
Seroprevalence of Dengue and Chikungunya Virus Infections in Children Living in Sub-Saharan Africa: Systematic Review and Meta-Analysis
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Search Strategy
2.4. Literature Selection and Data Extraction
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
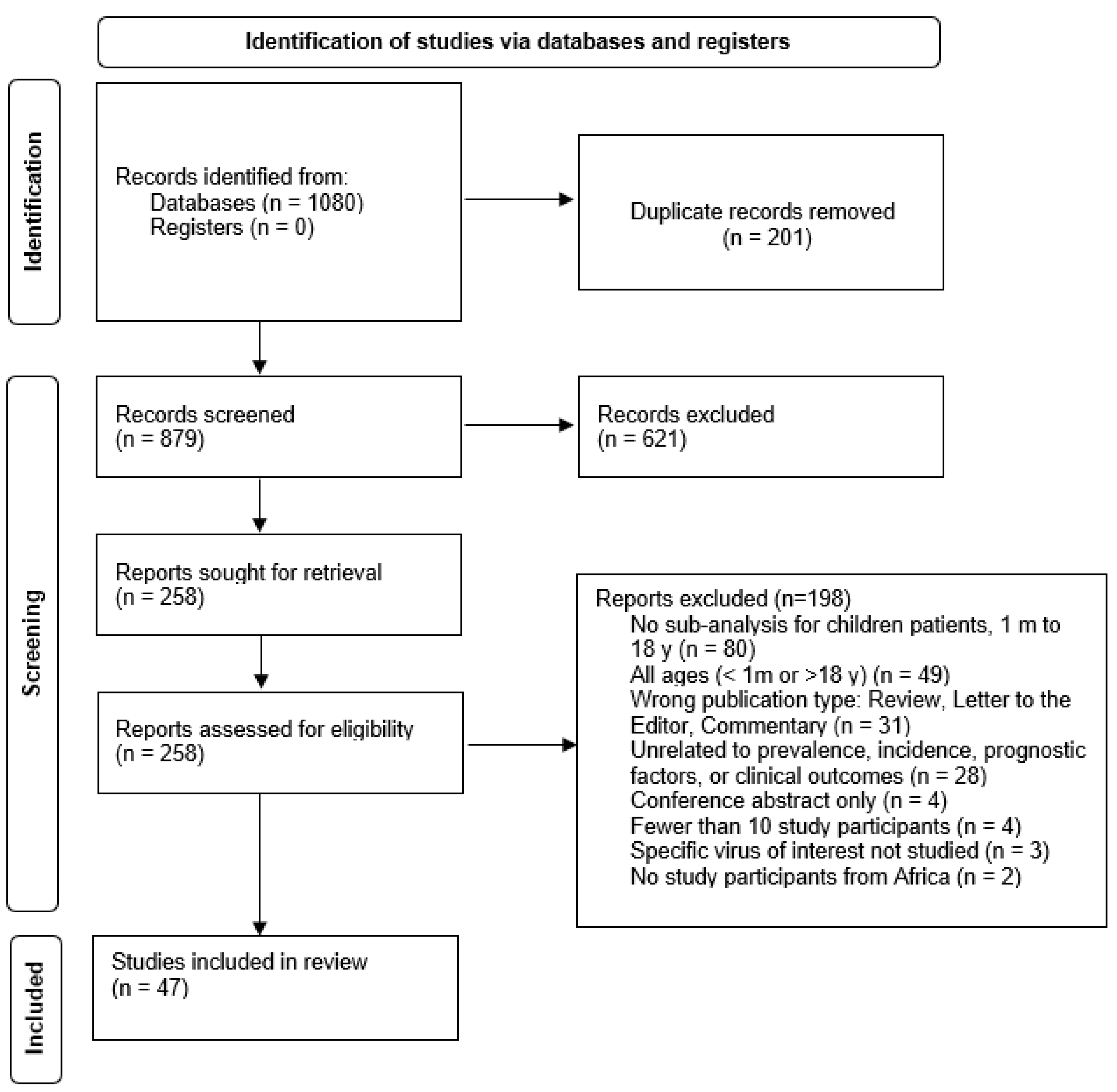
3.1. Study Selection and Characteristics
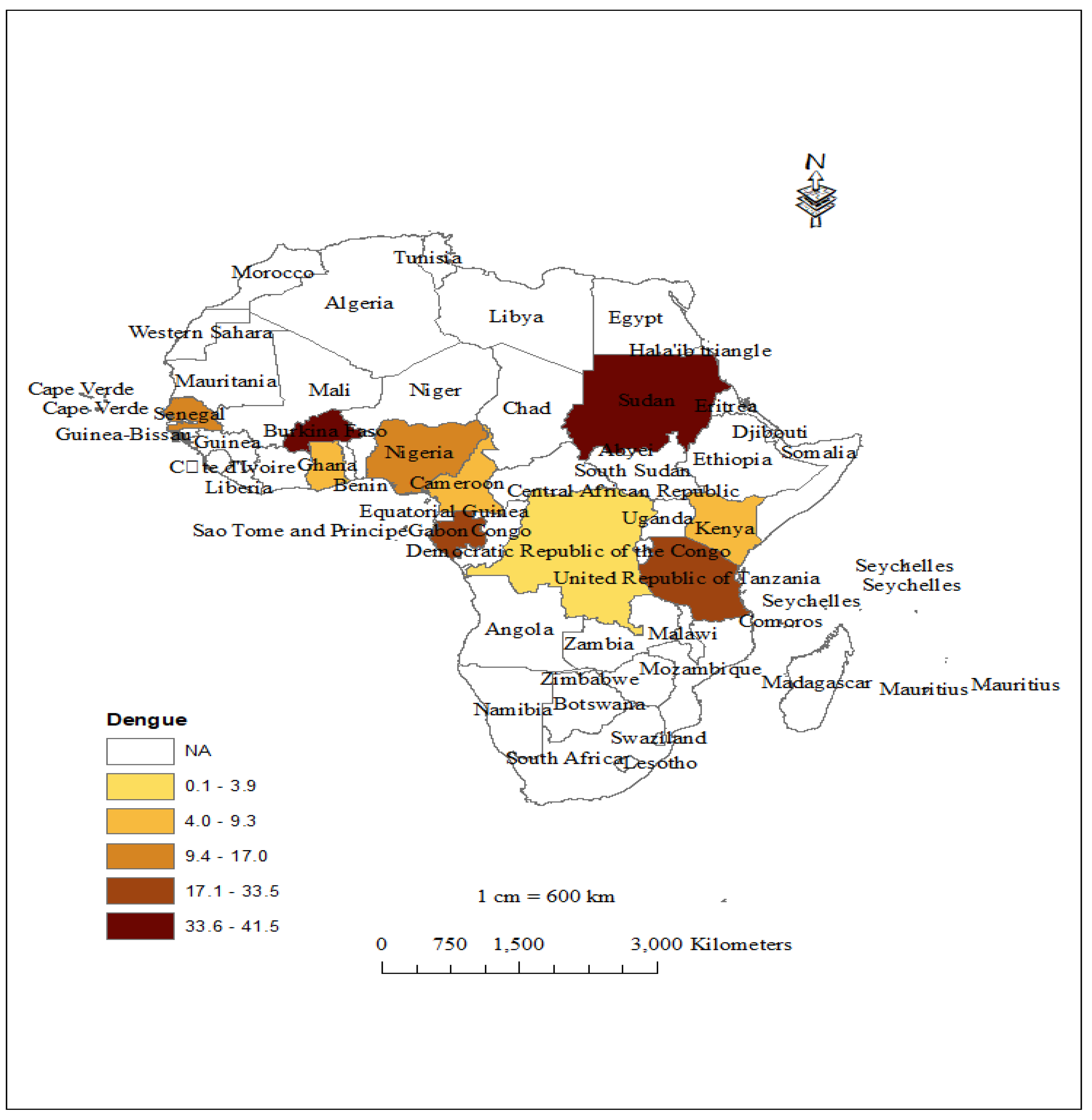
3.2. Prevalence of DENV and Geographic Coverage
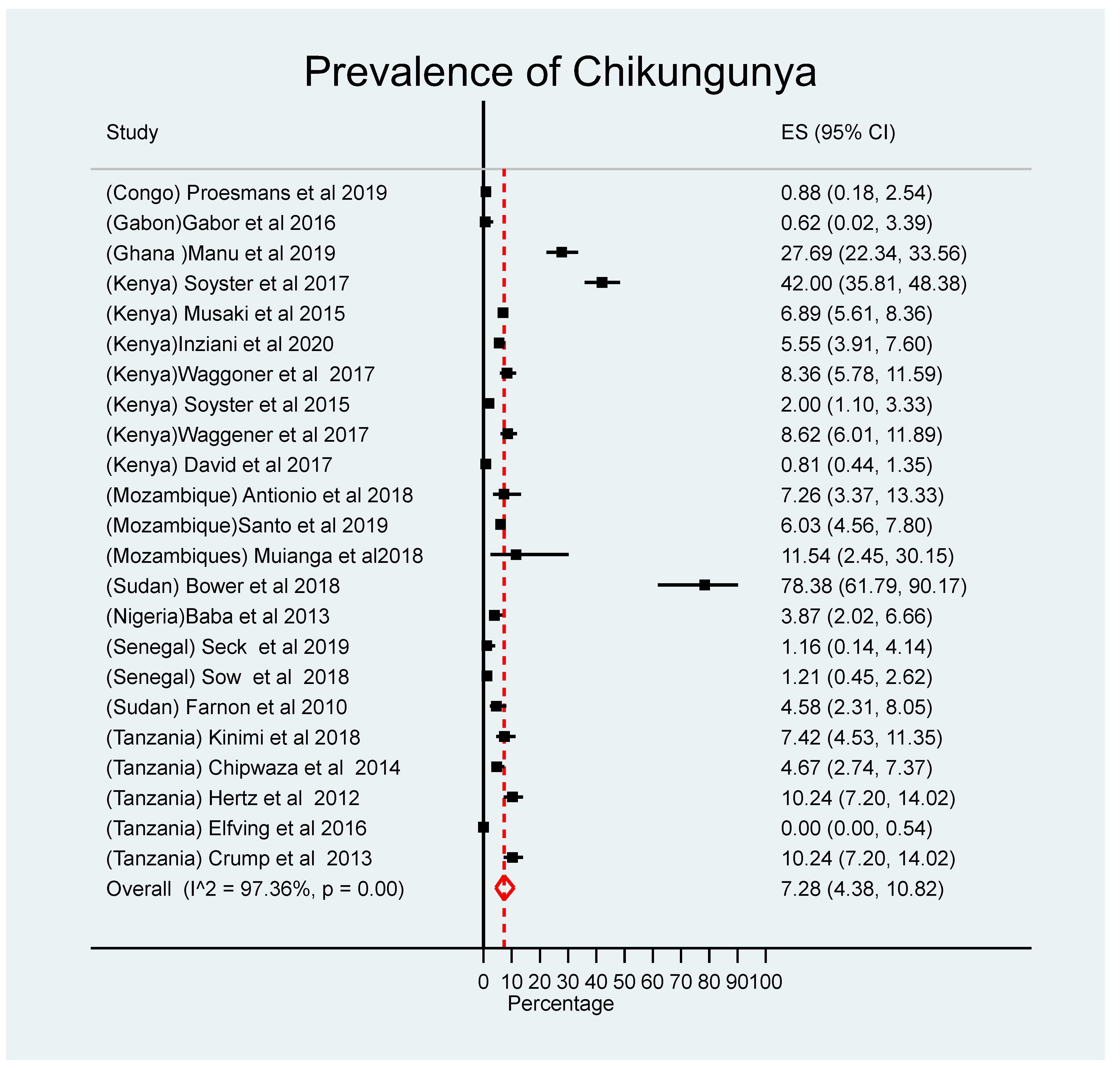
3.3. Prevalence of Chikungunya and Geographical Coverage
3.4. Pooled Prevalence of DENV and CHIKV by Region
3.5. Laboratory Method Used to Diagnose Arbovirus Infections
3.6. DENV and CHIKV Co-Infections
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Subhadra, S.; Sabat, J.; Dwibedi, B.; Panda, S.; Mandal, M.C.; Rath, S.; Ho, L.M.; Palo, S.K.; Pati, S.; Turuk, J. Prevalence and trend of emerging and re-emerging arboviral infections in the state of Odisha. Virus Dis. 2021, 32, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Gould, E.; Pettersson, J.; Higgs, S.; Charrel, R.; De Lamballerie, X. Emerging arboviruses: Why today? One Health 2017, 4, 1–13. [Google Scholar] [CrossRef]
- World Health Organization. Disease Outbreak News: Geographical expansion of cases of dengue and chikungunya beyond the historical areas of transmission in the Region of Americas. Available online: http://www.who.int/emergencies/disease-outbreak-news/item/2023-DON448 (accessed on 23 March 2023).
- Irekeola, A.A.; Syafirah, E.A.R.E.N.; Islam, A.; Shueb, R.H. Global prevalence of dengue and chikungunya coinfection: A systematic review and meta-analysis of 43,341 participants. Acta Trop. 2022, 231, 106408. [Google Scholar] [CrossRef]
- Martins, M.M.; Prata-Barbosa, A.; Cunha, A.J. Arboviral diseases in pediatrics. J. Pediatr. 2020, 96, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, A.; Murray, N.E.A.; Quam, M.B. Epidemiology of dengue: Past, present and future prospects. Clin. Epidemiol. 2013, 5, 299–309. [Google Scholar] [CrossRef]
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The global distribution and burden of dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Strategy for Dengue Prevention and Control 2012–2020. 2012. Available online: http://www.who.int/denguecontrol/9789241504034/en/ (accessed on 18 September 2018).
- Robinson, M.C. An epidemic of virus disease in Southern Province, Tanganyika territory, in 1952–1953. Trans. R. Soc. Trop. Med. Hyg. 1955, 49, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Zeller, H.; Van Bortel, W.; Sundre, B. Chikungunya. Its history in Africa and Asia and its spread to new regions in 2013–2014. J. Infect. Dis. 2016, 214 (Suppl. S5), S435–S440. [Google Scholar] [CrossRef] [PubMed]
- Wahid, B.; Ali, A.; Rafique, S.; Idrees, M. Global expansion of chikungunya virus: Mapping the 64-year history. Int. J. Infect. Dis. 2017, 58, 69–76. [Google Scholar] [CrossRef]
- Li, Z.; Wang, J.; Cheng, X.; Hu, H.; Guo, C.; Huang, J.; Chen, Z.; Lu, J. The worldwide seroprevalence of DENV, CHIKV and ZIKV infection: A systematic review and meta-analysis. PLoS Neglected Trop. Dis. 2021, 15, e0009337. [Google Scholar] [CrossRef]
- Rolph, M.S.; Foo, S.S.; Mahalingam, S. Emergent chikungunya virus and arthritis in the Americas. Lancet Infect. Dis. 2015, 15, 1007–1008. [Google Scholar] [CrossRef] [PubMed]
- Staples, J.E.; Breiman, R.F.; Powers, A.M. Chikungunya Fever: An Epidemiological Review of a Re-Emerging Infectious Disease. Clin. Infect. Dis. 2009, 49, 942–948. [Google Scholar] [CrossRef]
- Biswal, S.; Reynales, H.; Saez-Llorens, X.; Lopez, P.; Borja-Tabora, C.; Kosalaraksa, P.; Sirivichayakul, C.; Watanaveeradej, V.; Rivera, L.; Espinoza, F.; et al. Efficacy of a tetravalent dengue vaccine in healthy children and adolescents. N. Engl. J. Med. 2019, 381, 2009–2019. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Dengue vaccine: WHO positio paper, July 2016-recommendations. Vaccine 2017, 35, 1200–1201. [Google Scholar] [CrossRef] [PubMed]
- Boillat-Blanco, N.; Klaassen, B.; Mbarack, Z.; Samaka, J.; Mlaganile, T.; Masimba, J.; Franco Narvaez, L.; Mamin, A.; Genton, B.; Kaiser, L.; et al. Dengue fver in Dar s Salaam, Tanzania:clinical features and outcome in populations of black and non-black racial category. BMC Infect. Dis. 2018, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for sytematic reviews and meta-analyses: The PRISMA Statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observational epidemi-ological studies reporting prevalence and cumulative incidence data. JBI Evid. Implement. 2015, 13, 147–153. [Google Scholar]
- Elfving, K.; Shakely, D.; Andersson, M.; Baltzell, K.; Ali, A.S.; Bachelard, M.; Falk, K.I.; Ljung, A.; Msellem, M.I.; Omar, R.S.; et al. Acute uncomplicated febrile illness in children aged 2-59 months in Zanzibar–aetiologies, antibiotic treatment and outcome. PLoS ONE 2016, 11, e0146054. [Google Scholar] [CrossRef]
- Muianga, A.; Pinto, G.; Massangaie, M.; Ali, S.; Oludele, J.; Tivane, A.; Falk, K.I.; Lagerqvist, N.; Gudo, E.S. Antibodies Against Chikungunya in Northern Mozambique During Dengue Outbreak, 2014. Vector-Borne Zoonotic Dis. 2018, 18, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Chipwaza, B.; Mugasa, J.P.; Selemani, M.; Amuri, M.; Mosha, F.; Ngatunga, S.D.; Gwakisa, P.S. Dengue and Chikungunya Fever among Viral Diseases in Outpatient Febrile Children in Kilosa District Hospital, Tanzania. PLoS Neglected Trop. Dis. 2014, 8, e3335. [Google Scholar] [CrossRef]
- Ndenga, B.A.; Mutai, N.; Heath, C.; Vu, D.; Mutuku, F.; Mukoko, D.; Vulule, J.; King, C.; LaBeaud, A.D. acute febrile illness due to dengue infections, among children Kenya. Am. J. Trop. Med. Hyg. 2015, 93, 46. [Google Scholar]
- Camara, N.; Ngasala, B.; Leyna, G.; Abade, A.; Rumisha, S.F.; Oriyo, N.M.; Mboera, L.E. Socio-demographic determinants of dengue infection during an outbreak in Dar es Salaam City, Tanzania. Tanzan. J. Health Res. 2018, 20. [Google Scholar] [CrossRef]
- Vu, D.M.; Banda, T.; Teng, C.Y.; Heimbaugh, C.; Muchiri, E.M.; Mungai, P.L.; Mutuku, F.M.; Brichard, J.; Gildengorin, G.; Borland, E.M.; et al. Dengue and West Nile Virus Transmission in Children and Adults in Coastal Kenya. Am. J. Trop. Med. Hyg. 2016, 96, 141–143. [Google Scholar] [CrossRef]
- Kinimi, E.; Shayo, M.J.; Patrick, B.N.; Angwenyi, S.O.; Kasanga, C.J.; Weyer, J.; van Vuren, P.J.; Paweska, J.T.; Mboera, L.E.; Misinzo, G. Evidence of chikungunya virus infection among febrile patients seeking healthcare in selected districts of Tanzania. Infect. Ecol. Epidemiol. 2018, 8, 1553460. [Google Scholar] [CrossRef] [PubMed]
- Grossi-Soyster, E.N.; Mutuku, F.; Lipi, S.; Ng’ang’a, C.; LaBeaud, A.D. Seroprevalence of Flaviviruses and and Alphaviruses in children in coaster Kenya: A snapshot. Am. J. Trop. Med. Hyg. 2015, 95, 223. [Google Scholar]
- Grossi-Soyster, E.N.; Cook, E.A.; de Glanville, W.A.; Thomas, L.F.; Krystosik, A.R.; Lee, J.; Wamae, C.N.; Kariuki, S.; Fèvre, E.M.; LaBeaud, A.D. Serological and spatial analysis of alphavirus and flavivirus prevalence and risk factors in a rural community in western Kenya. PLoS Negl. Trop Dis. 2017, 11, e0005998. [Google Scholar] [CrossRef] [PubMed]
- Vairo, F.; Mboera, L.E.; De Nardo, P.; Oriyo, N.M.; Meschi, S.; Rumisha, S.F.; Colavita, F.; Mhina, A.; Carletti, F.; Mwakapeje, E.; et al. Clinical, Virologic, and Epidemiologic Characteristics of Dengue Outbreak, Dar es Salaam, Tanzania, 2014. Emerg. Infect. Dis. 2016, 22, 895–899. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.K.; Matendechero, S.H.; Alexander, N.; Lee, J.-S.; Lee, K.S.; Namkung, S.; Andia, E.; Oyembo, N.; Lim, S.-K.; Kanyi, H.; et al. Clinical and epidemiologic characteristics associated with dengue fever in Mombasa, Kenya. Int. J. Infect. Dis. 2020, 100, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Blaylock, J.M.; Maranich, A.; Bauer, K.; Nyakoe, N.; Waitumbi, J.; Martinez, L.J.; Lynch, J. The seroprevalence and seroincidence of dengue virus infection in western Kenya. Travel Med. Infect. Dis. 2011, 9, 246–248. [Google Scholar] [CrossRef] [PubMed]
- Waggoner, J.; Brichard, J.; Mutuku, F.; Ndenga, B.; Heath, C.J.; Mohamed-Hadley, A.; Sahoo, M.K.; Vulule, J.; Lefterova, M.; Banaei, N.; et al. Malaria and Chikungunya Detected Using Molecular Diagnostics Among Febrile Kenyan Children. Open Forum Infect. Dis. 2017, 4, ofx110. [Google Scholar] [CrossRef] [PubMed]
- Crump, J.A.; Morrissey, A.B.; Nicholson, W.L.; Massung, R.F.; Stoddard, R.A.; Galloway, R.L.; Ooi, E.E.; Maro, V.P.; Saganda, W.; Kinabo, G.D.; et al. Etiology of Severe Non-malaria Febrile Illness in Northern Tanzania: A Prospective Cohort Study. PLoS Neglected Trop. Dis. 2013, 7, e2324. [Google Scholar] [CrossRef]
- Hertz, J.T.; Saganda, W.; Munishi, O.M.; Crump, J.A.; Howe, S.; Kinabo, G.D.; Ooi, E.E.; Gubler, D.J.; Chow, A.; Lim, W.Y.; et al. Chikungunya and Dengue Fever among Hospitalized Febrile Patients in Northern Tanzania. Am. J. Trop. Med. Hyg. 2012, 86, 171–177. [Google Scholar] [CrossRef]
- Inziani, M.; Adungo, F.; Awando, J.; Kihoro, R.; Inoue, S.; Morita, K.; Obimbo, E.; Onyango, F.; Mwau, M. Seroprevalence of yellow fever, dengue, West Nile and chikungunya viruses in children in Teso South Sub-County, Western Kenya. Int. J. Infect. Dis. 2020, 91, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Musaki, S.; Grossi-Soyster, E.; Ndenga, B.; Mutuku, F.; LaBeaud, D. Prevalence of chikungunya and dengue virus exposure among children in Western Kenya. Am. J. Trop. Med. Hyg. 2018, 99, 282. [Google Scholar]
- António, V.S.; Muianga, A.F.; Wieseler, J.; Pereira, S.A.; Monteiro, V.O.; Mula, F.; Chelene, I.; Chongo, I.S.; Oludele, J.O.; Kümmerer, B.M.; et al. Seroepidemiology of Chikungunya Virus Among Febrile Patients in Eight Health Facilities in Central and Northern Mozambique, 2015–2016. Vector-Borne Zoonotic Dis. 2018, 18, 311–316. [Google Scholar] [CrossRef]
- Antonio, V.S.; Amade, N.A.; Muianga, A.F.; Ali, S.; Monteiro, V.; Mula, F.; Chelene, I.; Oludele, J.; Chongo, I.; José, A.; et al. Retrospective investigation of antibodies against chikungunya virus (CHIKV) in serum from febrile patients in Mozambique, 2009–2015: Implications for its prevention and control. PLoS ONE 2019, 14, e0213941. [Google Scholar] [CrossRef] [PubMed]
- Vu, D.M.; Mutai, N.; Heath, C.J.; Vulule, J.M.; Mutuku, F.M.; Ndenga, B.A.; LaBeaud, A.D. Unrecognized Dengue Virus Infections in Children, Western Kenya, 2014–2015. Emerg. Infect. Dis. 2017, 23, 1915–1917. [Google Scholar] [CrossRef] [PubMed]
- Vu, D.; Mutai, N.; Heath, C.; Ndenga, B.; Labeaud, A.D. Dengue Viremia in Kenyan children with Acute Febrile Illness. In Open Forum Infectious Diseases; Oxford University Press: Oxford, UK, 2016; Volume 3. [Google Scholar] [CrossRef]
- Vu, D.M.; Grossi-Soyster, E.N.; Krystosik, A.R.; Kiptoo, C.; King, C.H.; Vulule, J.; Mukoko, D.; Ndenga, B.A.; Mutuku, F.M.; LaBeaud, A.D. Differences in symptomatology of childhood dengue, chikungunya and malaria infections in Kenya. Am. J. Trop. Med. Hyg. 2017, 97, 552. [Google Scholar]
- Willcox, A.C.; Mumba, D.; Jadi, R.; de Silva, A.M.; Collins, M.H.; Meshnick, S.R.; Tshefu, A.; Parr, J.B.; Keeler, C.; Kashamuka, M. Seroepidemiology of Dengue, Zika, and Yellow Fever Viruses among Children in the Democratic Republic of the Congo. Am. J. Trop. Med. Hyg. 2018, 99, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Tchetgna, H.S.; Yousseu, F.S.; Kamgang, B.; Tedjou, A.; McCall, P.J.; Wondji, C.S. Concurrent circulation of dengue serotype 1, 2 and 3 among acute febrile patients in Cameroon. PLoS Neglected Trop. Dis. 2021, 15, e0009860. [Google Scholar] [CrossRef]
- Lim, J.K.; Fernandes, J.F.; Yoon, I.-K.; Lee, J.-S.; Mba, R.O.; Lee, K.S.; Namkung, S.; Yang, J.S.; Bae, S.H.; Lim, S.-K.; et al. Epidemiology of dengue fever in Gabon: Results from a health facility-based fever surveillance in Lambaréné and its surroundings. PLoS Neglected Trop. Dis. 2021, 15, e0008861. [Google Scholar] [CrossRef]
- Gabor, J.J.; Schwarz, N.G.; Esen, M.; Kremsner, P.G.; Grobusch, M.P. Dengue and chikungunya seroprevalence in Gabonese infants prior to major outbreaks in 2007 and 2010: A sero-epidemiological study. Travel Med. Infect. Dis. 2016, 14, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Demanou, M.; Pouillot, R.; Grandadam, M.; Boisier, P.; Kamgang, B.; Hervé, J.P.; Rogier, C.; Rousset, D.; Paupy, C. Evidence of Dengue Virus Transmission and Factors Associated with the Presence of Anti-Dengue Virus Antibodies in Humans in Three Major Towns in Cameroon. PLoS Neglected Trop. Dis. 2014, 8, e2950. [Google Scholar] [CrossRef] [PubMed]
- Tchuandom, S.B.; Tchouangueu, T.F.; Antonio-Nkondjio, C.; Lissom, A.; Djang, J.O.N.; Atabonkeng, E.P.; Kechia, A.; Nchinda, G.; Kuiate, J.-R. Seroprevalence of dengue virus among children presenting with febrile illness in some public health facilities in Cameroon. Pan Afr. Med. J. 2018, 31, 177. [Google Scholar] [CrossRef] [PubMed]
- Tchuandom, S.B.; Tchadji, J.C.; Tchouangueu, T.F.; Biloa, M.Z.; Atabonkeng, E.P.; Fumba, M.I.M.; Massom, E.S.; Nchinda, G.; Kuiate, J.-R. A cross-sectional study of acute dengue infection in paediatric clinics in Cameroon. BMC Public Health 2019, 19, 1–7. [Google Scholar] [CrossRef]
- Proesmans, S.; Katshongo, F.; Milambu, J.; Fungula, B.; Mavoko, H.M.; Ahuka-Mundeke, S.; da Luz, R.I.; Van Esbroeck, M.; Ariën, K.K.; Cnops, L.; et al. Dengue and chikungunya among outpatients with acute undifferentiated fever in Kinshasa, Democratic Republic of Congo: A cross-sectional study. PLoS Neglected Trop. Dis. 2019, 13, e0007047. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.; Earhart, K.; Mohareb, E.; Saad, M.; Saeed, M.; Ageep, A.; Soliman, A. Dengue hemorrhagic fever outbreak in children in Port Sudan. J. Infect. Public Heal. 2011, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Adam, A.; Schüttoff, T.; Reiche, S.; Jassoy, C. High seroprevalence of dengue virus indicates that dengue virus infections are frequent in central and eastern Sudan. Trop. Med. Int. Health 2018, 23, 960–967. [Google Scholar] [CrossRef] [PubMed]
- Farnon, E.C.; Laven, J.J.; Hayes, E.B.; Griffith, K.S.; Godsey, M.S.; Panella, A.J.; El Kholy, A.; Osman, M.S.; Perea, W.; Kosoy, O.; et al. Household-Based Sero-Epidemiologic Survey after a Yellow Fever Epidemic, Sudan, 2005. Am. J. Trop. Med. Hyg. 2010, 82, 1146–1152. [Google Scholar] [CrossRef]
- Bower, H.; El Karsany, M.; Adam, A.A.; Idriss, M.I.; Alzain, M.A.; Alfakiyousif, M.E.; Mohamed, R.; Mahmoud, I.; Albadri, O.; Mahmoud, S.A.; et al. “Kankasha” in Kassala: A prospective observational cohort study of the clinical characteristics, epidemiology, genetic origin, and chronic impact of the 2018 epidemic of Chikungunya virus infection in Kassala, Sudan. PLoS Negl. Trop Dis. 2021, 15, e0009387. [Google Scholar] [CrossRef] [PubMed]
- Adedayo, F.; Nioma, I.; Olanrewaju, M.B.; Adeyinka, A.; Ebele, A. Serological evidence of recent dengue virus infection among febrile children in a semi arid zone. Am. J. Infect. Dis. 2013, 9, 7–10. [Google Scholar] [CrossRef]
- Onoja, A.B.; Adeniji, J.A.; Olaleye, O.D. High rate of unrecognized dengue virus infection in parts of the rainforest region of Ni-geria. Acta Trop. 2016, 160, 39–43. [Google Scholar] [CrossRef]
- Sow, A.; Faye, O.; Diallo, M.; Diallo, D.; Chen, R.; Faye, O.; Diagne, C.T.; Guerbois, M.; Weidmann, M.; Ndiaye, Y.; et al. Chikungunya outbreak in Kedougou, southeastern Senegal in 2009–2010. Open Forum Infect. Dis. 2018, 5, ofx259. [Google Scholar] [CrossRef]
- Adesina, O.A.; Adeniji, J.A. Incidence of dengue virus infections in febrile episodes in Ile-Ife, Nigeria. Afr. J. Infect. Dis. 2015, 10, 21. [Google Scholar] [CrossRef]
- Boris, H.G.; Idrissa, D.; Louise, S.M.; Cheikh, T.; Aliou, B.M.; Fatoumata, D.S.; Rebecca, G.; Raymond, B.; Diamilatou, T.; Vincent, R.; et al. Identification of Pathogens Potentially Associated with Non-Malarial Fever in Children: A Pilot Study in Peri-Urban Dakar, Senegal. Am. J. Trop. Med. Hyg. 2021, 104, 1335–1341. [Google Scholar] [CrossRef] [PubMed]
- Dieng, I.; Diarra, M.; Diagne, M.M.; Faye, M.; Ndione, M.H.D.; Ba, Y.; Diop, M.; Ndiaye, E.H.; Zanotto, P.M.d.A.; Diop, B.; et al. Field Deployment of a Mobile Biosafety Laboratory Reveals the Co-Circulation of Dengue Viruses Serotype 1 and Serotype 2 in Louga City, Senegal, 2017. J. Trop. Med. 2021, 2021, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.K.; Seydou, Y.; Carabali, M.; Barro, A.; Dahourou, D.L.; Lee, K.S.; Nikiema, T.; Namkung, S.; Lee, J.-S.; Shin, M.Y.; et al. Clinical and epidemiologic characteristics associated with dengue during and outside the 2016 outbreak identified in health facility-based surveillance in Ouagadougou, Burkina Faso. PLoS Neglected Trop. Dis. 2019, 13, e0007882. [Google Scholar] [CrossRef]
- Lim, J.K.; Carabali, M.; Edwards, T.; Barro, A.; Lee, J.-S.; Dahourou, D.; Lee, K.S.; Nikiema, T.; Shin, M.Y.; Bonnet, E.; et al. Estimating the Force of Infection for Dengue Virus Using Repeated Serosurveys, Ouagadougou, Burkina Faso. Emerg. Infect. Dis. 2021, 27, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Seck, M.C.; Badiane, A.S.; Thwing, J.; Moss, D.; Fall, F.B.; Gomis, J.F.; Deme, A.B.; Diongue, K.; Sy, M.; Mbaye, A.; et al. Serological Data Shows Low Levels of Chikungunya Exposure in Senegalese Nomadic Pastoralists. Pathogens 2019, 8, 113. [Google Scholar] [CrossRef]
- Baba, M.; Logue, C.H.; Oderinde, B.; Abdulmaleek, H.; Williams, J.; Lewis, J.; Laws, T.R.; Hewson, R.; Marcello, A.; Agaro, P.D. Evidence of arbovirus co-infection in suspected febrile malaria and typhoid patients in Nigeria. J. Infect. Dev. Ctries. 2013, 7, 51–59. [Google Scholar] [CrossRef]
- Nassar, S.; Olayiwola, J.; Bakarey, A.; Enyhowero, S. Investigations of dengue virus and Plasmodium falciparum among febrile patients receiving care at a tertiary health facility in Osogbo, south-west Nigeria. Niger. J. Parasitol. 2019, 40, 18. [Google Scholar] [CrossRef]
- Kolawole, O.M.; Seriki, A.A.; Irekeola, A.A.; Bello, K.E.; Adeyemi, O.O. Dengue virus and malaria concurrent infection among febrile subjects within Ilorin metropolis, Nigeria. J. Med. Virol. 2017, 89, 1347–1353. [Google Scholar] [CrossRef] [PubMed]
- Manu, S.K.; Bonney, J.H.K.; Pratt, D.; Abdulai, F.N.; Agbosu, E.E.; Frimpong, P.O.; Adiku, T.K. Arbovirus circulation among febrile patients at the greater Accra Regional Hospital, Ghana. BMC Res. Notes 2019, 12, 332. [Google Scholar] [CrossRef] [PubMed]
- Eltom, K.; Enan, K.; El Hussein, A.R.; Elkhidir, I.M. Dengue virus infection in sub-Saharan Africa between 2010 and 2020: A sys-tematic review and meta-analysis. Front Cell Infect Microbiol. 2021, 11, 678945. [Google Scholar] [CrossRef] [PubMed]
- Simo, F.B.N.; Bigna, J.J.; Kenmoe, S.; Ndangang, M.S.; Temfack, E.; Moundipa, P.F.; Demanou, M. Dengue virus infection in people residing in Africa: A systematic review and meta-analysis of prevalence studies. Sci. Rep. 2019, 9, 13626. [Google Scholar] [CrossRef]
- Humphrey, J.M.; Cleton, N.B.; Reusken, C.B.E.M.; Glesby, M.J.; Koopmans, M.P.G.; Abu-Raddad, L.J. Dengue in the Middle East and North Africa: A Systematic Review. PLoS Neglected Trop. Dis. 2016, 10, e0005194. [Google Scholar] [CrossRef] [PubMed]
- Adam, A.; Jassoy, C. Epidemiology and Laboratory Diagnostics of Dengue, Yellow Fever, Zika, and Chikungunya Virus Infections in Africa. J. Pathog. 2021, 10, 1324. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.-Y.; Tsai, W.-Y.; Lin, S.-R.; Kao, C.-L.; Hu, H.-P.; King, C.-C.; Wu, H.-C.; Chang, G.-J.; Wang, W.-K. Antibodies to Envelope Glycoprotein of Dengue Virus during the Natural Course of Infection Are Predominantly Cross-Reactive and Recognize Epitopes Containing Highly Conserved Residues at the Fusion Loop of Domain II. J. Virol. 2008, 82, 6631–6643. [Google Scholar] [CrossRef]
- Mansfield, K.L.; Horton, D.L.; Johnson, N.; Li, L.; Barrett, A.D.T.; Smith, D.J.; Galbraith, S.E.; Solomon, T.; Fooks, A.R. Flavivirus-induced antibody cross-reactivity. J. Gen. Virol. 2011, 92, 2821–2829. [Google Scholar] [CrossRef]
- Fritzell, C.; Rousset, D.; Adde, A.; Kazanji, M.; Van Kerkhove, M.D.; Flamand, C. Current challenges and implications for dengue, chikungunya and Zika seroprevalence studies worldwide: A scoping review. PLoS Neglected Trop. Dis. 2018, 12, e0006533. [Google Scholar] [CrossRef]
- Petti, C.A.; Polage, C.R.; Quinn, T.C.; Ronald, A.R.; Sande, M.A. Laboratory Medicine in Africa: A Barrier to Effective Health Care. Clin. Infect. Dis. 2006, 42, 377–382. [Google Scholar] [CrossRef]
- Ward, T.; Samuel, M.; Maoz, D.; Runge-Ranzinger, S.; Boyce, R.; Toledo, J.; Velayudhan, R.; Horstick, O. Dengue data and sur-veillance in Tanzania: A systematic literature review. Trop Med. Int. Health 2017, 22, 960–970. [Google Scholar] [CrossRef] [PubMed]
- Katzelnick, L.C.; Coloma, J.; Harris, E. Dengue: Knowledge gaps, unmet needs, and research priorities. Lancet Infect Dis. 2017, 17, e88–e100. [Google Scholar] [CrossRef] [PubMed]
- D’Acremont, V.; Kilowoko, M.; Kyungu, E.; Philipina, S.; Sangu, W.; Kahama-Maro, J.; Lengeler, C.; Cherpillod, P.; Kaiser, L.; Genton, B. Beyond Malaria—Causes of Fever in Outpatient Tanzanian Children. N. Engl. J. Med. 2014, 370, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Kajeguka, D.C.; Kaaya, R.D.; Mwakalinga, S.; Ndossi, R.; Ndaro, A.; Chilongola, J.O.; Mosha, F.W.; Schiøler, K.L.; Kavishe, R.A.; Alifrangis, M. Prevalence of dengue and chikungunya virus infections in north-eastern Tanzania: A cross sectional study among participants presenting with malaria-like symptoms. BMC Infect. Dis. 2016, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.M.; Ndenga, B.A.; Mutuku, F.M.; Vu, D.M.; Grossi-Soyster, E.N.; Okuta, V.; Ronga, C.O.; Chebii, P.K.; Maina, P.; Jembe, Z.; et al. High Dengue Burden and Circulation of 4 Virus Serotypes among Children with Undifferentiated Fever, Kenya, 2014–2017. Emerg. Infect. Dis. 2020, 26, 2638–2650. [Google Scholar] [CrossRef] [PubMed]
- D’Acremont, V.; Lengeler, C.; Genton, B. Reduction in the proportion of fevers associated with Plasmodium falciparum parasitaemia in Africa: A systematic review. Malar. J. 2010, 9, 240. [Google Scholar] [CrossRef] [PubMed]
- Mwanyika, G.O.; Mboera, L.E.G.; Rugarabamu, S.; Ngingo, B.; Sindato, C.; Lutwama, J.J.; Paweska, J.T.; Misinzo, G. Dengue Virus Infection and Associated Risk Factors in Africa: A Systematic Review and Meta-Analysis. Viruses 2021, 13, 536. [Google Scholar] [CrossRef] [PubMed]
- Salam, N.; Mustafa, S.; Hafiz, A.; Chaudhary, A.A.; Deeba, F.; Parveen, S. Global prevalence and distribution of coinfection of malaria, dengue and chikungunya: A systematic review. BMC Public Health 2018, 18, 1–20. [Google Scholar] [CrossRef]
- Gandhi, B.S.; Kulkarni, K.; Godbole, M.; Dole, S.S.; Kapur, S.; Satpathy, P.; Khatri, A.M.; Deshpande, P.S.; Azad, F.; Gupte, N.; et al. Dengue and chikungunya co-infection associated with more severe clinical disease than mono-infection. Int. J. Health Biomed. Res. 2015, 3, 117–123. [Google Scholar]
- Castellanos, J.E.; Jaimes, N.; Coronel-Ruiza, C.; Rojas, J.P.; Mejía, L.F.; Villarreal, V.H.; Maya, L.E.; Claros, L.M.; Orjuela, C.; Calvo, E.; et al. Dengue-chikungunya coinfection outbreak in children from Cali, Colombia in 2018–2019. Int. J. Infect. Dis. 2020, 102, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Hooft, A.M.; Ripp, K.; Ndenga, B.; Mutuku, F.; Vu, D.; Baltzell, K.; Masese, L.N.; Vulule, J.; Mukoko, D.; LaBeaud, A.D. Principles, practices and knowledge of clinicians when assessing febrile children: A qualitative study in Kenya. Malar. J. 2017, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Mordecai, E.A.; Ryan, S.J.; Caldwell, J.M.; Shah, M.M.; LaBeaud, A.D. Climate change could shift disease burden from malaria to arboviruses in Africa. Lancet Planet. Health 2020, 4, e416–e423. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Region | Country | Sample Size (Children) | Sample Size (Adults + Children) | Female n (%) | Range Age <1–19 Years. | Epidemio-Logic Context | DQA Status | DENV | CHIKV | Ref |
|---|---|---|---|---|---|---|---|---|---|---|---|
| K. Elfving | Eastern | Tanzania | 83 | 677 | NA | 0–5 | Non-outbreak | H | 0(0.0) | 0 | [20] |
| A. Muianga | Eastern | Mozambique | 26 | 146 | NA | 0–19 | Outbreak | H | 15 (57.7) | 5 (19.2) | [21] |
| A. Chipwaza | Eastern | Tanzania | 364 | 364 | 178 (48.9) | 5–19 | Non-outbreak | H | 76 (20.9) | 17 (4.7) | [22] |
| B.A. Ndenga | Eastern | Kenya | 113 | 113 | NA | 2–17 | Non-outbreak | M | 31 (27.4) | NA | [23] |
| N. Camara | Eastern | Tanzania | 85 | 362 | NA | 15–19 | Outbreak | H | 9 (10.6) | NA | [24] |
| D.M. Vu | Eastern | Kenya | 48 | 1,863 | 850 (47.2) | 2–17 | Non-outbreak | H | 11 (22.9) | NA | [25] |
| E. Kinimi | Eastern | Tanzania | 256 | 728 | NA | 1–19 | Non-outbreak | H | NA | 19 (7.4) | [26] |
| E.N. Grossi-Soyster | Eastern | Kenya | 250 | 500 | NA | 15–19 | Non-outbreak | M | 2 (0.8) | 141 (56.4) | [27] |
| E.N. Grossi-Soyster | Eastern | Kenya | 968 | 968 | 51 | 1–17 | Non-outbreak | H | 12 (1.2) | 5 (0.5) | [28] |
| F. Vairo | Eastern | Tanzania | 129 | 481 | NA | 15–19 | Outbreak | M | 12 (9.3) | NA | [29] |
| J.K. Lim | Eastern | Kenya | 140 | 482 | NA | 1–19 | Non-outbreak | H | 76 (54.3) | NA | [30] |
| J.M. Blaylock | Eastern | Kenya | 354 | 354 | NA | 1–4 | Non-outbreak | H | 4 (1.1) | NA | [31] |
| J. Waggener | Eastern | Kenya | 383 | 383 | 193 (50.4) | 0–17 | Non-outbreak | H | NA | 32 (8.4) | [32] |
| J.A. Crump | Eastern | Tanzania | 332 | 870 | NA | 0.2–13 | Non-outbreak | H | 0 | 34 (10.2) | [33] |
| J.T. Hertz | Eastern | Tanzania | 712 | 1447 | NA | 0–19 | Non-outbreak | H | 35 (9.2) | 34 (10.2) | [34] |
| M. Inziani | Eastern | Kenya | 656 | 656 | 340 (51.8) | 1–12 | Non-outbreak | H | 103 (15.7) | 36 (5.5) | [35] |
| S.K. Musak | Eastern | Kenya | 1378 | 1378 | NA | 2–17 | Non-outbreak | M | 10 (0.73) | 95 (6.9) | [36] |
| V.S. Antonio | Eastern | Mozambique | 124 | 392 | NA | 0–19 | Non-outbreak | H | NA | 12 (9.7) | [37] |
| V.S. Antonio | Eastern | Mozambique | 857 | 895 | NA | 0–19 | Non-outbreak | H | NA | 49 (5.7) | [38] |
| D.M. Vu | Eastern | Kenya | 1104 | 1104 | 485 (43.9) | 1–17 | Non-outbreak | M | 82 (7.4) | NA | [39] |
| D.M. Vu | Eastern | Kenya | 1249 | 1249 | NA | 1–17 | Non-outbreak | M | 79 (6.3) | NA | [40] |
| D.M. Vu | Eastern | Kenya | 3835 | 3835 | NA | 1–17 | Non-outbreak | M | 83 (6.2) | 14 (0.8) | [41] |
| A.C. Willcox | Central | Congo | 978 | 978 | NR | 0.5–5 | Non-outbreak | H | 4 (0.4) | NA | [42] |
| H.S. TchetgnaI | Central | Cameroon | 75 | 320 | NR | 3–19 | Non-outbreak | H | 8 (10.7) | NA | [43] |
| J.K. Lim | Central | Gabon | 624 | 682 | NR | 1–19 | Non-outbreak | H | 107 (17.1) | NA | [44] |
| J.J. Gabor | Central | Gabon | 162 | 162 | 83 (51.0) | 3–19 | Outbreak | H | 31 (19.1) | 1 (0.6) | [45] |
| M. Demanou | Central | Cameroon | 435 | 2030 | NA | 2–19 | Non-outbreak | H | 102 (23.4) | NA | [46] |
| S.B. Tchuandom | Central | Cameroon | 961 | 961 | 466 (48.5) | 0.3–15 | Non-outbreak | H | 138 (14.4) | NA | [47] |
| S.B. Tchuandom | Central | Cameroon | 961 | 961 | 467 (48.6) | 0.3–15 | Non-outbreak | H | 59 (6.1) | NA | [48] |
| S. Proesmans | Central | Congo | 180 | 342 | NA | 0–19 | Non-outbreak | H | 9 (5) | 0 | [49] |
| A. Malik | Northern | Sudan | 312 | 312 | 126 (40.4) | 2–15 | Outbreak | M | 36(90) | NA | [50] |
| A. Adam | Northern | Sudan | 55 | 483 | NA | 0–19 | Non-outbreak | H | 29 (52.7) | NA | [51] |
| E.C. Farnon | Northern | Sudan | 240 | 552 | NA | 0–19 | Non-outbreak | M | NA | 13 (5.4) | [52] |
| H. Bower | Northern | Sudan | 37 | 155 | NA | 3–19 | Non-outbreak | H | NA | 34 (91.9) | [53] |
| F. Adedayo | Western | Nigeria | 130 | 130 | 62 (47.7) | 2–18 | Non-outbreak | H | 40 (30.8) | NA | [54] |
| A.B. Onoja | Western | Nigeria | 95 | 274 | NA | 0–10 | Non-outbreak | H | 20 (21.1) | NA | [55] |
| A. Sow | Western | Senegal | 659 | 1409 | NA | 0–14 | Outbreak | H | NA | 6 (0.09) | [56] |
| O.A. Adesina | Western | Nigeria | 15 | 179 | NA | 2–19 | Non-outbreak | H | 5 (33.3) | NA | [57] |
| H.G. Boris | Western | Senegal | 106 | 106 | 64 (60.0) | 0.3–10 | Non-outbreak | H | 3 (2.8) | 0 | [58] |
| I. Dieng | Western | Senegal | 181 | 960 | NA | 0–19 | Non-outbreak | H | 7 (3.9) | NA | [59] |
| J.K. Lim | Western | Burkina Faso | 994 | 2929 | NA | 1–19 | Non-outbreak | H | 210 (21.1) | NA | [60] |
| J.K. Lim | Western | Burkina Faso | 1381 | 2897 | NA | 1–19 | Non-outbreak | H | 611 (44.2) | NA | [61] |
| M.C. Seck | Western | Senegal | 472 | 1465 | NA | 0–15 | Non-outbreak | H | NA | 2 (0.04) | [62] |
| M. Baba | Western | Nigeria | 49 | 310 | 29 (59.2) | 0–19 | Non-outbreak | H | 31 (63.2) | 24 (49.0) | [63] |
| S.A. Nassar | Western | Nigeria | 42 | 170 | NA | 0–19 | Non-outbreak | H | 0 | NA | [64] |
| O.M. Kolawole | Western | Nigeria | 13 | 176 | NA | 0–19 | Non-outbreak | H | 3 (23.1) | NA | [65] |
| S.K. Manu | Western | Ghana | 14 | 260 | NA | 6–19 | Non-outbreak | H | 1 (7.1) | NA | [66] |
| Region | Pooled Prevalence (95% CI) | |
|---|---|---|
| Dengue | Chikungunya | |
| Eastern | 10.70 (4.70, 18.71) | 11.97 (5.45, 20.51) |
| Western | 30.78 (19.23, 43.61) | 4.99 (0.07, 15.33) |
| Central | 16.56 (7.49, 28.13) | 3.36 (0.25, 8.70) |
| Northern | 24.70 (9.31, 44.36) | 10.85 (7.30, 14.94) |
| Africa | 17.02% (95% CI: 11.79, 22.95) | 10.51% (95% CI: 5.66, 16.59) |
| Diagnostic Method | Dengue, n (%) | Chikungunya, n (%) |
|---|---|---|
| IgM-ELISA, IgG-ELISA | 29 (74.4) | 17 (73.9) |
| PCR | 22 (56.4) | 11 (47.8) |
| RT-PCR | 15 (38.5) | 8 (34.8) |
| PRNT | 2 (5.0) | 1 (4.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kayange, N.; Hau, D.K.; Pain, K.; Mshana, S.E.; Peck, R.; Gehring, S.; Groendahl, B.; Koliopoulos, P.; Revocatus, B.; Msaki, E.B.; et al. Seroprevalence of Dengue and Chikungunya Virus Infections in Children Living in Sub-Saharan Africa: Systematic Review and Meta-Analysis. Children 2023, 10, 1662. https://doi.org/10.3390/children10101662
Kayange N, Hau DK, Pain K, Mshana SE, Peck R, Gehring S, Groendahl B, Koliopoulos P, Revocatus B, Msaki EB, et al. Seroprevalence of Dengue and Chikungunya Virus Infections in Children Living in Sub-Saharan Africa: Systematic Review and Meta-Analysis. Children. 2023; 10(10):1662. https://doi.org/10.3390/children10101662
Chicago/Turabian StyleKayange, Neema, Duncan K Hau, Kevin Pain, Stephen E Mshana, Robert Peck, Stephan Gehring, Britta Groendahl, Philip Koliopoulos, Baraka Revocatus, Evarist B Msaki, and et al. 2023. "Seroprevalence of Dengue and Chikungunya Virus Infections in Children Living in Sub-Saharan Africa: Systematic Review and Meta-Analysis" Children 10, no. 10: 1662. https://doi.org/10.3390/children10101662