
Silver Diamine Fluoride in Pediatric Dentistry: Effectiveness in Preventing and Arresting Dental Caries—A Systematic Review

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. PICO
3. Results
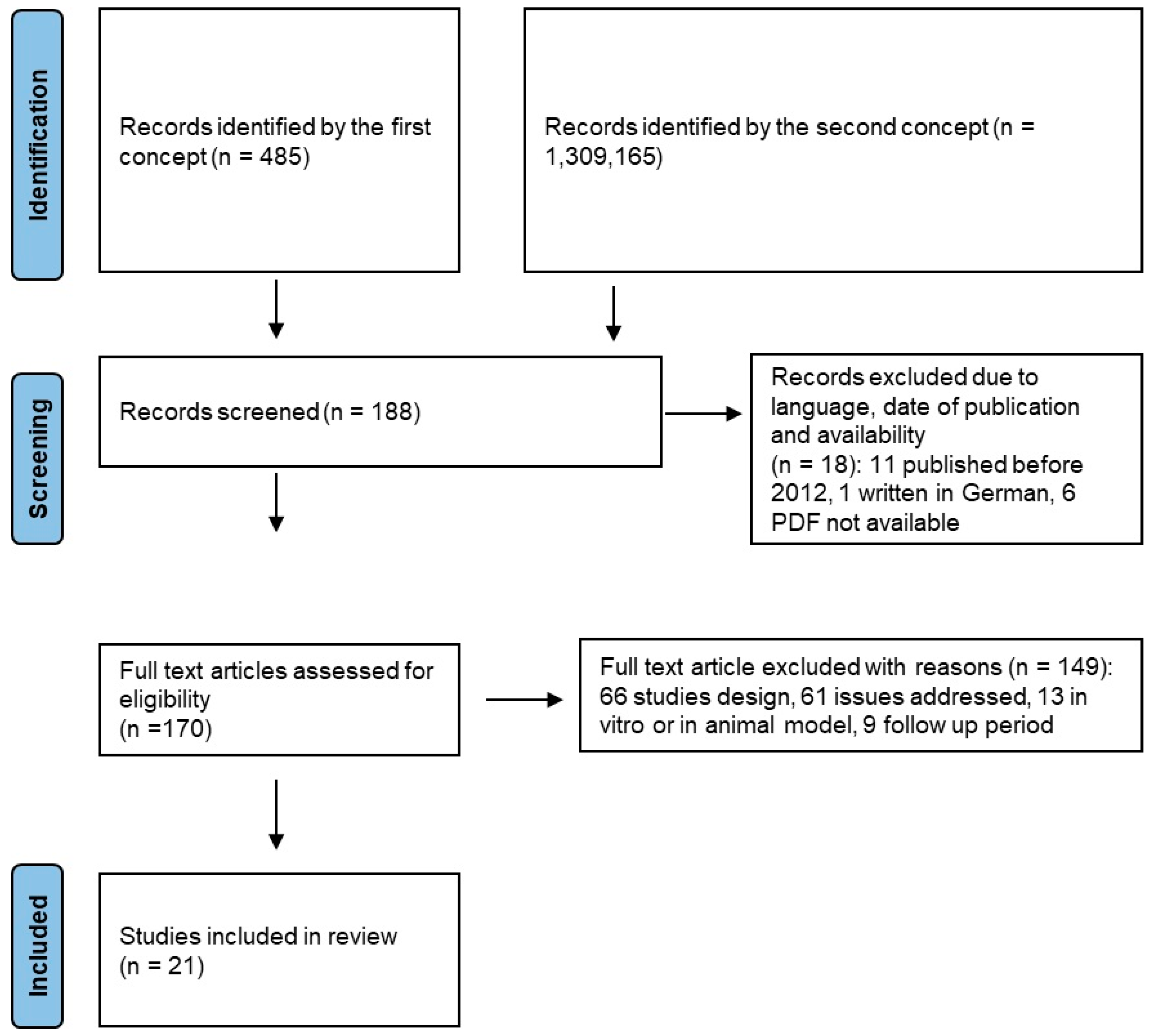
3.1. Study Selectionm
- 11 published before 2012,
- 1 written in German, and
- 6 PDF not available.
- 61 not responding to the object of this review.
- 66 presenting a study design other than a randomized controlled trial, including 21 systematic reviews, 12 narrative reviews, 8 cohort studies, 4 umbrella reviews, 5 commentary publications, 2 non-randomized comparative studies, 2 cross-sectional studies, 2 overviews, 2 guidelines, 1 case report, 1 pilot study, 1 retrospective study, 1 Delphi study, 1 letter to the editor, 1 selection of abstracts, 1 critical summary and 1 promotional publication.
- 9 study protocols not carried out on patients, 5 studies whose follow-up period was extended in randomized controlled trials selected for this study, 4 studies whose follow-up period is less than 6 months, 2 publications relating to animals and 2 in vivo studies.
- All this information is part of the Prisma flow chart.
Selected Studies
- -
- Bias due to confounding,
- -
- Bias arising from measurement of exposure,
- -
- Bias in the selection of participants into the study,
- -
- Bias due to post-exposure intervention,
- -
- Bias due to missing data,
- -
- Bias arising from measurement of the outcome, and
- -
- Bias in the selection of the reported results.
3.2. Quality Assessment and Risk of Bias of Included Articles
4. Discussion
4.1. Permanent Teeth
4.2. Temporary Teeth
- -
- HRI group: 65.7%, 5% and 40% at 24, 12 and 6 months, respectively.
- -
- HRB group: 75%, 42.9% and 45.9% at 24, 12 and 6 months, respectively.
- -
- LRB group: 21.1%, 10.5% and 5.3% at 24, 12 and 6 months, respectively.
4.3. 30% SDF
4.4. 12% SDF
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
References
- Manton, D.J. Child Dental Caries—A Global Problem of Inequality. eClinicalMedicine 2018, 1, 3–4. [Google Scholar] [CrossRef]
- Patano, A.; Malcangi, G.; De Santis, M.; Morolla, R.; Settanni, V.; Piras, F.; Inchingolo, A.D.; Mancini, A.; Inchingolo, F.; Dipalma, G.; et al. Conservative Treatment of Dental Non-Carious Cervical Lesions: A Scoping Review. Biomedicines 2023, 11, 1530. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Global Burden of Untreated Caries: A Systematic Review and Metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Hemati, G.; Imani, M.M.; Choubsaz, P.; Inchingolo, F.; Sharifi, R.; Sadeghi, M.; Tadakamadla, S.K. Evaluation of Beta-Defensin 1 and Mannose-Binding Lectin 2 Polymorphisms in Children with Dental Caries Compared to Caries-Free Controls: A Systematic Review and Meta-Analysis. Children 2023, 10, 232. [Google Scholar] [CrossRef]
- Marchetti, E.; Tecco, S.; Caterini, E.; Casalena, F.; Quinzi, V.; Mattei, A.; Marzo, G. Alcohol-Free Essential Oils Containing Mouthrinse Efficacy on Three-Day Supragingival Plaque Regrowth: A Randomized Crossover Clinical Trial. Trials 2017, 18, 154. [Google Scholar] [CrossRef]
- Piancino, M.G.; Di Benedetto, L.; Matacena, G.; Deregibus, A.; Marzo, G.; Quinzi, V. Paediatric Orthodontics Part 3: Masticatory Function during Development. Eur. J. Paediatr. Dent. 2019, 20, 247–249. [Google Scholar] [CrossRef]
- Systemic and Topical Photodynamic Therapy (PDT) on Oral Mucosa Lesions: An Overview. Available online: https://pubmed.ncbi.nlm.nih.gov/29460529/ (accessed on 22 January 2024).
- Jiang, M.; Wong, M.C.M.; Chu, C.H.; Dai, L.; Lo, E.C.M. A 24-Month Randomized Controlled Trial on the Success Rates of Restoring Untreated and SDF-Treated Dentine Caries Lesions in Primary Teeth with the ART Approach. J. Dent. 2020, 100, 103435. [Google Scholar] [CrossRef] [PubMed]
- Patano, A.; Malcangi, G.; Sardano, R.; Mastrodonato, A.; Garofoli, G.; Mancini, A.; Inchingolo, A.D.; Di Venere, D.; Inchingolo, F.; Dipalma, G.; et al. White Spots: Prevention in Orthodontics—Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2023, 20, 5608. [Google Scholar] [CrossRef]
- Marinelli, G.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Limongelli, L.; Montenegro, V.; Coloccia, G.; Laudadio, C.; Patano, A.; Inchingolo, F.; et al. White Spot Lesions in Orthodontics: Prevention and Treatment. A Descriptive Review. J. Biol. Regul. Homeost. Agents 2021, 35, 227–240. [Google Scholar] [CrossRef]
- Minervini, G.; Marrapodi, M.M.; Cicciù, M. Online Bruxism-related information: Can people understand what they read? A Cross-Sectional Study. J. Oral Rehabil. 2023, 50, 1211–1216. [Google Scholar] [CrossRef]
- Jain, V. A Review on Applications of Silver Diamine Fluoride in Dentistry. Int. J. Oral Health Dent. 2018, 4, 58–62. [Google Scholar] [CrossRef]
- Contractor, I.A.; Girish, M.S.; Indira, M.D. Silver Diamine Fluoride: Extending the Spectrum of Preventive Dentistry, a Literature Review. Pediatr. Dent. J. 2021, 31, 17–24. [Google Scholar] [CrossRef]
- Inchingolo, F.; Tatullo, M.; Abenavoli, F.M.; Marrelli, M.; Inchingolo, A.D.; Palladino, A.; Inchingolo, A.M.; Dipalma, G. Oral Piercing and Oral Diseases: A Short Time Retrospective Study. Int. J. Med. Sci. 2011, 8, 649–652. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, F.; Tatullo, M.; Marrelli, M.; Inchingolo, A.M.; Inchingolo, A.D.; Dipalma, G.; Flace, P.; Girolamo, F.; Tarullo, A.; Laino, L.; et al. Regenerative Surgery Performed with Platelet-Rich Plasma Used in Sinus Lift Elevation before Dental Implant Surgery: An Useful Aid in Healing and Regeneration of Bone Tissue. Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 1222–1226. [Google Scholar]
- Vimercati, L.; De Maria, L.; Quarato, M.; Caputi, A.; Gesualdo, L.; Migliore, G.; Cavone, D.; Sponselli, S.; Pipoli, A.; Inchingolo, F.; et al. Association between Long COVID and Overweight/Obesity. J. Clin. Med. 2021, 10, 4143. [Google Scholar] [CrossRef]
- Inchingolo, F.; Tatullo, M.; Abenavoli, F.M.; Marrelli, M.; Inchingolo, A.D.; Gentile, M.; Inchingolo, A.M.; Dipalma, G. Non-Syndromic Multiple Supernumerary Teeth in a Family Unit with a Normal Karyotype: Case Report. Int. J. Med. Sci. 2010, 7, 378–384. [Google Scholar] [CrossRef]
- Marrelli, M.; Tatullo, M.; Dipalma, G.; Inchingolo, F. Oral Infection by Staphylococcus Aureus in Patients Affected by White Sponge Nevus: A Description of Two Cases Occurred in the Same Family. Int. J. Med. Sci. 2012, 9, 47–50. [Google Scholar] [CrossRef]
- Malcangi, G.; Inchingolo, A.D.; Inchingolo, A.M.; Piras, F.; Settanni, V.; Garofoli, G.; Palmieri, G.; Ceci, S.; Patano, A.; Mancini, A.; et al. COVID-19 Infection in Children and Infants: Current Status on Therapies and Vaccines. Children 2022, 9, 249. [Google Scholar] [CrossRef] [PubMed]
- Dohan Ehrenfest, D.M.; Del Corso, M.; Inchingolo, F.; Sammartino, G.; Charrier, J.-B. Platelet-Rich Plasma (PRP) and Platelet-Rich Fibrin (PRF) in Human Cell Cultures: Growth Factor Release and Contradictory Results. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 110, 418–421. [Google Scholar] [CrossRef]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Di Blasio, M.; Ronsivalle, V.; Cicciù, M. Children Oral Health and Parents Education Status: A Cross Sectional Study. BMC Oral Health 2023, 23, 787. [Google Scholar] [CrossRef]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Almeida, L.E.; Ronsivalle, V.; Cicciù, M. Prevalence of Temporomandibular Disorders (TMD) in Obesity Patients: A Systematic Review and Meta-analysis. J. Oral Rehabil. 2023, 50, 1544–1553. [Google Scholar] [CrossRef]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Di Blasio, M.; Isola, G.; Cicciù, M. Conservative Treatment of Temporomandibular Joint Condylar Fractures: A Systematic Review Conducted According to PRISMA Guidelines and the Cochrane Handbook for Systematic Reviews of Interventions. J. Oral Rehabil. 2023, 50, 886–893. [Google Scholar] [CrossRef]
- Franco, R.; Miranda, M.; Di Renzo, L.; De Lorenzo, A.; Barlattani, A.; Bollero, P. Glanzmann’s Thrombastenia: The Role of Tranexamic Acid in Oral Surgery. Case Rep. Dent. 2018, 2018, 9370212. [Google Scholar] [CrossRef]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Fiorillo, L.; Cervino, G.; Cicciù, M. Post-traumatic Stress, Prevalence of Temporomandibular Disorders in War Veterans: Systematic Review with Meta-analysis. J. Oral Rehabil. 2023, 50, 1101–1109. [Google Scholar] [CrossRef]
- Cicciù, M.; Minervini, G.; Franco, R.; Marrapodi, M.M.; Fiorillo, L.; Cervino, G. The Association between Parent Education Level, Oral Health, and Oral-Related Sleep Disturbance. An Observational Crosssectional Study. Eur. J. Paediatr. Dent. 2023, 24, 218–223. [Google Scholar] [CrossRef]
- Yamaga, R.; Nishino, M.; Yoshida, S.; Yokomizo, I. Diammine Silver Fluoride and Its Clinical Application. J. Osaka Univ. Dent. Sch. 1972, 12, 1–20. [Google Scholar] [PubMed]
- Enhanced Tooth Structure via Silver Microwires Following Treatment with 38 Percent Silver Diamine Fluoride. Available online: https://pubmed.ncbi.nlm.nih.gov/32522328/ (accessed on 8 July 2023).
- Woolfolk, S.K.; Cloyd, A.K.; Ye, Q.; Boone, K.; Spencer, P.; Snead, M.L.; Tamerler, C. Peptide-Enabled Nanocomposites Offer Biomimetic Reconstruction of Silver Diamine Fluoride-Treated Dental Tissues. Polymers 2022, 14, 1368. [Google Scholar] [CrossRef]
- Crystal, Y.O.; Rabieh, S.; Janal, M.N.; Rasamimari, S.; Bromage, T.G. Silver and Fluoride Content and Short-Term Stability of 38% Silver Diamine Fluoride. J. Am. Dent. Assoc. 2019, 150, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Mei, M.-L.; Chu, C.-H.; Low, K.-H.; Che, C.-M.; Lo, E.-C.-M. Caries Arresting Effect of Silver Diamine Fluoride on Dentine Carious Lesion with S. Mutans and L. Acidophilus Dual-Species Cariogenic Biofilm. Med. Oral Patol. Oral Cirugia Bucal 2013, 18, e824–e831. [Google Scholar] [CrossRef]
- Ruff, R.R.; Whittemore, R.; Grochecki, M.; Bateson, J.; Barry Godín, T.J. Silver Diamine Fluoride and Oral Health-Related Quality of Life: A Review and Network Meta-Analysis. PLoS ONE 2022, 17, e0261627. [Google Scholar] [CrossRef]
- Crincoli, V.; Anelli, M.G.; Quercia, E.; Piancino, M.G.; Di Comite, M. Temporomandibular Disorders and Oral Features in Early Rheumatoid Arthritis Patients: An Observational Study. Int. J. Med. Sci. 2019, 16, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Crincoli, V.; Di Comite, M.; Guerrieri, M.; Rotolo, R.P.; Limongelli, L.; Tempesta, A.; Iannone, F.; Rinaldi, A.; Lapadula, G.; Favia, G. Orofacial Manifestations and Temporomandibular Disorders of Sjögren Syndrome: An Observational Study. Int. J. Med. Sci. 2018, 15, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Crincoli, V.; Ballini, A.; Fatone, L.; Di Bisceglie, M.B.; Nardi, G.M.; Grassi, F.R. Cytokine Genotype Distribution in Patients with Periodontal Disease and Rheumatoid Arthritis or Diabetes Mellitus. J. Biol. Regul. Homeost. Agents 2016, 30, 863–866. [Google Scholar] [PubMed]
- Jain, A.; Bahuguna, R. Role of Matrix Metalloproteinases in Dental Caries, Pulp and Periapical Inflammation: An Overview. J. Oral Biol. Craniofacial Res. 2015, 5, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Mei, M.L.; Li, Q.L.; Chu, C.H.; Yiu, C.K.Y.; Lo, E.C.M. The Inhibitory Effects of Silver Diamine Fluoride at Different Concentrations on Matrix Metalloproteinases. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2012, 28, 903–908. [Google Scholar] [CrossRef]
- Minervini, G.; Lucchese, A.; Perillo, L.; Serpico, R.; Minervini, G. Unilateral Superior Condylar Neck Fracture with Dislocation in a Child Treated with an Acrylic Splint in the Upper Arch for Functional Repositioning of the Mandible. Cranio J. Craniomandib. Pract. 2017, 35, 337–341. [Google Scholar] [CrossRef] [PubMed]
- BaniHani, A.; Santamaría, R.M.; Hu, S.; Maden, M.; Albadri, S. Minimal Intervention Dentistry for Managing Carious Lesions into Dentine in Primary Teeth: An Umbrella Review. Eur. Arch. Paediatr. Dent. Off. J. Eur. Acad. Paediatr. Dent. 2022, 23, 667–693. [Google Scholar] [CrossRef] [PubMed]
- Reddy, L.K.V.; Madithati, P.; Narapureddy, B.R.; Ravula, S.R.; Vaddamanu, S.K.; Alhamoudi, F.H.; Minervini, G.; Chaturvedi, S. Perception about Health Applications (Apps) in Smartphones towards Telemedicine during COVID-19: A Cross-Sectional Study. J. Pers. Med. 2022, 12, 1920. [Google Scholar] [CrossRef]
- BaniHani, A.; Gardener, C.; Raggio, D.P.; Santamaría, R.M.; Albadri, S. Could COVID-19 Change the Way We Manage Caries in Primary Teeth? Current Implications on Paediatric Dentistry. Int. J. Paediatr. Dent. 2020, 30, 523–525. [Google Scholar] [CrossRef]
- Gao, S.S.; Chen, K.J.; Duangthip, D.; Wong, M.C.M.; Lo, E.C.M.; Chu, C.H. Arresting Early Childhood Caries Using Silver and Fluoride Products—A Randomised Trial. J. Dent. 2020, 103, 103522. [Google Scholar] [CrossRef]
- Duangthip, D.; Wong, M.C.M.; Chu, C.H.; Lo, E.C.M. Caries Arrest by Topical Fluorides in Preschool Children: 30-Month Results. J. Dent. 2018, 70, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Fung, M.H.T.; Duangthip, D.; Wong, M.C.M.; Lo, E.C.M.; Chu, C.H. Randomized Clinical Trial of 12% and 38% Silver Diamine Fluoride Treatment. J. Dent. Res. 2018, 97, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.Y.; Lo, E.C.M.; Chu, C.H.; Lin, H.C. Randomized Trial on Fluorides and Sealants for Fissure Caries Prevention. J. Dent. Res. 2012, 91, 753–758. [Google Scholar] [CrossRef]
- Mabangkhru, S.; Duangthip, D.; Chu, C.H.; Phonghanyudh, A.; Jirarattanasopha, V. A Randomized Clinical Trial to Arrest Dentin Caries in Young Children Using Silver Diamine Fluoride. J. Dent. 2020, 99, 103375. [Google Scholar] [CrossRef] [PubMed]
- Pisarnturakit, P.; Detsomboonrat, P. Comparison of Two Caries Prevention Programs among Thai Kindergarten: A Randomized Controlled Trial. BMC Oral Health 2020, 20, 119. [Google Scholar] [CrossRef] [PubMed]
- Phonghanyudh, A.; Duangthip, D.; Mabangkhru, S.; Jirarattanasopha, V. Is Silver Diamine Fluoride Effective in Arresting Enamel Caries? A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2022, 19, 8992. [Google Scholar] [CrossRef]
- Zhi, Q.H.; Lo, E.C.M.; Lin, H.C. Randomized Clinical Trial on Effectiveness of Silver Diamine Fluoride and Glass Ionomer in Arresting Dentine Caries in Preschool Children. J. Dent. 2012, 40, 962–967. [Google Scholar] [CrossRef]
- Abdellatif, H.M.; Ali, A.M.; Baghdady, S.I.; ElKateb, M.A. Caries Arrest Effectiveness of Silver Diamine Fluoride Compared to Alternative Restorative Technique: Randomized Clinical Trial. Eur. Arch. Paediatr. Dent. 2021, 22, 575–585. [Google Scholar] [CrossRef]
- Tirupathi, S.; SVSG, N.; Rajasekhar, S.; Nuvvula, S. Comparative Cariostatic Efficacy of a Novel Nano-Silver Fluoride Varnish with 38% Silver Diamine Fluoride Varnish a Double-Blind Randomized Clinical Trial. J. Clin. Exp. Dent. 2019, 11, e105–e112. [Google Scholar] [CrossRef]
- Joshi, K.H.; Basheer, S.M.; Ehsan, A.; Singh, S.; Kaur, R.; Suman, S.; Babaji, P. Clinical Assessment of SDF Effect in Arresting Dental Caries in Deciduous Teeth. J. Pharm. Bioallied Sci. 2023, 15, S1201–S1203. [Google Scholar] [CrossRef]
- Monse, B.; Heinrich-Weltzien, R.; Mulder, J.; Holmgren, C.; van Palenstein Helderman, W.H. Caries Preventive Efficacy of Silver Diammine Fluoride (SDF) and ART Sealants in a School-Based Daily Fluoride Toothbrushing Program in the Philippines. BMC Oral Health 2012, 12, 52. [Google Scholar] [CrossRef] [PubMed]
- Vollú, A.L.; Rodrigues, G.F.; Rougemount Teixeira, R.V.; Cruz, L.R.; Dos Santos Massa, G.; de Lima Moreira, J.P.; Luiz, R.R.; Barja-Fidalgo, F.; Fonseca-Gonçalves, A. Efficacy of 30% Silver Diamine Fluoride Compared to Atraumatic Restorative Treatment on Dentine Caries Arrestment in Primary Molars of Preschool Children: A 12-Months Parallel Randomized Controlled Clinical Trial. J. Dent. 2019, 88, 103165. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, V.E.; de Vasconcelos, F.M.N.; Ribeiro, A.G.; Rosenblatt, A. Paradigm Shift in the Effective Treatment of Caries in Schoolchildren at Risk. Int. Dent. J. 2012, 62, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Ballikaya, E.; Erbas Unverdi, G.; Cehreli, Z. Management of Initial Carious Lesions of Hypomineralized Molars (MIH) with Silver Diamine Fluoride or Silver-Modified Atraumatic Restorative Treatment (SMART): 1-Year Results of a Prospective, Randomized Clinical Trial. Clin. Oral Investig. 2022, 26, 2197–2205. [Google Scholar] [CrossRef] [PubMed]
- Cleary, J.; Al-Hadidi, R.; Scully, A.; Yahn, W.; Zaid, Z.; Boynton, J.R.; Eckert, G.J.; Yanca, E.; Fontana, M. A 12-Month Randomized Clinical Trial of 38% SDF vs. Restorative Treatment. JDR Clin. Transl. Res. 2022, 7, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Horst, J.A.; Ellenikiotis, H.; Milgrom, P.M. UCSF Protocol for Caries Arrest Using Silver Diamine Fluoride: Rationale, Indications, and Consent. J. Calif. Dent. Assoc. 2016, 44, 16–28. [Google Scholar] [CrossRef] [PubMed]
- Ruff, R.R.; Barry-Godín, T.; Niederman, R. Effect of Silver Diamine Fluoride on Caries Arrest and Prevention: The CariedAway School-Based Randomized Clinical Trial. JAMA Netw. Open 2023, 6, e2255458. [Google Scholar] [CrossRef] [PubMed]
- Antonioni, M.B.; Fontana, M.; Salzmann, L.B.; Inglehart, M.R. Pediatric Dentists’ Silver Diamine Fluoride Education, Knowledge, Attitudes, and Professional Behavior: A National Survey. J. Dent. Educ. 2019, 83, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Ronsivalle, V.; Shapira, I.; Cicciù, M. Prevalence of Temporomandibular Disorders in Subjects Affected by Parkinson Disease: A Systematic Review and Metanalysis. J. Oral Rehabil. 2023, 50, 877–885. [Google Scholar] [CrossRef]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Fiorillo, L.; Cervino, G.; Cicciù, M. Economic Inequalities and Temporomandibular Disorders: A Systematic Review with Meta-Analysis. J. Oral Rehabil. 2023, 50, 715–723. [Google Scholar] [CrossRef]
- Teledentistry: Evaluation of Instagram Posts Related to Bruxism. Available online: https://pubmed.ncbi.nlm.nih.gov/36872812/ (accessed on 22 January 2024).
- Quinzi, V.; Ferro, R.; Rizzo, F.A.; Marranzini, E.M.; Federici Canova, F.; Mummolo, S.; Mattei, A.; Marzo, G. The Two by Four Appliance: A Nationwide Cross-Sectional Survey. Eur. J. Paediatr. Dent. 2018, 19, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Mummolo, S.; Tieri, M.; Tecco, S.; Mattei, A.; Albani, F.; Giuca, M.R.; Marzo, G. Clinical Evaluation of Salivary Indices and Levels of Streptococcus Mutans and Lactobacillus in Patients Treated with Occlus-o-Guide. Eur. J. Paediatr. Dent. 2014, 15, 367–370. [Google Scholar] [PubMed]
- Bernardi, S.; Mummolo, S.; Tecco, S.; Continenza, M.A.; Marzo, G. Histological Characterization of Sacco’s Concentrated Growth Factors Membrane. Int. J. Morphol. 2017, 35, 114–119. [Google Scholar] [CrossRef]
- Ultra-Low-Frequency Transcutaneous Electric Nerve Stimulation (ULF-TENS) in Subjects with Craniofacial Pain: A Retrospective Study. Available online: https://pubmed.ncbi.nlm.nih.gov/30295164/ (accessed on 22 January 2024).
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral Diseases: A Global Public Health Challenge. Lancet Lond. Engl. 2019, 394, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Tinanoff, N.; Baez, R.J.; Diaz Guillory, C.; Donly, K.J.; Feldens, C.A.; McGrath, C.; Phantumvanit, P.; Pitts, N.B.; Seow, W.K.; Sharkov, N.; et al. Early Childhood Caries Epidemiology, Aetiology, Risk Assessment, Societal Burden, Management, Education, and Policy: Global Perspective. Int. J. Paediatr. Dent. 2019, 29, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Ruff, R.R.; Senthi, S.; Susser, S.R.; Tsutsui, A. Oral Health, Academic Performance, and School Absenteeism in Children and Adolescents: A Systematic Review and Meta-Analysis. J. Am. Dent. Assoc. 2019, 150, 111–121.e4. [Google Scholar] [CrossRef]
- Mummolo, S.; Sapio, S.; Falco, A.; Vittorini, O.L.; Quinzi, V. Management of Pedodontic Patients in Moderate Sedation in Clinical Dentistry: Evaluation of Behaviour before and after Treatment. J. Biol. Regul. Homeost. Agents 2020, 34, 55–62. [Google Scholar]
- Crystal, Y.O.; Janal, M.N.; Hamilton, D.S.; Niederman, R. Parental Perceptions and Acceptance of Silver Diamine Fluoride Staining. J. Am. Dent. Assoc. 2017, 148, 510–518.e4. [Google Scholar] [CrossRef] [PubMed]
- Torres, P.J.; Phan, H.T.; Bojorquez, A.K.; Garcia-Godoy, F.; Pinzon, L.M. Minimally Invasive Techniques Used for Caries Management in Dentistry—A Review. J. Clin. Pediatr. Dent. 2021, 45, 224–232. [Google Scholar] [CrossRef]
- BaniHani, A.; Hamid, A.; Van Eeckhoven, J.; Gizani, S.; Albadri, S. Minimal Intervention Dentistry (MID) Mainstream or Unconventional Option? Study Exploring the Impact of COVID-19 on Paediatric Dentists’ Views and Practices of MID for Managing Carious Primary Teeth in Children across the United Kingdom and European Union. Eur. Arch. Paediatr. Dent. Off. J. Eur. Acad. Paediatr. Dent. 2022, 23, 835–844. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Malcangi, G.; Semjonova, A.; Inchingolo, A.M.; Patano, A.; Coloccia, G.; Ceci, S.; Marinelli, G.; Di Pede, C.; Ciocia, A.M.; et al. Oralbiotica/Oralbiotics: The Impact of Oral Microbiota on Dental Health and Demineralization: A Systematic Review of the Literature. Children 2022, 9, 1014. [Google Scholar] [CrossRef]
- Schwendicke, F.; Frencken, J.E.; Bjørndal, L.; Maltz, M.; Manton, D.J.; Ricketts, D.; Van Landuyt, K.; Banerjee, A.; Campus, G.; Doméjean, S.; et al. Managing Carious Lesions: Consensus Recommendations on Carious Tissue Removal. Adv. Dent. Res. 2016, 28, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Dorri, M.; Dunne, S.M.; Walsh, T.; Schwendicke, F. Micro-Invasive Interventions for Managing Proximal Dental Decay in Primary and Permanent Teeth. Cochrane Database Syst. Rev. 2015, 2015, CD010431. [Google Scholar] [CrossRef] [PubMed]
- Frencken, J.E.; Peters, M.C.; Manton, D.J.; Leal, S.C.; Gordan, V.V.; Eden, E. Minimal Intervention Dentistry for Managing Dental Caries—A Review: Report of a FDI Task Group. Int. Dent. J. 2012, 62, 223–243. [Google Scholar] [CrossRef] [PubMed]
- Libonati, A.; Di Taranto, V.; Mea, A.; Montemurro, E.; Gallusi, G.; Angotti, V.; Nardi, R.; Paglia, L.; Marzo, G.; Campanella, V. Clinical Antibacterial Effectiveness Healozone Technology after Incomplete Caries Removal. Eur. J. Paediatr. Dent. 2019, 20, 73–78. [Google Scholar] [CrossRef]
- Manuschai, J.; Talungchit, S.; Naorungroj, S. Penetration of Silver Diamine Fluoride in Deep Carious Lesions of Human Permanent Teeth: An In Vitro Study. Int. J. Dent. 2021, 2021, 3059129. [Google Scholar] [CrossRef]
- Seifo, N.; Cassie, H.; Radford, J.R.; Innes, N.P.T. Silver Diamine Fluoride for Managing Carious Lesions: An Umbrella Review. BMC Oral Health 2019, 19, 145. [Google Scholar] [CrossRef]
- Inchingolo, A.M.; Malcangi, G.; Ferrante, L.; Del Vecchio, G.; Viapiano, F.; Mancini, A.; Inchingolo, F.; Inchingolo, A.D.; Di Venere, D.; Dipalma, G.; et al. Damage from Carbonated Soft Drinks on Enamel: A Systematic Review. Nutrients 2023, 15, 1785. [Google Scholar] [CrossRef] [PubMed]
- Sharma, G.; Puranik, M.P.; Sowmya, K.R. Approaches to Arresting Dental Caries: An Update. J. Clin. Diagn. Res. JCDR 2015, 9, ZE08–ZE11. [Google Scholar] [CrossRef]
- Contreras, V.; Toro, M.J.; Elías-Boneta, A.R.; Encarnación-Burgos, A. Effectiveness of Silver Diamine Fluoride in Caries Prevention and Arrest: A Systematic Literature Review. Gen. Dent. 2017, 65, 22–29. [Google Scholar]
- Crystal, Y.O.; Niederman, R. Evidence-Based Dentistry Update on Silver Diamine Fluoride. Dent. Clin. N. Am. 2019, 63, 45–68. [Google Scholar] [CrossRef] [PubMed]
- Hafiz, Z.; Allam, R.; Almazyad, B.; Bedaiwi, A.; Alotaibi, A.; Almubrad, A. Effectiveness of Silver Diamine Fluoride in Arresting Caries in Primary and Early Mixed Dentition: A Systematic Review. Children 2022, 9, 1289. [Google Scholar] [CrossRef] [PubMed]
- Tecco, S.; Mummolo, S.; Marchetti, E.; Tetè, S.; Campanella, V.; Gatto, R.; Gallusi, G.; Tagliabue, A.; Marzo, G. sEMG Activity of Masticatory, Neck, and Trunk Muscles during the Treatment of Scoliosis with Functional Braces. A Longitudinal Controlled Study. J. Electromyogr. Kinesiol. Off. J. Int. Soc. Electrophysiol. Kinesiol. 2011, 21, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Zaffarano, L.; Salerno, C.; Campus, G.; Cirio, S.; Balian, A.; Karanxha, L.; Cagetti, M.G. Silver Diamine Fluoride (SDF) Efficacy in Arresting Cavitated Caries Lesions in Primary Molars: A Systematic Review and Metanalysis. Int. J. Environ. Res. Public Health 2022, 19, 12917. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, B.H.; Rajendra, A.; Veitz-Keenan, A.; Niederman, R. The Effect of Silver Diamine Fluoride in Preventing Caries in the Primary Dentition: A Systematic Review and Meta-Analysis. Caries Res. 2019, 53, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Dinoi, M.T.; Marchetti, E.; Garagiola, U.; Caruso, S.; Mummolo, S.; Marzo, G. Orthodontic Treatment of an Unerupted Mandibular Canine Tooth in a Patient with Mixed Dentition: A Case Report. J. Med. Case Rep. 2016, 10, 170. [Google Scholar] [CrossRef] [PubMed]
- Duangthip, D.; Jiang, M.; Chu, C.H.; Lo, E.C.M. Restorative Approaches to Treat Dentin Caries in Preschool Children: Systematic Review. Eur. J. Paediatr. Dent. 2016, 17, 113–121. [Google Scholar] [PubMed]
- Campanella, V.; Syed, J.; Santacroce, L.; Saini, R.; Ballini, A.; Inchingolo, F. Oral Probiotics Influence Oral and Respiratory Tract Infections in Pediatric Population: A Randomized Double-Blinded Placebo-Controlled Pilot Study. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 8034–8041. [Google Scholar] [CrossRef]
- Punhagui, M.-F.; Jussiani, E.-I.; Andrello, A.-C.; Favaro, J.-C.; Guiraldo, R.-D.; Lopes, M.-B.; Berger, S.-B. Effect of Application Time and Concentration of Silver Diamine Fluoride on the Enamel Remineralization. J. Clin. Exp. Dent. 2021, 13, e653–e658. [Google Scholar] [CrossRef]
- Marchetti, E.; Ratta, S.; Mummolo, S.; Tecco, S.; Pecci, R.; Bedini, R.; Marzo, G. Mechanical Reliability Evaluation of an Oral Implant-Abutment System According to UNI EN ISO 14801 Fatigue Test Protocol. Implant Dent. 2016, 25, 613–618. [Google Scholar] [CrossRef]
- Dentinal Substrate Variability and Bonding Effectiveness: SEM Investigation. Available online: https://pubmed.ncbi.nlm.nih.gov/32064835/ (accessed on 22 January 2024).
- Libonati, A.; Di Taranto, V.; Agostini, C.D.; Santoro, M.M.; Di Carlo, D.; Ombres, D.; Gallusi, G.; Favalli, C.; Marzo, G.; Campanella, V. Comparison of Coronal Leakage of Different Root Canal Filling Techniques: An Ex Vivo Study. J. Biol. Regul. Homeost. Agents 2018, 32, 397–405. [Google Scholar] [PubMed]
- Haiat, A.; Ngo, H.C.; Samaranayake, L.P.; Fakhruddin, K.S. The Effect of the Combined Use of Silver Diamine Fluoride and Potassium Iodide in Disrupting the Plaque Biofilm Microbiome and Alleviating Tooth Discoloration: A Systematic Review. PLoS ONE 2021, 16, e0252734. [Google Scholar] [CrossRef] [PubMed]
- Ammar, N.; El-Tekeya, M.M.; Essa, S.; Essawy, M.M.; Talaat, D.M. Antibacterial Effect and Impact on Caries Activity of Nanosilver Fluoride and Silver Diamine Fluoride in Dentin Caries of Primary Teeth: A Randomized Controlled Clinical Trial. BMC Oral Health 2022, 22, 657. [Google Scholar] [CrossRef] [PubMed]
- Knight, G.M.; McIntyre, J.M.; Craig, G.G.; Mulyani, N.; Zilm, P.S.; Gully, N.J. An in Vitro Model to Measure the Effect of a Silver Fluoride and Potassium Iodide Treatment on the Permeability of Demineralized Dentine to Streptococcus Mutans. Aust. Dent. J. 2005, 50, 242–245. [Google Scholar] [CrossRef] [PubMed]
- Tanzer, J.M.; Livingston, J.; Thompson, A.M. The Microbiology of Primary Dental Caries in Humans. J. Dent. Educ. 2001, 65, 1028–1037. [Google Scholar] [CrossRef] [PubMed]
- Mummolo, S.; Tieri, M.; Nota, A.; Caruso, S.; Darvizeh, A.; Albani, F.; Gatto, R.; Marzo, G.; Marchetti, E.; Quinzi, V.; et al. Salivary Concentrations of Streptococcus Mutans and Lactobacilli during an Orthodontic Treatment. An Observational Study Comparing Fixed and Removable Orthodontic Appliances. Clin. Exp. Dent. Res. 2020, 6, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Mummolo, S.; Nota, A.; Albani, F.; Marchetti, E.; Gatto, R.; Marzo, G.; Quinzi, V.; Tecco, S. Salivary Levels of Streptococcus Mutans and Lactobacilli and Other Salivary Indices in Patients Wearing Clear Aligners versus Fixed Orthodontic Appliances: An Observational Study. PLoS ONE 2020, 15, e0228798. [Google Scholar] [CrossRef] [PubMed]
- Nagireddy, V.R.; Reddy, D.; Kondamadugu, S.; Puppala, N.; Mareddy, A.; Chris, A. Nanosilver Fluoride—A Paradigm Shift for Arrest in Dental Caries in Primary Teeth of Schoolchildren: A Randomized Controlled Clinical Trial. Int. J. Clin. Pediatr. Dent. 2019, 12, 484–490. [Google Scholar] [CrossRef]
- Mubaraki, H.; Ingle, N.A.; Baseer, M.A.; AlMugeiren, O.M.; Mubaraki, S.; Cicciù, M.; Minervini, G. Effect of Silver Diamine Fluoride on Bacterial Biofilms-A Review Including In Vitro and In Vivo Studies. Biomedicines 2023, 11, 1641. [Google Scholar] [CrossRef]
- Roberts, A.; Bradley, J.; Merkley, S.; Pachal, T.; Gopal, J.V.; Sharma, D. Does Potassium Iodide Application Following Silver Diamine Fluoride Reduce Staining of Tooth? A Systematic Review. Aust. Dent. J. 2020, 65, 109–117. [Google Scholar] [CrossRef]
- Comparison between Rapid and Slow Palatal Expansion: Evaluation of Selected Periodontal Indices. Available online: https://pubmed.ncbi.nlm.nih.gov/25128278/ (accessed on 22 January 2024).
- Paediatric Orthodontics. Part 4: SEC III Protocol in Class III Malocclusion. Available online: https://pubmed.ncbi.nlm.nih.gov/31850779/ (accessed on 22 January 2024).
- Yin, I.X.; Zhang, J.; Zhao, I.S.; Mei, M.L.; Li, Q.; Chu, C.H. The Antibacterial Mechanism of Silver Nanoparticles and Its Application in Dentistry. Int. J. Nanomed. 2020, 15, 2555–2562. [Google Scholar] [CrossRef] [PubMed]
- Almuqrin, A.; Kaur, I.P.; Walsh, L.J.; Seneviratne, C.J.; Zafar, S. Amelioration Strategies for Silver Diamine Fluoride: Moving from Black to White. Antibiotics 2023, 12, 298. [Google Scholar] [CrossRef] [PubMed]
- Duangthip, D.; Chu, C.H.; Lo, E.C.M. A Randomized Clinical Trial on Arresting Dentine Caries in Preschool Children by Topical Fluorides--18 Month Results. J. Dent. 2016, 44, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Guntermann, L.; Rohrbach, A.; Schäfer, E.; Dammaschke, T. Remineralization and Protection from Demineralization: Effects of a Hydroxyapatite-Containing, a Fluoride-Containing and a Fluoride- and Hydroxyapatite-Free Toothpaste on Human Enamel in Vitro. Head Face Med. 2022, 18, 26. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, S.; Mummolo, S.; Varvara, G.; Marchetti, E.; Continenza, M.A.; Marzo, G.; Macchiarelli, G. Bio-Morphological Evaluation of Periodontal Ligament Fibroblasts on Mineralized Dentin Graft: An in Vitro Study. J. Biol. Regul. Homeost. Agents 2019, 33, 275–280. [Google Scholar]
- Periodontal Status of Buccally and Palatally Impacted Maxillary Canines after Surgical-Orthodontic Treatment with Open Technique. Available online: https://pubmed.ncbi.nlm.nih.gov/29984786/ (accessed on 22 January 2024).
- Bernardi, S.; Mummolo, S.; Ciavarelli, L.M.; Li Vigni, M.; Continenza, M.A.; Marzo, G. Cone Beam Computed Tomography Investigation of the Antral Artery Anastomosis in a Population of Central Italy. Folia Morphol. 2016, 75, 149–153. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study/ Region | Age Range | Treated Teeth | Follow Up/ Months | SDF Group(s)/ Sample Size | Other Group(s)/ Sample Size | Effectiveness of SDF in Arresting/ Preventing Decays | Effectiveness of Other Materials in Arresting/ Preventing Decays |
|---|---|---|---|---|---|---|---|
| Ruff et al., 2023 United States [60] | 5–13 years | Primary and permanent teeth | 24 months | 38% SDF/413 patients | NA | Arrest rate for the experimental treatment was considerably higher than for the active control-(80%) | 50% |
| Phonghanyudh et al., 2022 Thailand [49] | 1–3 years | Primary teeth | 18 months | 147 patieints | 143 patients | 59.1% | 58.1% |
| Cleary J. et al., 2022 United States [58] | 2–10 years | 1 randomly selected primary tooth per child, with at least 1/3 of the crown remaining, no signs of periapical infection and whose anticipated exfoliation > 12 months | 12 months | 38% SDF (2× per year)/ 40 patients | Conventional restorative treatment; Material selected, following AAPD guidelines 29 patients | At 12 months: 74% At 6 months: 57% Minor failures: 65% Major failures: 13% | Minor failures: 23% Major failures: 3% |
| Ballikaya E. et al., 2021 Turkey [57] | 6–13 years | Permanent molars; -at least 2 first permanent molars that have erupted -MIH/hypomineralization -ICDAS lesions 1–2 | 12 months | Group 1: 38%SDF (2× per year)/45 patients Group 2: 38% SDF + ART (SMART)/+ GIC/ 45 patients | Cumulative rates at 12 months-88.7% for the occlusal surfaces and 58.8% for the palatal surfaces | ||
| Abdellatif HM et al., 2021 Saudi Arabia [51] | 3–8 years | Primary teeth | 12 months | 38% SDF(2×/year) 27 patients 82 carious lesions | ART—cavity restored with GIC + Protective varnish 26 patients/85 carious lesions | At 6 months: 100% At 12 months: 99% | At 6 months: 96% At 12 months: 94% |
| Turton B. et al., 2021 Cambodia [11] | 3–11 years | At least one active decay in deciduous teeth without pulp exposure | 12 months | Group 1: 38% SDF/(2× per year)/66 patients Group 2: 38% SDF + KI/(2× per year)/ 110 patients | Group 3: AgF/85 children Group 4: AgF + KI/ 57 children | Group 1: 77.3% Group 2: 65.4% | Group 3: 75.3% Group 4: 51.2% |
| Gao Sherry Shiqian et al., 2020 Hong Kong [43] | 3–4 years | Primary teeth with ECC | 30 months | 38% SDF/500 patients | 25% AgNO3 +5% NaF/495 patients | At 12 months: 60% At 30 months: 68.9% | At 12 months: 62.4% At 30 months: 70.6% |
| Jiang M. et al., 2020 Hong Kong [8] | 3–4 years | Primary teeth | 24 months | 38% SDF (10 s) +GIC restorations (10 weeks after)/ 88 patients | Tonic water as Placebo +GIC restorations (10 weeks after)/84 patients | 57.8% at 6 months 46.3% at 12 months 37.2% at 18 months 28.8% at 24 months | 60.3% at 6 months 48.4% at 12 months 33.8% at 18 months 26.9% at 24 months |
| Mabangkhru S. et al., 2020 Thailand [47] | 1–3 years | Primary teeth | 12 months | 38% SDF (10 s)/ 130 patients | 5% NaF Varnish/133 patients | 35.7% | 20.9% |
| Pisarnturakit P. et Detsomboonrat P., 2020 Thailand [48] | 3–5 years | Primary teeth | 24 months | HRI Group: 38% SDF +Fluoride Varnish every 6 months | HRB Group LRB Group/ No intervention | Percentage of new caries in HRI group increased from 40% (at 6 months) to 65.7% (at 24 months). | Percentage of new caries in HRB group increased from 45.9% (at 6 months) to 75% (at 24 months). |
| Vollú AL et al., 2019 Brazil [55] | 2–5 years | Occlusal decays on the primary molars | 12 months | 30% SDF (3 min./2×/year)/34 patients | ART with GIC /33 patients | 84.6% | 82.7% |
| Tirupathi S. et al., 2019 India [52] | 6–10 years | Primary molars | 12 months | 38% SDF (1/year)/24 patients | 5% NSSF (1×/year)/ 23 patients | 71.05% | 77% |
| Duangthip D. et al., 2018 Hong Kong [44] | 3–4 years | Primary teeth | 30 months | Group 1: 30% SDF (1×/year)/101 patients Group 2:30% SDF (3 applications at weekly intervals/year)/102 patients | Group 3: 5% NaF Varnish (3 applications at weekly intervals/year) | Group 1: 45% Group 2: 44% | Group 3: 51% ICDAS: 3–4 |
| Fung MHT et al., 2018 Hong Kong [45] | 3–4 years | Primary teeth | 30 months | Group 1: 12% SDF (1×/year)/198 patients Group 2: 12% SDF (2×/year)/203 patients Group 3: 38% SDF (1×/year)/202 patients Group 4:38% SDF (2×/year)/196 patients | Group 1: 55.2% Group 2: 58.6% Group 3: 66.9% Group 4: 75.7% | ||
| Monse B. et al., 2012 Filipine [54] | 6–8 years | First permanentmolars: without dentinal carious lesions visible at the occlusal surface | 18 months | 38% SDF with tannic acid to precipitate silver (1×/year)/91 patients 38% SDF (1×/year)/ 139 patients | ART sealant: 90 patients No Treatment: 45 patients | 91% 87.5% | 99% 93.8% |
| Zhi QH et al., 2012 China [50] | 3–4 years | Primary teeth | 24 months | Group 1: 38% SDF (1×/year)/91 patients Group 2: 38% SDF (2×/year)/ 59 patients | Group 3: GIC | Group 1: 79.2% Group 2: 90.7% | Group 3: 81.8% |
| Liu BY et al., 2012 Hong Kong [46] | 9 years | First permanent molar | 24 months | 38% SDF (1×/year)/ 121 patients | Resin Sealant/ 121 patients 5% NaF Varnish (2×/year)/ 116 patients Placebo-Water (1×/year)/ 124 patients | 87.8% | Sealant Group: 92.6% NaF Group: 87.2% Placebo: 83.1% |
| Dos Santos VE Jr et al., 2012 Brazil [56] | 5–6 years | Primary molars | 12 months | 30% SDF/48 patients | IRT with GIC/43 patients | 66.9% | 38.6% |
| Joshi et al., 2023 India [53] | 2–6 years | Primary teeth | 1, 3, 6 months | 24 patients | SDF | 96% | |
| Duangthip et al., 2016 Hong Kong [64] | 3–4 years | Primary teeth | 18 months | 304 patients: Group 1 receives 30% silver diamine fluoride (SDF) annually, Group 2 undergoes three weekly applications of 30% SDF | Group 3 three weekly applications of 5% sodium fluoride (NaF) varnish. | Both SDF protocols are more effective than intensive NaF varnish applications in stopping caries | |
| Antonioni et al., 2019 United States [61] | 2–17 years | Primary and permanent teeth | 582 | SDF |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muntean, A.; Mzoughi, S.M.; Pacurar, M.; Candrea, S.; Inchingolo, A.D.; Inchingolo, A.M.; Ferrante, L.; Dipalma, G.; Inchingolo, F.; Palermo, A.; et al. Silver Diamine Fluoride in Pediatric Dentistry: Effectiveness in Preventing and Arresting Dental Caries—A Systematic Review. Children 2024, 11, 499. https://doi.org/10.3390/children11040499
Muntean A, Mzoughi SM, Pacurar M, Candrea S, Inchingolo AD, Inchingolo AM, Ferrante L, Dipalma G, Inchingolo F, Palermo A, et al. Silver Diamine Fluoride in Pediatric Dentistry: Effectiveness in Preventing and Arresting Dental Caries—A Systematic Review. Children. 2024; 11(4):499. https://doi.org/10.3390/children11040499
Chicago/Turabian StyleMuntean, Alexandrina, Soundouss Myriam Mzoughi, Mariana Pacurar, Sebastian Candrea, Alessio Danilo Inchingolo, Angelo Michele Inchingolo, Laura Ferrante, Gianna Dipalma, Francesco Inchingolo, Andrea Palermo, and et al. 2024. "Silver Diamine Fluoride in Pediatric Dentistry: Effectiveness in Preventing and Arresting Dental Caries—A Systematic Review" Children 11, no. 4: 499. https://doi.org/10.3390/children11040499