contribution to rheumatoid arthritis using data from twins. Arthritis Rheum. 2000, 43, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Kido, J.I.; Ishihara, Y.; Omori, K.; Ito, S.; Matsuura, T.; Bando, T.; Wada, J.; Murasawa, A.; Nakazono, K.; et al. The KCNQ1 gene polymorphism as a shared genetic risk for rheumatoid arthritis and chronic periodontitis in Japanese adults: A pilot case-control study. J. Periodontol. 2018, 89, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Schulz, S.; Putz, N.; Jurianz, E.; Schaller, H.G.; Reichert, S. Are There Any Common Genetic Risk Markers for Rheumatoid Arthritis and Periodontal Diseases? A Case-Control Study. Mediat. Inflamm. 2019, 2019, 2907062. [Google Scholar] [CrossRef]
- Schulz, S.; Zimmer, P.; Putz, N.; Jurianz, E.; Schaller, H.G.; Reichert, S. rs2476601 in PTPN22 gene in rheumatoid arthritis and periodontitis-a possible interface? J. Transl. Med. 2020, 18, 389. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.; Gao, L.; Huang, P.; Luo, D.; Bi, C.; Chen, X. Genetic causal association between rheumatoid arthritis and periodontitis: A bidirectional two-sample Mendelian randomization analysis. Clin. Oral. Investig. 2024, 28, 107. [Google Scholar] [CrossRef]
- Yin, K.J.; Huang, J.X.; Wang, P.; Yang, X.K.; Tao, S.S.; Li, H.M.; Ni, J.; Pan, H.F. No Genetic Causal Association Between Periodontitis and Arthritis: A Bidirectional Two-Sample Mendelian Randomization Analysis. Front. Immunol. 2022, 13, 808832. [Google Scholar] [CrossRef]
- Kaur, S.; Bright, R.; Proudman, S.M.; Bartold, P.M. Does periodontal treatment influence clinical and biochemical measures for rheumatoid arthritis? A systematic review and meta-analysis. Semin. Arthritis Rheum. 2014, 44, 113–122. [Google Scholar] [CrossRef]
- Buwembo, W.; Munabi, I.G.; Kaddumukasa, M.; Kiryowa, H.; Mbabali, M.; Nankya, E.; Johnson, W.E.; Okello, E.; Sewankambo, N.K. Non-surgical oral hygiene interventions on disease activity of Rheumatoid arthritis patients with periodontitis: A randomized controlled trial. J. Dent. Res. Dent. Clin. Dent. Prospect. 2020, 14, 26–36. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total Participants | ||
|---|---|---|---|
| RA | Control | Standardized Difference | |
| Age (y), n (%) | 0.00 | ||
| 40–44 | 63 (1.77) | 252 (1.77) | |
| 45–49 | 333 (9.33) | 1332 (9.33) | |
| 50–54 | 654 (18.33) | 2616 (18.33) | |
| 55–59 | 706 (19.79) | 2824 (19.79) | |
| 60–64 | 660 (18.50) | 2640 (18.50) | |
| 65–69 | 514 (14.41) | 2056 (14.41) | |
| 70–74 | 343 (9.61) | 1372 (9.61) | |
| 75–79 | 213 (5.97) | 852 (5.97) | |
| 80–84 | 68 (1.91) | 272 (1.91) | |
| 85+ | 14 (0.39) | 56 (0.39) | |
| Sex, n (%) | 0.00 | ||
| Male | 1055 (29.57) | 4220 (29.57) | |
| Female | 2513 (70.43) | 10,052 (70.43) | |
| Income, n (%) | 0.00 | ||
| 1 (lowest) | 611 (17.12) | 2444 (17.12) | |
| 2 | 530 (14.85) | 2120 (14.85) | |
| 3 | 585 (16.40) | 2340 (16.40) | |
| 4 | 747 (20.94) | 2988 (20.94) | |
| 5 (highest) | 1095 (30.69) | 4380 (30.69) | |
| Region of residence, n (%) | 0.00 | ||
| Urban | 1541 (43.19) | 6164 (43.19) | |
| Rural | 2027 (56.81) | 8108 (56.81) | |
| Obesity, n (%) | 0.04 | ||
| Underweight | 69 (1.93) | 319 (2.24) | |
| Normal | 1334 (37.39) | 5134 (35.97) | |
| Overweight | 945 (26.49) | 3862 (27.06) | |
| Obese I | 1115 (31.25) | 4476 (31.36) | |
| Obese II | 105 (2.94) | 481 (3.37) | |
| Smoking status, n (%) | 0.03 | ||
| Nonsmoker | 2853 (79.96) | 11,551 (80.93) | |
| Past smoker | 308 (8.63) | 1204 (8.44) | |
| Current smoker | 407 (11.41) | 1517 (10.63) | |
| Alcohol consumption, n (%) | 0.04 | ||
| <1 time a week | 2690 (75.39) | 10,492 (73.51) | |
| ≥1 time a week | 878 (24.61) | 3780 (26.49) | |
| Systolic blood pressure (n, %) | 0.05 | ||
| <120 mmHg | 1161 (32.54) | 4675 (32.76) | |
| 120–139 mmHg | 1764 (49.44) | 6645 (46.56) | |
| ≥140 mmHg | 643 (18.02) | 2952 (20.68) | |
| Diastolic blood pressure (n, %) | 0.04 | ||
| <80 mmHg | 1826 (51.18) | 6977 (48.89) | |
| 80–89 mmHg | 1211 (33.94) | 4928 (34.53) | |
| ≥90 mmHg | 531 (14.88) | 2367 (16.58) | |
| Fasting blood glucose (n, %) | 0.07 | ||
| <100 mg/dL | 2381 (66.73) | 9154 (64.14) | |
| 100–125 mg/dL | 925 (25.92) | 3878 (27.17) | |
| ≥126 mg/dL | 262 (7.34) | 1240 (8.69) | |
| Total cholesterol (n, %) | 0.04 | ||
| <200 mg/dL | 1907 (53.45) | 7302 (51.16) | |
| 200–239 mg/dL | 1178 (33.02) | 4848 (33.97) | |
| ≥240 mg/dL | 483 (13.54) | 2122 (14.87) | |
| CCI score (n, %) | 0.21 | ||
| 0 | 1991 (55.80) | 9045 (63.38) | |
| 1 | 740 (20.74) | 2298 (16.10) | |
| ≥2 | 837 (23.46) | 2929 (20.52) | |
| The number of CP treatments (Mean, SD) | |||
| within 1 year | 0.50 (1.31) | 0.49 (1.31) | 0.04 |
| within 2 years | 0.94 (1.98) | 0.93 (2.07) | 0.05 |
| RA | Control | Odd Ratios for RA (95% Confidence Interval) | ||||||
|---|---|---|---|---|---|---|---|---|
| (Exposure/Total, %) | (Exposure/Total, %) | Crude † | p | Model 1 †‡ | p | Model 2 †§ | p | |
| From the index date to the before the 1-year period | ||||||||
| Total participants (n = 17,840) | ||||||||
| No CP | 2770/3568 (77.6%) | 11,219/14,272 (78.6%) | 1 | 1 | 1 | |||
| CP ≥ 1 | 798/3568 (22.4%) | 3053/14,272 (21.4%) | 1.06 (0.97–1.16) | 0.201 | 1.08 (0.99–1.19) | 0.079 | 1.09 (0.99–1.19) | 0.074 |
| CP < 2 | 2770/3568 (77.6%) | 11,219/14,272 (78.6%) | 1 | 1 | 1 | |||
| CP ≥ 2 | 798/3568 (22.4%) | 3053/14,272 (21.4%) | 1.04 (0.93–1.17) | 0.501 | 1.07 (0.95–1.20) | 0.283 | 1.07 (0.95–1.20) | 0.300 |
| CP < 3 | 3348/3568 (93.8%) | 13,401/14,272 (93.9%) | 1 | 1 | 1 | |||
| CP ≥ 3 | 220/3568 (6.2%) | 871/14,272 (6.1%) | 1.01 (0.87–1.18) | 0.888 | 1.04 (0.89–1.21) | 0.612 | 1.04 (0.89–1.21) | 0.625 |
| From the index date to the before the 2-year period | ||||||||
| Total participants (n = 17,840) | ||||||||
| No CP | 2316/3568 (64.9%) | 9529/14,272 (66.8%) | 1 | 1 | 1 | |||
| CP ≥ 1 | 1252/3568 (35.1%) | 4743/14,272 (33.2%) | 1.09 (1.01–1.18) | 0.033 * | 1.12 (1.03–1.21) | 0.006 * | 1.12 (1.04–1.21) | 0.005 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, H.S.; Kim, J.-H.; Kim, J.H.; Bang, W.J.; Choi, H.G.; Yoo, D.M.; Lee, N.-E.; Han, K.M.; Kim, N.Y.; Park, H.Y.; et al. The Association of Chronic Periodontitis as a Potential Risk Factor with Rheumatoid Arthritis: A Nested Case-Control Study Using a Korean National Health Screening Cohort. Biomedicines 2024, 12, 936. https://doi.org/10.3390/biomedicines12050936
Kang HS, Kim J-H, Kim JH, Bang WJ, Choi HG, Yoo DM, Lee N-E, Han KM, Kim NY, Park HY, et al. The Association of Chronic Periodontitis as a Potential Risk Factor with Rheumatoid Arthritis: A Nested Case-Control Study Using a Korean National Health Screening Cohort. Biomedicines. 2024; 12(5):936. https://doi.org/10.3390/biomedicines12050936
Chicago/Turabian StyleKang, Ho Suk, Joo-Hee Kim, Ji Hee Kim, Woo Jin Bang, Hyo Geun Choi, Dae Myoung Yoo, Na-Eun Lee, Kyeong Min Han, Nan Young Kim, Ha Young Park, and et al. 2024. "The Association of Chronic Periodontitis as a Potential Risk Factor with Rheumatoid Arthritis: A Nested Case-Control Study Using a Korean National Health Screening Cohort" Biomedicines 12, no. 5: 936. https://doi.org/10.3390/biomedicines12050936