
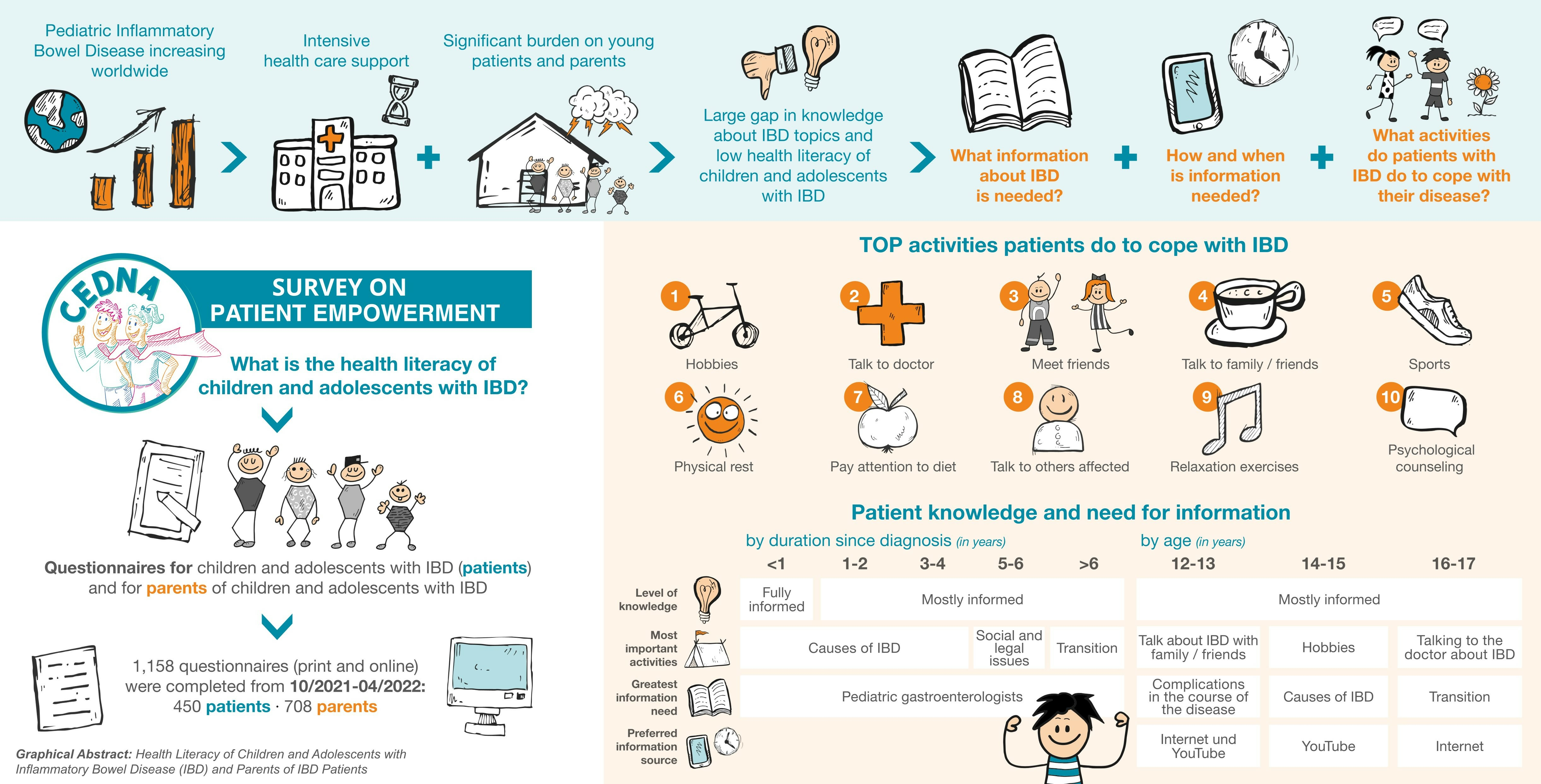
Health Literacy of Children and Adolescents with Inflammatory Bowel Disease (IBD) and Parents of IBD Patients—Coping and Information Needs

 , and
, and
Abstract
:
1. Introduction
2. Methods
2.1. Data Basis
2.2. Presentation of Results
3. Results
3.1. General Information about Patients and Their Disease
3.2. Main Contacts for Patients and Parents
3.3. Activities to Cope with Disease
3.4. Information Needs of Patients and Parents on IBD Topics
3.5. Preferred Sources of Information
3.6. Provision of Information about IBD
3.7. Preferred Timing of Relevant Information at Different Stages of the Illness
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alatab, S.; Sepanlou, S.G.; Ikuta, K.; Vahedi, H.; Bisignano, C.; Safiri, S.; Sadeghi, A.; Nixon, M.R.; Abdoli, A.; Abolhassani, H.; et al. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.; Kuenzig, M.E.; Benchimol, E.I. Epidemiology of Pediatric Inflammatory Bowel Disease. Gastroenterol. Clin. N. Am. 2023, 52, 483–496. [Google Scholar] [CrossRef] [PubMed]
- Coward, S.; Benchimol, E.I.; Kuenzig, M.E.; Windsor, J.W.; Bernstein, C.N.; Bitton, A.; Jones, J.L.; Lee, K.; Murthy, S.K.; Targownik, L.E.; et al. The 2023 Impact of Inflammatory Bowel Disease in Canada: Epidemiology of IBD. J. Can. Assoc. Gastroenterol. 2023, 6, S9–S15. [Google Scholar] [CrossRef] [PubMed]
- Kuenzig, M.E.; Fung, S.G.; Marderfeld, L.; Mak, J.W.Y.; Kaplan, G.G.; Ng, S.C.; Wilson, D.C.; Cameron, F.; Henderson, P.; Kotze, P.G.; et al. Twenty-first Century Trends in the Global Epidemiology of Pediatric-Onset Inflammatory Bowel Disease: Systematic Review. Gastroenterology 2022, 162, 1147–1159.e4. [Google Scholar] [CrossRef] [PubMed]
- Wittig, R.; Albers, L.; Koletzko, S.; Saam, J.; Kries, R. von. Pediatric Chronic Inflammatory Bowel Disease in a German Statutory Health INSURANCE-Incidence Rates From 2009 to 2012. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Bouhuys, M.; Lexmond, W.S.; van Rheenen, P.F. Pediatric Inflammatory Bowel Disease. Pediatrics 2023, 151, 3204. [Google Scholar] [CrossRef] [PubMed]
- Brooks, A.J.; Norman, P.; Peach, E.J.; Ryder, A.; Scott, A.J.; Narula, P.; Corfe, B.M.; Lobo, A.J.; Rowse, G. Prospective Study of Psychological Morbidity and Illness Perceptions in Young People with Inflammatory Bowel Disease. J. Crohn’s Colitis 2019, 13, 1003–1011. [Google Scholar] [CrossRef] [PubMed]
- McCartney, S.; Lindsay, J.O.; Russell, R.K.; Gaya, D.R.; Shaw, I.; Murray, C.D.; Finney-Hayward, T.; Sebastian, S. Benefits of Structured Pediatric to Adult Transition in Inflammatory Bowel Disease: The TRANSIT Observational Study. J. Pediatr. Gastroenterol. Nutr. 2022, 74, 208–214. [Google Scholar] [CrossRef] [PubMed]
- van Tilburg, M.A.L.; Claar, R.L.; Romano, J.M.; Langer, S.L.; Drossman, D.A.; Whitehead, W.E.; Abdullah, B.; Levy, R.L. Psychological Factors May Play an Important Role in Pediatric Crohn’s Disease Symptoms and Disability. J. Pediatr. 2017, 184, 94–100.e1. [Google Scholar] [CrossRef]
- Gamwell, K.L.; Baudino, M.N.; Bakula, D.M.; Sharkey, C.M.; Roberts, C.M.; Grunow, J.E.; Jacobs, N.J.; Gillaspy, S.R.; Mullins, L.L.; Chaney, J.M. Perceived Illness Stigma, Thwarted Belongingness, and Depressive Symptoms in Youth With Inflammatory Bowel Disease (IBD). Inflamm. Bowel Dis. 2018, 24, 960–965. [Google Scholar] [CrossRef]
- Tempchin, J.; Storch, B.; Reigada, L.C. Systematic review: Psychosocial factors of resilience in young people with inflammatory bowel disease. J. Psychosom. Res. 2021, 148, 110558. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.M.; Gamwell, K.L.; Baudino, M.N.; Grunow, J.E.; Jacobs, N.J.; Tung, J.; Gillaspy, S.R.; Hommel, K.A.; Mullins, L.L.; Chaney, J.M. The Contributions of Illness Stigma, Health Communication Difficulties, and Thwarted Belongingness to Depressive Symptoms in Youth with Inflammatory Bowel Disease. J. Pediatr. Psychol. 2020, 45, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Riemann, L.; Lubasch, J.S.; Heep, A.; Ansmann, L. The Role of Health Literacy in Health Behavior, Health Service Use, Health Outcomes, and Empowerment in Pediatric Patients with Chronic Disease: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 12464. [Google Scholar] [CrossRef] [PubMed]
- Brooks, A.J.; Rowse, G.; Ryder, A.; Peach, E.J.; Corfe, B.M.; Lobo, A.J. Systematic review: Psychological morbidity in young people with inflammatory bowel disease—Risk factors and impacts. Aliment. Pharmacol. Ther. 2016, 44, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, G. Health literacy: Ways to maximise the impact and effectiveness of vaccination information. Hum. Vaccin. Immunother. 2014, 10, 2130–2135. [Google Scholar] [CrossRef] [PubMed]
- Nutbeam, D.; Muscat, D.M. Health Promotion Glossary 2021. Health Promot. Int. 2021, 36, 1578–1598. [Google Scholar] [CrossRef] [PubMed]
- Dray, J.; Bowman, J.; Campbell, E.; Freund, M.; Wolfenden, L.; Hodder, R.K.; McElwaine, K.; Tremain, D.; Bartlem, K.; Bailey, J.; et al. Systematic Review of Universal Resilience-Focused Interventions Targeting Child and Adolescent Mental Health in the School Setting. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 813–824. [Google Scholar] [CrossRef] [PubMed]
- Lambrinou, E.; Hansen, T.B.; Beulens, J.W. Lifestyle factors, self-management and patient empowerment in diabetes care. Eur. J. Prev. Cardiol. 2019, 26, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Ausili, D.; Barbaranelli, C.; Rossi, E.; Rebora, P.; Fabrizi, D.; Coghi, C.; Luciani, M.; Vellone, E.; Di Mauro, S.; Riegel, B. Development and psychometric testing of a theory-based tool to measure self-care in diabetes patients: The Self-Care of Diabetes Inventory. BMC Endocr. Disord. 2017, 17, 66. [Google Scholar] [CrossRef]
- Lozano, P.; Houtrow, A. Supporting Self-Management in Children and Adolescents With Complex Chronic Conditions. Pediatrics 2018, 141, S233–S241. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Li, P.K.T.; Tantisattamo, E.; Kumaraswami, L.; Liakopoulos, V.; Lui, S.F.; Ulasi, I.; Andreoli, S.; Balducci, A.; Dupuis, S.; et al. Living well with kidney disease by patient and care partner empowerment: Kidney health for everyone everywhere. Hong Kong Med. J. 2021, 27, 97–98. [Google Scholar] [CrossRef] [PubMed]
- Kaul, K.; Schumann, S.; Sander, C.; Däbritz, J.; de Laffolie, J. A Nationwide Survey on Patient Empowerment in Pediatric Inflammatory Bowel Disease in Germany. Children 2023, 10, 1904. [Google Scholar] [CrossRef] [PubMed]
- Feierabend, S.; Rathgeb, T.; Kheredmand, H.; Glöckler, S. JIM 2023: Jugend, Information, Medien—Basisuntersuchung zum Medienumgang 12-bis 19-Jähriger in Deutschland. Available online: https://www.mpfs.de/fileadmin/files/Studien/JIM/2022/JIM_2023_web_final_kor.pdf (accessed on 10 March 2024).
- Ricardo, A.C.; Pereira, L.N.; Betoko, A.; Goh, V.; Amarah, A.; Warady, B.A.; Moxey-Mims, M.; Furth, S.; Lash, J.P. Parental Health Literacy and Progression of Chronic Kidney Disease in Children. Pediatr. Nephrol. 2018, 33, 1759–1764. [Google Scholar] [CrossRef] [PubMed]
- Was Halten 16-26-Jährige Persönlich im LEBEN Für Besonders Wichtig und Erstrebenswert? Available online: https://de.statista.com/statistik/daten/studie/816718/umfrage/als-besonders-wichtig-erachtete-aspekte-im-leben-bei-16-bis-26-jaehrigen/ (accessed on 9 February 2024).
- Hald, M.; Carlsen, K.; Wewer, V. Transition of Adolescents with Inflammatory Bowel Disease—Are the Pediatric Teams up to the Task? Children 2021, 8, 900. [Google Scholar] [CrossRef]
- Stiftung Gesundheitswissen. Menschen mit Chronischen Erkrankungen: Hausarzt Erster Ansprechpartner. Available online: https://www.stiftung-gesundheitswissen.de/projekte/menschen-mit-chronischen-erkrankungen-hausarzt-erster-ansprechpartner (accessed on 12 March 2024).
- Jugendliche in Deutschland zum Vertrauen in Medien und Öffentliche Einrichtungen 2022. Available online: https://de.statista.com/statistik/daten/studie/1368071/umfrage/jugendliche-in-deutschland-zum-vertrauen-in-medien-und-oeffentliche-einrichtungen/ (accessed on 9 February 2024).
- Zhong, B.; Xie, W.; Davis Kempton, S.; Zhi, M.; Zhao, J. Health Information Processing and Symptom Management in a Cross-Cultural Setting: Insights from IBD Patients. Health Commun. 2023, 1–10. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Responses in % | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patients | Parents | |||||||||||||||||||
| Activity | n | Yes | No | n | Never | Rarely | Regularly | Often | ||||||||||||
| Pursue hobbies | 380 | 84.7 | 15.3 | 582 | 8.4 | 13.5 | 46.0 | 32.1 | ||||||||||||
| Age (in years) | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | ||
| 273 | 23.4 | 25.3 | 37.4 | 2.9 | 1.5 | 9.5 | 578 | 1.2 | 3.5 | 1.7 | 0.0 | 3.8 | 3.5 | 9.9 | 13.1 | 11.1 | 5.5 | 10.7 | 7.6 | |
| Talk to the doctor about IBD | 372 | 83.3 | 16.7 | 587 | 6.8 | 33.4 | 53.2 | 6.6 | ||||||||||||
| Age (in years) | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | ||
| 269 | 20.4 | 23.0 | 39.4 | 7.1 | 3.3 | 6.7 | 583 | 0.7 | 2.1 | 0.9 | 7.9 | 8.7 | 7.7 | 8.6 | 18.2 | 14.6 | 1.0 | 2.1 | 1.2 | |
| Meet friends | 376 | 83.2 | 16.8 | 583 | 7.5 | 19.9 | 43.4 | 29.2 | ||||||||||||
| Age (in years) | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | ||
| 273 | 22.7 | 22.0 | 37.7 | 3.3 | 4.8 | 9.2 | 579 | 1.4 | 1.6 | 1.9 | 2.9 | 7.3 | 4.5 | 10.0 | 13.6 | 8.5 | 4.1 | 8.5 | 8.6 | |
| Talk about IBD with family/friends | 380 | 82.6 | 17.4 | 595 | 7.6 | 39.3 | 39.2 | 13.9 | ||||||||||||
| Age (in years) | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | ||
| 273 | 24.9 | 20.5 | 17.0 | 3.7 | 4.4 | 9.5 | 591 | 0.5 | 2.5 | 1.7 | 8.0 | 12.2 | 9.6 | 7.1 | 11.2 | 11.0 | 2.4 | 4.9 | 2.0 | |
| Do sports and be physically active | 370 | 74.3 | 25.7 | 595 | 7.6 | 39.3 | 39.2 | 13.9 | ||||||||||||
| Age (in years) | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | ||
| 268 | 19.8 | 20.9 | 34.3 | 7.5 | 5.2 | 12.3 | 589 | 1.4 | 2.9 | 1.9 | 4.2 | 8.1 | 7.1 | 8.0 | 13.6 | 11.4 | 4.8 | 6.3 | 3.7 | |
| Take it easy physically | 355 | 47.6 | 52.4 | 580 | 18.1 | 38.6 | 31.2 | 12.1 | ||||||||||||
| Age (in years) | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | ||
| 258 | 12.4 | 12.0 | 23.3 | 14.3 | 13.6 | 24.4 | 576 | 1.9 | 6.4 | 4.2 | 9.0 | 9.7 | 9.7 | 5.6 | 9.7 | 7.3 | 1.6 | 5.0 | 3.1 | |
| Pay particular attention to the diet | 354 | 38.7 | 61.3 | 586 | 17.4 | 33.8 | 33.1 | 15.7 | ||||||||||||
| Age (in years) | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | ||
| 258 | 8.9 | 9.7 | 19.0 | 19.0 | 16.7 | 26.7 | 582 | 4.1 | 4.1 | 4.6 | 6.7 | 12.0 | 7.6 | 5.5 | 11.0 | 7.9 | 1.7 | 4.0 | 4.0 | |
| Talk about IBD with others affected | 358 | 20.7 | 79.3 | 575 | 73.6 | 20.8 | 4.0 | 1.6 | ||||||||||||
| Age (in years) | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | ||
| 260 | 6.2 | 5.0 | 11.2 | 21.9 | 20.8 | 35.0 | 571 | 12.1 | 21.7 | 18.4 | 4.4 | 7.5 | 4.9 | 0.4 | 1.4 | 1.4 | 0.4 | 0.4 | 0.2 | |
| Perform relaxation exercises | 356 | 19.1 | 80.9 | 567 | 65.8 | 27.5 | 4.8 | 1.9 | ||||||||||||
| Age (in years) | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | ||
| 258 | 4.3 | 6.2 | 10.9 | 23.3 | 19.8 | 35.7 | 564 | 12.9 | 20.7 | 14.5 | 4.8 | 7.6 | 6.7 | 0.7 | 1.8 | 1.8 | 0.0 | 0.9 | 0.7 | |
| Use psychological counseling | 357 | 16.0 | 84.0 | 576 | 77.8 | 10.0 | 10.6 | 1.6 | ||||||||||||
| Age (in years) | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | ||
| 260 | 24.6 | 21.5 | 35.4 | 3.5 | 4.6 | 10.4 | 572 | 14.2 | 23.8 | 17.7 | 1.9 | 3.7 | 2.6 | 2.3 | 3.1 | 3.1 | 0.2 | 0.0 | 0.7 | |
| Take part in a self-help group | 359 | 0.8 | 99.2 | 579 | 97.4 | 1.7 | 0.7 | 0.2 | ||||||||||||
| Age (in years) | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | ||
| 258 | 0.0 | 0.0 | 0.8 | 27.5 | 26.4 | 45.3 | 575 | 18.4 | 29.9 | 22.8 | 0.2 | 0.3 | 1.0 | 0.0 | 0.2 | 0.3 | 0.0 | 0.2 | 0.0 | |
| Responses in % | ||||||||
|---|---|---|---|---|---|---|---|---|
| Patients (n = 289) | ||||||||
| Knowledge | Age | Duration since Diagnosis | ||||||
| 12–13 | 14–15 | 16–17 | <1 Year | 1–2 Years | 3–4 Years | 5–6 Years | >6 Years | |
| Fully informed | 41.8 | 37.3 | 35.8 | 46.0 | 32.4 | 37.9 | 41.5 | 35.7 |
| Mostly informed | 43.0 | 54.7 | 52.6 | 40.0 | 56.5 | 47.4 | 50.9 | 53.6 |
| Little informed | 15.2 | 6.7 | 8.8 | 12.0 | 6.5 | 12.6 | 5.7 | 7.1 |
| Not enough informed | 0.0 | 0.0 | 2.2 | 2.0 | 0.9 | 2.1 | 1.9 | 2.4 |
| Parents (n = 586) | ||||||||
| Knowledge | Age | Duration since diagnosis | ||||||
| 12–13 | 14–15 | 16–17 | <1 Year | 1–2 Years | 3–4 Years | 5–6 Years | >6 Years | |
| Fully informed | 28.6 | 34.5 | 25.5 | 19.2 | 23.4 | 33.1 | 28.8 | 28.6 |
| Mostly informed | 44.7 | 59.8 | 66.7 | 67.3 | 68.3 | 55.4 | 65.8 | 63.4 |
| Little informed | 7.6 | 5.8 | 7.8 | 11.5 | 6.6 | 10.8 | 4.1 | 8.0 |
| Not enough informed | 0.0 | 1.2 | 0.0 | 1.9 | 1.8 | 0.8 | 1.4 | 0.0 |
| Responses (Yes, I Would Like to Know More about These Topics) in % | |||||
|---|---|---|---|---|---|
| Topics | Patients | Parents | Patients | Parents | |
| Causes | 60.7 | 22.0 | Drug Treatment Options | 44.0 | 20.8 |
| Disease duration | n = 288 | n = 321 | Disease duration | n = 282 | n = 331 |
| <1 year | 8.7 | 4.7 | <1 year | 5.0 | 3.9 |
| 1–2 years | 17.4 | 8.1 | 1–2 years | 13.5 | 8.8 |
| 3–4 years | 15.6 | 5.3 | 3–4 years | 11.3 | 4.2 |
| 5–6 years | 8.0 | 1.6 | 5–6 years | 6.4 | 1.2 |
| >6 years | 10.8 | 2.5 | >6 years | 7.8 | 2.7 |
| Age | n = 211 | n = 321 | Age | n = 212 | n = 331 |
| 12–13 years | 9.6 | 3.7 | 12–13 years | 10.4 | 3.9 |
| 14–15 years | 23.9 | 5.6 | 14–15 years | 11.3 | 5.4 |
| 16–17 years | 20.3 | 6.5 | 16–17 years | 25.0 | 4.5 |
| Transition | 58.5 | 22.4 | Nutrition | 41.3 | 19.7 |
| Disease duration | n = 283 | n = 307 | Disease duration | n = 274 | n = 319 |
| <1 year | 6.7 | 2.9 | <1 year | 6.2 | 3.1 |
| 1–2 years | 17.3 | 6.2 | 1–2 years | 12.4 | 6.9 |
| 3–4 years | 13.4 | 5.9 | 3–4 years | 8.8 | 5.0 |
| 5–6 years | 8.1 | 3.6 | 5–6 years | 5.8 | 1.9 |
| >6 years | 13.1 | 3.9 | >6 years | 7.7 | 2.8 |
| Age | n = 214 | n = 307 | Age | n = 208 | n = 319 |
| 12–13 years | 12.1 | 4.9 | 12–13 years | 7.7 | 3.4 |
| 14–15 years | 16.8 | 7.5 | 14–15 years | 9.6 | 4.7 |
| 16–17 years | 31.8 | 6.8 | 16–17 years | 25.0 | 4.4 |
| Concomitant diseases | 51.4 | 18.1 | Preventive health care | 42.1 | 17.9 |
| Disease duration | n = 282 | n = 319 | Disease duration | n = 270 | n = 311 |
| <1 year | 7.4 | 3.8 | <1 year | 7.8 | 2.6 |
| 1–2 years | 15.2 | 5.0 | 1–2 years | 10.4 | 5.8 |
| 3–4 years | 13.1 | 4.7 | 3–4 years | 11.1 | 4.8 |
| 5–6 years | 7.1 | 2.5 | 5–6 years | 4.8 | 1.6 |
| >6 years | 8.2 | 2.2 | >6 years | 8.1 | 3.2 |
| Age | n = 211 | n = 319 | Age | n = 203 | n = 311 |
| 12–13 years | 11.4 | 3.1 | 12–13 years | 8.9 | 3.2 |
| 14–15 years | 14.7 | 5.3 | 14–15 years | 8.9 | 4.5 |
| 16–17 years | 27.0 | 5.3 | 16–17 years | 24.1 | 4.8 |
| Social and law issues | 52.6 | 22.2 | Medication side effects | 38.0 | 17.6 |
| Disease duration | n = 272 | n = 310 | Disease duration | n = 282 | n = 323 |
| <1 year | 7.7 | 3.5 | <1 year | 4.6 | 2.5 |
| 1–2 years | 14.7 | 6.5 | 1–2 years | 9.9 | 6.2 |
| 3–4 years | 11.0 | 4.5 | 3–4 years | 10.3 | 5.0 |
| 5–6 years | 8.5 | 3.9 | 5–6 years | 6.4 | 1.5 |
| > 6 years | 10.7 | 3.9 | >6 years | 6.7 | 2.5 |
| Age | n = 205 | n = 310 | Age | n = 212 | n = 321 |
| 12–13 years | 10.2 | 4.5 | 12–13 years | 9.4 | 2.8 |
| 14–15 years | 12.2 | 6.1 | 14–15 years | 8.0 | 5.9 |
| 16–17 years | 31.7 | 5.5 | 16–17 years | 22.2 | 5.0 |
| Complications in the course of the disease | 49.5 | 17.0 | Patient Organizations | 17.8 | 10.7 |
| Disease duration | n = 281 | n = 317 | Disease duration | n = 268 | n = 298 |
| <1 year | 7.1 | 2.8 | <1 year | 1.1 | 2.3 |
| 1–2 years | 13.9 | 5.4 | 1–2 years | 3.4 | 3.7 |
| 3–4 years | 13.2 | 5.4 | 3–4 years | 6.3 | 1.3 |
| 5–6 years | 6.4 | 1.6 | 5–6 years | 3.0 | 1.3 |
| >6 years | 8.9 | 1.9 | >6 years | 3.7 | 2.0 |
| Age | n = 210 | n = 317 | Age | n = 203 | n = 298 |
| 12–13 years | 14.3 | 3.2 | 12–13 years | 3.4 | 2.0 |
| 14–15 years | 13.8 | 5.0 | 14–15 years | 4.9 | 2.4 |
| 16–17 years | 23.8 | 5.4 | 16–17 years | 11.3 | 2.0 |
| School and training | 47.3 | 20.3 | Self-help groups | 17.8 | 9.2 |
| Disease duration | n = 278 | n = 314 | Disease duration | n = 250 | n = 393 |
| <1 year | 6.5 | 3.2 | <1 year | 2.0 | 3.0 |
| 1–2 years | 14.7 | 6.7 | 1–2 years | 4.4 | 3.3 |
| 3–4 years | 12.2 | 4.5 | 3–4 years | 4.4 | 1.0 |
| 5–6 years | 5.8 | 2.9 | 5–6 years | 2.0 | 1.0 |
| >6 years | 7.6 | 3.2 | >6 years | 4.0 | 1.0 |
| Age | n = 213 | n = 314 | Age | n = 118 | n = 302 |
| 12–13 years | 12.2 | 3.2 | 12–13 years | 2.7 | 0.9 |
| 14–15 years | 12.7 | 3.5 | 14–15 years | 6.4 | 2.3 |
| 16–17 years | 25.4 | 5.1 | 16–17 years | 9.6 | 1.3 |
| Dealing with mental strain and stress | 46.6 | 20.2 | IBD in general | 42.9 | 15.7 |
| Disease duration | n = 279 | n = 321 | Disease duration | n = 273 | n = 331 |
| <1 year | 4.7 | 3.1 | <1 year | 6.6 | 3.9 |
| 1–2 years | 12.2 | 6.5 | 1–2 years | 11.0 | 6.9 |
| 3–4 years | 11.8 | 5.6 | 3–4 years | 12.1 | 3.3 |
| 5–6 years | 7.5 | 1.9 | 5–6 years | 5.5 | 0.9 |
| >6 years | 10.0 | 3.1 | >6 years | 6.6 | 0.6 |
| Age | n = 214 | n = 321 | Age | n = 205 | n = 331 |
| 12–13 years | 9.8 | 4.4 | 12–13 years | 8.8 | 1.5 |
| 14–15 years | 12.1 | 4.7 | 14–15 years | 12.7 | 3.9 |
| 16–17 years | 26.2 | 5.0 | 16–17 years | 25.4 | 4.2 |
| Surgical treatment options | 31.5 | 11.0 | Prognosis | 43.8 | 17.2 |
| Disease duration | n = 288 | n = 316 | Disease duration | n = 270 | n = 313 |
| <1 year | 2.8 | 2.8 | <1 year | 6.3 | 3.8 |
| 1–2 years | 9.7 | 3.8 | 1–2 years | 11.5 | 5.8 |
| 3–4 years | 8.7 | 2.8 | 3–4 years | 11.5 | 3.2 |
| 5–6 years | 5.2 | 0.9 | 5–6 years | 5.2 | 1.6 |
| >6 years | 4.9 | 0.6 | >6 years | 9.3 | 2.9 |
| Age | n = 216 | n = 316 | Age | n = 204 | n = 313 |
| 12–13 years | 7.9 | 0.9 | 12–13 years | 10.8 | 2.2 |
| 14–15 years | 9.3 | 2.5 | 14–15 years | 12.3 | 5.1 |
| 16–17 years | 14.8 | 3.2 | 16–17 years | 23.0 | 4.8 |
| Responses (in This Way I Would Like to Have Information) in % | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Source of Information | n | Patients | n | Parents | Source of Information | n | Patients | n | Parents | |||
| Internet | 375 | 57.9 | 578 | 60.6 | Specialist magazines and books | 376 | 33.2 | 578 | 48.8 | |||
| YouTube | 375 | 54.7 | 576 | 22.9 | Brochures and information leaflets | 376 | 32.4 | 578 | 44.8 | |||
| Explanatory films | 375 | 47.2 | 577 | 40.7 | Forums for patients/parents | 375 | 32.0 | 577 | 50.8 | |||
| Lectures | 375 | 42.7 | 578 | 54.0 | Apps (communication platform) | 375 | 28.3 | 578 | 18.3 | |||
| Books for children/adolescents | 376 | 37.5 | 578 | 57.4 | Blogs | 375 | 25.3 | 577 | 10.7 | |||
| Workshops (1 day) | 376 | 35.4 | 578 | 47.6 | Chats | 375 | 21.1 | 577 | 9.5 | |||
| Apps (online information) | 374 | 35.3 | 576 | 27.3 | Counseling offers for patients | 375 | 17.3 | 577 | 41.1 | |||
| Preferred Information Gathering by Age Responses (in This Way I Would Like Information) in % | ||||||||||||
| Source of Information | Patients: Age in Years | Parents: Age of Their Children (Patients) in Years | ||||||||||
| n | 12–13 | 14–15 | 16–17 | n | 0–5 | 6–7 | 8–9 | 10–11 | 12–13 | 14–15 | 16–17 | |
| Internet | 281 | 12.5 | 13.9 | 29.9 | 575 | 3.3 | 1.4 | 3.5 | 8.3 | 11.5 | 19.3 | 13.2 |
| YouTube | 281 | 12.5 | 15.3 | 29.5 | 573 | 1.0 | 0.5 | 1.7 | 4.4 | 3.8 | 6.1 | 5.4 |
| Explanatory films | 281 | 11.4 | 13.2 | 23.8 | 574 | 2.6 | 1.4 | 3.5 | 7.0 | 7.1 | 11.1 | 8.2 |
| Lectures | 281 | 12.1 | 11.4 | 19.6 | 575 | 3.0 | 1.2 | 4.2 | 7.3 | 9.7 | 16.3 | 12.5 |
| Books for children/adolescents | 282 | 11.3 | 11.3 | 16.7 | 575 | 4.7 | 2.4 | 4.5 | 10.4 | 11.5 | 15.5 | 8.7 |
| Workshops (1 day) | 282 | 8.5 | 10.3 | 17.7 | 575 | 3.0 | 1.2 | 3.1 | 7.3 | 8.7 | 14.6 | 9.7 |
| Apps (online information) | 280 | 7.1 | 10.4 | 18.2 | 573 | 2.6 | 1.0 | 2.3 | 3.7 | 4.0 | 8.4 | 5.1 |
| Specialist magazines and books | 282 | 7.8 | 7.4 | 18.1 | 575 | 2.3 | 1.6 | 2.8 | 6.6 | 9.0 | 14.8 | 12.0 |
| Brochures and information leaflets | 282 | 6.0 | 9.2 | 16.3 | 575 | 2.1 | 1.4 | 2.8 | 5.4 | 8.3 | 13.9 | 11.1 |
| Forum for patients/parents | 291 | 4.3 | 12.1 | 16.7 | 574 | 3.7 | 1.9 | 3.5 | 8.2 | 9.2 | 14.6 | 9.6 |
| Apps (communication platform) | 281 | 7.8 | 6.8 | 13.9 | 575 | 1.7 | 0.7 | 1.4 | 3.3 | 2.3 | 5.7 | 3.1 |
| Blogs | 281 | 3.2 | 6.8 | 14.9 | 574 | 0.2 | 0.5 | 0.5 | 2.3 | 1.7 | 3.5 | 1.9 |
| Chats | 291 | 4.6 | 6.0 | 10.0 | 574 | 0.9 | 0.5 | 0.9 | 1.6 | 1.2 | 3.0 | 1.4 |
| Counseling offers for patients | 281 | 2.8 | 5.7 | 8.9 | 574 | 2.8 | 1.6 | 1.7 | 5.2 | 7.8 | 10.3 | 11.3 |
| Responses in % | |||||||||||||
| Information Source | n | Patients | n | Parents | Information Source | n | Patients | n | Parents | ||||
| Pediatric gastroenterologists | 387 | 87.3 | 577 | 95.3 | Sports Professionals | 387 | 14.7 | 577 | 14.2 | ||||
| Adult gastroenterologists | 386 | 56.2 | 576 | 40.6 | Patient Associations | 387 | 12.7 | 577 | 22.2 | ||||
| Active research scientists | 387 | 40.8 | 577 | 43.2 | Representatives of self-help groups | 387 | 7.2 | 577 | 18.4 | ||||
| Nutritionists | 387 | 37.7 | 577 | 52.9 | Social Worker | 387 | 5.7 | 577 | 9.0 | ||||
| Young people affected | 387 | 33.9 | 577 | 38.5 | Lawyers | 387 | 3.4 | 577 | 6.4 | ||||
| Psychologists | 387 | 25.8 | 577 | 38.8 | Health insurance companies | 387 | 3.1 | 577 | 14.0 | ||||
| Families affected | 387 | 23.0 | 577 | 39.7 | Outdoor and music educators | 387 | 2.1 | 577 | 6.8 | ||||
| Breakdown of Preferred Information Source by Duration Since Diagnosis Responses in % | |||||||||||||
| Patients: Disease Duration in Years | Parents: Disease Duration of Child (Patients) in Years | ||||||||||||
| Information Source | n | <1 | 1–2 | 3–4 | 5–6 | >6 | n | <1 | 1–2 | 3–4 | 5–6 | >6 | |
| Pediatric gastroenterologists | 384 | 11.5 | 25.5 | 20.1 | 11.2 | 19.3 | 575 | 17.0 | 27.3 | 20.7 | 12.2 | 18.1 | |
| Adult gastroenterologists | 383 | 5.5 | 13.6 | 13.6 | 9.7 | 13.8 | 574 | 8.0 | 10.8 | 8.4 | 5.2 | 8.0 | |
| Active research scientist | 384 | 5.5 | 12.8 | 8.9 | 5.5 | 8.6 | 575 | 8.2 | 12.7 | 8.9 | 4.7 | 8.5 | |
| Nutritionists | 384 | 6.0 | 10.9 | 8.9 | 6.0 | 5.7 | 575 | 9.7 | 16.0 | 12.3 | 6.8 | 8.2 | |
| Young people concerned | 384 | 3.9 | 9.4 | 7.3 | 6.0 | 7.0 | 575 | 7.1 | 12.9 | 8.0 | 4.7 | 5.9 | |
| Psychologists | 384 | 3.9 | 5.2 | 6.0 | 5.2 | 5.5 | 575 | 6.4 | 10.3 | 9.4 | 5.2 | 7.5 | |
| Families affected | 384 | 3.4 | 5.2 | 6.5 | 4.4 | 3.6 | 575 | 8.0 | 11.1 | 9.7 | 4.3 | 6.6 | |
| Sports professionals | 384 | 2.3 | 3.6 | 3.4 | 1.8 | 3.1 | 575 | 1.7 | 4.2 | 4.0 | 1.7 | 2.6 | |
| Patient associations | 384 | 1.3 | 3.9 | 2.9 | 2.1 | 2.6 | 575 | 3.3 | 7.1 | 4.9 | 3.3 | 3.7 | |
| Representatives of self-help groups | 384 | 0.8 | 3.1 | 0.8 | 1.0 | 1.6 | 575 | 3.7 | 6.1 | 3.8 | 2.1 | 2.8 | |
| Social worker | 384 | 0.3 | 2.1 | 1.0 | 0.3 | 2.1 | 575 | 1.6 | 3.1 | 2.3 | 1.2 | 0.9 | |
| Lawyers | 384 | 0.5 | 0.5 | 0.5 | 0.3 | 0.8 | 575 | 0.7 | 1.7 | 1.6 | 1.2 | 1.2 | |
| Health insurance companies | 384 | 0.3 | 1.3 | 0.5 | 0.3 | 0.8 | 575 | 2.1 | 5.0 | 2.4 | 2.3 | 2.3 | |
| Outdoor and music educators | 384 | 0.0 | 0.8 | 0.8 | 0.0 | 0.5 | 575 | 0.7 | 2.3 | 2.4 | 0.9 | 0.5 | |
| At What Point Information Is Needed | n | At Diagnosis | In the First Year | During the Further Disease Course | No Need for Information | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IBD Topics | Responses in % and Age in Years | ||||||||||||
| General | 552 | 67.6 | 10.5 | 17.0 | 4.9 | ||||||||
| Age | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | |
| 387 | 14.2 | 25.8 | 22.5 | 4.4 | 7.0 | 5.4 | 4.1 | 7.5 | 4.4 | 1.8 | 1.6 | 1.3 | |
| Causes | 535 | 63.2 | 16.3 | 15.9 | 4.7 | ||||||||
| Age | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | |
| 372 | 14.0 | 25.5 | 22.6 | 4.3 | 7.0 | 5.6 | 4.3 | 7.5 | 4.3 | 1.9 | 1.6 | 1.3 | |
| Nutrition | 538 | 49.8 | 22.1 | 21.9 | 6.1 | ||||||||
| Age | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | |
| 387 | 10.9 | 20.2 | 16.5 | 4.1 | 9.3 | 7.8 | 7.2 | 9.6 | 7.8 | 1.6 | 3.6 | 1.6 | |
| Medical treatment options | 555 | 47.7 | 16.8 | 32.1 | 3.4 | ||||||||
| Age | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | |
| 400 | 10.8 | 18.0 | 17.8 | 3.3 | 8.0 | 5.0 | 9.8 | 15.8 | 8.8 | 0.8 | 1.3 | 1.0 | |
| Medication side effects | 542 | 45.2 | 21.2 | 28.4 | 5.2 | ||||||||
| Age | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | |
| 389 | 10.0 | 18.3 | 16.2 | 4.4 | 9.0 | 8.2 | 8.0 | 13.1 | 8.5 | 2.3 | 1.5 | 0.5 | |
| Prognosis | 536 | 37.3 | 20.5 | 36.6 | 5.6 | ||||||||
| Age | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | |
| 392 | 8.4 | 12.2 | 12.2 | 3.8 | 9.9 | 6.9 | 9.4 | 15.6 | 12.2 | 2.0 | 3.3 | 3.8 | |
| Dealing with psychological stress/stress management | 532 | 33.1 | 26.1 | 32.7 | 8.1 | ||||||||
| Age | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | |
| 381 | 5.8 | 15.0 | 11.3 | 6.3 | 9.2 | 10.5 | 9.4 | 14.7 | 10.0 | 1.8 | 4.2 | 1.8 | |
| Psychotherapeutic accompanying measures | 526 | 31.6 | 22.6 | 33.8 | 12.0 | ||||||||
| Age | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | |
| 375 | 5.1 | 12.3 | 12.3 | 5.3 | 9.6 | 8.0 | 9.9 | 14.7 | 10.4 | 3.7 | 5.6 | 3.2 | |
| Concomitant diseases | 540 | 29.1 | 25.4 | 41.7 | 3.9 | ||||||||
| Age | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | |
| 387 | 7.8 | 10.6 | 11.4 | 3.9 | 10.9 | 9.6 | 11.6 | 18.9 | 11.9 | 1.0 | 2.1 | 0.5 | |
| School and vocational training | 528 | 24.2 | 28.2 | 40.3 | 7.2 | ||||||||
| Age | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | |
| 384 | 7.6 | 10.4 | 7.3 | 6.3 | 12.8 | 10.2 | 9.6 | 16.4 | 2.1 | 2.1 | 3.6 | ||
| Patient organizations and self-help groups | 489 | 25.8 | 24.1 | 31.7 | 18.4 | ||||||||
| Age | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | |
| 347 | 4.6 | 11.2 | 7.2 | 4.9 | 9.8 | 9.8 | 9.8 | 12.7 | 9.5 | 5.2 | 7.8 | 7.5 | |
| Measures for preventive health care | 509 | 21.4 | 23.6 | 45.0 | 10.0 | ||||||||
| Age | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | |
| 368 | 4.1 | 8.7 | 6.8 | 4.6 | 9.2 | 8.4 | 13.0 | 19.8 | 15.8 | 2.2 | 5.2 | 2.2 | |
| Complications during course of the disease | 532 | 19.7 | 19.4 | 56.0 | 4.9 | ||||||||
| Age | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | |
| 384 | 5.2 | 6.5 | 7.3 | 3.6 | 7.0 | 8.1 | 14.8 | 25.8 | 17.4 | 1.0 | 2.3 | 0.8 | |
| Social law issues | 509 | 11.0 | 16.7 | 63.5 | 8.8 | ||||||||
| Age | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | |
| 369 | 2.2 | 5.1 | 3.5 | 3.5 | 6.8 | 4.9 | 17.6 | 27.6 | 20.9 | 1.4 | 3.0 | 3.5 | |
| Transition to adult health care | 525 | 3.6 | 4.4 | 84.2 | 7.8 | ||||||||
| Age | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | 12–13 | 14–15 | 16–17 | |
| 383 | 1.0 | 1.6 | 0.8 | 0.5 | 1.3 | 3.1 | 21.4 | 37.9 | 27.9 | 1.0 | 1.8 | 1.6 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaul, K.; Schumann, S.; Sander, C.; Däbritz, J.; de Laffolie, J. Health Literacy of Children and Adolescents with Inflammatory Bowel Disease (IBD) and Parents of IBD Patients—Coping and Information Needs. Children 2024, 11, 481. https://doi.org/10.3390/children11040481
Kaul K, Schumann S, Sander C, Däbritz J, de Laffolie J. Health Literacy of Children and Adolescents with Inflammatory Bowel Disease (IBD) and Parents of IBD Patients—Coping and Information Needs. Children. 2024; 11(4):481. https://doi.org/10.3390/children11040481
Chicago/Turabian StyleKaul, Kalina, Stefan Schumann, Cornelia Sander, Jan Däbritz, and Jan de Laffolie. 2024. "Health Literacy of Children and Adolescents with Inflammatory Bowel Disease (IBD) and Parents of IBD Patients—Coping and Information Needs" Children 11, no. 4: 481. https://doi.org/10.3390/children11040481