
Emerging Therapeutic Potential of Nanoparticles in Pancreatic Cancer: A Systematic Review of Clinical Trials


 , and
, and
Abstract
:1. Introduction
2. Methods Section
2.1. Literature Search
2.2. Inclusion/Exclusion Criteria
2.3. Data Collection
2.4. Quality of Methods Assessment
3. Results
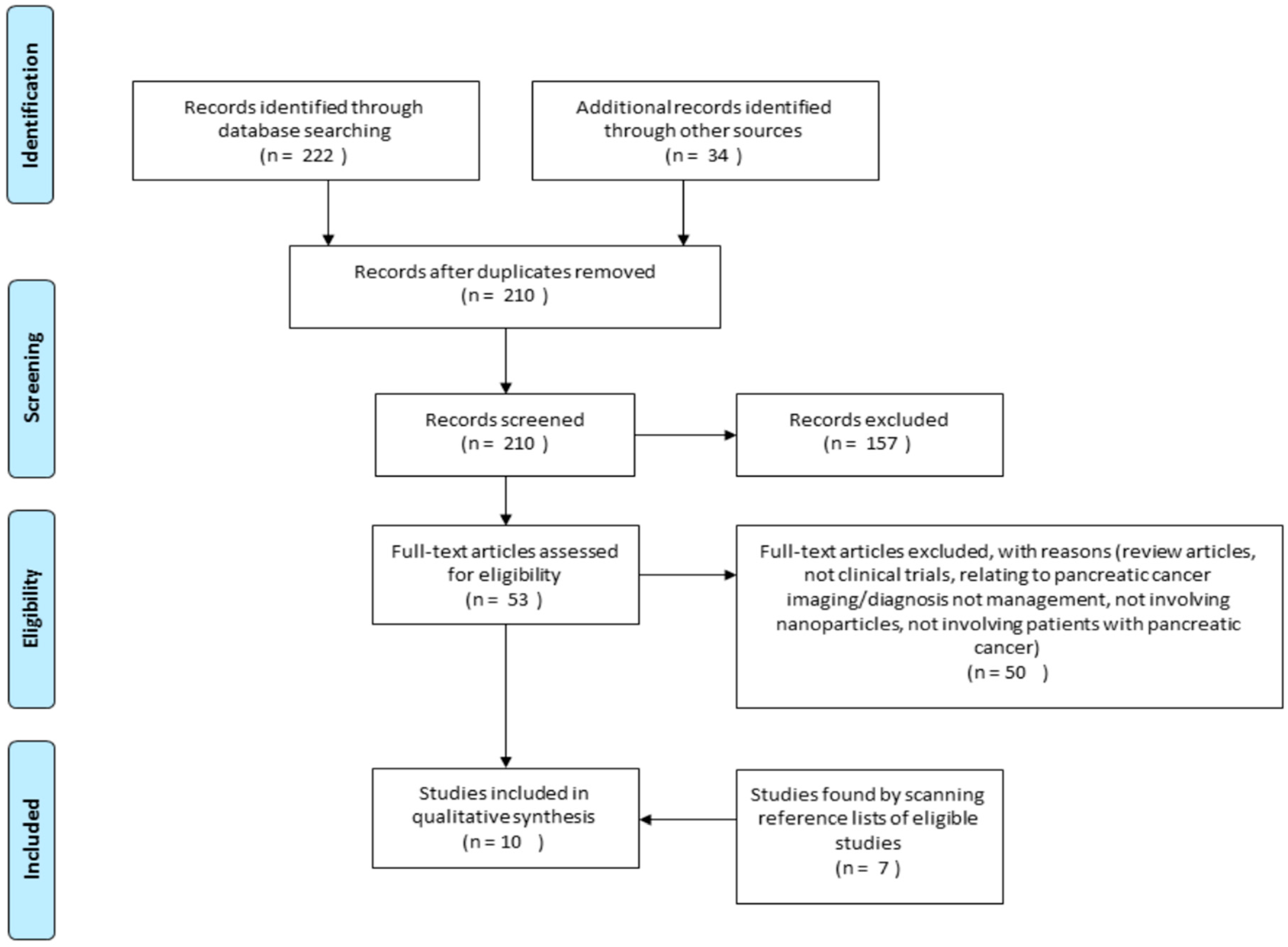
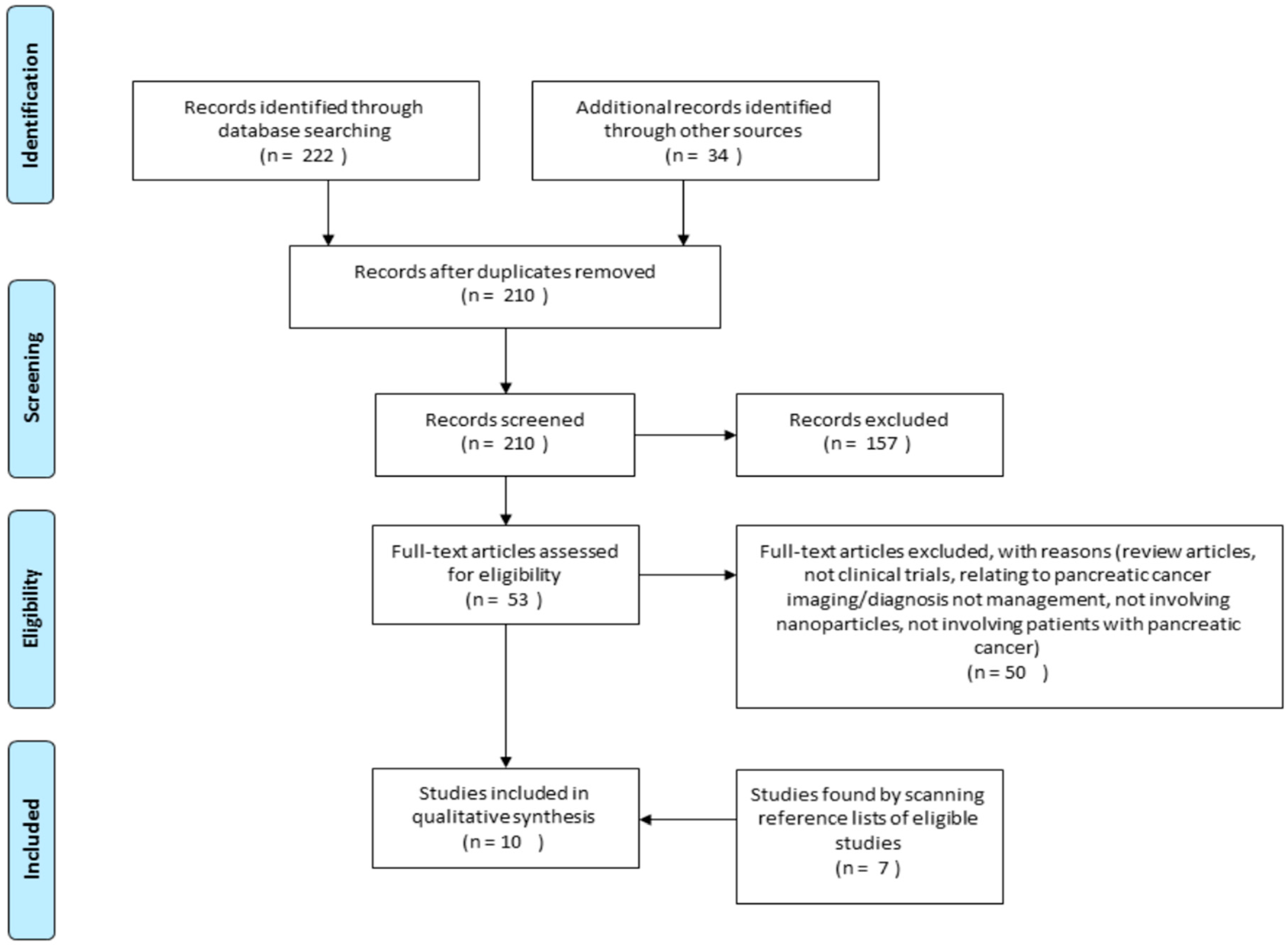
3.1. Study Selection
3.2. Study Characteristics
4. Synthesis of Study Results
4.1. Nanoparticle Albumin Bound Paclitaxel
4.2. Pathotrophic Nanoparticle Gene Delivery
4.3. Gold Nanoparticles
4.4. Micelle Nanoparticles
4.5. Liposomal Nanoparticles
4.6. Quality of Methods of Included Studies
5. Discussion
5.1. Current Progress
5.2. Limitations
5.3. Future Research
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| % | percentage |
| CI | confidence interval |
| FDG | fluorodeoxyglucose |
| IV | intravenous |
| mg/m2 | milligram per meter square |
| nab-paclitaxel | nanoparticle albumin bound-paclitaxel |
| RCT | randomised control trials |
| PET | positron emission tomography |
References
- Robotin, M.C.; Jones, S.C.; Biankin, A.V.; Waters, L.; Iverson, D.; Gooden, H.; Barraclough, B.; Penman, A.G. Defining research priorities for pancreatic cancer in Australia: Results of a consensus development process. Cancer Causes Control 2010, 21, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in globocan 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Hariharan, D.; Saied, A.; Kocher, H. Analysis of mortality rates for pancreatic cancer across the world. HPB 2008, 10, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Ansari, D.; Chen, B.-C.; Dong, L.; Zhou, M.-T.; Andersson, R. Pancreatic cancer: Translational research aspects and clinical implications. World J. Gastroenterol. 2012, 18, 1417–1424. [Google Scholar] [CrossRef] [PubMed]
- Tingstedt, B.; Weitkamper, C.; Andersson, R. Early onset pancreatic cancer: A controlled trial. Ann. Gastroenterol. 2011, 24, 206–212. [Google Scholar] [PubMed]
- Australian Institute of Health and Welfere; Australasian Association of Cancer Registries. Cancer in Australia: An Overview 2012; Australian Institute of Health and Welfare: Canberra, Australia, 2012. [Google Scholar]
- Gordon, E.M.; Lopez, F.F.; Cornelio, G.H.; Lorenzo, C.C.; Levy, J.P.; Reed, R.A.; Liu, L.; Bruckner, H.W.; Hall, F.L. Pathotropic nanoparticles for cancer gene therapy Rexin-G™ IV: Three-year clinical experience. Int. J. Oncol. 2006, 29, 1053–1064. [Google Scholar] [CrossRef] [PubMed]
- Hosein, P.J.; de Lima Lopes, G., Jr.; Pastorini, V.H.; Gomez, C.; Macintyre, J.; Zayas, G.; Reis, I.; Montero, A.J.; Merchan, J.R.; Rocha Lima, C.M. A phase II trial of nab-paclitaxel as second-line therapy in patients with advanced pancreatic cancer. Am. J. Clin. Oncol. 2013, 36, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Zhang, Y.; Chen, C.; Yao, Q.; Li, M. Targeted drug delivery in pancreatic cancer. Biochim. Biophys. Acta 2010, 1805, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Shaib, Y.H.; Davila, J.A.; El-Serag, H.B. The epidemiology of pancreatic cancer in the united states: Changes below the surface. Aliment. Pharmacol. Ther. 2006, 24, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Oberstein, P.E.; Olive, K.P. Pancreatic cancer: Why is it so hard to treat? Ther. Adv. Gastroenterol. 2013, 6, 321–337. [Google Scholar] [CrossRef] [PubMed]
- Buzea, C.; Pacheco, I.I.; Robbie, K. Nanomaterials and nanoparticles: Sources and toxicity. Biointerphases 2007, 2. [Google Scholar] [CrossRef]
- Jain, K. Advances in the field of nanooncology. BMC Med. 2010, 8. [Google Scholar] [CrossRef] [PubMed]
- Malekigorji, M.; Curtis, A.; Hoskins, C. The use of iron oxide nanoparticles for pancreatic cancer therapy. J. Nanomed. Res. 2014, 1. [Google Scholar] [CrossRef]
- Kunjachan, S.; Pola, R.; Gremse, F.; Theek, B.; Ehling, J.; Moeckel, D.; Hermanns-Sachweh, B.; Pechar, M.; Ulbrich, K.; Hennink, W.E.; et al. Passive versus active tumor targeting using RGD- and NGR-modified polymeric nanomedicines. Nano Lett. 2014, 14, 972–981. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Madhunapantula, S.V.; Robertson, G.P. Toxicological considerations when creating nanoparticle based drugs and drug delivery systems? Expert Opin. Drug Metab. Toxicol. 2012, 8, 47–69. [Google Scholar] [CrossRef] [PubMed]
- Dokka, S.; Toledo, D.; Shi, X.; Castranova, V.; Rojanasakul, Y. Oxygen radical-mediated pulmonary toxicity induced by some cationic liposomes. Pharm. Res. 2000, 17, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Lv, H.; Zhang, S.; Wang, B.; Cui, S.; Yan, J. Toxicity of cationic lipids and cationic polymers in gene delivery. J. Control. Release 2006, 114, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Keelan, J.A. Nanotoxicology: Nanoparticles versus the placenta. Nat. Nanotechnol. 2011, 6, 263–264. [Google Scholar] [CrossRef] [PubMed]
- Chang, C. The immune effects of naturally occurring and synthetic nanoparticles. J. Autoimmun. 2010, 34, J234–J246. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S.; Mahmoudi, M. Superparamagnetic iron oxide nanoparticles: Promises for diagnosis and treatment of cancer. Int. J. Mol. Epidemiol. Genet. 2011, 2, 367–390. [Google Scholar] [PubMed]
- Wang, C.; Zhang, H.; Chen, B.; Yin, H.; Wang, W. Study of the enhanced anticancer efficacy of gambogic acid on Capan-1 pancreatic cancer cells when mediated via magnetic Fe3O4 nanoparticles. Int. J. Nanomed. 2011, 6, 1929–1935. [Google Scholar]
- Papa, A.-L.; Basu, S.; Sengupta, P.; Banerjee, D.; Sengupta, S.; Harfouche, R. Mechanistic studies of gemcitabine-loaded nanoplatforms in resistant pancreatic cancer cells. BMC Cancer 2012, 12. [Google Scholar] [CrossRef] [PubMed]
- Gannon, C.J.; Patra, C.R.; Bhattacharya, R.; Mukherjee, P.; Curley, S.A. Intracellular gold nanoparticles enhance non-invasive radiofrequency thermal destruction of human gastrointestinal cancer cells. J. Nanobiotechnol. 2008, 6. [Google Scholar] [CrossRef] [PubMed]
- Ristorcelli, E.; Beraud, E.; Verrando, P.; Villard, C.; Lafitte, D.; Sbarra, V.; Lombardo, D.; Verine, A. Human tumor nanoparticles induce apoptosis of pancreatic cancer cells. FASEB J. 2008, 22, 3358–3369. [Google Scholar] [CrossRef] [PubMed]
- Kudgus, R.A.; Szabolcs, A.; Khan, J.A.; Walden, C.A.; Reid, J.M.; Robertson, J.D.; Bhattacharya, R.; Mukherjee, P. Inhibiting the growth of pancreatic adenocarcinoma in vitro and in vivo through targeted treatment with designer gold nanotherapeutics. PLoS ONE 2013, 8, e57522. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Liong, M.; Zink, J.I.; Tamanoi, F. Mesoporous silica nanoparticles as a delivery system for hydrophobic anticancer drugs. Small 2007, 3, 1341–1346. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, M.; Takimoto, R.; Murase, K.; Sato, Y.; Hirakawa, M.; Tamura, F.; Sato, T.; Iyama, S.; Osuga, T.; Miyanishi, K. Targeting anticancer drug delivery to pancreatic cancer cells using a fucose-bound nanoparticle approach. PLoS ONE 2012, 7, e39545. [Google Scholar] [CrossRef] [PubMed]
- Patra, C.R.; Bhattacharya, R.; Wang, E.; Katarya, A.; Lau, J.S.; Dutta, S.; Muders, M.; Wang, S.; Buhrow, S.A.; Safgren, S.L. Targeted delivery of gemcitabine to pancreatic adenocarcinoma using cetuximab as a targeting agent. Cancer Res. 2008, 68, 1970–1978. [Google Scholar] [CrossRef] [PubMed]
- Glazer, E.S.; Zhu, C.; Massey, K.L.; Thompson, C.S.; Kaluarachchi, W.D.; Hamir, A.N.; Curley, S.A. Noninvasive radiofrequency field destruction of pancreatic adenocarcinoma xenografts treated with targeted gold nanoparticles. Clin. Cancer Res. 2010, 16, 5712–5721. [Google Scholar] [CrossRef] [PubMed]
- Frese, K.K.; Neesse, A.; Cook, N.; Bapiro, T.E.; Lolkema, M.P.; Jodrell, D.I.; Tuveson, D.A. Nab-paclitaxel potentiates gemcitabine activity by reducing cytidine deaminase levels in a mouse model of pancreatic cancer. Cancer Discov. 2012, 2, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.A.; Kudgus, R.A.; Szabolcs, A.; Dutta, S.; Wang, E.; Cao, S.; Curran, G.L.; Shah, V.; Curley, S.; Mukhopadhyay, D. Designing nanoconjugates to effectively target pancreatic cancer cells in vitro and in vivo. PLoS ONE 2011, 6, e20347. [Google Scholar] [CrossRef] [PubMed]
- Batist, G.; Gelmon, K.A.; Chi, K.N.; Miller, W.H.; Chia, S.K.; Mayer, L.D.; Swenson, C.E.; Janoff, A.S.; Louie, A.C. Safety, pharmacokinetics, and efficacy of CPX-1 liposome injection in patients with advanced solid tumors. Clin. Cancer Res. 2009, 15, 692–700. [Google Scholar] [CrossRef] [PubMed]
- Seymour, L.W.; Ferry, D.R.; Kerr, D.J.; Rea, D.; Whitlock, M.; Poyner, R.; Boivin, C.; Hesslewood, S.; Twelves, C.; Blackie, R. Phase II studies of polymer-doxorubicin (PK1, FCE28068) in the treatment of breast, lung and colorectal cancer. Int. J. Oncol. 2009, 34, 1629–1636. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, Y.; Gotoh, M.; Muro, K.; Yamada, Y.; Shirao, K.; Shimada, Y.; Okuwa, M.; Matsumoto, S.; Miyata, Y.; Ohkura, H. Phase I and pharmacokinetic study of MCC-465, a doxorubicin (DXR) encapsulated in peg immunoliposome, in patients with metastatic stomach cancer. Ann. Oncol. 2004, 15, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Gradishar, W. Superior efficacy of albumin-bound paclitaxel, ABI-007, compared with polythylated castor oil-based pclitaxel in women with metastatic breast cancer: Results of a phase III trial. J. Clin. Oncol. 2005, 23, 5983–5992. [Google Scholar] [CrossRef] [PubMed]
- Valle, J.W.; Armstrong, A.; Newman, C.; Alakhov, V.; Pietrzynski, G.; Brewer, J.; Campbell, S.; Corrie, P.; Rowinsky, E.K.; Ranson, M. A phase 2 study of SP1049C, doxorubicin in P-glycoprotein-targeting pluronics, in patients with advanced adenocarcinoma of the esophagus and gastroesophageal junction. Investig. New Drugs 2011, 29, 1029–1037. [Google Scholar] [CrossRef] [PubMed]
- Liberatti, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.; Ioannidis, J. The PRISMA statement for reporting systematic review and meta-analysis of studies that evaluate healthcare interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151. [Google Scholar] [CrossRef]
- Halpern, S.H.; Joanne Douglas, M. Jadad scale for reporting randomized controlled trials. In Evidence-Based Obstetric Anesthesia; Halpern, S.H., Joanne Douglas, M., Eds.; Blackwell Publishing: Malden, MA, USA, 2005; pp. 237–238. [Google Scholar]
- Centre for Evidence-Based Medicine. Therapy Critical Appraisal Worksheet. Canadian Institute of Health Research. Available online: http://ktclearinghouse.ca/cebm/teaching/worksheets/therapy (accessed on 30 March 2015).
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [PubMed]
- Von Hoff, D.D.; Ramanathan, R.K.; Borad, M.J.; Laheru, D.A.; Smith, L.S.; Wood, T.E.; Korn, R.L.; Desai, N.; Trieu, V.; Iglesias, J.L. Gemcitabine plus nab-paclitaxel is an active regimen in patients with advanced pancreatic cancer: A phase I/II trial. J. Clin. Oncol. 2011, 29, 4548–4554. [Google Scholar] [CrossRef] [PubMed]
- Gordon, E.M.; Cornelio, G.H.; Lorenzo, C.C.; Levy, J.P.; Reed, R.A.; Liu, L.; Hall, F.L. First clinical experience using a ‘pathotropic’ injectable retroviral vector (Rexin-G) as intervention for stage IV pancreatic cancer. Int. J. Oncol. 2004, 24, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Hamaguchi, T.; Kato, K.; Yasui, H.; Morizane, C.; Ikeda, M.; Ueno, H.; Muro, K.; Yamada, Y.; Okusaka, T.; Shirao, K. A phase I and pharmacokinetic study of NK105, a paclitaxel-incorporating micellar nanoparticle formulation. Br. J. Cancer 2007, 97, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Stathopoulos, G.P.; Boulikas, T.; Vougiouka, M.; Rigatos, S.K.; Stathopoulos, J.G. Liposomal cisplatin combined with gemcitabine in pretreated advanced pancreatic cancer patients: A phase I-II study. Oncol. Rep. 2006, 15, 1201–1204. [Google Scholar] [CrossRef] [PubMed]
- Libutti, S.K.; Paciotti, G.F.; Byrnes, A.A.; Alexander, H.R.; Gannon, W.E.; Walker, M.; Seidel, G.D.; Yuldasheva, N.; Tamarkin, L. Phase I and pharmacokinetic studies of CYT-6091, a novel PEGylated colloidal gold-rhTNF nanomedicine. Clin. Cancer Res. 2010, 16, 6139–6149. [Google Scholar] [CrossRef] [PubMed]
- Galanis, E.; Carlson, S.K.; Foster, N.R.; Lowe, V.; Quevedo, F.; McWilliams, R.R.; Grothey, A.; Jatoi, A.; Alberts, S.R.; Rubin, J. Phase I trial of a pathotropic retroviral vector expressing a cytocidal cyclin G1 construct (Rexin-G) in patients with advanced pancreatic cancer. Mol. Ther. 2008, 16, 979–984. [Google Scholar] [CrossRef] [PubMed]
- Chawla, S.P.; Chua, V.S.; Fernandez, L.; Quon, D.; Blackwelder, W.C.; Gordon, E.M.; Hall, F.L. Advanced phase I/II studies of targeted gene delivery in vivo: Intravenous Rexin-G for gemcitabine-resistant metastatic pancreatic cancer. Mol. Ther. 2010, 18, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Kratz, F. Albumin as a drug carrier: Design of prodrugs, drug conjugates and nanoparticles. J. Control. Release 2008, 132, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Torchilin, V.P. Multifunctional nanocarriers. Adv. Drug Deliv. Rev. 2006, 58, 1532–1555. [Google Scholar] [CrossRef] [PubMed]
- Stathopoulos, G.P.; Boulikas, T.; Vougiouka, M.; Deliconstantinos, G.; Rigatos, S.; Darli, E.; Viliotou, V.; Stathopoulos, J.G. Pharmacokinetics and adverse reactions of a new liposomal cisplatin (lipoplatin): Phase I study. Oncol. Rep. 2005, 13, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Berlin, J.D.; Catalano, P.; Thomas, J.P.; Kugler, J.W.; Haller, D.G. Phase III study of gemcitabine in combination with fluorouracil versus gemcitabine alone in patients with advanced pancreatic carcinoma: Eastern cooperative oncology group trial E2297. J. Clin. Oncol. 2002, 20, 3270–3275. [Google Scholar] [CrossRef] [PubMed]
- Lima, C.M.R.; Green, M.R.; Rotche, R.; Miller, W.H.; Jeffrey, G.M.; Cisar, L.A.; Morganti, A.; Orlando, N.; Gruia, G.; Miller, L.L. Irinotecan plus gemcitabine results in no survival advantage compared with gemcitabine monotherapy in patients with locally advanced or metastatic pancreatic cancer despite increased tumor response rate. J. Clin. Oncol. 2004, 22, 3776–3783. [Google Scholar] [CrossRef] [PubMed]
- Louvet, C.; Labianca, R.; Hammel, P.; Lledo, G.; De Braud, F.; Andre, T.; Cantore, M.; Ducreux, M.; Zaniboni, A.; De Gramont, A. GemOx (Gemcitabine + Oxaliplatin) versus Gem (Gemcitabine) in non resectable pancreatic adenocarcinoma: Final results of the GERCOR/GISCAD intergroup phase III. In Proceedings of the ASCO Annual Meeting, New Orleans, LA, USA, 5–8 June 2004; p. 4008.
- Oettle, H.; Richards, D.; Ramanathan, R.; van Laethem, J.; Peeters, M. A randomized phase III study comparing gemcitabine pemetrexed versus gemcitabine in patients with locally advanced and metastatic pancreas cancer. Ann. Oncol. 2005, 16, 1639–1645. [Google Scholar] [CrossRef] [PubMed]
- Abou-Alfa, G.K.; Letourneau, R.; Harker, G.; Modiano, M.; Hurwitz, H.; Tchekmedyian, N.S.; Feit, K.; Ackerman, J.; De Jager, R.L.; Eckhardt, S.G.; et al. Randomized phase III study of exatecan and gemcitabine compared with gemcitabine alone in untreated advanced pancreatic cancer. J. Clin. Oncol. 2006, 24, 4441–4447. [Google Scholar] [CrossRef] [PubMed]
- Poplin, E.; Levy, D.; Berlin, J.; Rothenberg, M.; O’Dwyer, P.; Cella, D. Phase III trial of gemcitabine (30-min infusion) versus gemcitabine (fixed-dose rate infusion) versus gemcitabine plus oxaliplatin (GEMOX) in patients with advanced pancreatic cancer. J. Clin. Oncol. 2006, 24, 933s. [Google Scholar]
- Van Cutsem, E.; van de Velde, H.; Karasek, P.; Oettle, H.; Vervenne, W.; Szawlowski, A.; Schoffski, P.; Post, S.; Verslype, C.; Neumann, H. Phase III trial of gemcitabine plus tipifarnib compared with gemcitabine plus placebo in advanced pancreatic cancer. J. Clin. Oncol. 2004, 22, 1430–1438. [Google Scholar] [CrossRef] [PubMed]
- Bramhall, S.; Schulz, J.; Nemunaitis, J.; Brown, P.; Baillet, M.; Buckels, J. A double-blind placebo-controlled, randomised study comparing gemcitabine and marimastat with gemcitabine and placebo as first line therapy in patients with advanced pancreatic cancer. Br. J. Cancer 2002, 87, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Watson, S.A.; Gilliam, A.D. G17DT—A new weapon in the therapeutic armoury for gastrointestinal malignancy. Expert Opin. Biol. Ther. 2001, 1, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.J.; Goldstein, D.; Hamm, J.; Figer, A.; Hecht, J.R.; Gallinger, S.; Au, H.J.; Murawa, P.; Walde, D.; Wolff, R.A. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: A phase III trial of the national cancer institute of Canada clinical trials group. J. Clin. Oncol. 2007, 25, 1960–1966. [Google Scholar] [CrossRef] [PubMed]
- Graham-Bonnalie, F.E. Gold for rheumatoid arthritis. Br. Med. J. 1971, 2, 277. [Google Scholar] [CrossRef] [PubMed]
- Myer, L.; Jones, D.; Tamarkin, L.; Paciotti, G. Nanomedicine-based enhancement of chemotherapy. Cancer Res. 2008, 68, 5718. [Google Scholar]
- Meng, H.; Mai, W.X.; Zhang, H.; Xue, M.; Xia, T.; Lin, S.; Wang, X.; Zhao, Y.; Ji, Z.; Zink, J.I.; et al. Codelivery of an optimal drug/sirna combination using mesoporous silica nanoparticles to overcome drug resistance in breast cancer in vitro and in vivo. ACS Nano 2013, 7, 994–1005. [Google Scholar] [CrossRef] [PubMed]
- Meng, H.; Wang, M.; Liu, H.; Liu, X.; Situ, A.; Wu, B.; Ji, Z.; Chang, C.H.; Nel, A.E. Use of a lipid-coated mesoporous silica nanoparticle platform for synergistic gemcitabine and paclitaxel delivery to human pancreatic cancer in mice. ACS Nano 2015, 9, 3540–3557. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, M. Cancer nanotechnology: Opportunities and challenges. Nat. Rev. Cancer 2005, 5, 161–171. [Google Scholar] [CrossRef] [PubMed]
- McCarroll, J.; Teo, J.; Boyer, C.; Goldstein, D.; Kavallaris, M.; Phillips, P.A. Potential applications of nanotechnology for the diagnosis and treatment of pancreatic cancer. Front. Physiol. 2014, 5. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Sharma, A.; Robertson, G.P. Realizing the clinical potential of cancer nanotechnology by minimizing toxicologic and targeted delivery concerns. Cancer Res. 2012, 72, 5663–5668. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, A.; Heller, D.A.; Winslow, M.M.; Dahlman, J.E.; Pratt, G.W.; Langer, R.; Jacks, T.; Anderson, D.G. Treating metastatic cancer with nanotechnology. Nat. Rev. Cancer 2012, 12, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Namiki, Y.; Fuchigami, T.; Tada, N.; Kawamura, R.; Matsunuma, S.; Kitamoto, Y.; Nakagawa, M. Nanomedicine for cancer: Lipid-based nanostructures for drug delivery and monitoring. Acc. Chem. Res. 2011, 44, 1080–1093. [Google Scholar] [CrossRef] [PubMed]
- Blanco, E.; Hsiao, A.; Mann, A.P.; Landry, M.G.; Meric-Bernstam, F.; Ferrari, M. Nanomedicine in cancer therapy: Innovative trends and prospects. Cancer Sci. 2011, 102, 1247–1252. [Google Scholar] [CrossRef] [PubMed]
- Robertson, C.A.; Evans, D.H.; Abrahamse, H. Photodynamic therapy (PDT): A short review on cellular mechanisms and cancer research applications for PDT. J. Photochem. Photobiol. B 2009, 96, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Piktel, E.; Niemirowicz, K.; Wątek, M.; Wollny, T.; Deptuła, P.; Bucki, R. Recent insights in nanotechnology-based drugs and formulations designed for effective anti-cancer therapy. J. Nanobiotechnol. 2016, 14, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Li, J.; Jia, W.; Yao, L.; Li, X.; Jiang, L.; Tian, Y. Photothermal therapy of cancer cells using novel hollow gold nanoflowers. Int. J. Nanomed. 2014, 9, 517–526. [Google Scholar]
- Fan, Z.; Dai, X.; Lu, Y.; Yu, E.; Brahmbatt, N.; Carter, N.; Tchouwou, C.; Singh, A.K.; Jones, Y.; Yu, H.; et al. Enhancing targeted tumor treatment by near IR light-activatable photodynamic–photothermal synergistic therapy. Mol. Pharm. 2014, 11, 1109–1116. [Google Scholar] [CrossRef] [PubMed]
- Hainfeld, J.F.; Dilmanian, F.A.; Slatkin, D.N.; Smilowitz, H.M. Radiotherapy enhancement with gold nanoparticles. J. Pharm. Pharmacol. 2008, 60, 977–985. [Google Scholar] [CrossRef] [PubMed]
- Townley, H.E.; Kim, J.; Dobson, P.J. In vivo demonstration of enhanced radiotherapy using rare earth doped titania nanoparticles. Nanoscale 2012, 4, 5043–5050. [Google Scholar] [CrossRef] [PubMed]
- Le Duc, G.; Miladi, I.; Alric, C.; Mowat, P.; Bräuer-Krisch, E.; Bouchet, A.; Khalil, E.; Billotey, C.; Janier, M.; Lux, F.; et al. Toward an image-guided microbeam radiation therapy using gadolinium-based nanoparticles. ACS Nano 2011, 5, 9566–9574. [Google Scholar] [CrossRef] [PubMed]
- Deer, E.L.; González-Hernández, J.; Coursen, J.D.; Shea, J.E.; Ngatia, J.; Scaife, C.L.; Firpo, M.A.; Mulvihill, S.J. Phenotype and genotype of pancreatic cancer cell lines. Pancreas 2010, 39, 425–435. [Google Scholar] [CrossRef] [PubMed]
- Eibl, G.; Bruemmer, D.; Okada, Y.; Duffy, J.P.; Law, R.E.; Reber, H.A.; Hines, O.J. PGE 2 is generated by specific COX-2 activity and increases VEGF production in COX-2-expressing human pancreatic cancer cells. Biochem. Biophys. Res. Commun. 2003, 306, 887–897. [Google Scholar] [CrossRef]
- Eibl, G.; Reber, H.A.; Wente, M.N.; Hines, O.J. The selective cyclooxygenase-2 inhibitor nimesulide induces apoptosis in pancreatic cancer cells independent of COX-2. Pancreas 2003, 26, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Molina, M.A.; Sitja-Arnau, M.; Lemoine, M.G.; Frazier, M.L.; Sinicrope, F.A. Increased cyclooxygenase-2 expression in human pancreatic carcinomas and cell lines growth inhibition by nonsteroidal anti-inflammatory drugs. Cancer Res. 1999, 59, 4356–4362. [Google Scholar] [PubMed]
- Yip-Schneider, M.T.; Sweeney, C.J.; Jung, S.-H.; Crowell, P.L.; Marshall, M.S. Cell cycle effects of nonsteroidal anti-inflammatory drugs and enhanced growth inhibition in combination with gemcitabine in pancreatic carcinoma cells. J. Pharmacol. Exp. Ther. 2001, 298, 976–985. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
| Country/Region | Sample Size | Age Range (Years) | % Males | Previous Treatment | Follow-Up (Months) | Mortality (%) | Assessment | Reference |
|---|---|---|---|---|---|---|---|---|
| North America, Eastern Europe, Australia, Western Europe | n = 861 | 27–88 | 58 | None | 24 | 692 total deaths (80) 333 in the treatment group (77) 359 in the gemcitabine group (83) | Nab-paclitaxel plus gemcitabine vs. gemcitabine monotherapy | Von Hoff et al. 2013 [41] |
| United States | n = 19 | 24–80 | 47.4 | Chemotherapy (gemcitabine containing regimen) * | 36 | 16 at 16 months (84) | Determine the effectiveness of nab-paclitaxel monotherapy as a second line agent | Hosein et al. 2013 [8] |
| United States | n = 67 | 30–72 | 48 | None | 18 | 32 at 12 months (48) | Identify the safety and maximum tolerated dose of nab-paclitaxel plus gemcitabine | Von Hoff et al. 2011 [42] |
| United States Philippines | Trial 1 n = 6 Trial 2 n = 3 Trial 3 n = 1 | Trial 1 45–64 Trial 2 53–68 Trial 3 Not stated | Not stated | Chemotherapy (gemcitabine containing regimen) | Trial 1: 13 Trial 2: 6 Trial 3: 6 | Trial 1: 6 (100) Trial 2: 1 (33) Trial 3: 1 (100) | Trial 1: Determine the safety of Rexin-G at varying doses Trial 2: Determine the safety of Rexin-G at varying doses Trial 3: Determine the effectiveness of a personal dosing regimen for Rexin-G | Gordon et al. 2006 [7] |
| Philippines | n = 3 | 47–56 | 33 | Surgical resection, chemotherapy (gemcitabine containing regimen) and external beam radiotherapy | 14 | 1 (33) | Evaluate the safety and efficacy of Rexin-G | Gordon et al. 2004 [43] |
| United States | n = 13 | 50–83 | 46 | Chemotherapy (gemcitabine containing regimen) | 12 | 13 (87) | Determine the effectiveness and most appropriate dose of Rexin-G | Chawla et al. 2010 [48] |
| Unites States | n = 12 | 42–71 | 75 | Chemotherapy (gemcitabine containing regimen) | 6 | 11 (92) | Determine the effectiveness and most appropriate dose of Rexin-G | Galanis et al. 2008 [47] |
| United States | n = 3 | Not stated | Not stated | Chemotherapy | Not analysed | Not analysed | Evaluate the efficacy and safety of CYT6091 | Libutti et al. 2010 [46] |
| Japan | n = 11 | 43–72 | Not stated | Chemotherapy | Not analysed | Not analysed | Determine the maximum tolerated dose, safety and efficacy of NK105 | Hamaguchi et al. 2007 [44] |
| Greece | n = 24 | 47–80 | 46 | Chemotherapy | 8 | 17 (71) | Evaluate the safety and efficacy of lipoplatin | Stathopolous et al. 2006 [45] |
| Authors | Study Design | Nanoparticle Formulation | Selection Criteria | Main Objective | Participants * | Overall Median Survival/Outcome | Adverse Reactions † | Conclusion |
|---|---|---|---|---|---|---|---|---|
| Von Hoff et al. [41] | Phase III Randomised control trial | Nanoparticle albumin bound paclitaxel (nab-paclitaxel) | Metastatic pancreatic cancer Karnofsky performance status score of 70+ | Evaluate the safety and efficacy of nab-paclitaxel plus gemcitabine vs. gemcitabine monotherapy in patients with metastatic pancreatic cancer | n = 861. Age 27–88 years. Metastatic pancreatic cancer | 8.5 months (95% CI, 7.89 to 9.53) | Major: neutropaenia Minor: fatigue, nausea, vomiting, anorexia and neuropathy | Increased overall survival. Adverse effects of peripheral neuropathy and myelosuppression increased |
| Hosein et al. [8] | Phase II clinical trial | Nanoparticle albumin bound paclitaxel (nab-paclitaxel) | Pre-treated advanced pancreatic cancer | Evaluate the safety and efficacy of nab-paclitaxel monotherapy in patients with advanced pancreatic cancer | n = 19. Age 22–80 years. Stage III and IV pancreatic cancer | 7.3 months (95% CI, 2.8–15.8) | Major: sepsis and neutropaenia Minor: fatigue and neuropathy | - |
| Von Hoff et al. [42] | Phase I/II clinical trial | Nanoparticle albumin bound paclitaxel (nab-paclitaxel) | Untreated advanced pancreatic cancer | Identify the safety and maximum tolerated dose of nab-paclitaxel plus gemcitabine in patients with untreated advanced pancreatic cancer | n = 67 Age 30–72 years | 12.2 months (95% CI, 9.8 to 17.9) | Major: sepsis and neutropaenia Minor: fatigue and neuropathy | Increased overall survival. Slightly higher occurrence of febrile neutropaenia (3% vs. 1%) |
| Gordon et al. [7] | (A) Phase I/II clinical trial | Rexin-G | Trial A: Locally advanced pancreatic cancer | Trial A: Determine the safety of Rexin-G at varying doses in patients with locally advanced pancreatic cancer | Trial A, n = 6 Age 45–64 years | Trial A: 24 months. (95% CI, 11.1 to 39.5) | Trial A: nil minor or major side effects | Trial A: Increased overall survival. Symptom relief |
| (B) Phase I/II clinical trial | Rexin-G | Trial B: Metastatic cancer | Trial B: Determine the safety of Rexin-G at varying doses in patients with various types of metastatic cancer | Trial B, n = 3 Age 53–68 years | Trial B: 9 months. (95% CI, 2.4 to 14.9) | Trial B: nil minor or major side effects | Trial B: Increased overall survival. Symptom relief | |
| (C) Expanded access clinical trial | Rexin-G | Trial C: Solid organ cancer | Trial C: Determine the effectiveness of a personal dosing regimen for Rexin-G in solid tumours. Nanoparticle: Rexin-G (non-replicating retroviral vector expressing a cytocidal gene) | Trial C, n = 1, Age (not stated) | Trial C: Unknown | Trial C: Major anaemia requiring red cell transfusions and sporadic thrombocytopaenia | Trial C: Reduction in size of metastatic lesions | |
| Gordon et al. [43] | Phase I/II clinical trial | Rexin-G | Stage 4 pancreatic cancer | Evaluate the safety and efficacy of Rexin-G in patients with stage 4 pancreatic cancer. Nanoparticle: Rexin-G | n = 3 Stage 4 pancreatic cancer | 14 months ** (95% CI, −5.8 to 31.8) | Major: nil Minor: nil | Increased overall survival. No adverse events |
| Chawla et al. [48] | Phase I/II clinical trial | Rexin-G | Gemcitabine resistant metastatic cancer | Determine the effectiveness and most appropriate dose of Rexin-G in patients with gemcitabine resistant metastatic cancer. Nanoparticle: Rexin G | n = 13 Age 50–83 years Gemcitabine refractory Metastatic disease | 2.6 months at dose 0–1, n = 6. 9.3 months at dose 2, n = 7 | Major: nil Minor: fatigue, chills and headache | Increased overall survival. Low severity of adverse events |
| Galanis et al. [47] | Phase I/II clinical trial | Rexin-G | Gemcitabine resistant metastatic disease | Determine the effectiveness and most appropriate dose of Rexin-G in patients with gemcitabine resistant metastatic cancer. Nanoparticle: Rexin G | n = 12 Age 42–71 years Gemcitabine refractory Metastatic disease | 3.5 months from treatment initiation | Major: nil Minor: nausea, fever, diarrhoea, hypermagnesaemia and raised liver enzymes (alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphate (ALP)) | Significant increase in tumour size. Low severity of adverse events |
| Libutti et al. [46] | Phase I clinical trial | Colloid gold nanoparticle PEGlycated with recombinant TNF | Solid organ cancer | Evaluate the efficacy and safety of CYT6091 in patients with advanced stage cancer | n = 3 with Pancreatic cancer | Not specified | Major: nil Minor: lymphopenia, hypoalbuminaemia, hypokalaemia, hypophosphataemia and deranged liver function tests (bilirubin and AST) | Nanoparticle CYT6091 preferentially targets tumour tissue |
| Hamaguchi et al. [44] | Phase I clinical trial | NK105 (micelle nanoparticle) | Refractory solid organ cancers | Determine the maximum tolerated dose, safety and efficacy of NK105 in 19 patients with refractory solid organ cancers | n = 11 Age 43–72 years (range for all participants) | Not specified. Antitumour response of 1 year for 1 patient, one had stable disease for 4 weeks | Major: neutropaenia Minor: fever. Nausea, fatigue, stomatitis, rash, alopecia (for all participants with a solid organ cancer) | Decrease in size of metastatic lesions. Low severity of adverse events |
| Stathopolous et al. [45] | Phase I/II clinical trial | Lipoplatin | Refractory pancreatic cancer | Evaluate the safety and efficacy of lipoplatin and gemcitabine in patients with refractory pancreatic cancer | n = 24 Age 47–80 years. Refractory pancreatic cancer | 4 months from beginning of treatment. (Range 2–8 months) | Major: no neurological/renal toxicity Minor: self- resolving abdominal pain. Myelotoxicity (grade 3) | Treatment resulted in symptom relief and a partial response/stable disease. Low severity of adverse events |
| Table 3a. Quality assessment of included randomised controlled trial using the JADAD score. | ||||||||||||
| Author and Year | Randomisation | Blinding | An Account of All Patients | Total Score | ||||||||
| Von Hoff et al. 2013 [41] | 2 | 0 | 1 | 3 | ||||||||
| Table 3b. Quality assessment of included studies using the Therapy CA Worksheet. | ||||||||||||
| Author and Year | Randomisation | Sufficient and Complete Follow-Up | Groups Analysed as per Randomisation | Blinding | Groups Treated Equally Apart from Intervention | Groups Have Similar Characteristics at the Start | Median Survival (Months) | 95% CI | ||||
| Hosein et al. 2013 [8] | N | Y | N/A | N | N/A | N/A | 7.3 | 2.8–15.8 | ||||
| Von Hoff et al. 2011 [42] | N | Y | N/A | N | N/A | N/A | 12.2 | 9.8–17.9 | ||||
| Gordon et al. 2006 [7] | Trial A: N Trial B: N Trial C: N | Trial A: Y Trial B:Y Trial C: N | Trial A: N/A Trial B: N/A Trial C: N/A | Trial A: N Trial B: N Trial C: N | Trial A: N/A Trial B: N/A Trial C: N/A | Trial A: N/A Trial B: N/A Trial C: N/A | Trial A: 25 Trial B: 9 Trial C: N/A | 12.36–38.30 * 3.58–13.76 * N/A | ||||
| Gordon et al. 2004 [43] | N | Y | N/A | N | N/A | N/A | 13 | −2.30–28.30 * | ||||
| Chawla et al. 2010 [48] | N | Y | N/A | N | N/A | N/A | Dose 0–1:4.3 Dose 2:9.2 | N/A † | ||||
| Galanis et al. 2008 [47] | N | Y | N/A | N | N/A | N/A | 3.5 | 2.66–4.34 * | ||||
| Libutti et al. 2010 [46] | N | N | N/A | N | N/A | N/A | N/A | N/A † | ||||
| Hamaguchi et al. 2007 [44] | N | N | N/A | N | N/A | N/A | N/A | N/A † | ||||
| Stathopolous et al. 2006 [45] | N | Y | N/A | N | N/A | N/A | 4 | 3.37–4.63 * | ||||
© 2016 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Au, M.; Emeto, T.I.; Power, J.; Vangaveti, V.N.; Lai, H.C. Emerging Therapeutic Potential of Nanoparticles in Pancreatic Cancer: A Systematic Review of Clinical Trials. Biomedicines 2016, 4, 20. https://doi.org/10.3390/biomedicines4030020
Au M, Emeto TI, Power J, Vangaveti VN, Lai HC. Emerging Therapeutic Potential of Nanoparticles in Pancreatic Cancer: A Systematic Review of Clinical Trials. Biomedicines. 2016; 4(3):20. https://doi.org/10.3390/biomedicines4030020
Chicago/Turabian StyleAu, Minnie, Theophilus I. Emeto, Jacinta Power, Venkat N. Vangaveti, and Hock C. Lai. 2016. "Emerging Therapeutic Potential of Nanoparticles in Pancreatic Cancer: A Systematic Review of Clinical Trials" Biomedicines 4, no. 3: 20. https://doi.org/10.3390/biomedicines4030020