
Schroth Physiotherapeutic Scoliosis-Specific Exercise (PSSE) Trials—Systematic Review of Methods and Recommendations for Future Research

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. General Characteristics, Methodological Approaches, Treatment Protocols, and Outcomes Reporting
3.1.1. General Characteristics of the Included Studies
3.1.2. Methodological Approaches of the Included Studies
3.1.3. Treatment Protocols of the Included Studies
3.1.4. Outcomes Reporting of the Included Studies
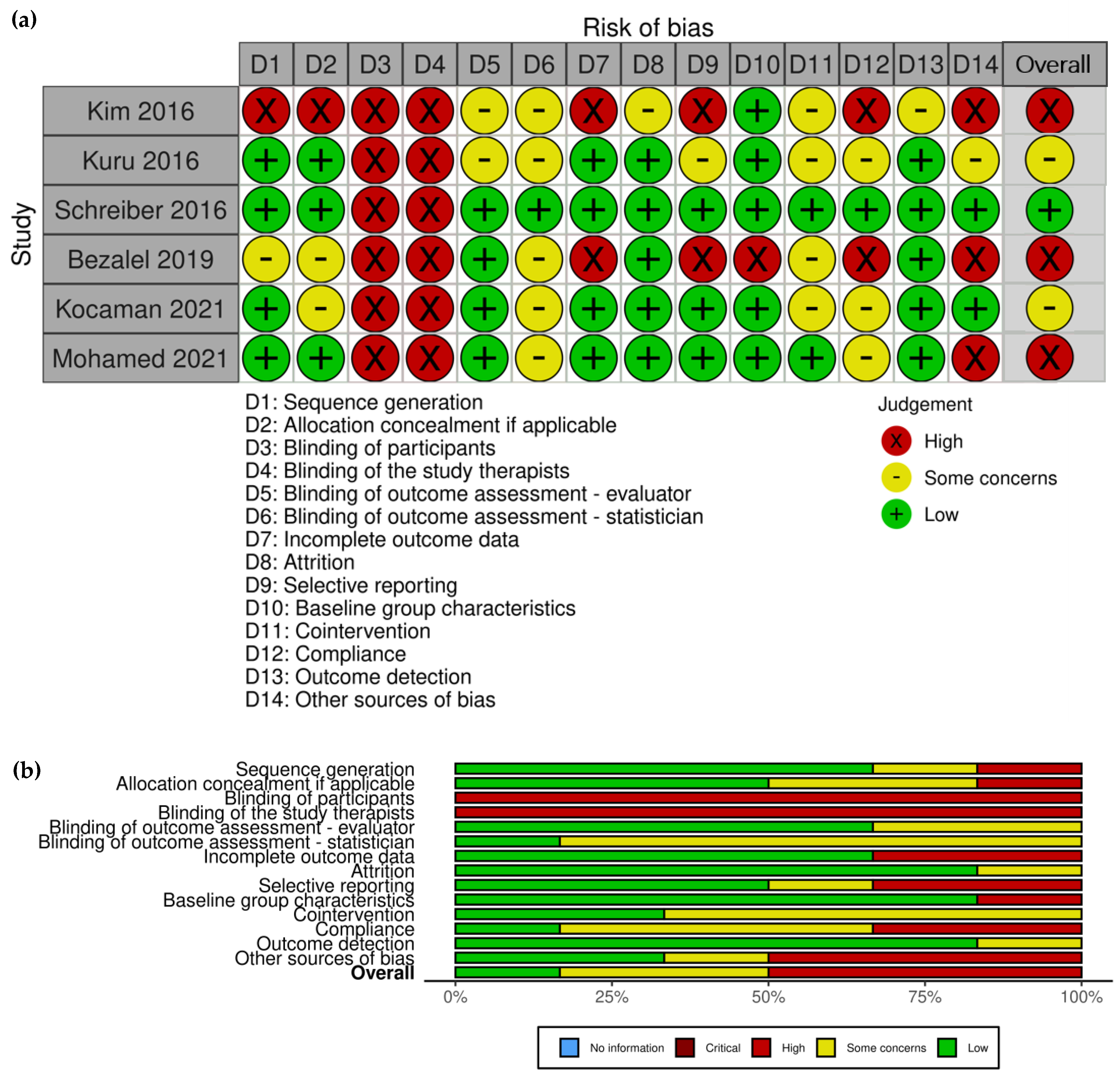
3.2. Risk of Bias Assessment
3.2.1. Risk of Bias of Included RCTs
3.2.2. Risk of Bias in Non-Randomized Studies (ROBINS) of Included NRSIs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weinstein, S.L.; Dolan, L.A.; Cheng, J.C.Y.; Danielsson, A.J.; Morcuende, J.A. Adolescent idiopathic scoliosis. Lancet 2008, 371, 1527–1537. [Google Scholar] [CrossRef] [Green Version]
- Miller, N.H. Cause and natural history of adolescent idiopathic scoliosis. Orthop. Clin. N. Am. 1999, 30, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Asher, M.A.; Burton, D.C. Adolescent idiopathic scoliosis: Natural history and long term treatment effects. Scoliosis 2006, 1, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, K.M.C.; Wang, T.; Qiu, G.X.; Luk, K.D.K. Recent advances in the aetiology of adolescent idiopathic scoliosis. Int. Orthop. 2008, 32, 729–734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konieczny, M.R.; Senyurt, H.; Krauspe, R. Epidemiology of adolescent idiopathic scoliosis. J. Child. Orthop. 2013, 7, 3–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kruse, L.M.; Buchan, J.G.; Gurnett, C.A.; Dobbs, M.B. Polygenic Threshold Model with Sex Dimorphism in Adolescent Idiopathic Scoliosis. J. Bone Jt. Surg. 2012, 94, 1485–1491. [Google Scholar] [CrossRef] [Green Version]
- Ueno, M.; Takaso, M.; Nakazawa, T.; Imura, T.; Saito, W.; Shintani, R.; Uchida, K.; Fukuda, M.; Takahashi, K.; Ohtori, S.; et al. A 5-year epidemiological study on the prevalence rate of idiopathic scoliosis in Tokyo: School screening of more than 250,000 children. J. Orthop. Sci. 2011, 16, 1–6. [Google Scholar] [CrossRef]
- Cheng, J.C.; Castelein, R.M.; Chu, W.C.; Danielsson, A.J.; Dobbs, M.B.; Grivas, T.B.; Gurnett, C.A.; Luk, K.D.; Moreau, A.; Newton, P.O.; et al. Adolescent idiopathic scoliosis. Nat. Rev. Dis. Prim. 2015, 1, 15030. [Google Scholar] [CrossRef] [Green Version]
- Danielsson, A.J.; Nachemson, A.L. Back pain and function 22 years after brace treatment for adolescent idiopathic scoliosis: A case-control study-part I. Spine 2003, 28, 2078–2085, discussion 2086. [Google Scholar] [CrossRef]
- Sato, T.; Hirano, T.; Ito, T.; Morita, O.; Kikuchi, R.; Endo, N.; Tanabe, N. Back pain in adolescents with idiopathic scoliosis: Epidemiological study for 43,630 pupils in Niigata City, Japan. Eur. Spine J. 2011, 20, 274–279. [Google Scholar] [CrossRef] [Green Version]
- Danielsson, A.J.; Nachemson, A.L. Childbearing, curve progression, and sexual function in women 22 years after treatment for adolescent idiopathic scoliosis: A case-control study. Spine 2001, 26, 1449–1456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tones, M.; Moss, N.; Polly, D.W. A review of quality of life and psychosocial issues in scoliosis. Spine 2006, 31, 3027–3038. [Google Scholar] [CrossRef] [PubMed]
- Rowe, D.E.; Bernstein, S.M.; Riddick, M.F.; Adler, F.; Emans, J.B.; Gardner-Bonneau, D. A meta-analysis of the efficacy of non-operative treatments for idiopathic scoliosis. J. Bone Jt. Surg. Am. Vol. 1997, 79, 664–674. [Google Scholar] [CrossRef] [PubMed]
- Boos, N.; Aebi, M. Spinal Disorders: Fundamentals of Diagnosis and Treatment; Boos, N., Aebi, M., Eds.; Springer: Berlin/Heidelberg, Germany, 2008. [Google Scholar]
- Smith, J.S.; Shaffrey, C.I.; Kuntz, C.; Mummaneni, P.V. Classification systems for adolescent and adult scoliosis. Neurosurgery 2008, 63 (Suppl. S3), 16–24. [Google Scholar] [CrossRef]
- Schwab, F.; Ungar, B.; Blondel, B.; Buchowski, J.; Coe, J.; Deinlein, D.; DeWald, C.; Mehdian, H.; Shaffrey, C.; Tribus, C.; et al. Scoliosis Research Society—Schwab Adult Spinal Deformity Classification: A Validation Study. Spine 2012, 37, 1077–1082. [Google Scholar] [CrossRef] [PubMed]
- Yelin, E.; Weinstein, S.; King, T. The burden of musculoskeletal diseases in the United States. Semin. Arthritis Rheu. 2016, 46, 259–260. [Google Scholar] [CrossRef] [PubMed]
- Schwab, F.; Farcy, J.P.; Bridwell, K.; Berven, S.; Glassman, S.; Harrast, J.; Horton, W. A Clinical Impact Classification of Scoliosis in the Adult. Spine 2006, 31, 2109–2114. [Google Scholar] [CrossRef]
- Schwab, F.; Dubey, A.; Gamez, L.; Fegoun, A.B.E.; Hwang, K.; Pagala, M.; Farcy, J.P. Adult Scoliosis & colon; Prevalence, SF-36, and Nutritional Parameters in an Elderly Volunteer Population. Spine 2005, 30, 1082–1085. [Google Scholar]
- Schwab, F.; Dubey, A.; Pagala, M.; Gamez, L.; Farcy, J.P. Adult Scoliosis: A Health Assessment Analysis by SF-36. Spine 2003, 28, 602–606. [Google Scholar] [CrossRef]
- Hallager, D.W.; Hansen, L.V.; Dragsted, C.R.; Peytz, N.; Gehrchen, M.; Dahl, B. A Comprehensive Analysis of the SRS-Schwab Adult Spinal Deformity Classification and Confounding Variables: A Prospective, Non-US Cross-sectional Study in 292 Patients. Spine 2016, 41, E589–E597. [Google Scholar] [CrossRef] [Green Version]
- Garrido, E.; Roberts, S.B.; Duckworth, A.; Fournier, J. Long-term follow-up of untreated Scheuermann’s kyphosis. Spine Deform. 2021, 9, 1633–1639. [Google Scholar] [CrossRef] [PubMed]
- Murray, P.M.; Weinstein, S.L.; Spratt, K.F. The natural history and long-term follow-up of Scheuermann kyphosis. J. Bone Jt. Surg. 1993, 75, 236–248. [Google Scholar] [CrossRef]
- Damborg, F.; Engell, V.; Andersen, M.O.; Kyvik, K.O.; Thomsen, K. There are only minor changes in quality of life in patients with Scheuermann’s disease. Dan. Med. J. 2014, 61, A4790. [Google Scholar] [PubMed]
- Martínez-Llorens, J.; Ramírez, M.; Colomina, M.J.; Bagó, J.; Molina, A.; Cáceres, E.; Gea, J. Muscle dysfunction and exercise limitation in adolescent idiopathic scoliosis. Eur. Respir. J. 2010, 36, 393–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bylund, P.; Jansson, E.; Dahlberg, E.; Eriksson, E. Muscle fiber types in thoracic erector spinae muscles. Fiber types in idiopathic and other forms of scoliosis. Clin. Orthop. Relat. Res. 1987, 214, 222–228. [Google Scholar] [CrossRef]
- Wang, W.J.; Yeung, H.Y.; Chu, W.C.W.; Tang, N.L.S.; Lee, K.M.; Qiu, Y.; Burwell, R.G.; Cheng, J.C.Y. Top theories for the etiopathogenesis of adolescent idiopathic scoliosis. J. Pediatr. Orthop. 2011, 31 (Suppl. S1), S14–S27. [Google Scholar] [CrossRef]
- Burwell, R. Etiology of Adolescent Idiopathic Scoliosis: Current Trends and Relevance to New Treatment Approaches; Hanley & Belfus: Philadelphia, PA, USA, 2000. [Google Scholar]
- Hall, C.M.; Brody, L.T. Therapeutic Exercise Moving toward Function, 2nd ed.; Lippincott Williams Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- Stokes, I.A.F. Analysis and simulation of progressive adolescent scoliosis by biomechanical growth modulation. Eur. Spine J. 2007, 16, 1621–1628. [Google Scholar] [CrossRef]
- Stokes, I.; Gardner-Morse, M. The role of muscles and effects of load on growth. Stud Health Technol Inform. 2002, 91, 314–317. [Google Scholar]
- Stokes, I.A.; Burwell, R.G.; Dangerfield, P.H. Biomechanical spinal growth modulation and progressive adolescent scoliosis—A test of the “vicious cycle” pathogenetic hypothesis: Summary of an electronic focus group debate of the IBSE. Scoliosis Spinal Disord. 2006, 1, 1. [Google Scholar] [CrossRef] [Green Version]
- Stokes, I.A.F. Mechanical modulation of spinal growth and progression of adolescent scoliosis. Stud. Health Technol. Inform. 2008, 135, 75–83. [Google Scholar]
- Hawes, M. The transformation of spinal curvature into spinal deformity: Pathological processes and implications for treatment. Scoliosis 2006, 1, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stokes, I.A.F.; Gardner-Morse, M. Muscle activation strategies and symmetry of spinal loading in the lumbar spine with scoliosis. Spine 2004, 29, 2103–2107. [Google Scholar] [CrossRef] [Green Version]
- Fusco, C.; Zaina, F.; Atanasio, S.; Romano, M.; Negrini, A.; Negrini, S. Physical exercises in the treatment of adolescent idiopathic scoliosis: An updated systematic review. Physiother. Theory Pract. 2011, 27, 80–114. [Google Scholar] [CrossRef]
- Negrini, S.; Atanasio, S.; Fusco, C.; Zaina, F. Effectiveness of complete conservative treatment for adolescent idiopathic scoliosis (bracing and exercises) based on SOSORT management criteria: Results according to the SRS criteria for bracing studies—SOSORT Award 2009 Winner. Scoliosis 2009, 4, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotwicki, T.; Negrini, S.; Grivas, T.B.; Rigo, M.; Maruyama, T.; Durmala, J.; Zaina, F.; SOSORT. Methodology of evaluation of morphology of the spine and the trunk in idiopathic scoliosis and other spinal deformities—6th SOSORT consensus paper. Scoliosis 2009, 4, 26. [Google Scholar] [CrossRef] [Green Version]
- Scoliosis Research Society. Adolescent Idiopathic Scoliosis. 2016. Available online: http://www.srs.org/patients-and-families/conditions-and-treatments/parents/scoliosis/adolescent-idiopathic-scoliosis (accessed on 30 January 2023).
- Bagnall, K.M.; Grivas, T.B.; Alos, N.; Asher, M.; Aubin, C.E.; Burwell, G.R.; Dangerfield, P.H.; Edouard, T.; Hill, D.; Lou, E.; et al. The International Research Society of Spinal Deformities (IRSSD) and its contribution to science. Scoliosis 2009, 4, 28. [Google Scholar] [CrossRef] [Green Version]
- Lehnert-Schroth, C. Three-Dimensional Treatment for Scoliosis, 7th ed.; The Martindale Press: Palo Alto, CA, USA, 2007. [Google Scholar]
- Stokes, I.A.F.; Sangole, A.P.; Aubin, C.E. Classification of scoliosis deformity three-dimensional spinal shape by cluster analysis. Spine 2009, 34, 584–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poncet, P.; Dansereau, J.; Labelle, H. Geometric torsion in idiopathic scoliosis: Three-dimensional analysis and proposal for a new classification. Spine 2001, 26, 2235–2243. [Google Scholar] [CrossRef]
- Kuklo, T.R.; Potter, B.K.; Lenke, L.G. Vertebral rotation and thoracic torsion in adolescent idiopathic scoliosis: What is the best radiographic correlate? J. Spinal Disord. Tech. 2005, 18, 139–147. [Google Scholar] [CrossRef]
- Aronsson, D.D.; Stokes, I.A. Nonfusion treatment of adolescent idiopathic scoliosis by growth modulation and remodeling. J. Pediatr. Orthop. 2011, 31 (Suppl. S1), S99–S106. [Google Scholar] [CrossRef] [Green Version]
- Diebo, B.G.; Shah, N.V.; Boachie-Adjei, O.; Zhu, F.; Rothenfluh, D.A.; Paulino, C.B.; Schwab, F.J.; Lafage, V. Adult spinal deformity. Lancet 2019, 394, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.S.; Shaffrey, C.I.; Ames, C.P.; Lenke, L.G. Treatment of adult thoracolumbar spinal deformity: Past, present, and future. J. Neurosurg. Spine 2019, 30, 551–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hennes, A. International Schroth 3D Scoliosis Therapy According to Katharina Schroth—Training Manual Part I; ISST—Training Institute: Bad Sobernheim, Germany, 2023; p. 63. [Google Scholar]
- Hennes, A. International Schroth 3D Scoliosis Therapy According to Katharina Schroth—Training Manual Part II; ISST—Training Institute Germany: Bad Sobernheim, Germany, 2023; p. 104. [Google Scholar]
- Schreiber, S.; Parent, E.C.; Moez, E.K.; Hedden, D.M.; Hill, D.; Moreau, M.J.; Lou, E.; Watkins, E.M.; Southon, S.C. The effect of Schroth exercises added to the standard of care on the quality of life and muscle endurance in adolescents with idiopathic scoliosis-an assessor and statistician blinded randomized controlled trial: “SOSORT 2015 Award Winner”. Scoliosis 2015, 10, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuru, T.; Yeldan, İ.; Dereli, E.E.; Özdinçler, A.R.; Dikici, F.; Çolak, İ. The efficacy of three-dimensional Schroth exercises in adolescent idiopathic scoliosis: A randomised controlled clinical trial. Clin. Rehabil. 2016, 30, 181–190. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Furlan, A.D.; Malmivaara, A.; Chou, R.; Maher, C.G.; Deyo, R.A.; Schoene, M.; Bronfort, G.; Tulder, M.W.V. 2015 Updated Method Guideline for Systematic Reviews in the Cochrane Back and Neck Group. Spine 2015, 40, 1660–1673. [Google Scholar] [CrossRef]
- McGuinness, L.A. Risk of Bias Plots. In: Doing Meta-Analysis with R: A Hands-On Guide (Online Version) [Internet]. 2021. Available online: https://bookdown.org/MathiasHarrer/Doing_Meta_Analysis_in_R/risk-of-bias-plots.html (accessed on 28 December 2022).
- Negrini, S.; Hresko, T.M.; O’Brien, J.P.; Price, N. Recommendations for research studies on treatment of idiopathic scoliosis: Consensus 2014 between SOSORT and SRS non–operative management committee. Scoliosis 2015, 10, 8. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 Explanation and Elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c869. [Google Scholar] [CrossRef] [Green Version]
- Altman, D.G.; Schulz, K.F.; Moher, D.; Egger, M.; Davidoff, F.; Elbourne, D.; Gøtzsche, P.C.; Lang, T. The Revised CONSORT Statement for Reporting Randomized Trials: Explanation and Elaboration. Ann. Intern. Med. 2001, 134, 663–694. [Google Scholar] [CrossRef]
- Boutron, I.; Moher, D.; Altman, D.G.; Schulz, K.F.; Ravaud, P.; Group, C. Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: Explanation and elaboration. Ann. Intern. Med. 2008, 148, 295–309. [Google Scholar] [CrossRef] [PubMed]
- Bezalel, T.; Carmeli, E.; Levi, D.; Kalichman, L. The Effect of Schroth Therapy on Thoracic Kyphotic Curve and Quality of Life in Scheuermann’s Patients: A Randomized Controlled Trial. Asian Spine J. 2019, 13, 490–499. [Google Scholar] [CrossRef] [Green Version]
- Schreiber, S.; Parent, E.C.; Moez, E.K.; Hedden, D.M.; Hill, D.L.; Moreau, M.; Lou, E.; Watkins, E.M.; Southon, S.C. Schroth Physiotherapeutic Scoliosis-Specific Exercises Added to the Standard of Care Lead to Better Cobb Angle Outcomes in Adolescents with Idiopathic Scoliosis—An Assessor and Statistician Blinded Randomized Controlled Trial. PLoS ONE 2016, 11, e0168746. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.; HwangBo, P.N. Effects of Schroth and Pilates exercises on the Cobb angle and weight distribution of patients with scoliosis. J. Phys. Ther. Sci. 2016, 28, 1012–1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohamed, R.A.; Yousef, A.M. Impact of Schroth three-dimensional vs. proprioceptive neuromuscular facilitation techniques in adolescent idiopathic scoliosis: A randomized controlled study. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 7717–7725. [Google Scholar]
- Zapata, K.A.; Sucato, D.J.; Jo, C.H. Physical Therapy Scoliosis-Specific Exercises May Reduce Curve Progression in Mild Adolescent Idiopathic Scoliosis Curves. Pediatr. Phys. Ther. 2019, 31, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Kocaman, H.; Bek, N.; Kaya, M.H.; Büyükturan, B.; Yetiş, M.; Büyükturan, Ö. The effectiveness of two different exercise approaches in adolescent idiopathic scoliosis: A single-blind, randomized-controlled trial. PLoS ONE 2021, 16, e0249492. [Google Scholar] [CrossRef]
- Richards, B.S.; Bernstein, R.M.; D’Amato, C.R.; Thompson, G.H. Standardization of criteria for adolescent idiopathic scoliosis brace studies: SRS Committee on Bracing and Nonoperative Management. Spine 2005, 30, 2068–2075, discussion 2076-7. [Google Scholar] [CrossRef] [Green Version]
- Kleuver M de Faraj, S.S.A.; Holewijn, R.M.; Germscheid, N.M.; Adobor, R.D.; Andersen, M.; Tropp, H.; Dahl, B.; Keskinen, H.; Olai, A.; Polly, D.W.; et al. Defining a core outcome set for adolescent and young adult patients with a spinal deformity. Acta Orthop. 2017, 88, 612–618. [Google Scholar] [CrossRef] [Green Version]
- Parent, E.C.; Vaclavik, M.; Bourgoin, C.; Hebert, C.; Bouwmeester, M.; Cheslock, S.; Collins, R.; Potgieter, S.; Coles, M.; Schreiber, S.; et al. Inventory of Patient-Reported Outcome Measures Used in the Non-Operative Care of Scoliosis: A Scoping Review. Children 2023, 10, 239. [Google Scholar] [CrossRef]
- Close, C.; Wisener, L.-G.; Toner, P. Development of a Person-Centred Core Outcome Set for Adolescents and Young Adults with Spinal Deformity Undergoing Surgery: Creation of a Meaningful Long List of Candidate Outcome Domains (SPINE-COS-AYA) [Internet]. 2021. Available online: https://osf.io/h4qas/ (accessed on 24 March 2023).
- Lenke, L.G.; Betz, R.R.; Harms, J.; Bridwell, K.H.; Clements, D.H.; Lowe, T.G.; Blanke, K. Adolescent idiopathic scoliosis: A new classification to determine extent of spinal arthrodesis. J. Bone Jt. Surg. Am. 2001, 83, 1169–1181. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schreiber, S.; Whibley, D.; Somers, E.C. Schroth Physiotherapeutic Scoliosis-Specific Exercise (PSSE) Trials—Systematic Review of Methods and Recommendations for Future Research. Children 2023, 10, 954. https://doi.org/10.3390/children10060954
Schreiber S, Whibley D, Somers EC. Schroth Physiotherapeutic Scoliosis-Specific Exercise (PSSE) Trials—Systematic Review of Methods and Recommendations for Future Research. Children. 2023; 10(6):954. https://doi.org/10.3390/children10060954
Chicago/Turabian StyleSchreiber, Sanja, Daniel Whibley, and Emily C Somers. 2023. "Schroth Physiotherapeutic Scoliosis-Specific Exercise (PSSE) Trials—Systematic Review of Methods and Recommendations for Future Research" Children 10, no. 6: 954. https://doi.org/10.3390/children10060954