
Effects of Combined Movement and Storytelling Intervention on Fundamental Motor Skills, Language Development and Physical Activity Level in Children Aged 3 to 6 Years: Study Protocol for a Randomized Controlled Trial

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Material and Methods
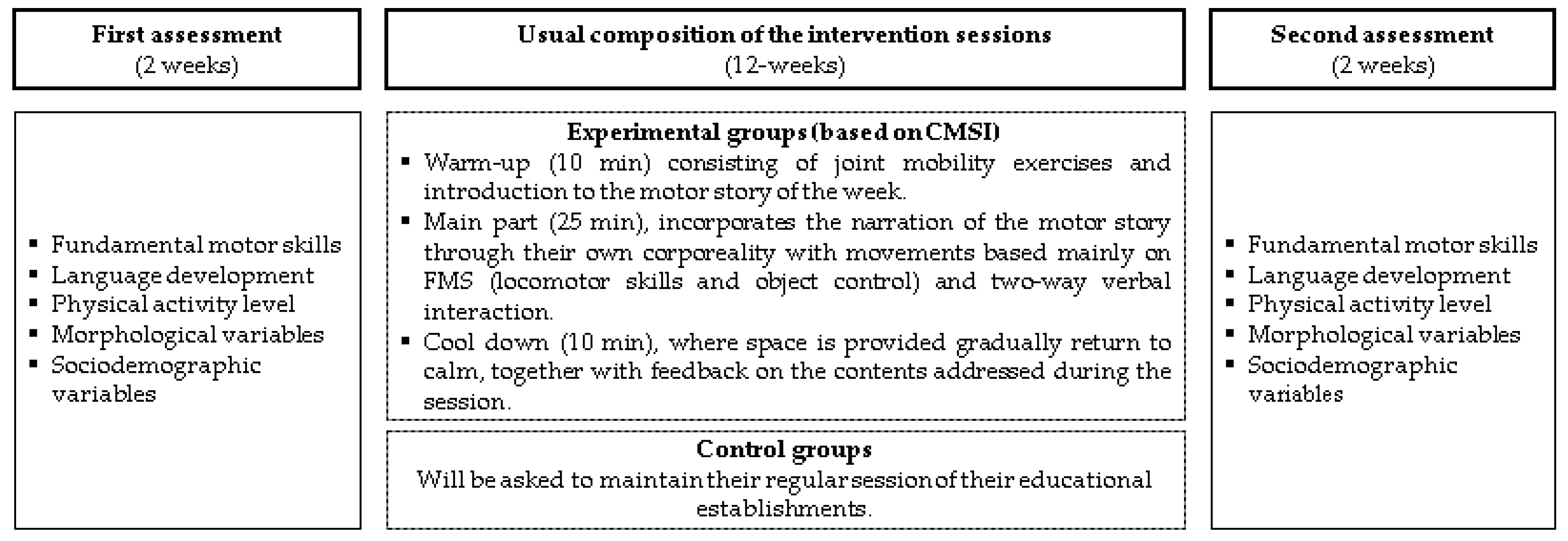
2.1. Study Design
2.2. Ethical Approval
2.3. Sample Size Calculation
2.4. Randomization and Blinding
2.5. Participants
2.6. Intervention
2.7. Control Groups
2.8. Outcomes and Procedures
2.9. Primary Outcomes
2.9.1. Fundamental Motor Skills (FMSs)
2.9.2. Language Development
2.9.3. Physical Activity Level
2.10. Secondary Outcomes
2.10.1. Morphological Variables
2.10.2. Sociodemographic Variables
2.11. Statistical Analysis
2.12. Intention-to-Treat Analysis
2.13. Analysis by Protocol
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Willumsen, J.; Bull, F. Development of WHO Guidelines on Physical Activity, Sedentary Behavior, and Sleep for Children Less Than 5 Years of Age. J. Phys. Act. Health 2020, 17, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- den Uil, A.R.; Janssen, M.; Busch, V.; Kat, I.T.; Scholte, R.H.J. The relationships between children’s motor competence, physical activity, perceived motor competence, physical fitness and weight status in relation to age. PLoS ONE 2023, 18, e0278438. [Google Scholar] [CrossRef]
- Ma, F.-F.; Luo, D.-M. Relationships between physical activity, fundamental motor skills, and body mass index in preschool children. Front. Public Health 2023, 11, 1094168. [Google Scholar] [CrossRef]
- Duncan, M.J.; Hall, C.; Eyre, E.; Barnett, L.M.; James, R.S. Pre-schoolers fundamental movement skills predict BMI, physical activity, and sedentary behavior: A longitudinal study. Scand. J. Med. Sci. Sports 2021, 31 (Suppl. 1), 8–14. [Google Scholar] [CrossRef] [PubMed]
- Webster, E.K.; Sur, I.; Stevens, A.; Robinson, L.E. Associations between body composition and fundamental motor skill competency in children. BMC Pediatr. 2021, 21, 444. [Google Scholar] [CrossRef]
- Bolger, L.E.; Bolger, L.A.; O’Neill, C.; Coughlan, E.; O’Brien, W.; Lacey, S.; Burns, C.; Bardid, F. Global levels of fundamental motor skills in children: A systematic review. J. Sports Sci. 2021, 39, 717–753. [Google Scholar] [CrossRef]
- Mulé, D.; Jeger, I.; Dötsch, J.; Breido, F.; Ferrari, N.; Joisten, C. Correlation between Language Development and Motor Skills, Physical Activity, and Leisure Time Behaviour in Preschool-Aged Children. Children 2022, 9, 431. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.V.; Lekhal, R.; Aaro, L.E.; Holte, A.; Schjolberg, S. The developmental relationship between language and motor performance from 3 to 5 years of age: A prospective longitudinal population study. BMC Psychol. 2014, 2, 34. [Google Scholar] [CrossRef]
- Lin, J.; Zhang, R.; Shen, J.; Zhou, A. Effects of school-based neuromuscular training on fundamental movement skills and physical fitness in children: A systematic review. PeerJ 2022, 10, e13726. [Google Scholar] [CrossRef]
- Van Capelle, A.; Broderick, C.R.; van Doorn, N.; Ward, R.E.; Parmenter, B.J. Interventions to improve fundamental motor skills in pre-school aged children: A systematic review and meta-analysis. J. Sci. Med. Sports 2017, 20, 658–666. [Google Scholar] [CrossRef]
- Han, X.; Zhao, M.; Kong, Z.; Xie, J. Association between fundamental motor skills and executive function in preschool children: A cross-sectional study. Front. Psychol. 2022, 13, 978994. [Google Scholar] [CrossRef]
- Jylänki, P.; Mbay, T.; Hakkarainen, A.; Sääkslahti, A.; Aunio, P. The effects of motor skill and physical activity interventions on preschoolers’ cognitive and academic skills: A systematic review. Prev. Med. 2022, 155, 106948. [Google Scholar] [CrossRef]
- Duncan, M.; Cunningham, A.; Eyre, E. A combined movement and story-telling intervention enhances motor competence and language ability in pre-schoolers to a greater extent than movement or story-telling alone. Eur. Phys. Educ. Rev. 2019, 25, 221–235. [Google Scholar] [CrossRef]
- Eyre, E.L.J.; Clark, C.C.T.; Tallis, J.; Hodson, D.; Lowton-Smith, S.; Nelson, C.; Noon, M.; Duncan, M.J. The Effects of Combined Movement and Storytelling Intervention on Motor Skills in South Asian and White Children Aged 5–6 Years Living in the United Kingdom. Int. J. Environ. Res. Public Health 2020, 17, 3391. [Google Scholar] [CrossRef]
- Kline, R. Becoming a Behavioral Science Researcher: A Guide to Producing Research That Matters, 2nd ed.; Wiley: Hoboken, NJ, USA, 2020. [Google Scholar]
- Turner, L.; Shamseer, L.; Altman, D.G.; Weeks, L.; Peters, J.; Kober, T.; Dias, S.; Schulz, K.F.; Plint, A.C.; Moher, D. Consolidated standards of reporting trials (CONSORT) and the completeness of reporting of randomised controlled trials (RCTs) published in medical journals. Cochrane Database Syst. Rev. 2012, 11, Mr000030. [Google Scholar] [CrossRef]
- Parker, K.; Nunns, M.P.; Xiao, Z.; Ford, T.; Ukoumunne, O.C. Characteristics and practices of school-based cluster randomised controlled trials for improving health outcomes in pupils in the UK: A systematic review protocol. BMJ Open 2021, 11, e044143. [Google Scholar] [CrossRef]
- Spybrook, J.; Zhang, Q.; Kelcey, B.; Dong, N. Learning from Cluster Randomized Trials in Education: An Assessment of the Capacity of Studies to Determine What Works, For Whom, and Under What Conditions. Educ. Eval. Policy Anal. 2020, 42, 354–374. [Google Scholar] [CrossRef]
- Chilean Ministry of Education. Diversificacion de la Enseñanza; Ministerio de Educación: Santiago, Chile, 2015.
- Vargas Vitoria, R.; Carrasco Sánchez, L. El Cuento motor y su incidencia en la educación por el movimiento. Pensam. Educ. Rev. Investig. Latinoam. 2006, 38, 108–124. [Google Scholar]
- Conde, J.L. Cuentos Motores, 3rd ed.; Paidotribo, Ed.; Paidotribo: Madrid, Spain, 2008. [Google Scholar]
- Manacero, S.; Nunes, M.L. Longitudinal study of sleep behavior and motor development in low-birth-weight preterm children from infancy to preschool years. J. Pediatr. 2021, 97, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, D. Test of Gross Motor Development-2; Patrones básicos; Alianza: Madrid, Spain, 2000. [Google Scholar]
- Cano-Cappellacci, M.; Leyton, F.A.; Carreño, J.D. Content validity and reliability of test of gross motor development in Chilean children. Rev. Saude Publica 2015, 49, s0034–s8910. [Google Scholar] [CrossRef] [PubMed]
- Pavez-Adasme, G.; Hernández-Mosqueira, C.; Urrutia, S.; Iturra, M.; Palavecino, C.; Bobadilla, M.; Torres, M.; Gómez-Alvarez, N. Test de desarrollo motor aplicados en Chile entre el período 2014–2018. Una revisión sistemática. Rev. Cienc. Act. Física 2020, 21, 1–13. [Google Scholar] [CrossRef]
- Valentini, N.C. Validity and reliability of the TGMD-2 for Brazilian children. J. Mot. Behav. 2012, 44, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kim, M.J.; Valentini, N.C.; Clark, J.E. Validity and reliability of the TGMD-2 for South Korean children. J. Mot. Behav. 2014, 46, 351–356. [Google Scholar] [CrossRef]
- Pinto-Guevara, A.; Chamorro-Oschilewsky, R. Prueba de Desarrollo del Lenguaje para Pre-Escolares Telepre, 1st ed.; Universidad Católica del Maule, Ed.; Universidad Católica del Maule: Talca, Chile, 2009. [Google Scholar]
- Estivaleti, J.M.O.; Bergamo, R.R.; Oliveira, L.C.; Beltran, D.C.G.; Silva Junior, J.P.D.; Santos, M.D.; Matsudo, V.K.R. Physical activity level measured by accelerometry and physical fitness of schoolchildren. Rev. Paul. Pediatr. 2022, 41, e2021230. [Google Scholar] [CrossRef]
- Lettink, A.; Altenburg, T.M.; Arts, J.; van Hees, V.T.; Chinapaw, M.J. Systematic review of accelerometer-based methods for 24-h physical behavior assessment in young children (0–5 years old). Int. J. Behav. Nutr. Phys. Act. 2022, 19, 116. [Google Scholar] [CrossRef]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nyström, C.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef]
- Marfell-Jones, M.J.; Stewart, A.; de Ridder, J.H. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Wellington, New Zeland, 2012. [Google Scholar]
- Kuzik, N.; Naylor, P.J.; Spence, J.C.; Carson, V. Movement behaviours and physical, cognitive, and social-emotional development in preschool-aged children: Cross-sectional associations using compositional analyses. PLoS ONE 2020, 15, e0237945. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing (4.1.1). R Foundation for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 1 August 2023).
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Robinson, L.E.; Stodden, D.F.; Barnett, L.M.; Lopes, V.P.; Logan, S.W.; Rodrigues, L.P.; D’Hondt, E. Motor Competence and its Effect on Positive Developmental Trajectories of Health. Sports Med. 2015, 45, 1273–1284. [Google Scholar] [CrossRef]
- Logan, S.W.; Ross, S.M.; Chee, K.; Stodden, D.F.; Robinson, L.E. Fundamental motor skills: A systematic review of terminology. J. Sports Sci. 2018, 36, 781–796. [Google Scholar] [CrossRef] [PubMed]
- Lyster, S.H.; Lervåg, A.O.; Hulme, C. Preschool morphological training produces long-term improvements in reading comprehension. Read. Writ. 2016, 29, 1269–1288. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, L.; Souza, V.d.F.M.d.; Rocha, F.F.d.; Silva, P.N.d.; Cheuczuk, F.; Vieira, J.L.L. Relação entre o perfil sociodemográfico e a competência motora de crianças. Cad. Bras. Ter. Ocup. 2023, 31, e3201. [Google Scholar]


{kind=link}
{kind=link}
| Motor Story | Materials | Warm-Up (5 min) | Main Part (25 min) | Cool Down (10 min) |
|---|---|---|---|---|
| Week 1: Who I am | Chairs, hoops, balls, mats, pencils, erasers and masking tape | Joint mobility exercises 1 and introduction to motor story | Locomotion skills 2 and verbal interaction 4 | Return to calm 5 and feedback from the motor story |
| Week 2: We go on an excursion | Mats, chairs and rope | Notion and body image, and dynamic balance | ||
| Week 3: The school | Mats, chairs, hula hoops and voice | Notion and body image, dynamic balance and visuomotor coordination | ||
| Week 4: The recess | Mats, materials available in the patio or classroom | Dynamic balance, object control 3 and free play | ||
| Week 5: The weekend has arrived | Music, blanket, mats, hoops, balls and newsprint | Object control 3 and verbal interaction 4 | ||
| Week 6: Visiting the park | Games found in the kindergarten playground and hula hoops | Dynamic balance, tone control, eye–motor coordination and object control 3 | ||
| Week 7: My days in the field | Lentil cones, and ping pong balls from reused paper | Dynamic balance, eye–motor coordination and free play | ||
| Week 8: My days at the beach | Relaxing music, speaker and elements in hand | Sensorimotor, dynamic balance and visuomotor coordination | ||
| Week 9: We go to the stadium | Exercise machines, speaker, relaxing music and relaxation audio | Dynamic balance, eye–motor coordination and free play | ||
| Week 10: We are going to know my environment | Ball, relaxing music, speaker and voice | Dynamic balance and eye–motor coordination | ||
| Week 11: Let’s go to the circus | Balls, ropes, mats and bottles | Locomotion skills 2, object control 3 and verbal interaction 4 | ||
| Week 12: Tell me your adventures | Speaker, relaxation music, sock balls and other materials available | Dynamic balance, eye–motor coordination and tone control |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vargas-Vitoria, R.; Faúndez-Casanova, C.; Cruz-Flores, A.; Hernandez-Martinez, J.; Jarpa-Preisler, S.; Villar-Cavieres, N.; González-Muzzio, M.T.; Garrido-González, L.; Flández-Valderrama, J.; Valdés-Badilla, P. Effects of Combined Movement and Storytelling Intervention on Fundamental Motor Skills, Language Development and Physical Activity Level in Children Aged 3 to 6 Years: Study Protocol for a Randomized Controlled Trial. Children 2023, 10, 1530. https://doi.org/10.3390/children10091530
Vargas-Vitoria R, Faúndez-Casanova C, Cruz-Flores A, Hernandez-Martinez J, Jarpa-Preisler S, Villar-Cavieres N, González-Muzzio MT, Garrido-González L, Flández-Valderrama J, Valdés-Badilla P. Effects of Combined Movement and Storytelling Intervention on Fundamental Motor Skills, Language Development and Physical Activity Level in Children Aged 3 to 6 Years: Study Protocol for a Randomized Controlled Trial. Children. 2023; 10(9):1530. https://doi.org/10.3390/children10091530
Chicago/Turabian StyleVargas-Vitoria, Rodrigo, César Faúndez-Casanova, Alberto Cruz-Flores, Jordan Hernandez-Martinez, Stefany Jarpa-Preisler, Natalia Villar-Cavieres, María Teresa González-Muzzio, Lorena Garrido-González, Jorge Flández-Valderrama, and Pablo Valdés-Badilla. 2023. "Effects of Combined Movement and Storytelling Intervention on Fundamental Motor Skills, Language Development and Physical Activity Level in Children Aged 3 to 6 Years: Study Protocol for a Randomized Controlled Trial" Children 10, no. 9: 1530. https://doi.org/10.3390/children10091530
APA StyleVargas-Vitoria, R., Faúndez-Casanova, C., Cruz-Flores, A., Hernandez-Martinez, J., Jarpa-Preisler, S., Villar-Cavieres, N., González-Muzzio, M. T., Garrido-González, L., Flández-Valderrama, J., & Valdés-Badilla, P. (2023). Effects of Combined Movement and Storytelling Intervention on Fundamental Motor Skills, Language Development and Physical Activity Level in Children Aged 3 to 6 Years: Study Protocol for a Randomized Controlled Trial. Children, 10(9), 1530. https://doi.org/10.3390/children10091530