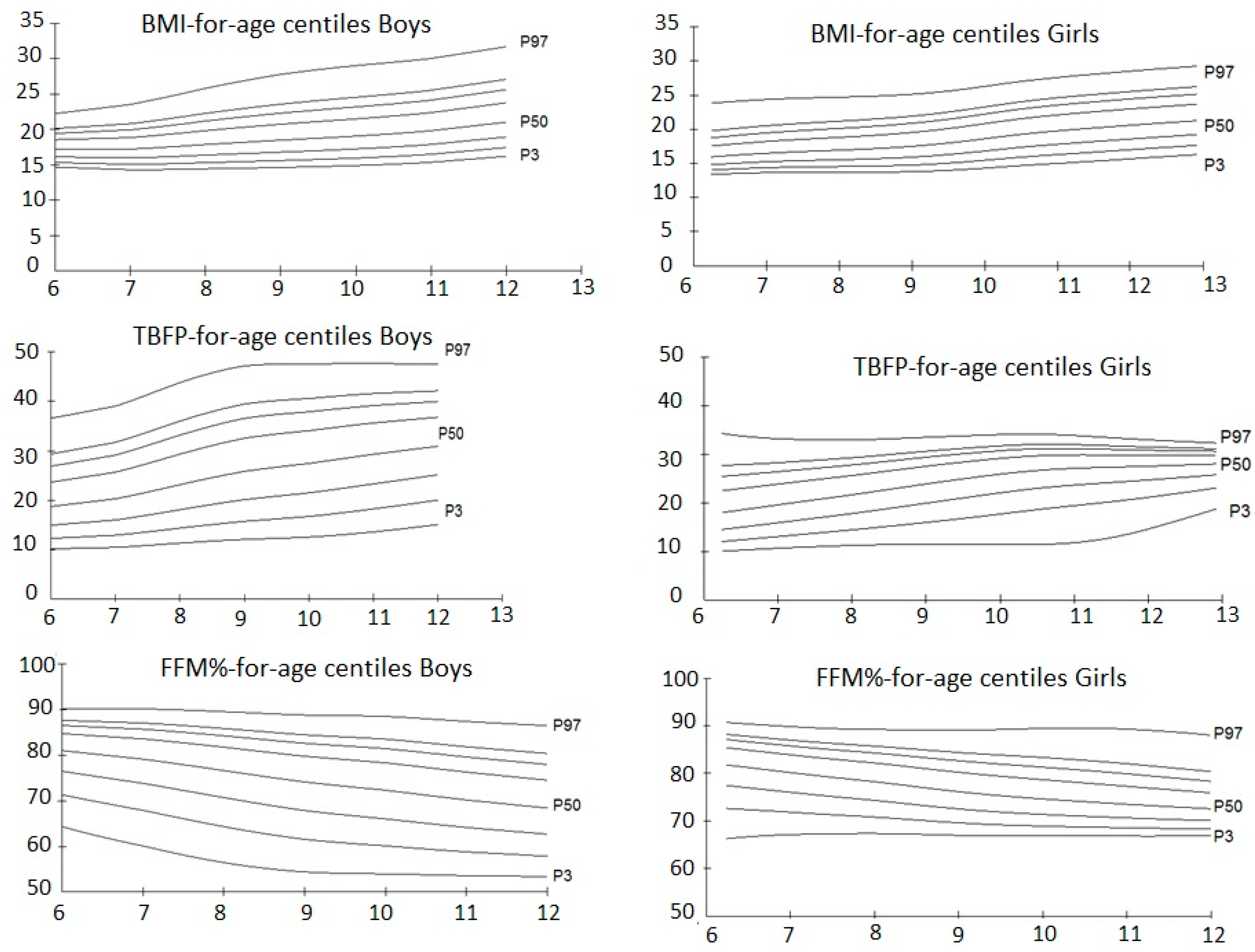
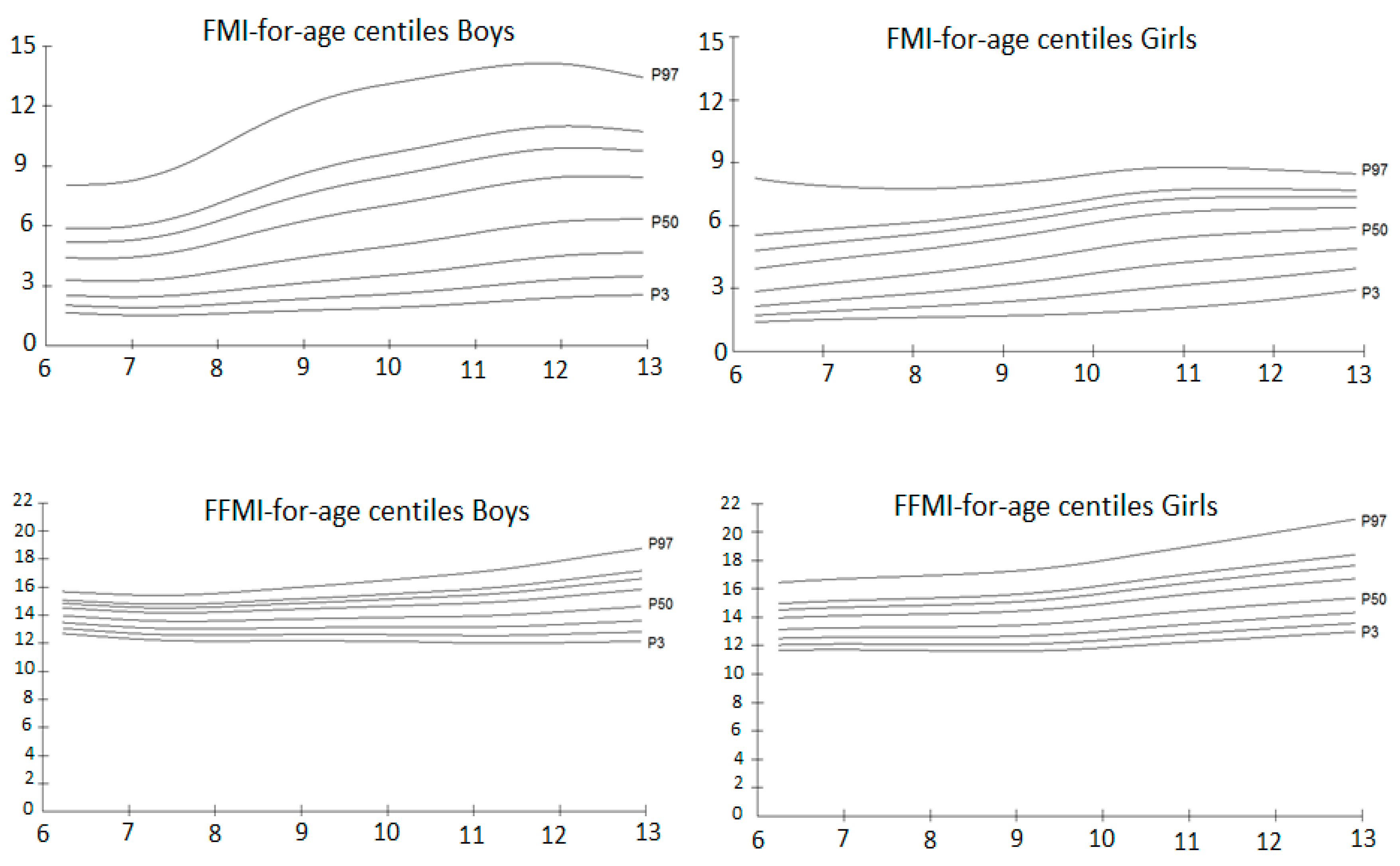
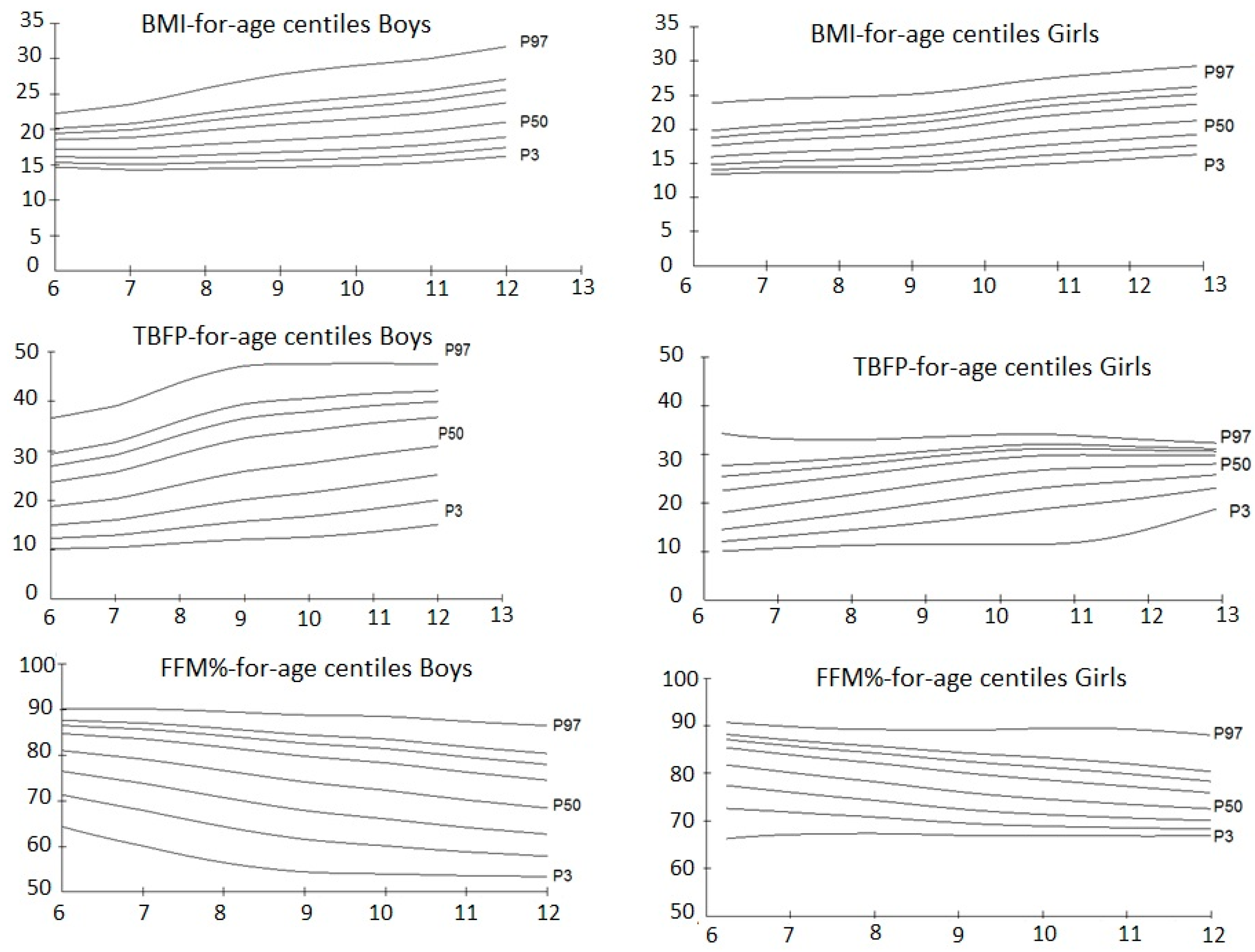
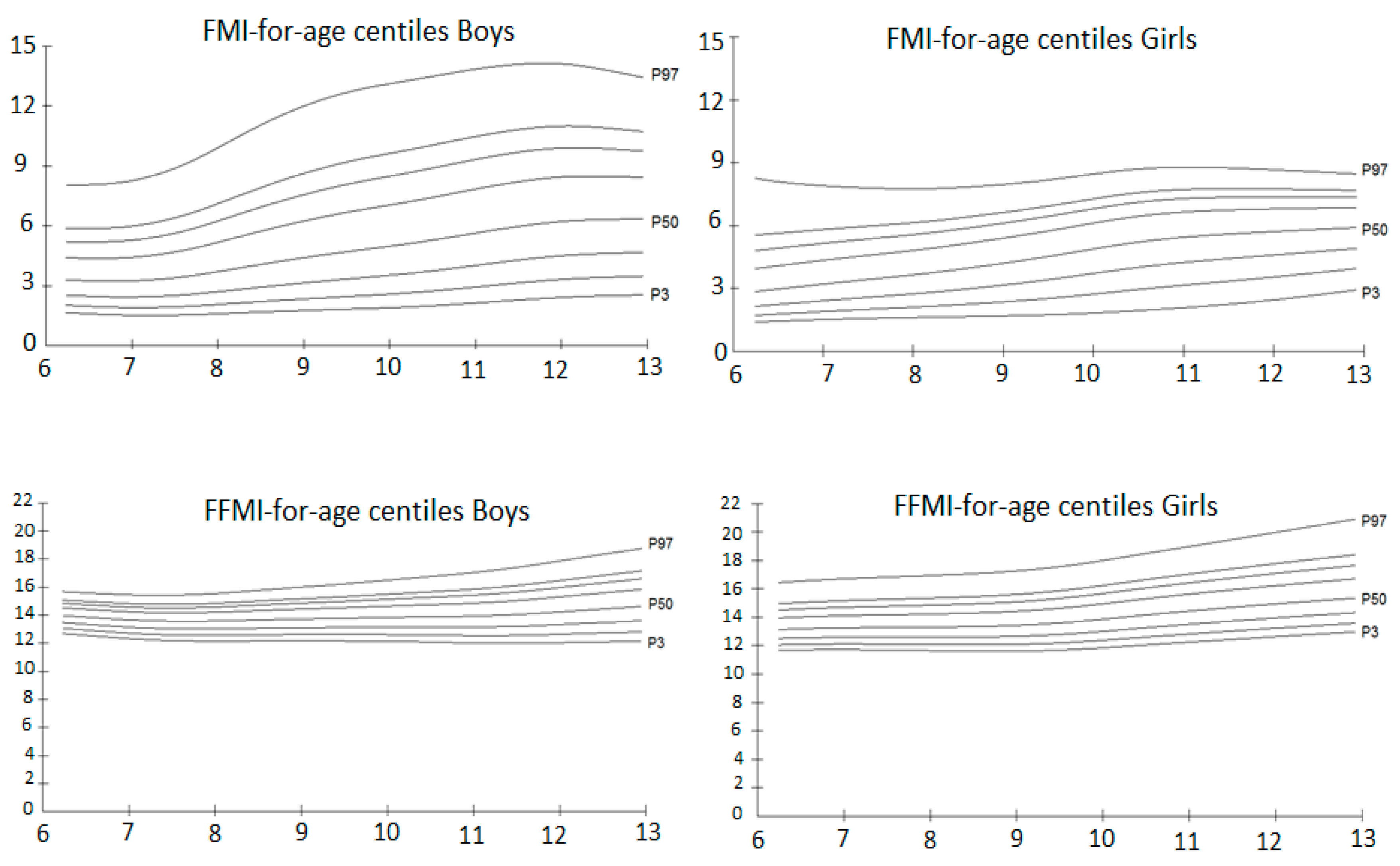
Smoothed Body Composition Percentiles Curves for Mexican Children Aged 6 to 12 Years

 ,
,
Abstract
:1. Background
2. Methods
2.1. Subjects
2.2. Body Composition
- FMI = FM/height2 (kg/m2) where, FM = (TBFP × weight)/100
- FFMI = BMI − FMI (kg/m2)
- Note that, BMI (kg/m2) = FMI (kg/m2) + FFMI (kg/m2)
2.3. Statistical Analysis and Centile Curves
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Ethics Approval
References
- World Health Organization (WHO). Obesity and Overweight, Fact Sheet, Updated June 2017. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 29 September 2016).
- Ministry of Health. National Health and Nutrition Survey 2016. In Final Results Report; National Institute of Public Health: Cuernavaca, Mexico, 2016. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Body Mass Index: Considerations for Practitioners; CDC: Atlanta, GA, USA, 2016.
- Wells, J.C.K. Towards Body Composition Reference Data for Infants, Children, and Adolescents. Adv. Nutr. 2014, 5, 320S–329S. [Google Scholar] [CrossRef] [PubMed]
- VanItallie, T.B.; Yang, M.; Heymsfield, S.B.; Funk, R.C.; Boileau, R.A. Height-normalized indices of the body’s fat-free mass and fat mass: Potentially useful indicators of nutritional status. Am. J. Clin. Nutr. 1990, 52, 953–959. [Google Scholar] [PubMed]
- Mei, Z.; Grummer-Strawn, L.M.; Pietrobelli, A.; Goulding, A.; Goran, M.I.; Dietz, W.H. Validity of body mass index compared with other body-composition screening indexes for the assessment of body fatness in children and adolescents. Am. J. Clin. Nutr. 2002, 75, 978–985. [Google Scholar] [PubMed]
- Rogol, A.D.; Roemmich, J.N.; Clark, P.A. Growth at puberty. J. Adolesc. Health 2002, 31, 192–200. [Google Scholar] [CrossRef]
- Kim, K.; Yun, S.H.; Jang, M.J.; Oh, K.W. Body Fat Percentile Curves for Korean Children and Adolescents: A Data from the Korea National Health and Nutrition. J. Korean Med. Sci. 2013, 28, 443–449. [Google Scholar] [CrossRef]
- Jeddi, M.; Dabbaghmanesh, M.H.; Ranjbar Omrani, G.; Ayatollahi, S.M.; Bagheri, Z.; Bakhshayeshkaram, M. Body Composition Reference Percentiles of Healthy Iranian Children and Adolescents in southern Iran. Arch. Iran. Med. 2014, 17, 661–669. [Google Scholar] [PubMed]
- Cintra Ide, P.; Ferrari, G.L.; Soares, A.C.; Passos, M.A.; Fisberg, M.; Vitalle, M.S. Body fat percentiles of Brazilian adolescents according to age and sexual maturation: A cross-sectional study. BMC Pediatr. 2013, 13, 96. [Google Scholar] [CrossRef] [Green Version]
- Escobar-Cardozo, G.; Correa-Bautista, J.E.; González-Jiménez, E.; Schmidt-RioValle, J.; Ramírez-Vélez, R. Percentiles of body fat measured by bioelectrical impedance in children and adolescents from Bogota (Colombia): The FUPRECOL study. Arch. Argent. Pediatr. 2016, 114, 135–142. [Google Scholar] [PubMed]
- Orta Duarte, M.; Flores Ruelas, Y.; López-Alacaraz, F.; Del Toro-Equihua, M.; Sánchez-Ramírez, C.A. Correlation between percentage of body fat measured by the Slaughter equation and bio impedance analysis technique in Mexican school children. Nut Hosp. 2014, 29, 88–93. [Google Scholar]
- Kriemler, S.; Puder, J.; Zahner, L.; Roth, R.; Meyer, U.; Bedogni, G. Estimation of percentage body fat in 6- to 13-year-old children by skinfold thickness, body mass index and waist circumference. Br. J. Nutr. 2010, 104, 1565–1572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deurenberg, P.; Pieters, J.J.L.; Hautvast, J.G.A. The assessment of the body fat percentage by skinfold thickness measurements in childhood and young adolescence. Br. J. Nutr. 1990, 63, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.C.K.; Coward, W.A.; Cole, T.J.; Davies, P.S.W. The contribution of fat and fat-free tissue to body mass index in contemporary children and the reference child. Int. J. Obes. Relat. Metab. Disord. 2012, 26, 1323–1328. [Google Scholar] [CrossRef] [PubMed]
- Slaughter, M.H.; Lohman, T.G.; Boileau, R.A.; Horswill, C.A.; Stillman, R.J.; Van Loan, M.D.; Bemben, D.A. Skinfold equations for estimation of body fatness in children and youth. Hum. Biol. 1988, 60, 709–723. [Google Scholar] [PubMed]
- Wells, J.C.; Fewtrell, M.S. Measuring body composition. Arch. Dis. Child. 2006, 91, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Green, P.J. Smoothing reference centile curves: The LMS method and penalized likelihood. Stat. Med. 1992, 11, 1305–1319. [Google Scholar] [CrossRef] [PubMed]
- Del Rio-Navarro, B.E. Mexican anthropometric percentiles for ages 10–18. Eur. J. Clin. Nutr. 2007, 61, 963–975. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J. Mexican anthropometry percentiles and the LMS method. Eur. J. Clin. Nutr. 2009, 63, 588. [Google Scholar] [CrossRef] [PubMed]
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Datta-Banik, S.; Azcorra, H.; Valentín, G.; Falfán, I.; Dickinson, F. Height, Weight and Body Mass Index by Age and Sex in Children Aged 4 to 6 Years in Merida, Mexico, Comparisons to International References After Normalization with LMS. Coll. Antropol. 2014, 4, 1163–1169. [Google Scholar]
- Carolina Avalos, F. Waist circumference percentiles in children and adolescents between 6 and 14 years from Santiago, Chile. Endocrinol. Nutr. 2012, 59, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Laurson, K.R.; Eisenmann, J.C.; Welk, G.J. Body Fat Percentile Curves for U.S. Children and Adolescents. Am. J. Prev. Med. 2011, 41, S87–S92. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Wilson, J.; Durnin, J.V. Determination of body composition from skinfold thickness: Validation study. Arch. Dis. Child. 1995, 73, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Williams, P. Body Fatness and Risk for Elevated Blood Pressure, Total Cholesterol, and Serum Lipoprotein Ratios in Children and Adolescents. Am. J. Public Health 1992, 82, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Peltz, G.; Aguirre, M.T.; Sanderson, M.; Fadden, M.K. The role of fat mass index in determining obesity. Am. J. Hum. Boil. 2010, 22, 639–647. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Boys (n = 2026) | Age 6 (n = 306) | Age 7 (n = 286) | Age 8 (n = 295) | Age 9 (n = 279) | Age 10 (n = 239) | Age 11 (n = 260) | Age 12 (n = 361) |
| Weight (kg) | 25.1 ± 4.5 ‡ | 26.2 ± 4.1 * | 31.9 ± 7.1 ‡ | 35.2 ± 9.0 ** | 39.4 ± 9.5 ** | 44.2 ± 9.5 | 50.4 ± 11.6 |
| Height (cm) | 119.1 ± 4.9 ‡ | 122.7 ± 4.5 * | 129.8 ± 5.2 ‡ | 133.8 ± 5.9 | 140.0 ± 6.2 ** | 147.7 ± 6.4 | 151.2 ± 7.0 |
| Waist circunference (cm) | 58.1 ± 6.0 ‡ | 58.6 ± 5.7 ** | 64.3 ± 9.3 ‡ | 66.9 ± 10.5 ‡ | 69.7 ± 10.3 | 68.9 ± 9.4 | 76.5 ± 11.5 ‡ |
| BMI (kg/m2) | 17.6 ± 2.1 ‡ | 17.3 ± 2.0 | 18.8 ± 3.3 ‡ | 19.4 ± 3.6 ‡ | 20.0 ± 3.8 * | 20.2 ± 3.5 | 21.9 ± 4.3 |
| TBFP (%) | 20.2 ± 7.1 | 21.0 ± 6.7 | 24.6 ± 9.2 | 27.4 ± 9.7 ‡ | 27.6 ± 9.5 | 30.0 ± 8.9 ‡ | 31.1 ± 8.5 ‡ |
| TBFM (kg) | 5.3 ± 2.9 * | 5.7 ± 2.7 | 8.4 ± 4.9 ** | 10.4 ± 6.0 ‡ | 11.6 ± 6.5 | 13.9 ± 6.6 * | 16.3 ± 7.6 ‡ |
| FFM (%) | 79.8 ± 7.1 | 79.0 ± 6.7 | 75.4 ± 9.1 | 72.6 ± 9.7 ‡ | 72.4 ± 9.5 | 70.0 ± 9.0 ‡ | 69.0 ± 8.4 ‡ |
| FFM (kg) | 19.8 ± 2.1 ‡ | 20.4 ± 1.9 ** | 23.5 ± 2.8 ‡ | 24.8 ± 3.4 | 27.8 ± 4.0 ‡ | 30.3 ± 4.2 ‡ | 34.1 ± 5.6 |
| FMI (kg/m2) | 3.7 ± 1.8 | 3.8 ± 1.6 | 4.9 ± 2.7 * | 5.6 ± 3.0 ‡ | 5.8 ± 3.0 | 6.3 ± 2.8 ** | 7.1 ± 3.1 ‡ |
| FFMI (kg/m2) | 13.9 ± 0.9 ‡ | 13.5 ± 0.8 ‡ | 13.9 ± 1.1 ‡ | 13.8 ± 1.0 | 14.1 ± 2.3 ** | 13.9 ± 1.3 ‡ | 14.8 ± 1.7 ** |
| Girls (n = 1488) | Age 6 (n = 261) | Age 7 (n = 278) | Age 8 (n = 195) | Age 9 (n = 266) | Age 10 (n = 200) | Age 11 (n = 174) | Age 12 (n = 114) |
| Weight (kg) | 23.4 ± 5.2 ‡ | 26.2 ± 6.0 * | 29.1 ± 6.4 ‡ | 32.8 ± 7.3 ** | 40.9 ± 8.6 ** | 44.6 ± 10.1 | 48.1 ± 9.3 |
| Height (cm) | 117.3 ± 5.1 ‡ | 121.9 ± 5.1 * | 127.5 ± 4.7 ‡ | 133.5 ± 6.2 | 141.7 ± 6.4 ** | 147.0 ± 6.5 | 150.5 ± 6.8 |
| Waist circumference (cm) | 56.2 ± 7.6 ‡ | 58.2 ± 7.7 ** | 60.4 ± 7.6 ‡ | 62.8 ± 8.3 ‡ | 68.5 ± 8.5 | 68.8 ± 9.6 | 70.1 ± 8.1 ‡ |
| BMI (kg/m2) | 16.9 ± 2.6 ‡ | 17.5 ± 3.0 | 17.8 ± 3.0 ‡ | 18.2 ± 3.0 ‡ | 20.2 ± 3.3 * | 20.5 ± 3.7 | 21.1 ± 3.0 |
| TBFP (%) | 19.5 ± 6.0 | 21.3 ± 5.9 | 22.3 ± 5.9 | 23.8 ± 6.2 ‡ | 26.8 ± 5.1 | 25.9 ± 5.2 ‡ | 26.7 ± 4.3 ‡ |
| TBFM (kg) | 4.8 ± 2.5 * | 5.9 ± 2.9 | 6.8 ± 3.1 ** | 8.2 ± 3.5 ‡ | 11.2 ± 3.8 | 11.9 ± 4.4 * | 13.1 ± 3.9 ‡ |
| FFM (%) | 80.5 ± 5.9 | 78.7 ± 5.9 | 77.6 ± 5.8 | 76.1 ± 6.2 ‡ | 73.2 ± 5.1 | 74.1 ± 5.2 ‡ | 73.3 ± 4.3 ‡ |
| FFM (kg) | 18.6 ± 2.9 ‡ | 20.3 ± 3.4 ** | 22.3 ± 3.5 ‡ | 24.6 ± 4.0 | 29.6 ± 5.2 ‡ | 32.7 ± 6.1 ‡ | 35.0 ± 5.9 |
| FMI (kg/m2) | 3.4 ± 1.6 | 3.9 ± 1.7 | 4.1 ± 1.7 * | 4.5 ± 1.8 ‡ | 5.5 ± 1.7 | 5.5 ± 1.8 ** | 5.7 ± 1.5 ‡ |
| FFMI (kg/m2) | 13.4 ± 1.3 ‡ | 13.6 ± 1.5 ‡ | 13.7 ± 1.5 ‡ | 13.7 ± 1.5 | 14.7 ± 1.9 ** | 15.0 ± 2.1 ‡ | 15.4 ± 1.8 ** |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alpizar, M.; Peschard, V.-G.; Escalante-Araiza, F.; Altamirano-Bustamante, N.F.; Murata, C.; Arenas-Pérez, R.; Rodriguez-Ayala, E. Smoothed Body Composition Percentiles Curves for Mexican Children Aged 6 to 12 Years. Children 2017, 4, 112. https://doi.org/10.3390/children4120112
Alpizar M, Peschard V-G, Escalante-Araiza F, Altamirano-Bustamante NF, Murata C, Arenas-Pérez R, Rodriguez-Ayala E. Smoothed Body Composition Percentiles Curves for Mexican Children Aged 6 to 12 Years. Children. 2017; 4(12):112. https://doi.org/10.3390/children4120112
Chicago/Turabian StyleAlpizar, Melchor, Vanessa-Giselle Peschard, Fabiola Escalante-Araiza, Nelly F. Altamirano-Bustamante, Chiharu Murata, Ramón Arenas-Pérez, and Ernesto Rodriguez-Ayala. 2017. "Smoothed Body Composition Percentiles Curves for Mexican Children Aged 6 to 12 Years" Children 4, no. 12: 112. https://doi.org/10.3390/children4120112