
The Respiratory Management of the Extreme Preterm in the Delivery Room
 ,
,  ,
,  and
and
Abstract
:1. Introduction
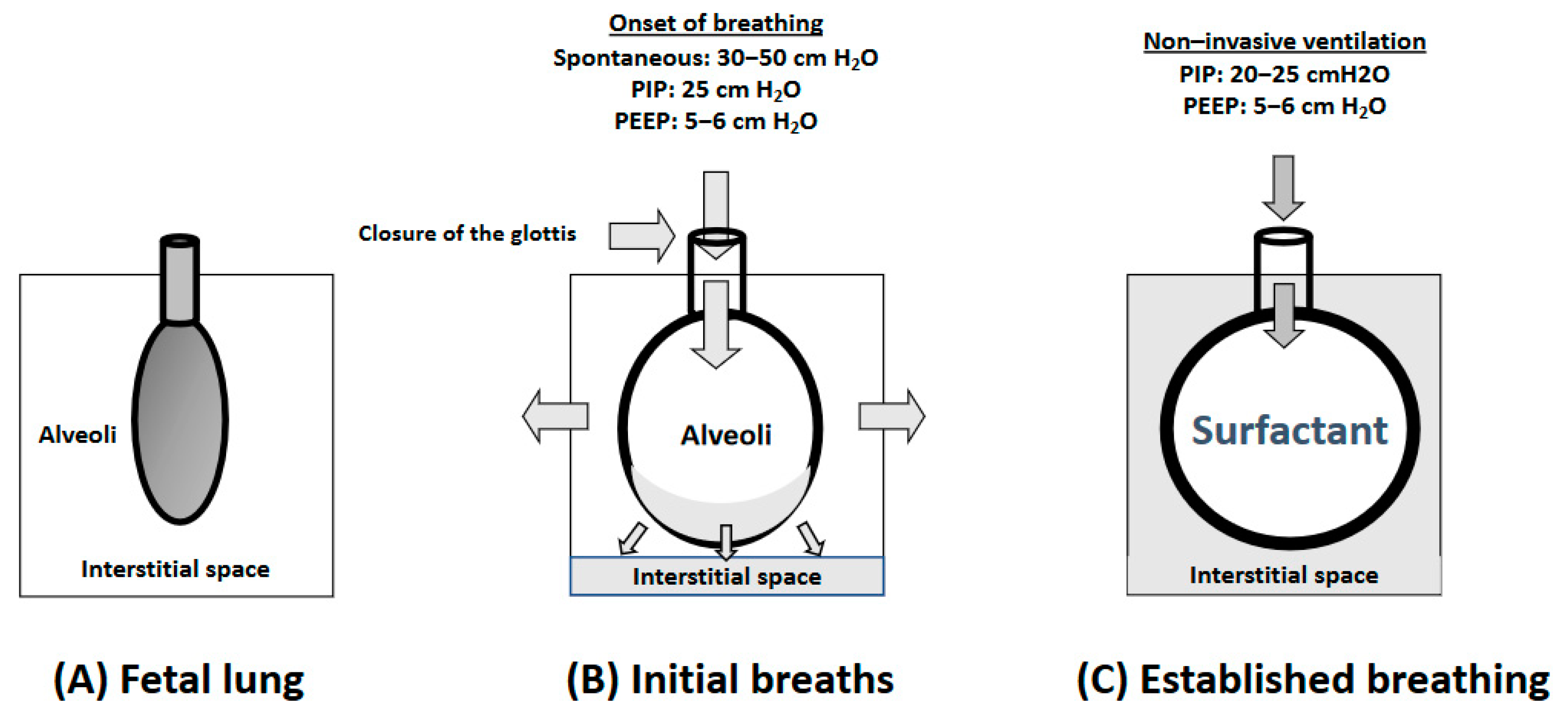
2. Physiology of the Respiratory Fetal-to-Neonatal Transition
3. Oxygen Supplementation in the Delivery Room
3.1. Oxygen in the Fetal-to-Neonatal Transition
3.2. What Initial FiO2 Is Best for Very Preterm Infants in the First Minutes after Birth?
3.3. Long-Term Outcomes and the Initial FiO2
3.4. SpO2 Targets and Oxygen Titration
3.5. Current Recommendations
4. Respiratory Support
4.1. Ventilation in Preterm Infants in the Delivery Room
4.2. Modalities of Non-Invasive Ventilation: CPAP and PPV Plus PEEP
4.3. Type of Devices: T-Piece Resuscitator (TPR), Self-Inflating Bag (SIB), Mechanical Ventilators
4.4. Interfaces for Delivering Mask Non-Invasive Ventilation
4.5. Heated and Humidified Gas (HHG)
4.6. Endotracheal Intubation
4.7. Resuscitation of Extreme Preterm in the Limit of Viability
4.8. Respiratory Function Monitor (RFM)
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gao, Y.; Raj, J.U. Regulation of the pulmonary circulation in the fetus and newborn. Physiol. Rev. 2010, 90, 1291–1335. [Google Scholar] [CrossRef] [PubMed]
- te Pas, A.B.; Wong, C.; Kamlin, C.O.F.; Dawson, J.A.; Morley, C.J.; Davis, P.G. Breathing patterns in preterm and term infants immediately after birth. Pediatr. Res. 2009, 65, 352–356. [Google Scholar] [CrossRef] [PubMed]
- Baixauli-Alacreu, S.; Padilla-Sánchez, C.; Hervás-Marín, D.; Lara-Cantón, I.; Solaz-García, A.; Alemany-Anchel, M.J.; Vento, M. Expired Tidal Volume and Respiratory Rate During Postnatal Stabilization of Newborn Infants Born at Term via Cesarean Delivery. J. Pediatr. X 2021, 6, 100063. [Google Scholar] [CrossRef]
- te Pas, A.B.; Davis, P.G.; Hooper, S.B.; Morley, C.J. From liquid to air: Breathing after birth. J. Pediatr. 2008, 152, 607–611. [Google Scholar] [CrossRef] [PubMed]
- Rawat, M.; Lakshminrusimha, S.; Vento, M. Pulmonary hypertension and oxidative stress: Where is the link? Semin. Fetal Neonatal Med. 2022, 27, 101347. [Google Scholar] [CrossRef]
- Lee, A.C.C.; Kozuki, N.; Blencowe, H.; Vos, T.; Bahalim, A.; Darmstadt, G.L.; Niermeyer, S.; Ellis, M.; Robertson, N.J.; Cousens, S.; et al. Intrapartum-related neonatal encephalopathy incidence and impairment at regional and global levels for 2010 with trends from 1990. Pediatr. Res. 2013, 74 (Suppl. S1), 50–72. [Google Scholar] [CrossRef]
- Wyckoff, M.H.; Wyllie, J.; Aziz, K.; de Almeida, M.F.; Fabres, J.; Fawke, J.; Guinsburg, R.; Hosono, S.; Isayama, T.; Kapadia, V.S.; et al. Neonatal Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2020, 142, S185–S221. [Google Scholar] [CrossRef]
- Vento, M.; Lista, G. Managing preterm infants in the first minutes of life. Paediatr. Respir. Rev. 2015, 16, 151–156. [Google Scholar] [CrossRef]
- Weydig, H.; Ali, N.; Kakkilaya, V. Noninvasive Ventilation in the Delivery Room for the Preterm Infant. Neoreviews 2019, 20, e489–e499. [Google Scholar] [CrossRef]
- Vento, M.; Cheung, P.-Y.; Aguar, M. The first golden minutes of the extremely-low-gestational-age neonate: A gentle approach. Neonatology 2009, 95, 286–298. [Google Scholar] [CrossRef]
- Gomersall, J.; Berber, S.; Middleton, P.; McDonald, S.J.; Niermeyer, S.; El-Naggar, W.; Davis, P.G.; Schmölzer, G.M.; Ovelman, C.; Soll, R.F.; et al. Umbilical Cord Management at Term and Late Preterm Birth: A Meta-analysis. Pediatrics 2021, 147, e2020015404. [Google Scholar] [CrossRef] [PubMed]
- Seidler, A.L.; Gyte, G.M.L.; Rabe, H.; Díaz-Rossello, J.L.; Duley, L.; Aziz, K.; Testoni Costa-Nobre, D.; Davis, P.G.; Schmölzer, G.M.; Ovelman, C.; et al. Umbilical Cord Management for Newborns <34 Weeks’ Gestation: A Meta-analysis. Pediatrics 2021, 147, e20200576. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.A.; Kamlin, C.O.F.; Vento, M.; Wong, C.; Cole, T.J.; Donath, S.M.; Davis, P.G.; Morley, C.J. Defining the reference range for oxygen saturation for infants after birth. Pediatrics 2010, 125, e1340–e1347. [Google Scholar] [CrossRef] [PubMed]
- Padilla-Sánchez, C.; Baixauli-Alacreu, S.; Cañada-Martínez, A.J.; Solaz-García, Á.; Alemany-Anchel, M.J.; Vento, M. Delayed vs. Immediate Cord Clamping Changes Oxygen Saturation and Heart Rate Patterns in the First Minutes after Birth. J. Pediatr. 2020, 227, 149–156.e1. [Google Scholar] [CrossRef] [PubMed]
- Polglase, G.R.; Dawson, J.A.; Kluckow, M.; Gill, A.W.; Davis, P.G.; Te Pas, A.B.; Crossley, K.J.; McDougall, A.; Wallace, E.M.; Hooper, S.B. Ventilation onset prior to umbilical cord clamping (physiological-based cord clamping) improves systemic and cerebral oxygenation in preterm lambs. PLoS One 2015, 10, e0117504. [Google Scholar] [CrossRef] [PubMed]
- Badurdeen, S.; Davis, P.G.; Hooper, S.B.; Donath, S.; Santomartino, G.A.; Heng, A.; Zannino, D.; Hoq, M.; Kamlin, C.O.F.; Kane, S.C.; et al. Physiologically based cord clamping for infants ≥32+0 weeks gestation: A randomised clinical trial and reference percentiles for heart rate and oxygen saturation for infants ≥35+0 weeks gestation. PLoS Med. 2022, 19, e1004029. [Google Scholar] [CrossRef] [PubMed]
- Katheria, A.C.; Brown, M.K.; Faksh, A.; Hassen, K.O.; Rich, W.; Lazarus, D.; Steen, J.; Daneshmand, S.S.; Finer, N.N. Delayed Cord Clamping in Newborns Born at Term at Risk for Resuscitation: A Feasibility Randomized Clinical Trial. J. Pediatr. 2017, 187, 313–317.e1. [Google Scholar] [CrossRef]
- Knol, R.; Brouwer, E.; van den Akker, T.; DeKoninck, P.L.J.; Lopriore, E.; Onland, W.; Vermeulen, M.J.; van den Akker-van Marle, M.E.; van Bodegom-Vos, L.; de Boode, W.P.; et al. Physiological-based cord clamping in very preterm infants: The Aeration, Breathing, Clamping 3 (ABC3) trial-study protocol for a multicentre randomised controlled trial. Trials 2022, 23, 838. [Google Scholar] [CrossRef]
- Ekelöf, K.; Sæther, E.; Santesson, A.; Wilander, M.; Patriksson, K.; Hesselman, S.; Thies-Lagergren, L.; Rabe, H.; Andersson, O. A hybrid type I, multi-center randomized controlled trial to study the implementation of a method for Sustained cord circulation And VEntilation (the SAVE-method) of late preterm and term neonates: A study protocol. BMC Pregnancy Childbirth 2022, 22, 593. [Google Scholar] [CrossRef]
- Pratesi, S.; Montano, S.; Ghirardello, S.; Mosca, F.; Boni, L.; Tofani, L.; Dani, C. Placental Circulation Intact Trial (PCI-T)-Resuscitation with the Placental Circulation Intact vs. Cord Milking for Very Preterm Infants: A Feasibility Study. Front. Pediatr. 2018, 6, 364. [Google Scholar] [CrossRef]
- Finnemore, A.; Groves, A. Physiology of the fetal and transitional circulation. Semin. Fetal Neonatal Med. 2015, 20, 210–216. [Google Scholar] [CrossRef]
- Heldt, G.P.; McIlroy, M.B. Dynamics of chest wall in preterm infants. J. Appl. Physiol. 1987, 62, 170–174. [Google Scholar] [CrossRef] [PubMed]
- te Pas, A.B.; Davis, P.G.; Kamlin, C.O.F.; Dawson, J.; O’Donnell, C.P.F.; Morley, C.J. Spontaneous breathing patterns of very preterm infants treated with continuous positive airway pressure at birth. Pediatr. Res. 2008, 64, 281–285. [Google Scholar] [CrossRef]
- Barker, P.M.; Gowen, C.W.; Lawson, E.E.; Knowles, M.R. Decreased sodium ion absorption across nasal epithelium of very premature infants with respiratory distress syndrome. J. Pediatr. 1997, 130, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Morton, S.U.; Brodsky, D. Fetal Physiology and the Transition to Extrauterine Life. Clin. Perinatol. 2016, 43, 395–407. [Google Scholar] [CrossRef] [PubMed]
- te Pas, A.B.; Siew, M.; Wallace, M.J.; Kitchen, M.J.; Fouras, A.; Lewis, R.A.; Yagi, N.; Uesugi, K.; Donath, S.; Davis, P.G.; et al. Establishing functional residual capacity at birth: The effect of sustained inflation and positive end-expiratory pressure in a preterm rabbit model. Pediatr. Res. 2009, 65, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Hooper, S.B.; Kitchen, M.J.; Polglase, G.R.; Roehr, C.C.; Te Pas, A.B. The physiology of neonatal resuscitation. Curr. Opin. Pediatr. 2018, 30, 187–191. [Google Scholar] [CrossRef]
- Lara-Cantón, I.; Solaz, A.; Parra-Llorca, A.; García-Robles, A.; Millán, I.; Torres-Cuevas, I.; Vento, M. Oxygen Supplementation During Preterm Stabilization and the Relevance of the First 5 min After Birth. Front. Pediatr. 2020, 8, 12. [Google Scholar] [CrossRef]
- Sotiropoulos, J.X.; Vento, M.; Saugstad, O.D.; Oei, J.L. The quest for optimum oxygenation during newborn delivery room resuscitation: Is it the baby or is it us? Semin. Perinatol. 2022, 46, 151622. [Google Scholar] [CrossRef]
- Aziz, K.; Lee, H.C.; Escobedo, M.B.; Hoover, A.V.; Kamath-Rayne, B.D.; Kapadia, V.S.; Magid, D.J.; Niermeyer, S.; Schmölzer, G.M.; Szyld, E.; et al. Part 5: Neonatal Resuscitation: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S524–S550. [Google Scholar] [CrossRef]
- Andersson, O.; Mercer, J.S. Cord Management of the Term Newborn. Clin. Perinatol. 2021, 48, 447–470. [Google Scholar] [CrossRef] [PubMed]
- Kc, A.; Singhal, N.; Gautam, J.; Rana, N.; Andersson, O. Effect of early versus delayed cord clamping in neonate on heart rate, breathing and oxygen saturation during first 10 minutes of birth—randomized clinical trial. Matern. Health Neonatol. Perinatol. 2019, 5, 7. [Google Scholar] [CrossRef]
- Saugstad, O.D.; Ramji, S.; Soll, R.F.; Vento, M. Resuscitation of newborn infants with 21% or 100% oxygen: An updated systematic review and meta-analysis. Neonatology 2008, 94, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Perlman, J.M.; Wyllie, J.; Kattwinkel, J.; Atkins, D.L.; Chameides, L.; Goldsmith, J.P.; Guinsburg, R.; Hazinski, M.F.; Morley, C.; Richmond, S.; et al. Part 11: Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Circulation 2010, 122, S516–S538. [Google Scholar] [CrossRef] [PubMed]
- Kattwinkel, J.; Perlman, J.M.; Aziz, K.; Colby, C.; Fairchild, K.; Gallagher, J.; Hazinski, M.F.; Halamek, L.P.; Kumar, P.; Little, G.; et al. Part 15: Neonatal resuscitation: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010, 122, S909–S919. [Google Scholar] [CrossRef]
- Richmond, S.; Wyllie, J. European Resuscitation Council Guidelines for Resuscitation 2010 Section 7. Resuscitation of babies at birth. Resuscitation 2010, 81, 1389–1399. [Google Scholar] [CrossRef]
- Kapadia, V.S.; Chalak, L.F.; Sparks, J.E.; Allen, J.R.; Savani, R.C.; Wyckoff, M.H. Resuscitation of preterm neonates with limited versus high oxygen strategy. Pediatrics 2013, 132, e1488–e1496. [Google Scholar] [CrossRef]
- Vento, M.; Moro, M.; Escrig, R.; Arruza, L.; Villar, G.; Izquierdo, I.; Roberts, L.J.; Arduini, A.; Escobar, J.J.; Sastre, J.; et al. Preterm resuscitation with low oxygen causes less oxidative stress, inflammation, and chronic lung disease. Pediatrics 2009, 124, e439–e449. [Google Scholar] [CrossRef]
- Wyckoff, M.H.; Aziz, K.; Escobedo, M.B.; Kapadia, V.S.; Kattwinkel, J.; Perlman, J.M.; Simon, W.M.; Weiner, G.M.; Zaichkin, J.G. Part 13: Neonatal Resuscitation: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132, S543–S560. [Google Scholar] [CrossRef]
- Sotiropoulos, J.X.; Kapadia, V.; Vento, M.; Rabi, Y.; Saugstad, O.D.; Kumar, R.K.; Schmölzer, G.M.; Zhang, H.; Yuan, Y.; Lim, G.; et al. Oxygen for the delivery room respiratory support of moderate-to-late preterm infants. An international survey of clinical practice from 21 countries. Acta Paediatr. 2021, 110, 3261–3268. [Google Scholar] [CrossRef]
- Harling, A.E.; Beresford, M.W.; Vince, G.S.; Bates, M.; Yoxall, C.W. Does the use of 50% oxygen at birth in preterm infants reduce lung injury? Arch. Dis. Child. Fetal Neonatal Ed. 2005, 90, F401–F405. [Google Scholar] [CrossRef] [PubMed]
- Stola, A.; Schulman, J.; Perlman, J. Initiating delivery room stabilization/resuscitation in very low birth weight (VLBW) infants with an FiO(2) less than 100% is feasible. J. Perinatol. 2009, 29, 548–552. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.L.; Anderson, C.; Leone, T.A.; Rich, W.; Govindaswami, B.; Finer, N.N. Resuscitation of preterm neonates by using room air or 100% oxygen. Pediatrics 2008, 121, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- Escrig, R.; Arruza, L.; Izquierdo, I.; Villar, G.; Sáenz, P.; Gimeno, A.; Moro, M.; Vento, M. Achievement of targeted saturation values in extremely low gestational age neonates resuscitated with low or high oxygen concentrations: A prospective, randomized trial. Pediatrics 2008, 121, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.A.; Kamlin, C.O.F.; Wong, C.; te Pas, A.B.; O’Donnell, C.P.F.; Donath, S.M.; Davis, P.G.; Morley, C.J. Oxygen saturation and heart rate during delivery room resuscitation of infants <30 weeks’ gestation with air or 100% oxygen. Arch. Dis. Child. Fetal Neonatal Ed. 2009, 94, F87–F91. [Google Scholar] [CrossRef]
- Ezaki, S.; Suzuki, K.; Kurishima, C.; Miura, M.; Weilin, W.; Hoshi, R.; Tanitsu, S.; Tomita, Y.; Takayama, C.; Wada, M.; et al. Resuscitation of preterm infants with reduced oxygen results in less oxidative stress than resuscitation with 100% oxygen. J. Clin. Biochem. Nutr. 2009, 44, 111–118. [Google Scholar] [CrossRef]
- Rabi, Y.; Singhal, N.; Nettel-Aguirre, A. Room-air versus oxygen administration for resuscitation of preterm infants: The ROAR study. Pediatrics 2011, 128, e374–e381. [Google Scholar] [CrossRef]
- Armanian, A.M.; Badiee, Z. Resuscitation of preterm newborns with low concentration oxygen versus high concentration oxygen. J. Res. Pharm. Pract. 2012, 1, 25–29. [Google Scholar] [CrossRef]
- Rook, D.; Schierbeek, H.; Vento, M.; Vlaardingerbroek, H.; van der Eijk, A.C.; Longini, M.; Buonocore, G.; Escobar, J.; van Goudoever, J.B.; Vermeulen, M.J. Resuscitation of preterm infants with different inspired oxygen fractions. J. Pediatr. 2014, 164, 1322–1326.e3. [Google Scholar] [CrossRef]
- Aguar, M.; Brugada, M.; Escobar, J.J. Resuscitation of ELBW Infants with Initial FiO2 30% vs. 60%, a Randomized, Controlled, Blinded Study: The REOX Trial. In Proceedings of the PAS Annual Meeting, Washington, DC, USA, 4–7 May 2013. [Google Scholar]
- Oei, J.L.; Saugstad, O.D.; Lui, K.; Wright, I.M.; Smyth, J.P.; Craven, P.; Wang, Y.A.; McMullan, R.; Coates, E.; Ward, M.; et al. Targeted Oxygen in the Resuscitation of Preterm Infants, a Randomized Clinical Trial. Pediatrics 2017, 139, e20161452. [Google Scholar] [CrossRef] [Green Version]
- Lui, K.; Jones, L.J.; Foster, J.P.; Davis, P.G.; Ching, S.K.; Oei, J.L.; Osborn, D.A. Lower versus higher oxygen concentrations titrated to target oxygen saturations during resuscitation of preterm infants at birth. Cochrane Database Syst. Rev. 2018, 5, CD010239. [Google Scholar] [CrossRef]
- Welsford, M.; Nishiyama, C.; Shortt, C.; Weiner, G.; Roehr, C.C.; Isayama, T.; Dawson, J.A.; Wyckoff, M.H.; Rabi, Y. International Liaison Committee on Resuscitation Neonatal Life Support Task Force Initial Oxygen Use for Preterm Newborn Resuscitation: A Systematic Review With Meta-analysis. Pediatrics 2019, 143, e20181828. [Google Scholar] [CrossRef] [PubMed]
- Soraisham, A.S.; Rabi, Y.; Shah, P.S.; Singhal, N.; Synnes, A.; Yang, J.; Lee, S.K.; Lodha, A.K. Neurodevelopmental outcomes of preterm infants resuscitated with different oxygen concentration at birth. J. Perinatol. 2017, 37, 1141–1147. [Google Scholar] [CrossRef] [PubMed]
- Kapadia, V.S.; Lal, C.V.; Kakkilaya, V.; Heyne, R.; Savani, R.C.; Wyckoff, M.H. Impact of the Neonatal Resuscitation Program–Recommended Low Oxygen Strategy on Outcomes of Infants Born Preterm. J. Pediatr. 2017, 191, 35–41. [Google Scholar] [CrossRef]
- Boronat, N.; Aguar, M.; Rook, D.; Iriondo, M.; Brugada, M.; Cernada, M.; Nuñez, A.; Izquierdo, M.; Cubells, E.; Martinez, M.; et al. Survival and Neurodevelopmental Outcomes of Preterms Resuscitated With Different Oxygen Fractions. Pediatrics 2016, 138, e20161405. [Google Scholar] [CrossRef] [PubMed]
- Thamrin, V.; Saugstad, O.D.; Tarnow-Mordi, W.; Wang, Y.A.; Lui, K.; Wright, I.M.; De Waal, K.; Travadi, J.; Smyth, J.P.; Craven, P.; et al. Preterm Infant Outcomes after Randomization to Initial Resuscitation with FiO2 0.21 or 1.0. J. Pediatr. 2018, 201, 55–61.e1. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.A.; Vento, M.; Finer, N.N.; Rich, W.; Saugstad, O.D.; Morley, C.J.; Davis, P.G. Managing oxygen therapy during delivery room stabilization of preterm infants. J. Pediatr. 2012, 160, 158–161. [Google Scholar] [CrossRef]
- Madar, J.; Roehr, C.C.; Ainsworth, S.; Ersdal, H.; Morley, C.; Rüdiger, M.; Skåre, C.; Szczapa, T.; Te Pas, A.; Trevisanuto, D.; et al. European Resuscitation Council Guidelines 2021: Newborn resuscitation and support of transition of infants at birth. Resuscitation 2021, 161, 291–326. [Google Scholar] [CrossRef]
- Rabi, Y.; Lodha, A.; Soraisham, A.; Singhal, N.; Barrington, K.; Shah, P.S. Outcomes of preterm infants following the introduction of room air resuscitation. Resuscitation 2015, 96, 252–259. [Google Scholar] [CrossRef]
- Oei, J.L.; Vento, M.; Rabi, Y.; Wright, I.; Finer, N.; Rich, W.; Kapadia, V.; Aune, D.; Rook, D.; Tarnow-Mordi, W.; et al. Higher or lower oxygen for delivery room resuscitation of preterm infants below 28 completed weeks gestation: A meta-analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 102, F24–F30. [Google Scholar] [CrossRef]
- Oei, J.L.; Finer, N.N.; Saugstad, O.D.; Wright, I.M.; Rabi, Y.; Tarnow-Mordi, W.; Rich, W.; Kapadia, V.; Rook, D.; Smyth, J.P.; et al. Outcomes of oxygen saturation targeting during delivery room stabilisation of preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F446–F454. [Google Scholar] [CrossRef] [PubMed]
- Oei, J.L.; Kapadia, V.; Rabi, Y.; Saugstad, O.D.; Rook, D.; Vermeulen, M.J.; Boronat, N.; Thamrin, V.; Tarnow-Mordi, W.; Smyth, J.; et al. Neurodevelopmental outcomes of preterm infants after randomisation to initial resuscitation with lower (FiO2 < 0.3) or higher (FiO2 > 0.6) initial oxygen levels. An individual patient meta-analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2022, 107, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Dekker, J.; Hooper, S.B.; Croughan, M.K.; Crossley, K.J.; Wallace, M.J.; McGillick, E.V.; DeKoninck, P.L.J.; Thio, M.; Martherus, T.; Ruben, G.; et al. Increasing Respiratory Effort With 100% Oxygen During Resuscitation of Preterm Rabbits at Birth. Front. Pediatr. 2019, 7, 427. [Google Scholar] [CrossRef] [PubMed]
- Dekker, J.; Martherus, T.; Lopriore, E.; Giera, M.; McGillick, E.V.; Hutten, J.; van Leuteren, R.W.; van Kaam, A.H.; Hooper, S.B.; Te Pas, A.B. The Effect of Initial High vs. Low FiO2 on Breathing Effort in Preterm Infants at Birth: A Randomized Controlled Trial. Front. Pediatr. 2019, 7, 504. [Google Scholar] [CrossRef]
- Norman, M.; Jonsson, B.; Wallström, L.; Sindelar, R. Respiratory support of infants born at 22–24 weeks of gestational age. Semin. Fetal Neonatal Med. 2022, 27, 101328. [Google Scholar] [CrossRef] [PubMed]
- Schwaberger, B.; Urlesberger, B.; Schmölzer, G.M. Delivery Room Care for Premature Infants Born after Less than 25 Weeks’ Gestation—A Narrative Review. Children 2021, 8, 882. [Google Scholar] [CrossRef]
- García-Muñoz Rodrigo, F.; Losada Martínez, A.; Elorza Fernández, M.D.; Moreno Hernando, J.; Figueras Aloy, J.; Vento Torres, M. The Burden of Respiratory Disease in Very-Low-Birth-Weight Infants: Changes in Perinatal Care and Outcomes in a Decade in Spain. Neonatology 2017, 112, 30–39. [Google Scholar] [CrossRef]
- Sweet, D.G.; Carnielli, V.; Greisen, G.; Hallman, M.; Ozek, E.; te Pas, A.; Plavka, R.; Roehr, C.C.; Saugstad, O.D.; Simeoni, U.; et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome—2019 Update. Neonatology 2019, 115, 432–450. [Google Scholar] [CrossRef]
- Sindelar, R.; Nakanishi, H.; Stanford, A.H.; Colaizy, T.T.; Klein, J.M. Respiratory management for extremely premature infants born at 22 to 23 weeks of gestation in proactive centers in Sweden, Japan, and USA. Semin. Perinatol. 2022, 46, 151540. [Google Scholar] [CrossRef]
- Martherus, T.; Oberthuer, A.; Dekker, J.; Hooper, S.B.; McGillick, E.V.; Kribs, A.; te Pas, A.B. Supporting breathing of preterm infants at birth: A narrative review. Arch. Dis. Child. Fetal Neonatal Ed. 2019, 104, F102–F107. [Google Scholar] [CrossRef]
- Lista, G.; Fontana, P.; Castoldi, F.; Cavigioli, F.; Bianchi, S.; Bastrenta, P. ELBW infants: To intubate or not to intubate in the delivery room? J. Matern. Fetal Neonatal Med. 2012, 25, 55–57. [Google Scholar] [CrossRef]
- Hinder, M.; McEwan, A.; Drevhammer, T.; Donaldson, S.; Tracy, M.B. T-piece resuscitators: How do they compare? Arch. Dis. Child. Fetal Neonatal Ed. 2019, 104, F122–F127. [Google Scholar] [CrossRef]
- Jeevan, A.; Balasubramanian, H.; Kabra, N. Effect of T-Piece Resuscitator versus Self Inflating Bag on Arterial CO2 Levels in Preterm Neonates. Indian J. Pediatr. 2020, 87, 897–904. [Google Scholar] [CrossRef]
- Sarrato, G.Z.; Luna, M.S.; Sarrato, S.Z.; Pérez, A.P.; Chamorro, I.P.; Cano, J.M.B. New Strategies of Pulmonary Protection of Preterm Infants in the Delivery Room with the Respiratory Function Monitoring. Am. J. Perinatol. 2019, 36, 1368–1376. [Google Scholar] [CrossRef]
- Weiner, G.M.; Zaichkin, J. Textbook of Neonatal Resuscitation, 8th ed.; American Academy of Pediatrics: Itasca, IL, USA, 2021; ISBN 978-1-61002-524-9. [Google Scholar]
- Mehler, K.; Grimme, J.; Abele, J.; Huenseler, C.; Roth, B.; Kribs, A. Outcome of extremely low gestational age newborns after introduction of a revised protocol to assist preterm infants in their transition to extrauterine life. Acta Paediatr. 2012, 101, 1232–1239. [Google Scholar] [CrossRef]
- Petrillo, F.; Valenzano, L.; Franco, C.; Calò, G.; Dentico, D.; Manzoni, P.; D’Amato, G.; Del Vecchio, A. Pulmonary Recruitment Strategy in Preterm Neonates < 29 Weeks of Gestational Age to Reduce the Need for Intubation in the Delivery Room. Am. J. Perinatol. 2019, 36, S115–S119. [Google Scholar] [CrossRef] [PubMed]
- Mian, Q.; Cheung, P.-Y.; O’Reilly, M.; Barton, S.K.; Polglase, G.R.; Schmölzer, G.M. Impact of delivered tidal volume on the occurrence of intraventricular haemorrhage in preterm infants during positive pressure ventilation in the delivery room. Arch. Dis. Child. Fetal Neonatal Ed. 2019, 104, F57–F62. [Google Scholar] [CrossRef]
- PPolglase, G.R.; Hillman, N.H.; Pillow, J.J.; Cheah, F.-C.; Nitsos, I.; Moss, T.J.M.; Kramer, B.W.; Ikegami, M.; Kallapur, S.G.; Jobe, A.H. Positive end-expiratory pressure and tidal volume during initial ventilation of preterm lambs. Pediatr. Res. 2008, 64, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Mulrooney, N.; Champion, Z.; Moss, T.J.M.; Nitsos, I.; Ikegami, M.; Jobe, A.H. Surfactant and Physiologic Responses of Preterm Lambs to Continuous Positive Airway Pressure. Am. J. Respir. Crit. Care Med. 2005, 171, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Kitchen, M.J.; Siew, M.L.; Wallace, M.J.; Fouras, A.; Lewis, R.A.; Yagi, N.; Uesugi, K.; Pas, A.T.; Hooper, S.B. Changes in positive end-expiratory pressure alter the distribution of ventilation within the lung immediately after birth in newborn rabbits. PLoS ONE 2014, 9, e93391. [Google Scholar] [CrossRef]
- Morley, C.J.; Davis, P.G.; Doyle, L.W.; Brion, L.P.; Hascoet, J.-M.; Carlin, J.B. COIN Trial Investigators Nasal CPAP or intubation at birth for very preterm infants. N. Engl. J. Med. 2008, 358, 700–708. [Google Scholar] [CrossRef] [PubMed]
- SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research Network. Early CPAP versus surfactant in extremely preterm infants. N. Engl. J. Med. 2010, 362, 1970–1979. [Google Scholar] [CrossRef] [PubMed]
- Holte, K.; Ersdal, H.; Eilevstjønn, J.; Gomo, Ø.; Klingenberg, C.; Thallinger, M.; Linde, J.; Stigum, H.; Yeconia, A.; Kidanto, H.; et al. Positive End-Expiratory Pressure in Newborn Resuscitation Around Term: A Randomized Controlled Trial. Pediatrics 2020, 146, e20200494. [Google Scholar] [CrossRef] [PubMed]
- Hillman, N.H.; Moss, T.J.M.; Kallapur, S.G.; Bachurski, C.; Pillow, J.J.; Polglase, G.R.; Nitsos, I.; Kramer, B.W.; Jobe, A.H. Brief, Large Tidal Volume Ventilation Initiates Lung Injury and a Systemic Response in Fetal Sheep. Am. J. Respir. Crit. Care Med. 2007, 176, 575–581. [Google Scholar] [CrossRef]
- Haddad, L.; Mascaretti, R.; Valle, L.; Rebello, C. A Self-Inflating Bag May Cause Hypocapnia in a Rabbit Model of Manual Ventilation Compared to the T-piece Resuscitator. Am. J. Perinatol. 2017, 34, 1405–1410. [Google Scholar] [CrossRef]
- Hawkes, C.P.; Ryan, C.A.; Dempsey, E.M. Comparison of the T-piece resuscitator with other neonatal manual ventilation devices: A qualitative review. Resuscitation 2012, 83, 797–802. [Google Scholar] [CrossRef]
- Bennett, S.; Finer, N.N.; Rich, W.; Vaucher, Y. A comparison of three neonatal resuscitation devices. Resuscitation 2005, 67, 113–118. [Google Scholar] [CrossRef]
- Finer, N.N.; Rich, W.; Craft, A.; Henderson, C. Comparison of methods of bag and mask ventilation for neonatal resuscitation. Resuscitation 2001, 49, 299–305. [Google Scholar] [CrossRef]
- Roehr, C.C.; Davis, P.G.; Weiner, G.M.; Jonathan Wyllie, J.; Wyckoff, M.H.; Trevisanuto, D. T-piece resuscitator or self-inflating bag during neonatal resuscitation: A scoping review. Pediatr. Res. 2021, 89, 760–766. [Google Scholar] [CrossRef]
- Thakur, A.; Saluja, S.; Modi, M.; Kler, N.; Garg, P.; Soni, A.; Kaur, A.; Chetri, S. T-piece or self inflating bag for positive pressure ventilation during delivery room resuscitation: An RCT. Resuscitation 2015, 90, 21–24. [Google Scholar] [CrossRef]
- Guinsburg, R.; de Almeida, M.F.B.; de Castro, J.S.; Gonçalves-Ferri, W.A.; Marques, P.F.; Caldas, J.P.S.; Krebs, V.L.J.; de Souza Rugolo, L.M.S.; de Almeida, J.H.C.L.; Luz, J.H.; et al. T-piece versus self-inflating bag ventilation in preterm neonates at birth. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F49–F55. [Google Scholar] [CrossRef] [PubMed]
- Drevhammar, T.; Nilsson, K.; Zetterström, H.; Jonsson, B. Comparison of seven infant continuous positive airway pressure systems using simulated neonatal breathing. Pediatr. Crit. Care Med. 2012, 13, e113–e119. [Google Scholar] [CrossRef] [PubMed]
- Donaldsson, S.; Drevhammar, T.; Li, Y.; Bartocci, M.; Rettedal, S.I.; Lundberg, F.; Odelberg-Johnson, P.; Szczapa, T.; Thordarson, T.; Pilypiene, I.; et al. Comparison of Respiratory Support After Delivery in Infants Born Before 28 Weeks’ Gestational Age: The CORSAD Randomized Clinical Trial. JAMA Pediatr. 2021, 175, 911. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, C.P.F. Neonatal resuscitation 2: An evaluation of manual ventilation devices and face masks. Arch. Dis. Child. Fetal Neonatal Ed. 2005, 90, F392–F396. [Google Scholar] [CrossRef]
- Schmölzer, G.M.; Dawson, J.A.; Kamlin, C.O.F.; O’Donnell, C.P.F.; Morley, C.J.; Davis, P.G. Airway obstruction and gas leak during mask ventilation of preterm infants in the delivery room. Arch. Dis. Child. Fetal Neonatal Ed. 2011, 96, F254–F257. [Google Scholar] [CrossRef] [PubMed]
- Green, E.A.; Dawson, J.A.; Davis, P.G.; De Paoli, A.G.; Roberts, C.T. Assessment of resistance of nasal continuous positive airway pressure interfaces. Arch. Dis. Child. Fetal Neonatal Ed. 2019, 104, F535–F539. [Google Scholar] [CrossRef]
- Biniwale, M.; Wertheimer, F. Decrease in delivery room intubation rates after use of nasal intermittent positive pressure ventilation in the delivery room for resuscitation of very low birth weight infants. Resuscitation 2017, 116, 33–38. [Google Scholar] [CrossRef]
- van Vonderen, J.J.; Kamlin, C.O.; Dawson, J.A.; Walther, F.J.; Davis, P.G.; te Pas, A.B. Mask versus Nasal Tube for Stabilization of Preterm Infants at Birth: Respiratory Function Measurements. J. Pediatr. 2015, 167, 81–85.e1. [Google Scholar] [CrossRef]
- Mani, S.; Pinheiro, J.M.B.; Rawat, M. Laryngeal Masks in Neonatal Resuscitation—A Narrative Review of Updates 2022. Children 2022, 9, 733. [Google Scholar] [CrossRef]
- Pejovic, N.J.; Myrnerts Höök, S.; Byamugisha, J.; Alfvén, T.; Lubulwa, C.; Cavallin, F.; Nankunda, J.; Ersdal, H.; Segafredo, G.; Blennow, M.; et al. Neonatal resuscitation using a supraglottic airway device for improved mortality and morbidity outcomes in a low-income country: Study protocol for a randomized trial. Trials 2019, 20, 444. [Google Scholar] [CrossRef] [Green Version]
- Crawshaw, J.R.; Kitchen, M.J.; Binder-Heschl, C.; Thio, M.; Wallace, M.J.; Kerr, L.T.; Roehr, C.C.; Lee, K.L.; A Buckley, G.; Davis, P.G.; et al. Laryngeal closure impedes non-invasive ventilation at birth. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 103, F112–F119. [Google Scholar] [CrossRef] [PubMed]
- Kuypers, K.L.A.M.; Lamberska, T.; Martherus, T.; Dekker, J.; Böhringer, S.; Hooper, S.B.; Plavka, R.; te Pas, A.B. The effect of a face mask for respiratory support on breathing in preterm infants at birth. Resuscitation 2019, 144, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Kuypers, K.L.A.M.; Lamberska, T.; Martherus, T.; Dekker, J.; Böhringer, S.; Hooper, S.B.; Plavka, R.; te Pas, A.B. Comparing the effect of two different interfaces on breathing of preterm infants at birth: A matched-pairs analysis. Resuscitation 2020, 157, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, M.; Mense, L.; Springer, L.; Dekker, J. Tactile stimulation in the delivery room: Past, present, future. A systematic review. Pediatr. Res. 2022, 5, 1–9. [Google Scholar] [CrossRef]
- Abdel-Hady, H. Humidification and heating of inspired gas during delivery room stabilization improves admission temperature in preterm infants. Acta Paediatr. 2017, 106, 682. [Google Scholar] [CrossRef]
- Meyer, M.P.; Owen, L.S.; te Pas, A.B. Use of Heated Humidified Gases for Early Stabilization of Preterm Infants: A Meta-Analysis. Front. Pediatr. 2018, 6, 319. [Google Scholar] [CrossRef]
- Stevens, T.P.; Finer, N.N.; Carlo, W.A.; Szilagyi, P.G.; Phelps, D.L.; Walsh, M.C.; Gantz, M.G.; Laptook, A.R.; Yoder, B.A.; Faix, R.G.; et al. Respiratory Outcomes of the Surfactant Positive Pressure and Oximetry Randomized Trial (SUPPORT). J. Pediatr. 2014, 165, 240–249.e4. [Google Scholar] [CrossRef]
- Dunn, M.S.; Kaempf, J.; de Klerk, A.; de Klerk, R.; Reilly, M.; Howard, D.; Ferrelli, K.; O’Conor, J.; Soll, R.F. Vermont Oxford Network DRM Study Group Randomized trial comparing 3 approaches to the initial respiratory management of preterm neonates. Pediatrics 2011, 128, e1069–e1076. [Google Scholar] [CrossRef]
- Sandri, F.; Plavka, R.; Ancora, G.; Simeoni, U.; Stranak, Z.; Martinelli, S.; Mosca, F.; Nona, J.; Thomson, M.; Verder, H.; et al. Prophylactic or early selective surfactant combined with nCPAP in very preterm infants. Pediatrics 2010, 125, e1402–e1409. [Google Scholar] [CrossRef]
- Schmolzer, G.M.; Kumar, M.; Pichler, G.; Aziz, K.; O’Reilly, M.; Cheung, P.-Y. Non-invasive versus invasive respiratory support in preterm infants at birth: Systematic review and meta-analysis. BMJ 2013, 347, f5980. [Google Scholar] [CrossRef] [Green Version]
- Fischer, H.S.; Bührer, C. Avoiding Endotracheal Ventilation to Prevent Bronchopulmonary Dysplasia: A Meta-analysis. Pediatrics 2013, 132, e1351–e1360. [Google Scholar] [CrossRef]
- Abdel-Latif, M.E.; Davis, P.G.; Wheeler, K.I.; De Paoli, A.G.; Dargaville, P.A. Surfactant therapy via thin catheter in preterm infants with or at risk of respiratory distress syndrome. Cochrane Database Syst. Rev. 2021, 2021, CD011672. [Google Scholar] [CrossRef]
- Kusuda, S.; Nakanishi, H.; Oei, J.L. Practical procedures for the delivery room resuscitation of micropreemies. Semin. Fetal Neonatal Med. 2022, 27, 101349. [Google Scholar] [CrossRef] [PubMed]
- Zeballos-Sarrato, S.; Villar-Castro, S.; Zeballos-Sarrato, G.; Ramos-Navarro, C.; González-Pacheco, N.; Sánchez Luna, M. Survival estimations at the limit of viability. J. Matern. -Fetal Neonatal Med. 2016, 29, 3660–3664. [Google Scholar] [CrossRef]
- Murthy, V.; D’Costa, W.; Shah, R.; Fox, G.F.; Campbell, M.E.; Milner, A.D.; Greenough, A. Prematurely born infants’ response to resuscitation via an endotracheal tube or a face mask. Early Hum. Dev. 2015, 91, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Bhat, P.; Hunt, K.; Harris, C.; Murthy, V.; Milner, A.D.; Greenough, A. Inflation pressures and times during initial resuscitation in preterm infants. Pediatr. Int. 2017, 59, 906–910. [Google Scholar] [CrossRef]
- Lamberska, T.; Luksova, M.; Smisek, J.; Vankova, J.; Plavka, R. Premature infants born at <25 weeks of gestation may be compromised by currently recommended resuscitation techniques. Acta Paediatr. 2016, 105, e142–e150. [Google Scholar] [CrossRef]
- Schmölzer, G.M.; Morley, C.J.; Wong, C.; Dawson, J.A.; Kamlin, C.O.F.; Donath, S.M.; Hooper, S.B.; Davis, P.G. Respiratory function monitor guidance of mask ventilation in the delivery room: A feasibility study. J. Pediatr. 2012, 160, 377–381.e2. [Google Scholar] [CrossRef] [PubMed]
- van Zanten, H.A.; Kuypers, K.L.A.M.; van Zwet, E.W.; van Vonderen, J.J.; Kamlin, C.O.F.; Springer, L.; Lista, G.; Cavigioli, F.; Vento, M.; Núñez-Ramiro, A.; et al. A multi-centre randomised controlled trial of respiratory function monitoring during stabilisation of very preterm infants at birth. Resuscitation 2021, 167, 317–325. [Google Scholar] [CrossRef] [PubMed]
- de Medeiros, S.M.; Mangat, A.; Polglase, G.R.; Sarrato, G.Z.; Davis, P.G.; Schmölzer, G.M. Respiratory function monitoring to improve the outcomes following neonatal resuscitation: A systematic review and meta-analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2022, 107, 589–596. [Google Scholar] [CrossRef] [PubMed]
- International Liaison Committee on Resuscitation. Consensus on Science with Treatment Recommendations (CoSTR) Home Page. Available online: https://www.ilcor.org/home (accessed on 14 February 2022).
- Kuypers, K.L.A.M.; van Zanten, H.A.; Heesters, V.; Kamlin, O.; Springer, L.; Lista, G.; Cavigioli, F.; Vento, M.; Núñez-Ramiro, A.; Kuester, H.; et al. Resuscitators’ opinions on using a respiratory function monitor during neonatal resuscitation. Acta Paediatr. 2022, 112, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Finn, D.; Boylan, G.B.; Ryan, C.A.; Dempsey, E.M. Enhanced Monitoring of the Preterm Infant during Stabilization in the Delivery Room. Front. Pediatr. 2016, 4, 30. [Google Scholar] [CrossRef] [PubMed]
- Kakkilaya, V.; Jubran, I.; Mashruwala, V.; Ramon, E.; Simcik, V.N.; Marshall, M.; Brown, L.S.; Jaleel, M.A.; Kapadia, V.S. Quality Improvement Project to Decrease Delivery Room Intubations in Preterm Infants. Pediatrics 2019, 143, e20180201. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Study Design | [Initial FiO2] | Objectives | Outcomes |
|---|---|---|---|---|
| Harling 2005 [41] | RCT GA < 31 weeks No PO; No SpO2 targets, n = 52 | 0.5 vs. 1.0 | ↓ lung inflammation | No significant differences in lung inflammation. It is possible to use lower FiO2. |
| Stola 2005 [42] | Cohort WB < 1500 g PO & target SpO2; n = 100 | Variable vs. 1.0 | Viability PaO2 at NICU admission | ↓ PaO2 at NICU admission with lower FiO2 Is possible to use less FiO2. |
| Wang 2008 [43] | RCT GA < 32 weeks PO & target SpO2; n = 41 | 0.21 vs. 1.0 | Viability; SpO2 targets: 80–85% at 5 min 85–90% at 7 min | Supplemental O2 necessary in 21% group. |
| Escrig 2008 [44] Vento 2009 [38] | RCT GA < 28 weeks PO & target SpO2 n = 78 | 0.3 vs. 0.9 | SpO2 target 85% at 10 min Oxidative stress; Inflammation | It is possible use less FiO2. Less oxidative stress and inflammation in 30% arm. |
| Dawson 2009 [45] | Cohort GA < 30 weeks PO & target SpO2; n = 43 | 0.21 vs. 1.0 | Viability SpO2 target 90% at 10 min | Supplemental O2 is necessary in 21% arm. Is possible to use less FiO2 |
| Ezaki 2009 [46] | PO & target SpO2 n = 44 | Variable vs. 1.0 | Oxidative stress | ↑ oxidative stress in 100% group. |
| Rabi 2011 [47] | RCT GA < 32 weeks PO & target SpO2; n = 106 | Static 1 vs 0.21 titrate or 1.0 titrate | Viability SpO2 target 85–92% | Titrating is more effective than static No differences in timing between the 3 groups to reach the target SpO2 range |
| Armanian 2012 [48] | RCT GA 29–34 weeks PO & target SpO2 n = 32 | 0.3 vs. 1.0 | SpO2 target 85% | It is possible to use less FiO2. |
| Rook 2014 [49] | RCT GA < 32 weeks PO & target SpO2 n = 193 | 0.3 vs. 0.65 | Major neonatal illness Oxidative stress BPD 36 PMA SpO2 target 88–94% at 10 min | 30% is as safe as 65%. No differences in oxidate stress or BPD. No differences in oxidative stress biomarkers |
| Kapadia 2013 [37] | RCT GA 24–34 weeks PO & target SpO2 n = 193 | 0.21 vs. 1.0 | Oxidative stress Short-term morbidities SpO2 target 88–94% | It is possible to use less FiO2 Using 21% resulted in less oxidative stress, neonatal morbidities, and need for oxygen supplementation. |
| Aguar 2013 [50] | RCT GA < 30 weeks PO & target SpO2 n = 60 | 0.30 vs. 0.60 | Death at 28 days and morbidities SpO2 target 88–94% at 10 min | It is possible to use less FiO2 No differences in oxidative stress, neonatal morbidities, or mortality. |
| Oei 2017 [51] | RCT GA < 32 weeks PO & target SpO2 n = 287 | 0.21 vs. 1.0 | Major disability and death at 2 y SpO2 target 65–95% at 5 min and 85–95% until NICU admission | Increased risk of death in infants <28 weeks in the lower FiO2 group. |
| Study Design | [Initial FiO2] | Objectives | Neurodevelopmental Evaluation Test | Outcomes | |
|---|---|---|---|---|---|
| Boronat [56] | RCT GA ≤ 32 weeks Pulseoximetry Target SPO2 n = 206 | 0.3–0.6 | Outcome at 24 months postmenstrual age (PMA) | Bayley III | No differences |
| Soraisham [54] | Retrospective cohort GA ≤ 28 weeks n = 1509 | 0.21–1.0 | Outcome at 18–21 months PMA | Bayley III | Severe NDI in survivors was significantly higher in the 100% oxygen group |
| Kapadia [55] | Retrospective cohort GA ≤ 28 weeks n = 199 | 0.21–1.0 | Outcome at 22–26 months PMA | Bayley III | No differences |
| Thamrin [57] | RCT GA < 32 weeks n = 215 | 0.21–1.0 | Death or NDI at 24 months PMA | Bayley III | No differences SpO2 < 80% were more likely to die or to have NDI |
|
| Before birth | Assemble designated staff. Brief with attending team. Prepare delivery room. Use checklists. Information to parents. |
| Thermal care | Plastic bag without drying. Radiant warmer, room temperature 21–25 °C. Humidified, tempered (36–37 °C) gases for ventilation. |
| Delayed cord clamping [12] | Any gestational age if resuscitation isn’t needed. |
| Initial ventilatory support at stabilization (while placing ECG leads on the infant’s chest) |
|
| ETT size internal diameter/intubation depth |
|
| Initial PIP set not to exceed 20 cmH2O (TPR flow 10 L/min) [70,75] |
|
| If use RFM | set volume targeted 2.5 mL (5 mL/kg), Ti set <1 s and RR 60/min guide by CO2et |
| Initial FiO2 [13] | 0.3 Titration to achieve SpO2 targets of 80–85% at 5 min |
| Suggested first intended ventilatory settings [70,75,115] | CV: PIP = 20–22 cmH2O, PEEP = 5 cmH2O, backup frequency = 40–60/min, VT = 4–6 mL/kg. HFOV + VThf 1 mL: MAP = 10–12 cmH2O, frequency = 14–15 Hz, initial amplitude 40–50 cmH2O *, I:E 1:2 (1:1 if >15 Hz). Saturation limits: 90–92%. |
| Surfactant administration | within 2 h of life |
| After birth | Debriefing with the attending team |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Escrig-Fernández, R.; Zeballos-Sarrato, G.; Gormaz-Moreno, M.; Avila-Alvarez, A.; Toledo-Parreño, J.D.; Vento, M. The Respiratory Management of the Extreme Preterm in the Delivery Room. Children 2023, 10, 351. https://doi.org/10.3390/children10020351
Escrig-Fernández R, Zeballos-Sarrato G, Gormaz-Moreno M, Avila-Alvarez A, Toledo-Parreño JD, Vento M. The Respiratory Management of the Extreme Preterm in the Delivery Room. Children. 2023; 10(2):351. https://doi.org/10.3390/children10020351
Chicago/Turabian StyleEscrig-Fernández, Raquel, Gonzalo Zeballos-Sarrato, María Gormaz-Moreno, Alejandro Avila-Alvarez, Juan Diego Toledo-Parreño, and Máximo Vento. 2023. "The Respiratory Management of the Extreme Preterm in the Delivery Room" Children 10, no. 2: 351. https://doi.org/10.3390/children10020351