
Angiopoietin-2 and Angiopoietin-like Proteins with a Prospective Role in Predicting Diabetic Nephropathy
 ,
,  , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Anthropometric and Biochemical Measurements
2.3. Quantification of Creatinine and Urinary Protein
2.4. ANGPTL3, 4, and 8 Enzyme-Linked Immunosorbent Assays (ELISAs)
2.5. Quantification of Ang1 and Ang2
2.6. Statistical Analysis
3. Results
3.1. Circulating Angiopoietins 1 and 2 Are Elevated in People with DN
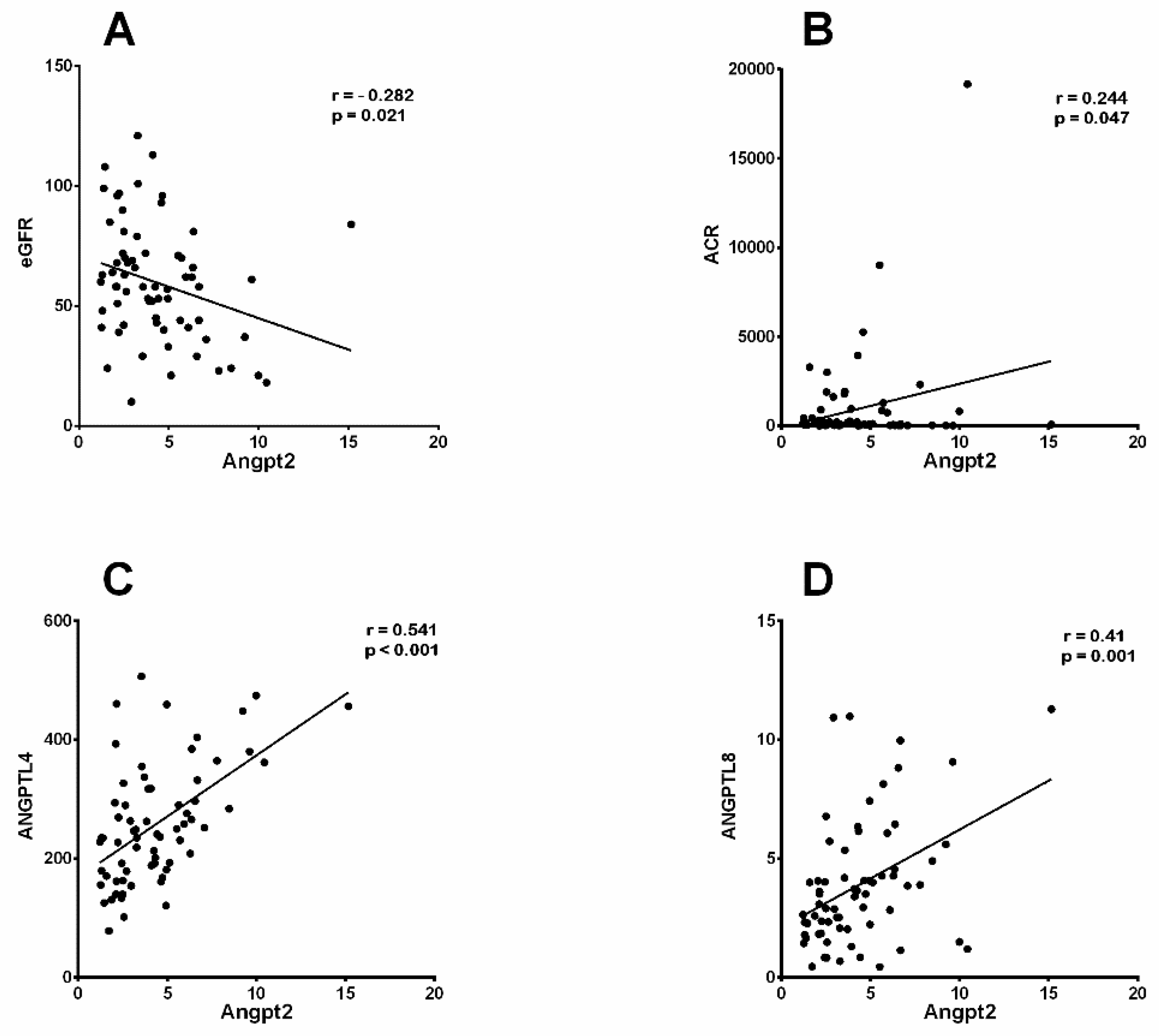
3.2. Increased Ang2 Correlated with Clinical Parameters of DN
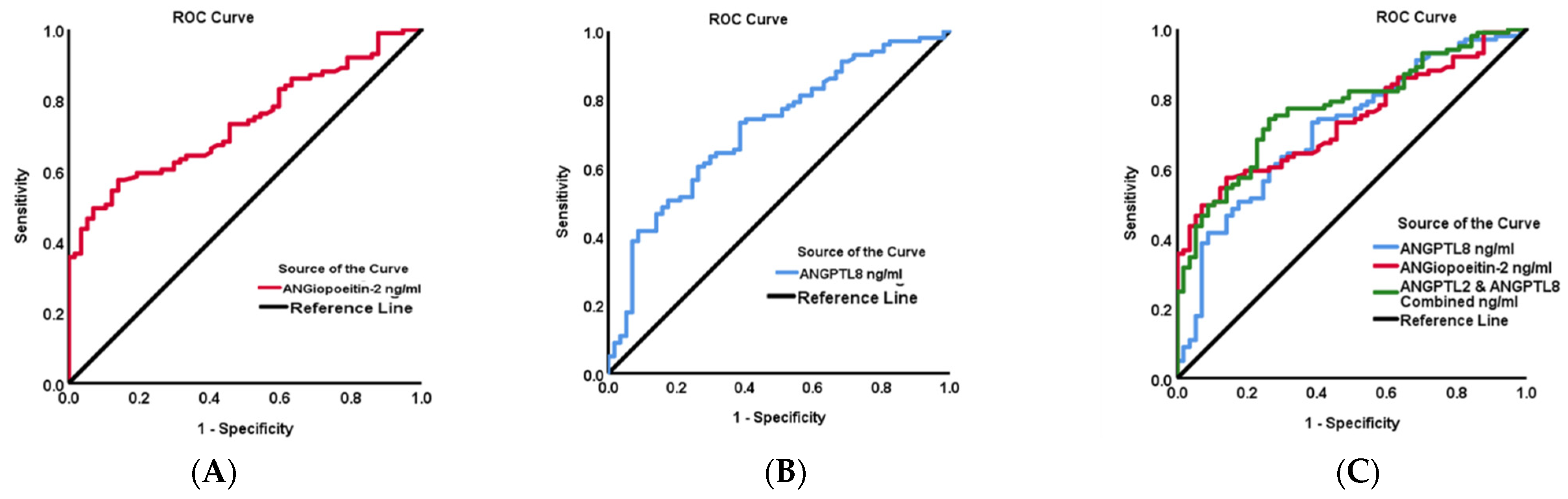
3.3. Predictive Analysis Suggests a Potential Ang2-ANGPTL8 Link with DN
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Koye, D.N.; Magliano, D.J.; Nelson, R.G.; Pavkov, M.E. The Global Epidemiology of Diabetes and Kidney Disease. Adv. Chronic Kidney Dis. 2018, 25, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Alkandari, A.; Alarouj, M.; Elkum, N.; Sharma, P.; Devarajan, S.; Abu-Farha, M.; Al-Mulla, F.; Tuomilehto, J.; Bennakhi, A. Adult Diabetes and Prediabetes Prevalence in Kuwait: Data from the Cross-Sectional Kuwait Diabetes Epidemiology Program. J. Clin. Med. 2020, 9, 3420. [Google Scholar] [CrossRef] [PubMed]
- Qi, C.; Mao, X.; Zhang, Z.; Wu, H. Classification and Differential Diagnosis of Diabetic Nephropathy. J. Diabetes Res. 2017, 2017, 8637138. [Google Scholar] [CrossRef] [PubMed]
- Federation, I.D. IDF Diabetes Atlas. Available online: https://diabetesatlas.org/data/en/country/106/kw.html (accessed on 15 February 2024).
- Brindle, N.P.; Saharinen, P.; Alitalo, K. Signaling and functions of angiopoietin-1 in vascular protection. Circ. Res. 2006, 98, 1014–1023. [Google Scholar] [CrossRef] [PubMed]
- He, F.F.; Zhang, D.; Chen, Q.; Zhao, Y.; Wu, L.; Li, Z.Q.; Zhang, C.; Jiang, Z.H.; Wang, Y.M. Angiopoietin-Tie signaling in kidney diseases: An updated review. FEBS Lett. 2019, 593, 2706–2715. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Popovic, Z.; Chu, C.; Reichetzeder, C.; Pommer, W.; Krämer, B.K.; Hocher, B. Impact of Angiopoietin-2 on Kidney Diseases. Kidney Dis. 2023, 9, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.T.; Khankin, E.V.; Karumanchi, S.A.; Parikh, S.M. Angiopoietin 2 is a partial agonist/antagonist of Tie2 signaling in the endothelium. Mol. Cell. Biol. 2009, 29, 2011–2022. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.S.; Blann, A.D.; Chong, A.Y.; Freestone, B.; Lip, G.Y. Plasma vascular endothelial growth factor, angiopoietin-1, and angiopoietin-2 in diabetes: Implications for cardiovascular risk and effects of multifactorial intervention. Diabetes Care 2004, 27, 2918–2924. [Google Scholar] [CrossRef] [PubMed]
- Bontekoe, J.; Lee, J.; Bansal, V.; Syed, M.; Hoppensteadt, D.; Maia, P.; Walborn, A.; Liles, J.; Brailovsky, E.; Fareed, J. Biomarker Profiling in Stage 5 Chronic Kidney Disease Identifies the Relationship between Angiopoietin-2 and Atrial Fibrillation. Clin. Appl. Thromb./Hemost. Off. J. Int. Acad. Clin. Appl. Thromb./Hemost. 2018, 24, 269s–276s. [Google Scholar] [CrossRef] [PubMed]
- Tsai, Y.C.; Lee, C.S.; Chiu, Y.W.; Lee, J.J.; Lee, S.C.; Hsu, Y.L.; Kuo, M.C. Angiopoietin-2, Renal Deterioration, Major Adverse Cardiovascular Events and All-Cause Mortality in Patients with Diabetic Nephropathy. Kidney Blood Press. Res. 2018, 43, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Tsai, Y.C.; Lee, C.S.; Chiu, Y.W.; Kuo, H.T.; Lee, S.C.; Hwang, S.J.; Kuo, M.C.; Chen, H.C. Angiopoietin-2, Angiopoietin-1 and subclinical cardiovascular disease in Chronic Kidney Disease. Sci. Rep. 2016, 6, 39400. [Google Scholar] [CrossRef] [PubMed]
- Shroff, R.C.; Price, K.L.; Kolatsi-Joannou, M.; Todd, A.F.; Wells, D.; Deanfield, J.; Johnson, R.J.; Rees, L.; Woolf, A.S.; Long, D.A. Circulating angiopoietin-2 is a marker for early cardiovascular disease in children on chronic dialysis. PLoS ONE 2013, 8, e56273. [Google Scholar] [CrossRef] [PubMed]
- Ren, G.; Kim, J.Y.; Smas, C.M. Identification of RIFL, a novel adipocyte-enriched insulin target gene with a role in lipid metabolism. Am. J. Physiol. Endocrinol. Metab. 2012, 303, E334–E351. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Peng, D. ANGPTL8: An Important Regulator in Metabolic Disorders. Front. Endocrinol. 2018, 9, 169. [Google Scholar] [CrossRef]
- Yin, Y.; Ding, X.; Peng, L.; Hou, Y.; Ling, Y.; Gu, M.; Wang, Y.; Peng, Y.; Sun, H. Increased Serum ANGPTL8 Concentrations in Patients with Prediabetes and Type 2 Diabetes. J. Diabetes Res. 2017, 2017, 8293207. [Google Scholar] [CrossRef] [PubMed]
- Abu-Farha, M.; Abubaker, J.; Tuomilehto, J. ANGPTL8 (betatrophin) role in diabetes and metabolic diseases. Diabetes/Metab. Res. Rev. 2017, 33, e2919. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-C.; Susanto, H.; Chuang, W.-H.; Liu, T.-Y.; Wang, C.-H. Higher serum betatrophin level in type 2 diabetes subjects is associated with urinary albumin excretion and renal function. Cardiovasc. Diabetol. 2016, 15, 3. [Google Scholar] [CrossRef] [PubMed]
- Issa, Y.A.; Abd ElHafeez, S.S.; Amin, N.G. The potential role of angiopoietin-like protein-8 in type 2 diabetes mellitus: A possibility for predictive diagnosis and targeted preventive measures? EPMA J. 2019, 10, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Xue, L.; Shuyan, T.; Xiaoli, L.; Zilong, L.; Qiuling, F.; Lining, W.; Yanqiu, L.; Li, Y. Glomerular Proteomic Profiles in the NZB/W F1 Hybrid Mouse Model of Lupus Nephritis. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2019, 25, 2122–2131. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.H.; Deng, A.G.; Li, N.; Song, M.N.; Yang, X.; Liu, J.S. Changes in angiopoietin expression in glomeruli involved in glomerulosclerosis in rats with daunorubicin-induced nephrosis. Acta Pharmacol. Sin. 2006, 27, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.T.; Tipping, P.G.; Li, X.Z.; Long, D.A.; Woolf, A.S. Angiopoietin correlates with glomerular capillary loss in anti-glomerular basement membrane glomerulonephritis. Kidney Int. 2002, 61, 2078–2089. [Google Scholar] [CrossRef]
- Davis, B.; Dei Cas, A.; Long, D.A.; White, K.E.; Hayward, A.; Ku, C.-H.; Woolf, A.S.; Bilous, R.; Viberti, G.; Gnudi, L. Podocyte-Specific Expression of Angiopoietin-2 Causes Proteinuria and Apoptosis of Glomerular Endothelia. J. Am. Soc. Nephrol. 2007, 18, 2320–2329. [Google Scholar] [CrossRef] [PubMed]
- Rizkalla, B.; Forbes, J.M.; Cao, Z.; Boner, G.; Cooper, M.E. Temporal renal expression of angiogenic growth factors and their receptors in experimental diabetes: Role of the renin–angiotensin system. J. Hypertens. 2005, 23, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Maeshima, Y.; Kitayama, H.; Kitamura, S.; Takazawa, Y.; Sugiyama, H.; Yamasaki, Y.; Makino, H. Tumstatin peptide, an inhibitor of angiogenesis, prevents glomerular hypertrophy in the early stage of diabetic nephropathy. Diabetes 2004, 53, 1831–1840. [Google Scholar] [CrossRef] [PubMed]
- Ichinose, K.; Maeshima, Y.; Yamamoto, Y.; Kitayama, H.; Takazawa, Y.; Hirokoshi, K.; Sugiyama, H.; Yamasaki, Y.; Eguchi, K.; Makino, H. Antiangiogenic Endostatin Peptide Ameliorates Renal Alterations in the Early Stage of a Type 1 Diabetic Nephropathy Model. Diabetes 2005, 54, 2891–2903. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Seegar, T.C.; Dalton, A.C.; Tzvetkova-Robev, D.; Goldgur, Y.; Rajashankar, K.R.; Nikolov, D.B.; Barton, W.A. Structural basis for angiopoietin-1-mediated signaling initiation. Proc. Natl. Acad. Sci. USA 2013, 110, 7205–7210. [Google Scholar] [CrossRef] [PubMed]
- Maisonpierre, P.C.; Suri, C.; Jones, P.F.; Bartunkova, S.; Wiegand, S.J.; Radziejewski, C.; Compton, D.; McClain, J.; Aldrich, T.H.; Papadopoulos, N.; et al. Angiopoietin-2, a natural antagonist for Tie2 that disrupts in vivo angiogenesis. Science 1997, 277, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Gale, N.W.; Thurston, G.; Hackett, S.F.; Renard, R.; Wang, Q.; McClain, J.; Martin, C.; Witte, C.; Witte, M.H.; Jackson, D.; et al. Angiopoietin-2 is required for postnatal angiogenesis and lymphatic patterning, and only the latter role is rescued by Angiopoietin-1. Dev. Cell 2002, 3, 411–423. [Google Scholar] [CrossRef]
- Fiedler, U.; Scharpfenecker, M.; Koidl, S.; Hegen, A.; Grunow, V.; Schmidt, J.M.; Kriz, W.; Thurston, G.; Augustin, H.G. The Tie-2 ligand angiopoietin-2 is stored in and rapidly released upon stimulation from endothelial cell Weibel-Palade bodies. Blood 2004, 103, 4150–4156. [Google Scholar] [CrossRef] [PubMed]
- Krikun, G.; Schatz, F.; Finlay, T.; Kadner, S.; Mesia, A.; Gerrets, R.; Lockwood, C.J. Expression of Angiopoietin-2 by Human Endometrial Endothelial Cells: Regulation by Hypoxia and Inflammation. Biochem. Biophys. Res. Commun. 2000, 275, 159–163. [Google Scholar] [CrossRef]
- Hakanpaa, L.; Sipila, T.; Leppanen, V.-M.; Gautam, P.; Nurmi, H.; Jacquemet, G.; Eklund, L.; Ivaska, J.; Alitalo, K.; Saharinen, P. Endothelial destabilization by angiopoietin-2 via integrin β1 activation. Nat. Commun. 2015, 6, 5962. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Lee, K.; Chuang, P.Y.; Liu, Z.; He, J.C. Glomerular endothelial cell injury and cross talk in diabetic kidney disease. Am. J. Physiol. Ren. Physiol. 2015, 308, F287–F297. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Li, H.; Zhang, C.; Li, Z.; Wang, Q.; Guo, J.; Luo, C.; Wang, Y. Urinary angiopoietin-2 is associated with albuminuria in patients with type 2 diabetes mellitus. Int. J. Endocrinol. 2015, 2015, 163120. [Google Scholar] [CrossRef] [PubMed]
- Abu-Farha, M.; Abubaker, J.; Al-Khairi, I.; Cherian, P.; Noronha, F.; Hu, F.B.; Behbehani, K.; Elkum, N. Higher plasma betatrophin/ANGPTL8 level in Type 2 Diabetes subjects does not correlate with blood glucose or insulin resistance. Sci. Rep. 2015, 5, 10949. [Google Scholar] [CrossRef]
- Al-Shawaf, E.; Al-Ozairi, E.; Al-Asfar, F.; Al-Beloushi, S.; Kumari, S.; Tuomilehto, J.; Arefanian, H. Biphasic changes in angiopoietin-like 8 level after laparoscopic sleeve gastrectomy and type 2 diabetes remission during a 1-year follow-up. Surg. Obes. Relat. Dis. Off. J. Am. Soc. Bariatr. Surg. 2018, 14, 1284–1294. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Lu, P.; He, W.; Zhang, J.; Liu, L.; Yang, Y.; Liu, Z.; Xie, J.; Shao, S.; Du, T.; et al. Circulating betatrophin levels are increased in patients with type 2 diabetes and associated with insulin resistance. J. Clin. Endocrinol. Metab. 2015, 100, E96–E100. [Google Scholar] [CrossRef]
- Fu, Z.; Berhane, F.; Fite, A.; Seyoum, B.; Abou-Samra, A.B.; Zhang, R. Elevated circulating lipasin/betatrophin in human type 2 diabetes and obesity. Sci. Rep. 2014, 4, 5013. [Google Scholar] [CrossRef]
- Gao, T.; Jin, K.; Chen, P.; Jin, H.; Yang, L.; Xie, X.; Yang, M.; Hu, C.; Yu, X. Circulating Betatrophin Correlates with Triglycerides and Postprandial Glucose among Different Glucose Tolerance Statuses—A Case-Control Study. PLoS ONE 2015, 10, e0133640. [Google Scholar] [CrossRef] [PubMed]
- Yamada, H.; Saito, T.; Aoki, A.; Asano, T.; Yoshida, M.; Ikoma, A.; Kusaka, I.; Toyoshima, H.; Kakei, M.; Ishikawa, S.E. Circulating betatrophin is elevated in patients with type 1 and type 2 diabetes. Endocr. J. 2015, 62, 417–421. [Google Scholar] [CrossRef]
- Zou, H.; Xu, Y.; Chen, X.; Yin, P.; Li, D.; Li, W.; Xie, J.; Shao, S.; Liu, L.; Yu, X. Predictive values of ANGPTL8 on risk of all-cause mortality in diabetic patients: Results from the REACTION Study. Cardiovasc. Diabetol. 2020, 19, 121. [Google Scholar] [CrossRef]
- AlMajed, H.T.; Abu-Farha, M.; Alshawaf, E.; Devarajan, S.; Alsairafi, Z.; Elhelaly, A.; Cherian, P.; Al-Khairi, I.; Ali, H.; Jose, R.M.; et al. Increased Levels of Circulating IGFBP4 and ANGPTL8 with a Prospective Role in Diabetic Nephropathy. Int. J. Mol. Sci. 2023, 24, 14244. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Song, J.; Zhang, X.; Xiao, L.; Hu, X.; Pan, H.; Qin, L.; Liu, H.; Ge, B.; Zheng, T. Association of Serum Angiopoietin-like Protein 8 with Albuminuria in Type 2 Diabetic Patients: Results from the GDMD Study in China. Front. Endocrinol. 2018, 9, 414. [Google Scholar] [CrossRef] [PubMed]
- Al Shawaf, E.; Abu-Farha, M.; Devarajan, S.; Alsairafi, Z.; Al-Khairi, I.; Cherian, P.; Ali, H.; Mathur, A.; Al-Mulla, F.; Al Attar, A.; et al. ANGPTL4: A Predictive Marker for Diabetic Nephropathy. J. Diabetes Res. 2019, 2019, 4943191. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | T2D | DN | p Value |
|---|---|---|---|
| N = 50 | N = 67 | ||
| Gender (M/F) | 18/32 | 45/22 | |
| Age (years) | 58.96 ± 1.02 | 60.09 ± 1.38 | 0.512 |
| BMI (kg/m2) | 33.94 ± 0.88 | 34.23 ± 0.85 | 0.816 |
| SBP (mmHg) | 132.98 ± 3.88 | 132.03 ± 3.41 | 0.911 |
| DBP (mmHg) | 69.72 ± 2.26 | 68.78 ± 1.98 | 0.909 |
| Height (cm) | 161.90 ± 1.30 | 162.04 ± 3.64 | 0.004 |
| Weight (kg) | 88.79 ± 2.35 | 92.03 ± 2.79 | 0.055 |
| Fasting Glucose (mmol/L) | 8.27 ± 0.36 | 9.61 ± 0.48 | 0.028 |
| HbA1C (%) | 9.53 ± 1.73 | 8.09 ± 0.22 | 0.415 |
| TChol (mmol/L) | 4.15 ± 0.13 | 4.02 ± 0.12 | 0.472 |
| TG (mmol/L) | 1.41 ± 0.16 | 1.77 ± 0.11 | 0.066 |
| HDL-C (mmol/L) | 1.25 ± 0.05 | 1.13 ± 0.03 | 0.067 |
| LDL-C (mmol/L) | 2.28 ± 0.11 | 2.10 ± 0.10 | 0.203 |
| VLDL (mmol/L) | 0.56 ± 0.06 | 0.71 ± 0.04 | 0.067 |
| C Peptide (pg/mL) | 0.65 ± 0.05 | 0.77 ± 0.06 | 0.136 |
| Serum Creatinine (mg/L) | 79.42 ± 3.54 | 118.36 ± 6.57 | 0.001 |
| eGFR (ml/min/1.73 m2) | 79.22 ± 3.19 | 59.70 ± 3.00 | 0.001 |
| BUN | 5.10 ± 0.29 | 7.53 ± 0.52 | 0.001 |
| Albumin (mcg/L) | 37.94 ± 0.50 | 37.28 ± 0.42 | 0.316 |
| Insulin (mU/L) | 22.08 ± 3.13 | 22.22 ± 1.93 | 0.969 |
| ACR | 137.27 ± 69.22 | 569.94 ± 174.39 | 0.005 |
| Urine Creatinine (mg/day) | 11.38 ± 0.84 | 10.17 ± 0.91 | 0.015 |
| Microalbumin (mg/day) | 157.58 ± 85.09 | 460.34 ± 169.37 | 0.001 |
| Ang1 | ||||
|---|---|---|---|---|
| Parameters | T2D | DN | ||
| r | p | r | p | |
| Age (years) | −0.036 | 0.808 | −0.045 | 0.715 |
| BMI (kg/m2) | 0.151 | 0.301 | −0.001 | 0.994 |
| SBP (mmHg) | 0.177 | 0.228 | 0.024 | 0.852 |
| DBP (mmHg) | −0.121 | 0.414 | 0.007 | 0.957 |
| Fasting Glucose (mmol/L) | 0.079 | 0.591 | −0.042 | 0.735 |
| HbA1C (%) | −0.003 | 0.985 | −0.140 | 0.257 |
| T. Chol (mmol/L) | −0.083 | 0.570 | 0.047 | 0.703 |
| TGL (mmol/L) | 0.061 | 0.675 | 0.009 | 0.941 |
| HDL (mmol/L) | −0.175 | 0.228 | 0.073 | 0.556 |
| LDL (mmol/L) | −0.078 | 0.599 | 0.020 | 0.872 |
| VLDL (mmol/L) | 0.063 | 0.667 | 0.008 | 0.952 |
| C peptide (pg/mL) | −0.014 | 0.927 | −0.049 | 0.696 |
| Serum Creatinine (mg/L) | 0.291 | 0.043 | −0.049 | 0.696 |
| eGFR (mL/min/1.73 m2) | −0.225 | 0.123 | 0.018 | 0.883 |
| BUN | 0.198 | 0.174 | −0.069 | 0.581 |
| Albumin (mcg/L) | −0.274 | 0.057 | −0.246 | 0.045 |
| Insulin (mU/L) | −0.013 | 0.931 | 0.131 | 0.291 |
| ACR (mg/g) | 0.065 | 0.659 | 0.177 | 0.152 |
| Urine Creatinine (mg/day) | −0.002 | 0.991 | −0.014 | 0.909 |
| Microalbumin (mg/day) | 0.057 | 0.697 | 0.353 | 0.003 |
| Ang2 (ng/mL) | 0.197 | 0.175 | 0.093 | 0.455 |
| ANGPTL3 (ng/mL) | 0.235 | 0.104 | 0.257 | 0.036 |
| ANGPTL4 (ng/mL) | 0.138 | 0.343 | −0.002 | 0.986 |
| ANGPTL8 (ng/mL) | 0.214 | 0.139 | 0.089 | 0.472 |
| Ang2 | ||||
|---|---|---|---|---|
| Parameters | T2D | DN | ||
| r | p | r | p | |
| Age (years) | 0.277 | 0.054 | 0.135 | 0.277 |
| BMI (kg/m2) | 0.240 | 0.096 | 0.070 | 0.580 |
| SBP (mmHg) | 0.013 | 0.932 | −0.280 | 0.024 |
| DBP (mmHg) | −0.211 | 0.150 | −0.209 | 0.095 |
| Fasting Glucose (mmol/L) | 0.203 | 0.162 | 0.100 | 0.419 |
| HbA1C (%) | −0.024 | 0.871 | 0.028 | 0.820 |
| T. Chol (mmol/L) | −0.204 | 0.159 | −0.007 | 0.955 |
| TGL (mmol/L) | 0.063 | 0.669 | 0.196 | 0.113 |
| HDL (mmol/L) | −0.176 | 0.227 | −0.049 | 0.692 |
| LDL (mmol/L) | −0.221 | 0.132 | −0.099 | 0.428 |
| VLDL (mmol/L) | 0.063 | 0.666 | 0.195 | 0.114 |
| C peptide (pg/mL) | 0.032 | 0.827 | −0.047 | 0.706 |
| Serum Creatinine (mg/L) | 0.300 | 0.036 | 0.215 | 0.081 |
| eGFR (mL/min/1.73 m2) | −0.307 | 0.034 | −0.282 | 0.021 |
| BUN | 0.320 | 0.025 | 0.236 | 0.054 |
| Albumin(mcg/L) | −0.220 | 0.129 | −0.189 | 0.126 |
| Insulin (mU/L) | −0.060 | 0.683 | −0.017 | 0.889 |
| ACR (mg/g) | 0.157 | 0.281 | 0.244 | 0.047 |
| Urine Creatinine (mg/day) | −0.160 | 0.272 | −0.157 | 0.204 |
| Microalbumin (mg/day) | −0.040 | 0.783 | 0.092 | 0.461 |
| Ang1 (ng/mL) | 0.197 | 0.175 | 0.093 | 0.455 |
| ANGPTL3 (ng/mL) | −0.123 | 0.401 | 0.190 | 0.123 |
| ANGPTL4 (ng/mL) | 0.555 | 0.001 | 0.541 | 0.001 |
| ANGPTL8 (ng/mL) | 0.020 | 0.889 | 0.410 | 0.001 |
| Parameters | T2D | DN | ||
|---|---|---|---|---|
| β Coefficient | p Value | β Coefficient | p Value | |
| SBP | −0.047 | 0.706 | −0.273 | 0.012 |
| ACR | 0.078 | 0.535 | 0.345 | 0.002 |
| ANGPTL4 | 0.552 | <0.001 | 0.082 | 0.614 |
| ANGPTL8 | −0.099 | 0.438 | 0.424 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshawaf, E.; Abu-Farha, M.; Mohammad, A.; Devarajan, S.; Al-Khairi, I.; Cherian, P.; Ali, H.; Al-Matrouk, H.; Al-Mulla, F.; Al Attar, A.; et al. Angiopoietin-2 and Angiopoietin-like Proteins with a Prospective Role in Predicting Diabetic Nephropathy. Biomedicines 2024, 12, 949. https://doi.org/10.3390/biomedicines12050949
Alshawaf E, Abu-Farha M, Mohammad A, Devarajan S, Al-Khairi I, Cherian P, Ali H, Al-Matrouk H, Al-Mulla F, Al Attar A, et al. Angiopoietin-2 and Angiopoietin-like Proteins with a Prospective Role in Predicting Diabetic Nephropathy. Biomedicines. 2024; 12(5):949. https://doi.org/10.3390/biomedicines12050949
Chicago/Turabian StyleAlshawaf, Eman, Mohamed Abu-Farha, Anwar Mohammad, Sriraman Devarajan, Irina Al-Khairi, Preethi Cherian, Hamad Ali, Hawra Al-Matrouk, Fahd Al-Mulla, Abdulnabi Al Attar, and et al. 2024. "Angiopoietin-2 and Angiopoietin-like Proteins with a Prospective Role in Predicting Diabetic Nephropathy" Biomedicines 12, no. 5: 949. https://doi.org/10.3390/biomedicines12050949