
Cytomegalovirus Immunoglobulin G Levels and Subclinical Arterial Disease among People Living with HIV in Botswana: A Cross-Sectional Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
- (1)
- PLWH on fully suppressive combination ART (cART);
- (2)
- PLWH who are ART-naïve, and;
- (3)
- HIV-uninfected controls.
2.2. Study Procedures
2.3. Carotid Imaging
2.4. Statistical Methods
3. Results
3.1. Demographic and Clinical Characteristics of Participants
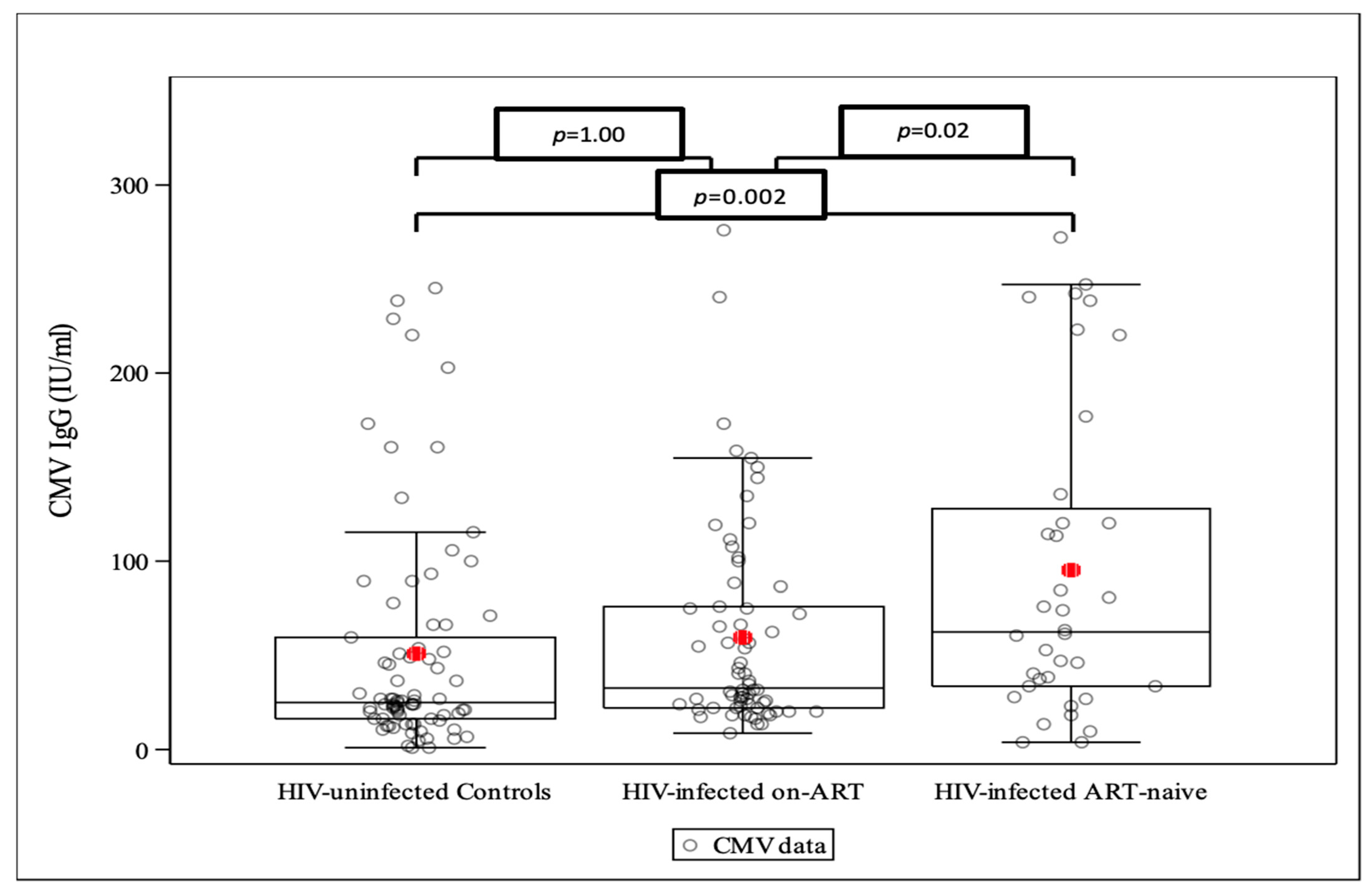
3.2. CMV IgG Levels across the Study Arms
3.3. The Association between CMV IgG and Demographic and Clinical Characteristics
3.4. The Association between CMV IgG Levels and Systemic Inflammation/Arterial Disease (Endothelial Injury) by Study Groups
4. Discussion
Limitations and Strengths
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Global Health Observatory. Available online: https://www.who.int/data/gho/data/themes/hiv-aids (accessed on 14 January 2023).
- Triant, V.A.; Grinspoon, S.K. Epidemiology of ischemic heart disease in HIV. Curr. Opin. HIV AIDS 2017, 12, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Abd-Elmoniem, K.Z.; Yeramosu, T.; Purdy, J.B.; Ouwerkerk, R.; Matta, J.R.; Ishaq, H.; Hawkins, K.; Curl, K.A.; Dee, N.; Gharib, A.M.; et al. The role of HIV as a risk modifier for coronary endothelial function in young adults. HIV Med. 2023, 24, 818–826. [Google Scholar] [CrossRef]
- Strauss, K.-L.E.; Phoswa, W.N.; Lebelo, S.L.; Modjadji, P.; Mokgalaboni, K. Endothelial dysfunction, a predictor of cardiovascular disease in HIV patients on antiretroviral therapy: A systematic review and meta-analysis. Thromb. Res. 2024, 234, 101–112. [Google Scholar] [CrossRef]
- Triant, V.A. Cardiovascular disease and HIV infection. Curr. HIV/AIDS Rep. 2013, 10, 199–206. [Google Scholar] [CrossRef]
- Hunt, P.W.; Lee, S.A.; Siedner, M.J. Immunologic Biomarkers, Morbidity, and Mortality in Treated HIV Infection. J. Infect. Dis. 2016, 214 (Suppl. S2), S44–S50. [Google Scholar] [CrossRef]
- Wang, H.; Peng, G.; Bai, J.; He, B.; Huang, K.; Hu, X.; Liu, D. Cytomegalovirus Infection and Relative Risk of Cardiovascular Disease (Ischemic Heart Disease, Stroke, and Cardiovascular Death): A Meta-Analysis of Prospective Studies Up to 2016. J. Am. Heart Assoc. 2017, 6, e005025. [Google Scholar] [CrossRef] [PubMed]
- Mezoh, G.; Lutchman, N.; Worsley, C.; Gededzha, M.; Mayne, E.; Martinson, N.; Moore, P.L.; Crowther, N.J. Biomarkers of Endothelial Activation in Black South African HIV-Positive Subjects are Associated with Both High Viral Load and Low CD4 Counts. AIDS Res. Hum. Retroviruses 2022, 38, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Pinto, D.S.M.; da Silva, M. Cardiovascular Disease in the Setting of Human Immunodeficiency Virus Infection. Curr. Cardiol. Rev. 2018, 14, 25–41. [Google Scholar] [CrossRef] [PubMed]
- Hsue, P.Y.; Deeks, S.G.; Hunt, P.W. Immunologic basis of cardiovascular disease in HIV-infected adults. J. Infect. Dis. 2012, 205 (Suppl. S3), S375–S382. [Google Scholar] [CrossRef]
- Hunt, P.W. HIV and inflammation: Mechanisms and consequences. Curr. HIV/AIDS Rep. 2012, 9, 139–147. [Google Scholar] [CrossRef]
- Grinspoon, S. Novel mechanisms and anti-inflammatory strategies to reduce cardiovascular risk in Human Immunodeficiency Virus. Trans. Am. Clin. Climatol. Assoc. 2018, 129, 140–154. [Google Scholar] [PubMed]
- Freeman, M.L.; Lederman, M.M.; Gianella, S. Partners in Crime: The Role of CMV in Immune Dysregulation and Clinical Outcome During HIV Infection. Curr. HIV/AIDS Rep. 2016, 13, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Parrinello, C.M.; Sinclair, E.; Landay, A.L.; Lurain, N.; Sharrett, A.R.; Gange, S.J.; Xue, X.; Hunt, P.W.; Deeks, S.G.; Hodis, H.N.; et al. Cytomegalovirus immunoglobulin G antibody is associated with subclinical carotid artery disease among HIV-infected women. J. Infect. Dis. 2012, 205, 1788–1796. [Google Scholar] [CrossRef]
- Schnittman, S.R.; Hunt, P.W. Clinical consequences of asymptomatic cytomegalovirus in treated human immunodeficency virus infection. Curr. Opin. HIV AIDS 2021, 16, 168–176. [Google Scholar] [CrossRef]
- Hsue, P.Y.; Hunt, P.W.; Sinclair, E.; Bredt, B.; Franklin, A.; Killian, M.; Hoh, R.; Martin, J.N.; McCune, J.M.; Waters, D.D.; et al. Increased carotid intima-media thickness in HIV patients is associated with increased cytomegalovirus-specific T-cell responses. Aids 2006, 20, 2275–2283. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, A.; Kristoffersen, U.S.; Panum, I.; Hansen, Y.B.; Skottrup, P.D.; Hasbak, P.; Kjaer, A.; Lebech, A.M. Coronary artery calcium and intima-media thickness are associated with level of cytomegalovirus immunoglobulin G in HIV-infected patients. HIV Med. 2019, 20, 60–62. [Google Scholar] [CrossRef]
- Mosepele, M.; Mohammed, T.; Mupfumi, L.; Moyo, S.; Bennett, K.; Lockman, S.; Hemphill, L.C.; Triant, V.A. HIV disease is associated with increased biomarkers of endothelial dysfunction despite viral suppression on long-term antiretroviral therapy in Botswana. Cardiovasc. J. Afr. 2018, 29, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Mosepele, M.; Hemphill, L.C.; Moloi, W.; Moyo, S.; Nkele, I.; Makhema, J.; Bennett, K.; Triant, V.A.; Lockman, S. Pre-clinical carotid atherosclerosis and sCD163 among virally suppressed HIV patients in Botswana compared with uninfected controls. PLoS ONE 2017, 12, e0179994. [Google Scholar] [CrossRef]
- Boikhutso, K. Ethnic identity in a ‘Homogeneous’ Nation State; University of Cape Town: Cape Town, South Africa, 2009. [Google Scholar]
- Mine, M.; Stafford, K.; Laws, R.L.; Marima, R.; Lekone, P.; Ramaabya, D.; Makhaola, K.; Mapondera, P.; Wray-Gordon, F.; Agbakwuru, C.; et al. Botswana achieved the Joint United Nations Programme on HIV/AIDS (UNAIDS) 95-95-95 targets: Results from the Fifth Botswana HIV/AIDS Impact Survey (BAIS V). In Proceedings of the International AIDS Society Conference, Montréal, QC, Canada, 29 July–2 August 2022. [Google Scholar]
- Burdo, T.H.; Lo, J.; Abbara, S.; Wei, J.; DeLelys, M.E.; Preffer, F.; Rosenberg, E.S.; Williams, K.C.; Grinspoon, S. Soluble CD163, a novel marker of activated macrophages, is elevated and associated with noncalcified coronary plaque in HIV-infected patients. J. Infect. Dis. 2011, 204, 1227–1236. [Google Scholar] [CrossRef]
- Lurain, N.S.; Hanson, B.A.; Hotton, A.L.; Weber, K.M.; Cohen, M.H.; Landay, A.L. The Association of Human Cytomegalovirus with Biomarkers of Inflammation and Immune Activation in HIV-1-Infected Women. AIDS Res. Hum. Retroviruses 2016, 32, 134–143. [Google Scholar] [CrossRef]
- Hodowanec, A.C.; Lurain, N.S.; Krishnan, S.; Bosch, R.J.; Landay, A.L. Increased CMV IgG Antibody Titer is Associated with Non-AIDS Events among Virologically Suppressed HIV-Positive Persons. Pathog. Immun. 2019, 4, 66–78. [Google Scholar] [CrossRef]
- Hsue, P.Y.; Lo, J.C.; Franklin, A.; Bolger, A.F.; Martin, J.N.; Deeks, S.G.; Waters, D.D. Progression of atherosclerosis as assessed by carotid intima-media thickness in patients with HIV infection. Circulation 2004, 109, 1603–1608. [Google Scholar] [CrossRef]
- Lorenz, M.W.; Stephan, C.; Harmjanz, A.; Staszewski, S.; Buehler, A.; Bickel, M.; von Kegler, S.; Ruhkamp, D.; Steinmetz, H.; Sitzer, M. Both long-term HIV infection and highly active antiretroviral therapy are independent risk factors for early carotid atherosclerosis. Atherosclerosis 2008, 196, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Grunfeld, C.; Delaney, J.A.; Wanke, C.; Currier, J.S.; Scherzer, R.; Biggs, M.L.; Tien, P.C.; Shlipak, M.G.; Sidney, S.; Polak, J.F.; et al. Preclinical atherosclerosis due to HIV infection: Carotid intima-medial thickness measurements from the FRAM study. Aids 2009, 23, 1841–1849. [Google Scholar] [CrossRef]
- Kaplan, R.C.; Kingsley, L.A.; Gange, S.J.; Benning, L.; Jacobson, L.P.; Lazar, J.; Anastos, K.; Tien, P.C.; Sharrett, A.R.; Hodis, H.N. Low CD4+ T-cell count as a major atherosclerosis risk factor in HIV-infected women and men. Aids 2008, 22, 1615–1624. [Google Scholar] [CrossRef]
- Currier, J.S.; Kendall, M.A.; Zackin, R.; Henry, W.K.; Alston-Smith, B.; Torriani, F.J.; Schouten, J.; Mickelberg, K.; Li, Y.; Hodis, H.N. Carotid artery intima-media thickness and HIV infection: Traditional risk factors overshadow impact of protease inhibitor exposure. Aids 2005, 19, 927–933. [Google Scholar] [CrossRef] [PubMed]
- Currier, J.S.; Kendall, M.A.; Henry, W.K.; Alston-Smith, B.; Torriani, F.J.; Tebas, P.; Li, Y.; Hodis, H.N. Progression of carotid artery intima-media thickening in HIV-infected and uninfected adults. Aids 2007, 21, 1137–1145. [Google Scholar] [CrossRef]
- Fourie, C.M.; Schutte, A.E.; Smith, W.; Kruger, A.; van Rooyen, J.M. Endothelial activation and cardiometabolic profiles of treated and never-treated HIV infected Africans. Atherosclerosis 2015, 240, 154–160. [Google Scholar] [CrossRef]
- Iloeje, U.; Yuan, Y.; L’Italien, G.; Mauskopf, J.; Holmberg, S.; Moorman, A.; Wood, K.; Moore, R. Protease inhibitor exposure and increased risk of cardiovascular disease in HIV-infected patients. HIV Med. 2005, 6, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.H. Dyslipidemia in the era of HIV protease inhibitors. Prog. Cardiovasc. Dis. 2003, 45, 293–304. [Google Scholar] [CrossRef]
- Temu, T.M.; Polyak, S.J.; Zifodya, J.S.; Wanjalla, C.N.; Koethe, J.R.; Masyuko, S.; Nyabiage, J.; Kinuthia, J.; Gervassi, A.L.; Oyugi, J.; et al. Endothelial Dysfunction Is Related to Monocyte Activation in Antiretroviral-Treated People With HIV and HIV-Negative Adults in Kenya. Open Forum. Infect. Dis. 2020, 7, ofaa425. [Google Scholar] [CrossRef]
- Fourie, C.; van Rooyen, J.; Pieters, M.; Conradie, K.; Hoekstra, T.; Schutte, A. Is HIV-1 infection associated with endothelial dysfunction in a population of African ancestry in South Africa? Cardiovasc. J. Afr. 2011, 22, 134–140. [Google Scholar] [CrossRef]
- Melendez, M.M.; McNurlan, M.A.; Mynarcik, D.C.; Khan, S.; Gelato, M.C. Endothelial Adhesion Molecules Are Associated with Inflammation in Subjects with HIV Disease. Clin. Infect. Dis. 2008, 46, 775–780. [Google Scholar] [CrossRef]
- Grinspoon, S.K.; Fitch, K.V.; Zanni, M.V.; Fichtenbaum, C.J.; Umbleja, T.; Aberg, J.A.; Overton, E.T.; Malvestutto, C.D.; Bloomfield, G.S.; Currier, J.S.; et al. Pitavastatin to Prevent Cardiovascular Disease in HIV Infection. N. Engl. J. Med. 2023, 389, 687–699. [Google Scholar] [CrossRef]
- Stein, J.H. Carotid Artery Imaging: Insights Into Inflammation and Cardiovascular Disease Risk in Patients With HIV Infection. J. Am. Heart Assoc. 2012, 1, e001396. [Google Scholar] [CrossRef]


{kind=link}
| HIV-Uninfected Controls, n = 79 | PLWH on-cART, n = 68 | PLWH Who Were ART-Naïve, n = 36 | p-Value | |
|---|---|---|---|---|
| N | 79 | 68 | 36 | 0.653 |
| Age | ||||
| Mean (SD) | 38.2 (5.4) | 38.7 (4.6) | 37.8 (5.4) | |
| 30–35 | 32 (41.0%) | 16 (24.0%) | 16 (44.0%) | 0.027 |
| 36–40 | 21 (27.0%) | 34 (50.0%) | 10 (28.0%) | |
| 41–50 | 26 (33.0%) | 18 (26.0%) | 10 (28.0%) | |
| Female Sex, N (%) | 36 (45.6%) | 35 (51.5%) | 21 (58.3%) | 0.434 |
| Cigarette Smoking, N (%) | ||||
| Ever | 27 (34.0%) | 27 (40.0%) | 7 (19.0%) | 0.102 |
| Current | 16 (20.0%) | 6 (9.0%) | 4 (11.0%) | 0.134 |
| Family history, N, (%) | ||||
| CAD | 4( 5.0%) | 1 (1.0%) | 0 | 0.278 |
| Stroke | 16 (20.0%) | 6 (9.0%) | 1 (3.0%) | 0.020 |
| Anthropometric data, mean (SD) | ||||
| SBP (mmHg) | 130.5 (17.3) | 128.5 (16.3) | 129.8 (17.5) | 0.768 |
| DBP (mmHg) | 84.7 (13.5) | 83.9 (12.2) | 85.2 (13.5) | 0.877 |
| Waist–Hip ratio, N(%) | ||||
| Male (≥0.90) | 7 (16.0%) | 8 (24.0%) | 7 (47.0%) | 0.065 |
| Female (≥0.85) | 14 (39.0%) | 17 (50.0%) | 6 (29.0%) | 0.300 |
| Medical History, N (%) | ||||
| Diabetes mellitus | 0 | 1 (1.0%) | 1 (3.0%) | 0.322 |
| Hypertension | 10 (13.0%) | 10 (15.0%) | 0 | 0.031 |
| Chronic kidney disease | 0 | 2 (3.0%) | 0 | 0.175 |
| Dyslipidemia | 2 (3.0%) | 6 (9.0%) | 0 | 0.093 |
| CVD Risk Blood Tests, mean (SD) | ||||
| Total cholesterol (mmol/L) | 4.4 (1.2) | 4.8 (1.3) | 4.1 (0.9) | 0.003 |
| LDL cholesterol (mmol/L) | 2.5 (1.0) | 2.9 (1.1) | 2.3 (0.8) | 0.020 |
| HDL cholesterol (mmol/L) | 1.4 (0.4) | 1.5 (0.5) | 1.2 (0.4) | 0.003 |
| Non-HDL cholesterol (mmol/L) | 2.9 (1.2) | 3.3 (1.3) | 2.9 (0.9) | 0.059 |
| Triglycerides (mmol/L) | 1.2 (1.5) | 1.4 (0.8) | 1.2 (0.6) | 0.541 |
| HbA1c (%) (SD) | 5.5 (1.0) | 5.3 (0.4) | 5.7 (0.5) | 0.021 |
| HIV Parameters, mean (SD) | ||||
| HIV disease duration (yrs) | N/A | 9.8 (3.2) | N/A | N/A |
| ART duration (yrs) | N/A | 8.6 (2.8) | N/A | N/A |
| CD4 nadir (cells/uL) | N/A | 123.5 (76) | N/A | N/A |
| Baseline CD4 count (cells/uL) | N/A | 122.9( 73.1) | N/A | |
| Current CD4 count (cells/uL) | N/A | 540.2 (230.8) | 381.5 (236.6) | 0.001 |
| Proportion with undetectable VL | N/A | 100% | N/A | N/A |
| Months since VL < 400 cp/mL | N/A | 3.4 (2) | N/A | N/A |
| Patients on NNRTI-based ART | N/A | 50 (75.0%) | N/A | N/A |
| Patients on PI-based ART | N/A | 17 (25.0%) | N/A | N/A |
| Carotid Assessment, mean (SD) | ||||
| Mean cIMT (mm) (SD) | 0.616 (0.1) | 0.595 (0.09) | 0.574 (0.06) | 0.059 |
| Any plaque, N (%) | 2 (3.0%) | 0 | 2 (6.0%) | 0.190 |
| Biomarkers, mean (SD) | ||||
| Soluble CD163 (ng/mL) | 7.1 (0.6) | 7.0 (0.7) | 7.3 (0.5) | 0.069 |
| ICAM-1 (ng/mL) | 446.3 (164.2) | 529.1 (156.6) | 574.1 (203.9) | <0.001 |
| Log-VCAM-1 (log ng/mL) | 6.5 (0.4) | 6.6 (0.3) | 7.0 (0.5) | <0.001 |
| e-Selectin (ng/mL) | 63.8 (18.4) | 61.6 (23.4) | 58.4 (32.5) | 0.710 |
| log VCAM-1 | ICAM-1 | e-Selectin | cIMT | sCD163 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model | Est (95% CI) | p | Est (95% CI) | p | Est (95% CI) | p | Est (95% CI) | p | Est (95% CI) | p | ||
| 1 | CMV IgG | 0.001 (0, 0.002) | 0.2 | 0.2 (−0.3, 0.6) | 0.4 | −0.01 (−0.08, 0.06) | 0.8 | 0 (0.0) | 0.09 | 0 (−0.001, 0.002) | 0.8 | |
| 2 * | CMV IgG | 0.09 (−0.4, 0.5) | 0.7 | 0.009 (−0.07, 0.08) | 0.8 | 0 (0.0) | 0.2 | 0 (−0.001, 0.002) | 0.8 | |||
| CMV among PLWH on ART | −0.001 (−0.002, 0.001) | 0.4 | PLWH on-ART | 88.4 (26.6, 150.3) | <0.01 | 1.07 (−8.5, 10.7) | 0.8 | −0.03 (−0.06, −0.003) | 0.03 | −0.2 (−0.4, 0.02) | 0.1 | |
| CMV among ART-naïve PLWH | 0.002 (0, 0.004) | 0.01 | ART-naïve PLWH | 102.2 (24.2, 180.2) | 0.01 | −12.1 (−27.4, 3.2) | 0.1 | −0.03 (−0.06, 0.004) | 0.09 | 0.03 (−0.2, 0.3) | 0.9 | |
| CMV among controls | 0 (−0.002, 0.001) | 0.5 | HIV-uninfected Controls | (ref) | (ref) | (ref) | (ref) | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moshomo, T.; Molefe-Baikai, O.J.; Bennett, K.; Gaolathe, T.; Moyo, S.; Gaseitsewe, S.; Mohammed, T.; Lockman, S.; Mosepele, M. Cytomegalovirus Immunoglobulin G Levels and Subclinical Arterial Disease among People Living with HIV in Botswana: A Cross-Sectional Study. Biomedicines 2024, 12, 935. https://doi.org/10.3390/biomedicines12050935
Moshomo T, Molefe-Baikai OJ, Bennett K, Gaolathe T, Moyo S, Gaseitsewe S, Mohammed T, Lockman S, Mosepele M. Cytomegalovirus Immunoglobulin G Levels and Subclinical Arterial Disease among People Living with HIV in Botswana: A Cross-Sectional Study. Biomedicines. 2024; 12(5):935. https://doi.org/10.3390/biomedicines12050935
Chicago/Turabian StyleMoshomo, Thato, Onkabetse Julia Molefe-Baikai, Kara Bennett, Tendani Gaolathe, Sikhulile Moyo, Simani Gaseitsewe, Terence Mohammed, Shahin Lockman, and Mosepele Mosepele. 2024. "Cytomegalovirus Immunoglobulin G Levels and Subclinical Arterial Disease among People Living with HIV in Botswana: A Cross-Sectional Study" Biomedicines 12, no. 5: 935. https://doi.org/10.3390/biomedicines12050935