
Clinical Significance of the Immunohistochemical Expression of Histone Deacetylases (HDACs)-2, -4, and -5 in Ovarian Adenocarcinomas
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Collective
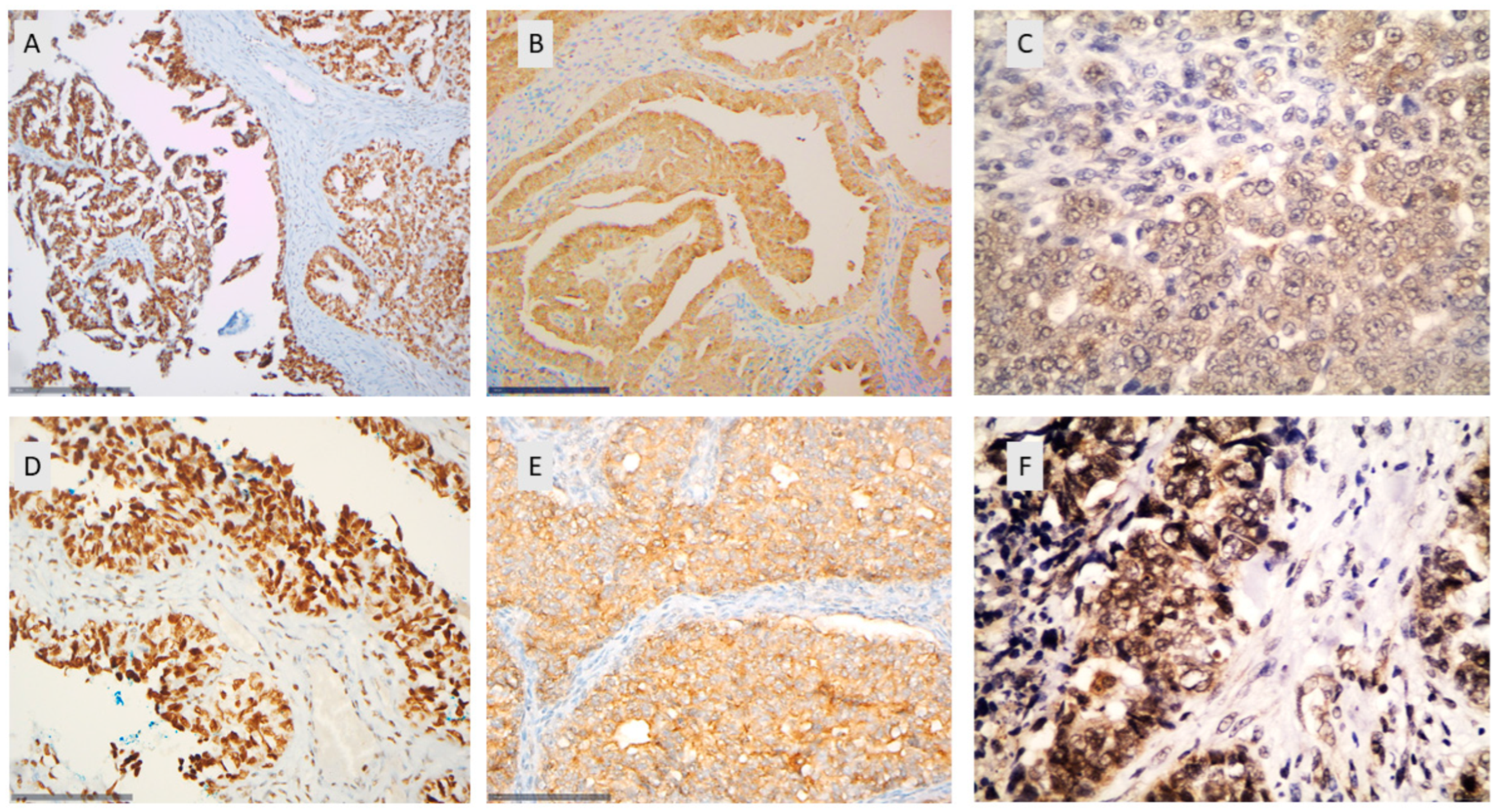
2.2. Immunohistochemical Analysis
2.3. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. HDAC-2 Expression and Associations with Clinicopathological Characteristics
3.3. HDAC-4 Expression and Associations with Clinicopathological Characteristics
3.4. HDAC-5 Expression and Associations with Clinicopathological Characteristics
3.5. Associations among HDAC-2, HDAC-4, and HDAC-5
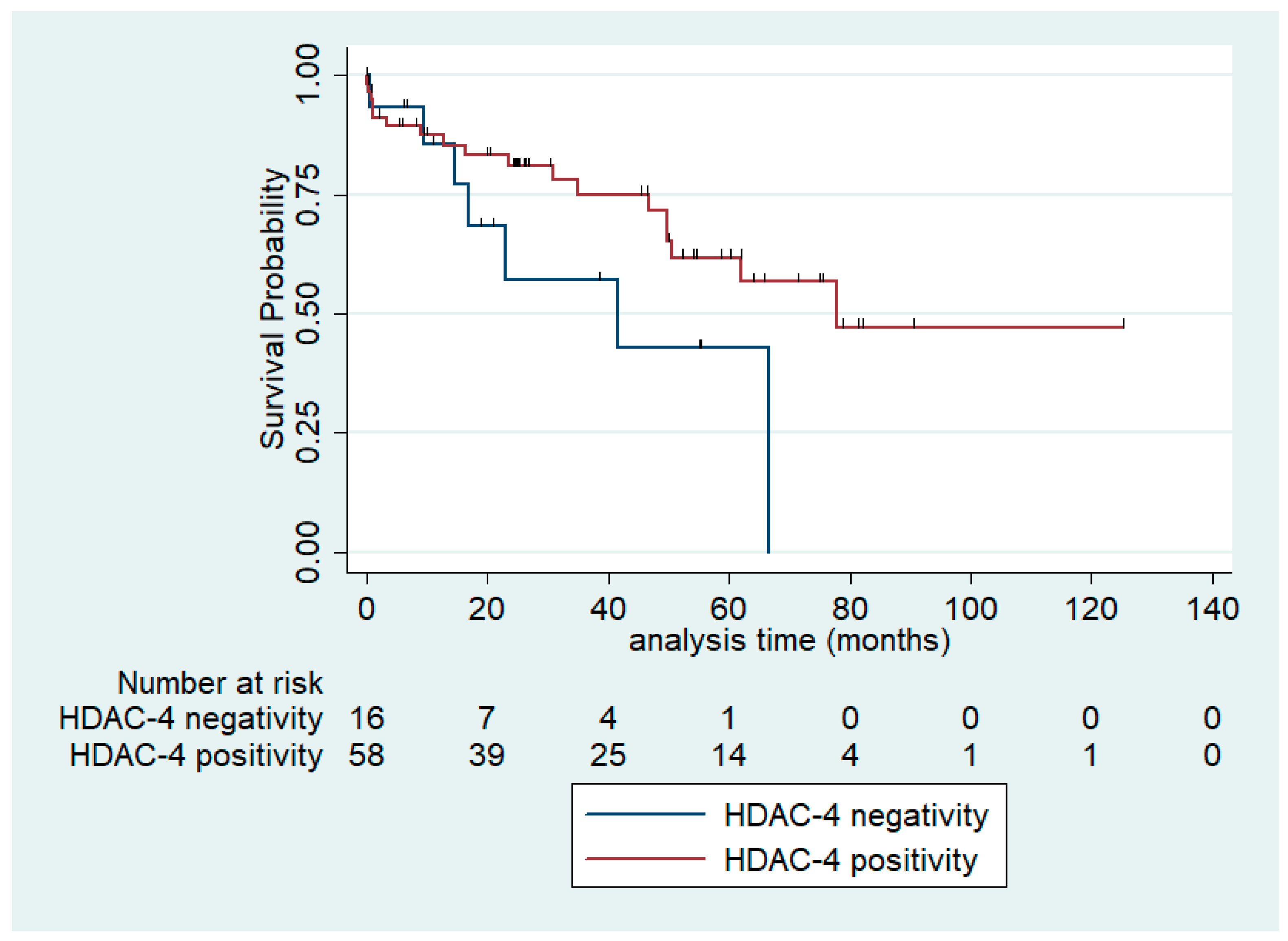
3.6. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gallinari, P.; Marco, S.D.; Jones, P.; Pallaoro, M.; Steinkühler, C. HDACs, Histone Deacetylation and Gene Transcription: From Molecular Biology to Cancer Therapeutics. Cell Res. 2007, 17, 195–211. [Google Scholar] [CrossRef] [PubMed]
- Roth, S.Y.; Denu, J.M.; Allis, C.D. Histone Acetyltransferases. Annu. Rev. Biochem. 2001, 70, 81–120. [Google Scholar] [CrossRef] [PubMed]
- Marks, P.; Miller, T.; Richon, V.M. Histone Deacetylases. Curr. Opin. Pharmacol. 2003, 3, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Blander, G.; Guarente, L. The Sir2 Family of Protein Deacetylases. Annu. Rev. Biochem. 2004, 73, 417–435. [Google Scholar] [CrossRef] [PubMed]
- de Ruijter, A.J.M.; van Gennip, A.H.; Caron, H.N.; Kemp, S.; van Kuilenburg, A.B. Histone Deacetylases (HDACs): Characterization of the Classical HDAC Family. Biochem. J. 2003, 370, 737–749. [Google Scholar] [CrossRef]
- Goutas, D.; Theocharis, S.; Tsourouflis, G. Unraveling the Epigenetic Role and Clinical Impact of Histone Deacetylases in Neoplasia. Diagnostics 2021, 11, 1346. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Xing, W.; Zhao, R.; Tan, Y.; Wu, X.; Ao, L.; Li, Z.; Yao, M.; Yuan, M.; Guo, W.; et al. HDAC2 Inhibits EMT-Mediated Cancer Metastasis by Downregulating the Long Noncoding RNA H19 in Colorectal Cancer. J. Exp. Clin. Cancer Res. 2020, 39, 270. [Google Scholar] [CrossRef] [PubMed]
- Levidou, G.; Gajdzis, P.; Cassoux, N.; Donizy, P.; Masaoutis, C.; Gajdzis, M.; Gardrat, S.; Pergaris, A.; Danas, E.; Klijanienko, J.; et al. Histone Deacetylase (HDAC)-1, -2, -4, and -6 in Uveal Melanomas: Associations with Clinicopathological Parameters and Patients’ Survival. Cancers 2021, 13, 4763. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, A.; Horiuchi, A.; Kikuchi, N.; Hayashi, T.; Fuseya, C.; Suzuki, A.; Konishi, I.; Shiozawa, T. Type-specific Roles of Histone Deacetylase (HDAC) Overexpression in Ovarian Carcinoma: HDAC1 Enhances Cell Proliferation and HDAC3 Stimulates Cell Migration with Downregulation of E-cadherin. Int. J. Cancer 2010, 127, 1332–1346. [Google Scholar] [CrossRef]
- Li, Y.; Seto, E. HDACs and HDAC Inhibitors in Cancer Development and Therapy. Cold Spring HarbPerspect Med. 2016, 6, a026831. [Google Scholar] [CrossRef]
- Moufarrij, S.; Dandapani, M.; Arthofer, E.; Gomez, S.; Srivastava, A.; Lopez-Acevedo, M.; Villagra, A.; Chiappinelli, K.B. Epigenetic Therapy for Ovarian Cancer: Promise and Progress. Clin. Epigenetics 2019, 11, 7. [Google Scholar] [CrossRef]
- Pouloudi, D.; Manou, M.; Sarantis, P.; Tsoukalas, N.; Tsourouflis, G.; Dana, E.; Karamouzis, M.V.; Klijanienko, J.; Theocharis, S. Clinical Significance of Histone Deacetylase (HDAC)-1, -2, -4 and -6 Expression in Salivary Gland Tumors. Diagnostics 2021, 11, 517. [Google Scholar] [CrossRef]
- Psilopatis, I.; Schaefer, J.I.; Arsenakis, D.; Bolovis, D.; Levidou, G. SOX11 and Epithelial-Mesenchymal Transition in Metastatic Serous Ovarian Cancer. Biomedicines 2023, 11, 2540. [Google Scholar] [CrossRef]
- Falzone, L.; Scandurra, G.; Lombardo, V.; Gattuso, G.; Lavoro, A.; Distefano, A.; Scibilia, G.; Scollo, P. A Multidisciplinary Approach Remains the Best Strategy to Improve and Strengthen the Management of Ovarian Cancer (Review). Int. J. Oncol. 2021, 59, 53. [Google Scholar] [CrossRef]
- Qazi, S.; Sharma, A.; Raza, K. The Role of Epigenetic Changes in Ovarian Cancer: A Review. Indian J. Gynecol. Oncol. 2021, 19, 27. [Google Scholar] [CrossRef]
- Caslini, C.; Capo-chichi, C.D.; Roland, I.H.; Nicolas, E.; Yeung, A.T.; Xu, X.-X. Histone Modifications Silence the GATA Transcription Factor Genes in Ovarian Cancer. Oncogene 2006, 25, 5446–5461. [Google Scholar] [CrossRef]
- Chan, M.W.Y.; Huang, Y.-W.; Hartman-Frey, C.; Kuo, C.-T.; Deatherage, D.; Qin, H.; Cheng, A.S.L.; Yan, P.S.; Davuluri, R.V.; Huang, T.H.-M.; et al. Aberrant Transforming Growth Factor Β1 Signaling and SMAD4 Nuclear Translocation Confer Epigenetic Repression of ADAM19 in Ovarian Cancer. Neoplasia 2008, 10, 908-IN2. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, A.H.M.; Afroze, S.; Osuji, G.; Kayani, S.; Colon, N.; Pantho, A.; Kuehl, T.; Pilkinton, K.; Uddin, M. Epigenetic Modifications in Ovarian Cancer: A Review. J. Cancer Treat. Diagn. 2020, 4, 17–35. [Google Scholar] [CrossRef]
- Jin, K.L.; Pak, J.H.; Park, J.-Y.; Choi, W.H.; Lee, J.-Y.; Kim, J.-H.; Nam, J.-H. Expression Profile of Histone Deacetylases 1, 2 and 3 in Ovarian Cancer Tissues. J. Gynecol. Oncol. 2008, 19, 185–190. [Google Scholar] [CrossRef]
- Weichert, W.; Denkert, C.; Noske, A.; Darb-Esfahani, S.; Dietel, M.; Kalloger, S.E.; Huntsman, D.G.; Köbel, M. Expression of Class I Histone Deacetylases Indicates Poor Prognosis in Endometrioid Subtypes of Ovarian and Endometrial Carcinomas. Neoplasia 2008, 10, 1021–1027. [Google Scholar] [CrossRef]
- Shen, Y.-F.; Wei, A.-M.; Kou, Q.; Zhu, Q.-Y.; Zhang, L. Histone Deacetylase 4 Increases Progressive Epithelial Ovarian Cancer Cells via Repression of P21 on Fibrillar Collagen Matrices. Oncol. Rep. 2016, 35, 948–954. [Google Scholar] [CrossRef]
- Levinzon, L.; Madigan, M.; Nguyen, V.; Hasic, E.; Conway, M.; Cherepanoff, S. Tumour Expression of Histone Deacetylases in Uveal Melanoma. Ocul. Oncol. Pathol. 2019, 5, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Mottet, D.; Castronovo, V. Histone Deacetylases: Target Enzymes for Cancer Therapy. Clin. Exp. Metastasis 2008, 25, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, M.; Nielsen, T.O. Histone Deacetylase 1 and 2 in Mesenchymal Tumors. Mod. Pathol. 2012, 25, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Mutze, K.; Langer, R.; Becker, K.; Ott, K.; Novotny, A.; Luber, B.; Hapfelmeier, A.; Göttlicher, M.; Höfler, H.; Keller, G. Histone Deacetylase (HDAC) 1 and 2 Expression and Chemotherapy in Gastric Cancer. Ann. Surg. Oncol. 2010, 17, 3336–3343. [Google Scholar] [CrossRef]
- Giaginis, C.; Damaskos, C.; Koutsounas, I.; Zizi-Serbetzoglou, A.; Tsoukalas, N.; Patsouris, E.; Kouraklis, G.; Theocharis, S. Histone Deacetylase (HDAC)-1, -2, -4 and -6 Expression in Human Pancreatic Adenocarcinoma: Associations with Clinicopathological Parameters, Tumor Proliferative Capacity and Patients′ Survival. BMC Gastroenterol. 2015, 15, 148. [Google Scholar] [CrossRef]
- Peng, D.; Wu, T.; Wang, J.; Huang, J.; Zheng, L.; Wang, P.; Li, J.; Wu, L.; Luo, M. microRNA-671-5p Reduces Tumorigenicity of Ovarian Cancer via Suppressing HDAC5 and HIF-1α Expression. Chem.-Biol. Interact. 2022, 355, 109780. [Google Scholar] [CrossRef] [PubMed]
- Weichert, W. HDAC Expression and Clinical Prognosis in Human Malignancies. Cancer Lett. 2009, 280, 168–176. [Google Scholar] [CrossRef]
- Xu, L.; Yan, X.; Wang, J.; Zhao, Y.; Liu, Q.; Fu, J.; Shi, X.; Su, J. The Roles of Histone Deacetylases in the Regulation of Ovarian Cancer Metastasis. Int. J. Mol. Sci. 2023, 24, 15066. [Google Scholar] [CrossRef]
- Garrett, L.A.; Growdon, W.B.; Rueda, B.R.; Foster, R. Influence of a Novel Histone Deacetylase Inhibitor Panobinostat (LBH589) on the Growth of Ovarian Cancer. J. Ovarian Res. 2016, 9, 58. [Google Scholar] [CrossRef]
- Zhou, M.; Yuan, M.; Zhang, M.; Lei, C.; Aras, O.; Zhang, X.; An, F. Combining Histone Deacetylase Inhibitors (HDACis) with Other Therapies for Cancer Therapy. Eur. J. Med. Chem. 2021, 226, 113825. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients’ Characteristics | Median Value | Min–Max |
|---|---|---|
| Age (in years) | 62 | 31–92 |
| Number of patients | Percentage | |
| Histological subtype | ||
| Serous carcinoma | 74 | 80.4% |
| Mucinous carcinoma | 3 | 3.3% |
| Endometrioid carcinoma | 5 | 5.4% |
| Clear cell carcinoma | 1 | 1.1% |
| Mixed mucinous–endometrioid carcinoma | 1 | 1.1% |
| Carcinosarcoma | 2 | 2.2% |
| Serous borderline tumor | 6 | 6.5% |
| FIGO stage | ||
| I | 27 | 30% |
| II | 10 | 11.1% |
| III | 36 | 40% |
| IV | 17 | 18.9% |
| NA | 2 | |
| Tumor grade | ||
| Low grade | 18 | 21% |
| High grade | 68 | 79% |
| T-status | ||
| T1 | 29 | 32% |
| T2 | 11 | 12% |
| T3 | 50 | 56% |
| NA * | 2 | |
| N-status | ||
| N0 | 39 | 60.9% |
| N1 | 25 | 39.1% |
| Metastasis | ||
| Metastatic cancer | 18 | 19.6% |
| Non-metastatic cancer | 74 | 80.4% |
| Residual disease | ||
| R0 | 25 | 29.1% |
| R1/R2 | 10 | 11.6% |
| Unknown | 51 | 59.3% |
| Event | ||
| Death from disease | 27/80 (follow-up: 0.1–77.9 months, median OS 16.9 months) | 28% |
| Censored | 53/80 (follow-up: 0.3–125.2 months) | 71% |
| Relapse | ||
| Present | 36 | 58.1% |
| Absent | 26 | |
| NA | 30 | |
| Adjuvant chemotherapy | ||
| Platinum | 16 | 20.5% |
| Platinum, Taxane | 30 | 38.5% |
| Platinum, Taxane, Bevacizumab | 21 | 26.9% |
| Platinum, Doxorubicin | 1 | 1.3% |
| None | 10 | 12.8% |
| NA | 14 |
| Positivity Rate * | Median | Min–Max | |
|---|---|---|---|
| Nuclear HDAC-2 | 94.4% | 100 | 0–100 |
| Cytoplasmic HDAC-4 | 80.4% | 30 | 0–95 |
| Cytoplasmic HDAC-5 | 28.1% | 0 | 0–55 |
| Nuclear HDAC-5 | 10% | 0 | 0–45 |
| Variable | Nuclear HDAC-2 | |
|---|---|---|
| Whole Cohort | Serous Tumors | |
| (median, min–max) | (median, min–max) | |
| Histologic type | ||
| Serous histology | 100 (0–100) | |
| Non-serous histology | 80 (30–100) | |
| p = 0.080 | ||
| Grade | ||
| Low | 87.5 (10–100) | 100 (10–100) |
| High | 100 (0–100) | 100 (0–100) |
| p = 0.531 | p = 0.255 | |
| FIGO stage | ||
| I/II | 90 (0–100) | 100 (0–100) |
| III/IV | 100 (0–100) | 100 (0–100) |
| p = 0.169 | p = 0.692 | |
| T-status | ||
| T1 | 100 (0–100) | 100 (0–100) |
| T2 | 85 (0–100) | 100 (0–100) |
| T3 | 100 (0–100) | 100 (0–100) |
| p = 0.417 | p = 0.907 | |
| N-status | ||
| N0 | 100 (0–100) | 100 (0–100) |
| N1 | 90 (0–100) | 90 (0–100) |
| p = 0.081 | p = 0.045 | |
| Metastasis | ||
| Metastatic cancer | 97.5 (0–100) | 97.5 (0–100) |
| Non-metastatic cancer | 100 (0–100) | 100 (0–100) |
| p = 0.819 | p = 0.866 | |
| Relapse | ||
| Present | 100 (0–100) | 100 (0–100) |
| Absent | 100 (0–100) | 100 (0–100) |
| p = 0.967 | p = 0.871 | |
| Variable | Cytoplasmic HDAC-4 | |||
|---|---|---|---|---|
| Whole Cohort | Serous Tumors | |||
| negative | positive | negative | positive | |
| N (%) | N (%) | N (%) | N (%) | |
| Histologic type | ||||
| Serous histology | 3 (27.3%) | 8 (72.7%) | ||
| Non-serous histology | 14 (18.4%) | 62 (81.6%) | ||
| p = 0.443 | ||||
| Grade | ||||
| Low | 1 (5.9%) | 16 (94.1%) | 0 (0%) | 9 (100%) |
| High | 15 (23.1%) | 50 (76.9%) | 13 (20.9%) | 49 (79.1%) |
| p = 0.171 | p = 0.195 | |||
| FIGO stage | ||||
| I/II/III | 11 (16.2%) | 57 (83.8%) | 8 (14%) | 49 (86%) |
| IV | 6 (35.3%) | 11 (64.7%) | 6 (35.3%) | 11 (64.7%) |
| p = 0.070 | p = 0.050 | |||
| T-status | ||||
| T1 | 3 (11.5%) | 23 (88.5%) | 1 (5.3%) | 18 (94.7%) |
| T2/T3 | 11 (22.9%) | 37 (77.1%) | 13 (23.6%) | 42 (76.4%) |
| p = 0.353 | p = 0.078 | |||
| N-status | ||||
| N0 | 3 (8.1%) | 34(91.9%) | 2 (6.45%) | 29 (93.5%) |
| N1 | 6 (25%) | 18 (75%) | 5 (21.7%) | 18 (78.3%) |
| p = 0.069 | p = 0.098 | |||
| Metastasis | ||||
| Metastatic cancer | 6 (33.3%) | 12 (66.7%) | 6 (33.3%) | 12 (66.7%) |
| Non-metastatic cancer | 11 (15.9%) | 58 (84.1%) | 8 (13.8%) | 50 (86.2%) |
| p = 0.097 | p = 0.062 | |||
| Relapse | ||||
| Present | 8 (23.5%) | 26 (76.5%) | 7 (21.2%) | 26 (78.8%) |
| Absent | 3 (13%) | 20 (87%) | 3 (13.6%) | 19 (86.4%) |
| p = 0.325 | p = 0.475 | |||
| Variable | HDAC-5 Expression | |||
|---|---|---|---|---|
| Cytoplasmic | Nuclear | |||
| negative | positive | negative | positive | |
| N (%) | N (%) | N (%) | N (%) | |
| Histologic type | ||||
| Serous histology | 8 (66.7%) | 4 (33.4%) | 11 (91.7%) | 1 (8.3%) |
| Non-serous histology | 56 (72.7%) | 21 (27.3%) | 69 (89.6%) | 8 (10.4%) |
| p = 0.664 | p = 0.826 | |||
| Grade | ||||
| Low | 12 (66.7%) | 3 (33.3%) | 17 (94.4%) | 1 (5.6%) |
| High | 50 (75.8%) | 16 (24.2%) | 59 (89.4%) | 7 (10.6%) |
| p = 0.437 | p = 0.518 | |||
| FIGO stage | ||||
| I/II | 23 (65.7%) | 12 (34.3%) | 31 (88.6%) | 4 (11.4%) |
| III/IV | 39 (75%) | 13 (25%) | 47 (90.4%) | 5 (9.6%) |
| p = 0.348 | p = 0.785 | |||
| T-status | ||||
| T1 | 18 (66.7%) | 9 (33.3%) | 25 (92.6%) | 2 (7.4%) |
| T2/T3 | 44 (73.3%) | 16 (26.7%) | 53 (88.3%) | 7 (11.7%) |
| p = 0.525 | p = 0.546 | |||
| N-status | ||||
| N0 | 30 (78.9%) | 8 (21.1%) | 37 (97.4%) | 1 (2.6%) |
| N1 | 16 (66.7%) | 8 (33.3%) | 20 (83.3%) | 4 (16.7%) |
| p = 0.282 | p = 0.048 | |||
| Metastasis | ||||
| Metastatic cancer | 15 (83.3%) | 3 (16.7%) | 17 (94.4%) | 1 (5.6%) |
| Non-metastatic cancer | 49 (69%) | 22 (31%) | 63 (88.7%) | 8 (11.3%) |
| p = 0.227 | p = 0.473 | |||
| Relapse | ||||
| Present | 27 (75%) | 9 (25%) | 32 (88.9%) | 4 (11.1%) |
| Absent | 15 (62.5%) | 9 (37.5%) | 22 (91.7%) | 2 (8.3%) |
| p = 0.301 | p = 0.725 | |||
| Nuclear HDAC-2 | Cytoplasmic HDAC-4 | Cytoplasmic HDAC-5 | |
|---|---|---|---|
| Cytoplasmic HDAC-4 | rho = −0.09 p = 0.390 | ||
| Cytoplasmic HDAC-5 | rho = −0.03 p = 0.781 | rho = 0.24 p = 0.029 * | |
| Nuclear HDAC-5 | rho = −0.03 p = 0.792 | rho = 0.27 p = 0.012 * | rho = 0.5274 p < 0.001 * |
| Parameter | Entire Cohort | Serous Carcinomas | ||||
|---|---|---|---|---|---|---|
| p-Value | Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | |
| FIGO stage | 0.002 | 2.05 | 1.31–3.22 | 0.001 | 2.5 | 1.46–4.31 |
| T-status | 0.014 | 2.13 | 1.16–3.89 | 0.014 | 2.66 | 1.22–5.80 |
| Histological grade | 0.367 | 1.73 | 0.52–5.76 | 0.043 | 1.81 | 1.02–2.05 |
| Serous histology | 0.060 | 0.31 | 0.08–1.12 | - | - | - |
| Presence of metastasis | 0.116 | 1.98 | 0.82–4.77 | 0.073 | 2.28 | 0.92–5.62 |
| Presence of lymph node metastasis | 0.112 | 2.09 | 0.84–5.22 | 0.183 | 1.96 | 0.72–5.28 |
| Presence of residual disease | 0.052 | 4.17 | 0.98–17.62 | 0.041 | 5.55 | 1.07–28.71 |
| Presence of relapse | 0.019 | 5.77 | 1.34–24.84 | 0.029 | 5.13 | 1.18–22.29 |
| HDAC-2 positivity | 0.789 | 1.31 | 0.17–9.83 | 0.835 | 1.23 | 0.16–9.32 |
| HDAC-4 positivity | 0.113 | 0.48 | 0.20–1.18 | 0.086 | 0.50 | 0.19–1.30 |
| HDAC-5 cytoplasmic positivity | 0.967 | 0.98 | 0.42–2.34 | 0.970 | 0.98 | 0.38–2.49 |
| HDAC-5 nuclear positivity | 0.330 | 1.70 | 0.58–5.01 | 0.512 | 1.51 | 0.44–5.12 |
| Model | Parameter | Hazard Ratio | SE | p-Value | 95% CI | |
|---|---|---|---|---|---|---|
| A (N = 73) | Cytoplasmic HDAC-4 positivity | 0.58 | 0.28 | 0.255 | 0.23 | 1.48 |
| Nuclear HDAC-2 positivity | 1.31 | 1.37 | 0.797 | 0.17 | 10.20 | |
| Nuclear HDAC-5 positivity | 1.85 | 1.73 | 0.509 | 0.30 | 11.56 | |
| Cytoplasmic HDAC-5 positivity | 0.65 | 0.41 | 0.493 | 0.18 | 2.26 | |
| FIGO | 2.06 | 0.54 | 0.006 | 1.23 | 3.45 | |
| B (N = 66) | Cytoplasmic HDAC-4 positivity | 0.64 | 0.33 | 0.381 | 0.23 | 1.75 |
| Nuclear HDAC-2 positivity | 1.20 | 1.27 | 0.861 | 0.15 | 9.56 | |
| Nuclear HDAC-5 positivity | 1.92 | 1.81 | 0.487 | 0.30 | 12.16 | |
| Cytoplasmic HDAC-5 positivity | 0.69 | 0.45 | 0.566 | 0.19 | 2.48 | |
| FIGO | 2.46 | 0.76 | 0.003 | 1.35 | 4.50 | |
| C (N = 46) | Cytoplasmic HDAC-4 positivity | 0.54 | 0.28 | 0.232 | 0.20 | 1.48 |
| Nuclear HDAC-2 positivity | 1.21 | 1.30 | 0.858 | 0.15 | 9.93 | |
| Nuclear HDAC-5 positivity | 2.12 | 1.99 | 0.423 | 0.34 | 13.32 | |
| Cytoplasmic HDAC-5 positivity | 0.75 | 0.49 | 0.662 | 0.21 | 2.69 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levidou, G.; Arsenakis, D.; Bolovis, D.I.; Meyer, R.; Brucker, C.V.M.; Papadopoulos, T.; Theocharis, S. Clinical Significance of the Immunohistochemical Expression of Histone Deacetylases (HDACs)-2, -4, and -5 in Ovarian Adenocarcinomas. Biomedicines 2024, 12, 947. https://doi.org/10.3390/biomedicines12050947
Levidou G, Arsenakis D, Bolovis DI, Meyer R, Brucker CVM, Papadopoulos T, Theocharis S. Clinical Significance of the Immunohistochemical Expression of Histone Deacetylases (HDACs)-2, -4, and -5 in Ovarian Adenocarcinomas. Biomedicines. 2024; 12(5):947. https://doi.org/10.3390/biomedicines12050947
Chicago/Turabian StyleLevidou, Georgia, Dimitrios Arsenakis, Dimitrios I. Bolovis, Roxanne Meyer, Cosima V. M. Brucker, Thomas Papadopoulos, and Stamatios Theocharis. 2024. "Clinical Significance of the Immunohistochemical Expression of Histone Deacetylases (HDACs)-2, -4, and -5 in Ovarian Adenocarcinomas" Biomedicines 12, no. 5: 947. https://doi.org/10.3390/biomedicines12050947