
Differential Influences of Parenting Dimensions and Parental Physical Abuse during Childhood on Overweight and Obesity in Adolescents

Abstract
:1. Introduction
2. Material and Methods
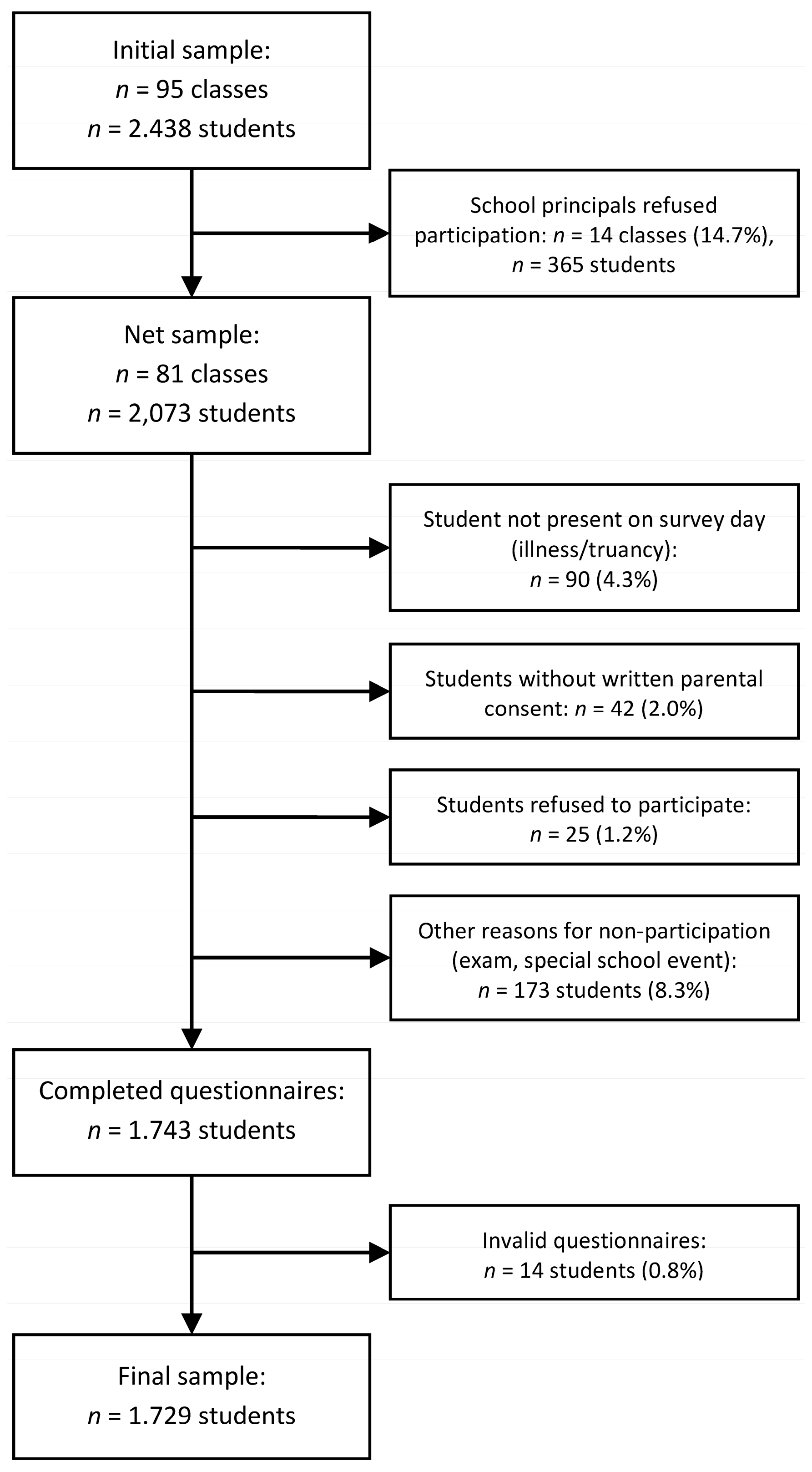
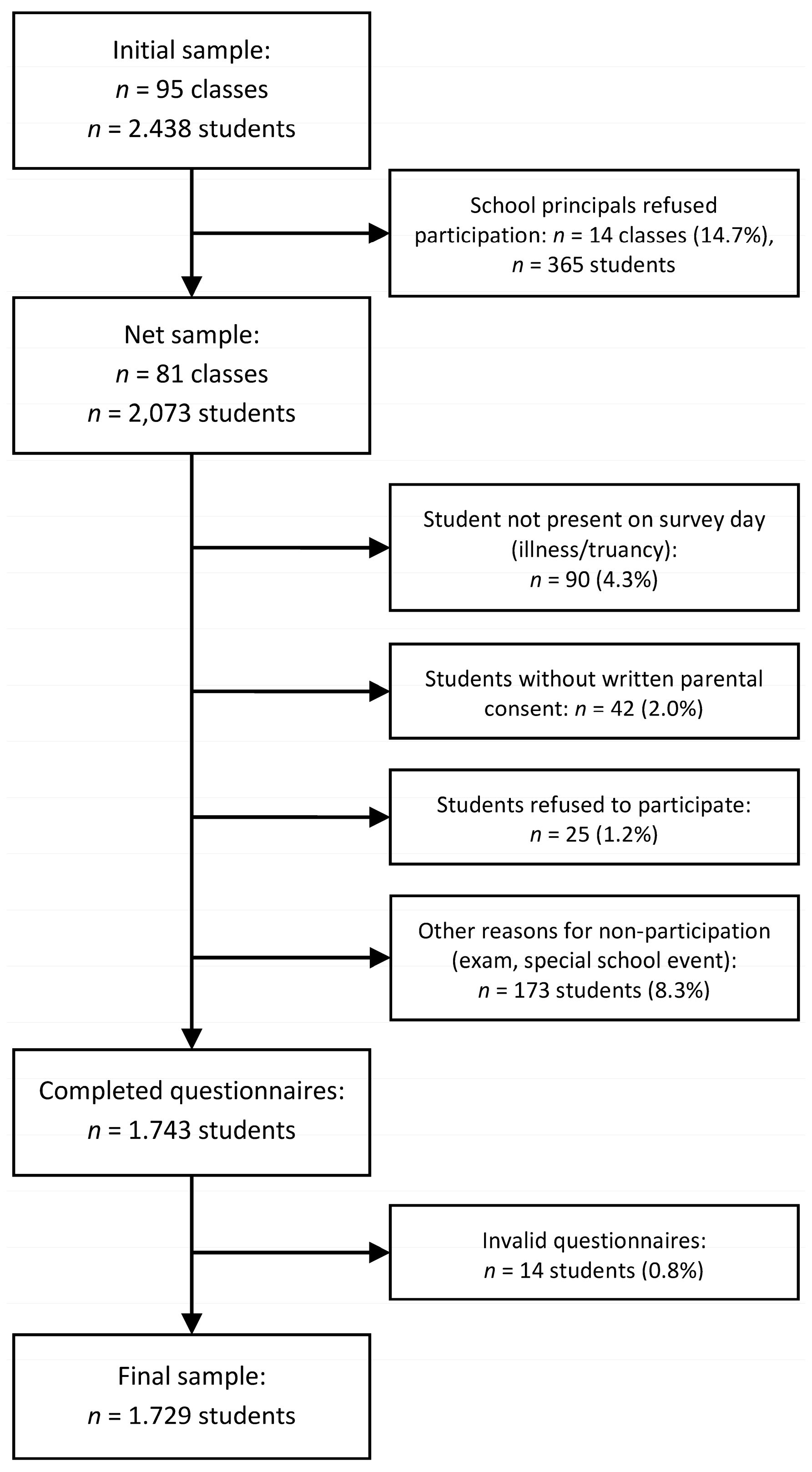
2.1. Participants and Procedure
2.2. Measures
2.2.1. Body Mass Index (BMI)
2.2.2. Parental Physical Abuse
2.2.3. Parenting Style—Warmth and Monitoring
2.2.4. Socioeconomic Status (SES) and Immigrant Backgrounds
2.3. Data Analysis
3. Results
3.1. Descriptive Statistics
3.2. Zero-Order Correlations
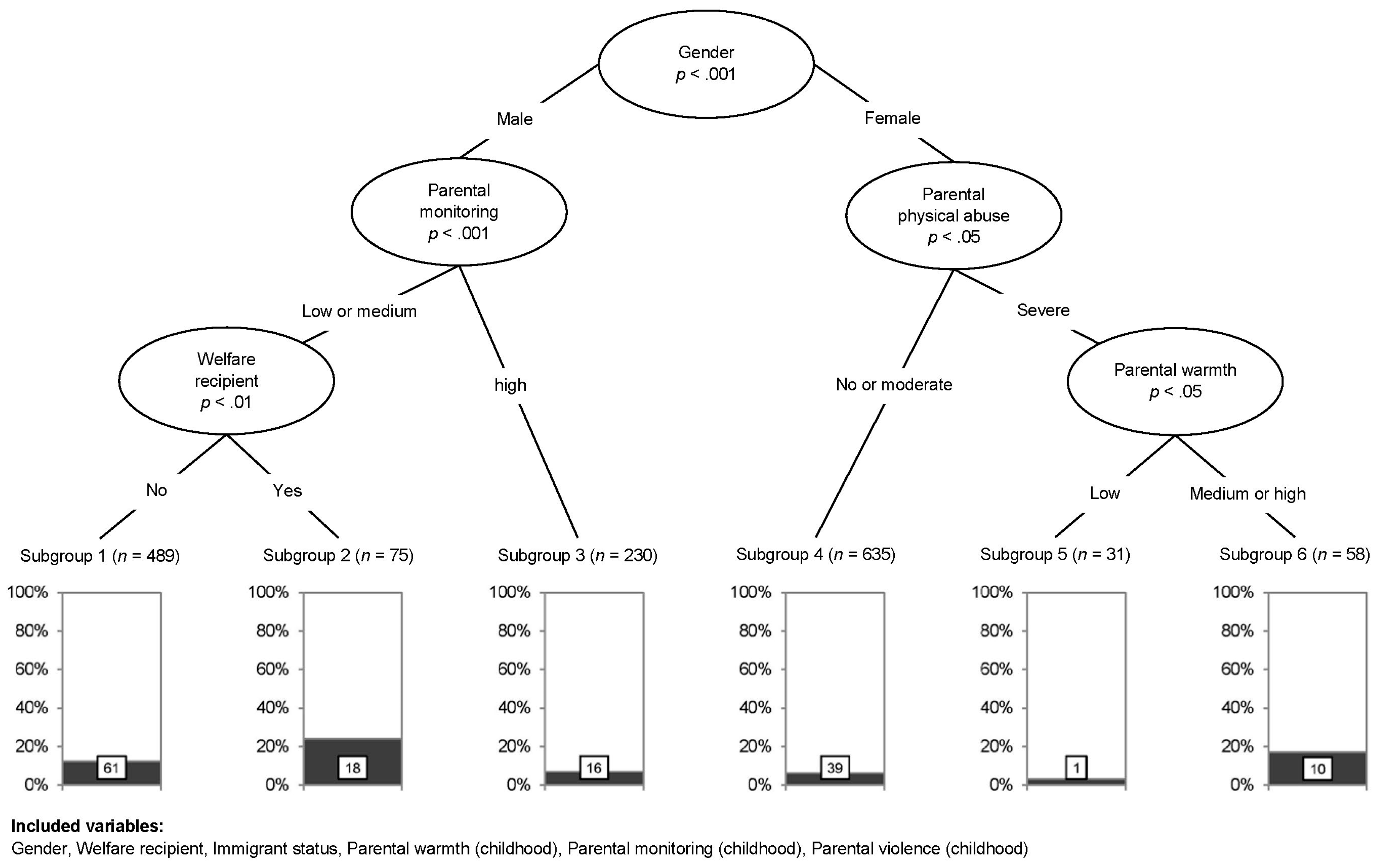
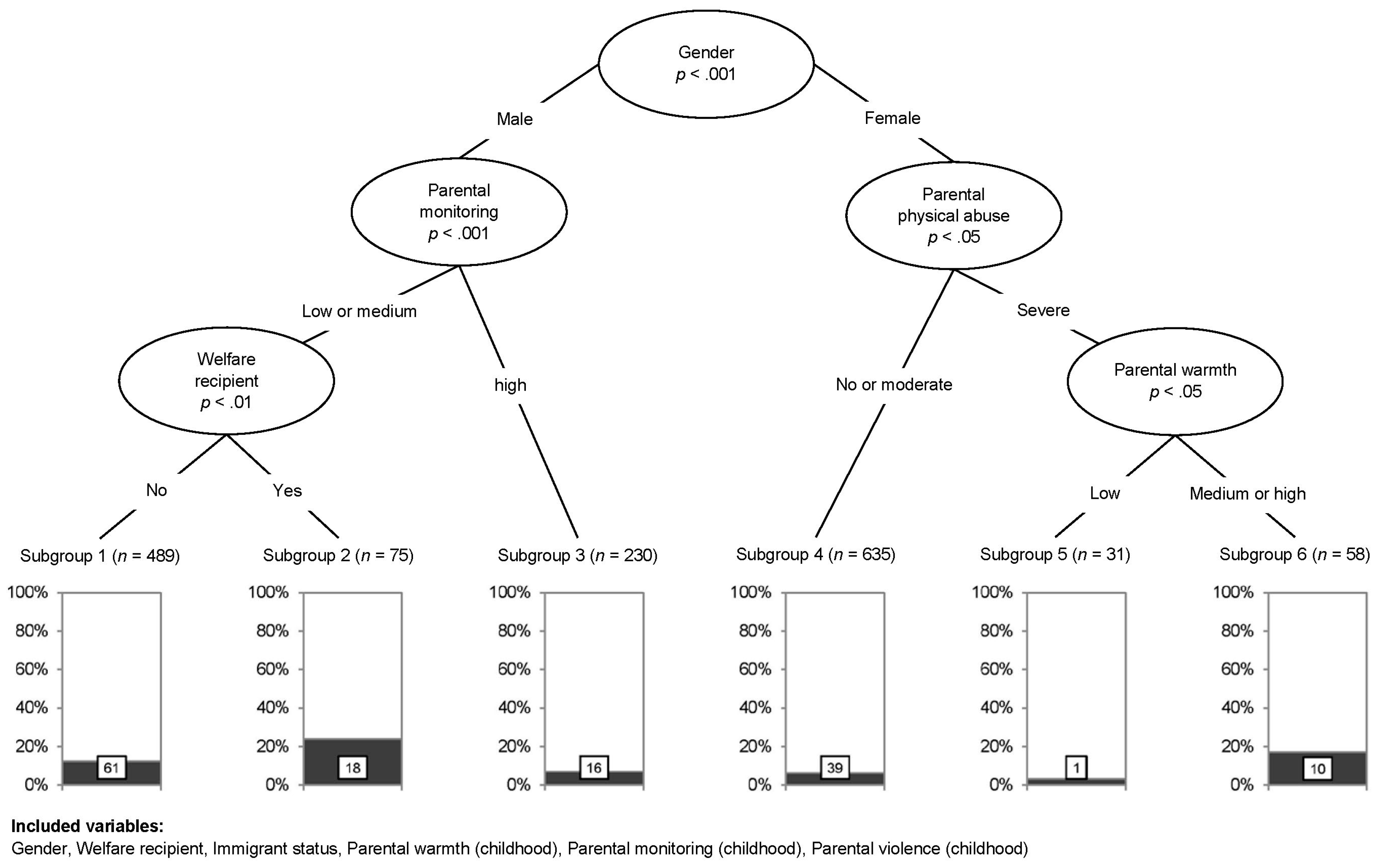
3.3. Non-Parametric Conditional Inference Trees
4. Discussion
Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kurth, B.-M.; Rosario, A.S. Übergewicht und adipositas bei kindern und jugendlichen in deutschland. Bundesgesundheitsblatt Gesundh. Gesundh. 2010, 53, 643–652. [Google Scholar] [CrossRef] [PubMed]
- Monasta, L.; Batty, G.D.; Cattaneo, A.; Lutje, V.; Ronfani, L.; Van Lenthe, F.J.; Brug, J. Early-life determinants of overweight and obesity: A review of systematic reviews. Obes. Rev. 2010, 11, 695–708. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M. Associations of general parenting and parent–child relationship with pediatric obesity: A meta-analysis. J. Pediatr. Psychol. 2014, 39, 381–393. [Google Scholar] [CrossRef] [PubMed]
- Davison, K.K.; Birch, L.L. Childhood overweight: A contextual model and recommendations for future research. Obes. Rev. 2001, 2, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Gerards, S.M.P.L.; Sleddens, E.F.C.; Dagnelie, P.C.; de Vries, N.K.; Kremers, S.P.J. Interventions addressing general parenting to prevent or treat childhood obesity. Int. J. Pediatr. Obes. 2011, 6, e28–e45. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.N.; Ashba, J.; Appugliese, D.P.; Kaciroti, N.; Corwyn, R.F.; Bradley, R.H.; Lumeng, J.C. Adolescent obesity and maternal and paternal sensitivity and monitoring. Int. J. Pediatr. Obes. 2011, 6, e457–e463. [Google Scholar] [CrossRef] [PubMed]
- Berge, J.M.; Wall, M.; Neumark-Sztainer, D.; Larson, N.; Story, M. Parenting style and family meals: Cross-sectional and 5-year longitudinal associations. J. Am. Diet. Assoc. 2010, 110, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Jago, R.; Davison, K.K.; Thompson, J.L.; Page, A.S.; Brockman, R.; Fox, K.R. Parental sedentary restriction, maternal parenting style, and television viewing among 10- to 11-year-olds. Pediatrics 2011, 128, e572–e578. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Harris, K.M.; Gordon-Larsen, P. Life course perspectives on the links between poverty and obesity during the transition to young adulthood. Popul. Res. Policy Rev. 2009, 28, 505–532. [Google Scholar] [CrossRef] [PubMed]
- Lansford, J.E.; Miller-Johnson, S.; Berlin, L.J.; Dodge, K.A.; Bates, J.E.; Pettit, G.S. Early physical abuse and later violent delinquency: A prospective longitudinal study. Child Maltreat 2007, 12, 233–245. [Google Scholar] [CrossRef] [PubMed]
- Donath, C.; Gräßel, E.; Baier, D.; Pfeiffer, C.; Bleich, S.; Hillemacher, T. Predictors of binge drinking in adolescents: Ultimate and distal factors-a representative study. BMC Public Health 2012, 12, 263. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, E.A.; Marks, N.F. Violence from parents in childhood and obesity in adulthood: Using food in response to stress as a mediator of risk. Soc. Sci. Med. 2009, 68, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Duncan, A.E.; Sartor, C.E.; Jonson-Reid, M.; Munn-Chernoff, M.A.; Eschenbacher, M.A.; Diemer, E.W.; Nelson, E.C.; Waldron, M.; Bucholz, K.K.; Madden, P.A.F.; et al. Associations between body mass index, post-traumatic stress disorder, and child maltreatment in young women. Child Abus. Negl. 2015. [Google Scholar] [CrossRef] [PubMed]
- Vámosi, M.; Heitmann, B.L.; Kyvik, K.O. The relation between an adverse psychological and social environment in childhood and the development of adult obesity: A systematic literature review. Obes. Rev. 2010, 11, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Danese, A.; Tan, M. Childhood maltreatment and obesity: Systematic review and meta-analysis. Mol. Psychiatry 2014, 19, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Hemmingsson, E.; Johansson, K.; Reynisdottir, S. Effects of childhood abuse on adult obesity: A systematic review and meta-analysis. Obes. Rev. 2014, 15, 882–893. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.H.; Miller, D.P. A longitudinal examination of childhood maltreatment and adolescent obesity: Results from the national longitudinal study of adolescent health (addhealth) study. Child Abus. Negl. 2012, 36, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Stensland, S.Ø.; Thoresen, S.; Wentzel-Larsen, T.; Dyb, G. Interpersonal violence and overweight in adolescents: The hunt study. Scand. J. Public Health 2015, 43, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Kromeyer-Hausschild, K.; Wabitsch, M.; Kunze, D.; Geller, F.; Geiß, H.C.; Hesse, V.; von Hippel, A.; Jaeger, U.; Johnsen, D.; Korte, W.; et al. Perzentile für den body-mass-index für das kindes- und jugendalter unter heranziehung verschiedener deutscher stichproben. Monatsschr Kinderheilkd. 2001, 149, 801–818. [Google Scholar] [CrossRef]
- Straus, M.A.; Hamby, S.; Warren, W. The Conflict Tactics Scales Handbook; WPS: Los Angeles, CA, USA, 2003. [Google Scholar]
- Loh, A.; Baier, D.; Donath, C.; Bleich, S.; Hillemacher, T.; Graessel, E. Binge drinking and experiences of victimization among adolescents: Findings of a nationwide representative study in germany. J. Public Health 2014, 22, 489–496. [Google Scholar] [CrossRef]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef] [PubMed]
- van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate imputation by chained equations. J. Stat. Softw. 2011, 45. [Google Scholar] [CrossRef]
- Hothorn, T.; Hornik, K.; Zeileis, A. Unbiased recursive partitioning: A conditional inference framework. J. Comp. Graph. Stat. 2006, 15, 651–674. [Google Scholar] [CrossRef]
- Strobl, C.; Malley, J.; Tutz, G. An introduction to recursive partitioning: Rationale, application, and characteristics of classification and regression trees, bagging, and random forests. Psychol. Meth. 2009, 14, 323. [Google Scholar] [CrossRef] [PubMed]
- Strasser, H.; Weber, C. On the Asymptotic Theory of Permutation Statistics; WU Vienna University of Economics and Business: Vienna, Austria, 1999. [Google Scholar]
- Hothorn, T.; Hornik, K.; Zeileis, A. Party: A Laboratory for Recursive Partytioning. Available online: http://cran.r-project.org/web/packages/party/party.pdf (accessed on 28 February 2017).
- Midei, A.J.; Matthews, K.A. Interpersonal violence in childhood as a risk factor for obesity: A systematic review of the literature and proposed pathways. Obes. Rev. 2011, 12, e159–e172. [Google Scholar] [CrossRef] [PubMed]
- Baier, D.; Pfeiffer, C.; Rabold, S. Jugendgewalt in deutschland. Befunde aus hell-und dunkelfelduntersuchungen unter besonderer berücksichtigung von geschlechterunterschieden. Kriminalistik 2009, 63, 323–333. [Google Scholar]
- MacMillan, H.L.; Fleming, J.E.; Streiner, D.L.; Lin, E.; Boyle, M.H.; Jamieson, E.; Duku, E.K.; Walsh, C.A.; Wong, M.Y.-Y.; Beardslee, W.R. Childhood abuse and lifetime psychopathology in a community sample. Am. J. Psychiatry 2001, 158, 1878–1883. [Google Scholar] [CrossRef] [PubMed]
- Dockray, S.; Susman, E.J.; Dorn, L.D. Depression, cortisol reactivity and obesity in childhood and adolescence. J. Adolesc. Health 2009, 45, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Harkness, K.L.; Stewart, J.G.; Wynne-Edwards, K.E. Cortisol reactivity to social stress in adolescents: Role of depression severity and child maltreatment. Psychoneuroendocrinology 2011, 36, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Fuemmeler, B.F.; Yang, C.; Costanzo, P.; Hoyle, R.H.; Siegler, I.C.; Williams, R.B.; Østbye, T. Parenting styles and body mass index trajectories from adolescence to adulthood. Health Psychol. 2012, 31, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Connell, L.E.; Francis, L.A. Positive parenting mitigates the effects of poor self-regulation on body mass index trajectories from ages 4–15 years. Health Psychol. 2014, 33, 757–764. [Google Scholar] [CrossRef] [PubMed]
- Herman, C.P.; Polivy, J. Sex and gender differences in eating behavior. In Handbook of Gender Research in Psychology: Volume 1: Gender Research in General and Experimental Psychology; Chrisler, J.C., McCreary, D.R., Eds.; Springer: New York, NY, USA, 2010; pp. 455–469. [Google Scholar]
- Avula, R.; Gonzalez, W.; Shapiro, C.; Fram, M.; Beets, M.; Jones, S.; Blake, C.; Frongillo, E. Positive parenting practices associated with subsequent childhood weight change. J. Prim. Prev. 2011, 32, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Olvera, N.; Power, T.G. Brief report: Parenting styles and obesity in mexican american children: A longitudinal study. J. Pediatr. Psychol. 2010, 35, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Baier, D.; Pfeiffer, C.; Simonson, J.; Rabold, S. Jugendliche in Deutschland als Opfer und Täter von Gewalt: Erster Forschungsbericht zum Gemeinsamen Forschungsprojekt des Bundesministerium des Innern und des kfn [Adolescents in Germany as Culprits and Victims of Violence: First Research Report on the Joint Research Project of the Federal Ministry of the Interior and the kfn]; 107; Kriminologisches Forschungsinstitut Niedersachsen: Hannover, Germany, 2009. [Google Scholar]
- Bowring, A.L.; Peeters, A.; Freak-Poli, R.; Lim, M.S.; Gouillou, M.; Hellard, M. Measuring the accuracy of self-reported height and weight in a community-based sample of young people. BMC Med. Res. Methodol. 2012, 12, 175. [Google Scholar] [CrossRef] [PubMed]
- Berge, J.M.; Wall, M.; Loth, K.; Neumark-Sztainer, D. Parenting style as a predictor of adolescent weight and weight-related behaviors. J. Adolesc. Health 2010, 46, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Mellin, A.E.; Neumark-Sztainer, D.; Story, M.; Ireland, M.; Resnick, M.D. Unhealthy behaviors and psychosocial difficulties among overweight adolescents: The potential impact of familial factors. J. Adolesc. Health 2002, 31, 145–153. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Total Sample (n = 1518) | Male Students (n = 794) | Female Students (n = 724) | BMI ≤P90 (n = 1373) | BMI >P90 (n = 145) | |
|---|---|---|---|---|---|
| Age | |||||
| Mean (SD) | 14.90 (0.68) | 14.99 (0.69) | 14.81 (0.66) | 14.90 (0.68) | 14.97 (0.67) |
| Range | 13–19 | 13–19 | 13–18 | 13–19 | 14–17 |
| Welfare recipients | 198 (13.0) | 91 (11.5) | 107 (14.8) | 169 (12.3) ** | 29 (20) |
| Immigrant background | 655 (43.1) | 433 (43.3) | 311 (43.0) | 575 (41.9) ** | 80 (55.2) |
| BMI | |||||
| Mean (SD) | 20.62 (3.04) | 21.08 (3.22) | 20.12 (2.74) | - | - |
| Range | 12.96–39.06 | 14.96–39.06 | 12.96–33.30 | - | - |
| >P90 (%) | 9.6 | 12.0 | 6.9 ** | - | - |
| Parental Physical Abuse in Childhood | |||||
| No (%) | 805 (53.0) | 426 (53.7) | 379 (52.3) | 741 (54.0) | 66 (45.5) |
| Moderate (%) | 527 (34.7) | 270 (34.0) | 257 (35.5) | 472 (34.4) | 52 (35.9) |
| Severe (%) | 186 (12.3) | 98 (12.3) | 88 (12.2) | 160 (11.7) * | 27 (18.6) |
| Parental Warmth in Childhood | |||||
| Low (%) | 130 (8.6) | 63 (8.4) | 63 (8.7) | 115 (8.4) | 13 (9.0) |
| Medium (%) | 805 (53.0) | 456 (57.4) | 349 (48.2) | 715 (52.1) | 93 (64.1) |
| High (%) | 583 (38.4) | 271 (34.1) | 312 (43.1) *** | 543 (39.5) | 39 (26.9) |
| Parental Monitoring in Childhood | |||||
| Low (%) | 143 (9.4) | 88 (11.1) | 55 (7.6) | 12 (8.8) | 19 (13.1) |
| Medium (%) | 866 (57.0) | 476 (59.9) | 390 (53.9) | 776 (56.5) | 92 (63.4) |
| High (%) | 509 (33.5) | 230 (29.0) | 279 (38.5) *** | 476 (34.7) | 34 (23.4) |
| BMI >P90 | PPA | PW | PM | |
|---|---|---|---|---|
| BMI >P90 | 0.04 | −0.09 ** | −0.11 ** | |
| PPA | 0.07 | −0.32 *** | −0.18 *** | |
| PW | −0.04 | −0.36 *** | 0.48 *** | |
| PM | −0.01 | −0.24 *** | 0.45 *** |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mößle, T.; Kliem, S.; Lohmann, A.; Bergmann, M.C.; Baier, D. Differential Influences of Parenting Dimensions and Parental Physical Abuse during Childhood on Overweight and Obesity in Adolescents. Children 2017, 4, 17. https://doi.org/10.3390/children4030017
Mößle T, Kliem S, Lohmann A, Bergmann MC, Baier D. Differential Influences of Parenting Dimensions and Parental Physical Abuse during Childhood on Overweight and Obesity in Adolescents. Children. 2017; 4(3):17. https://doi.org/10.3390/children4030017
Chicago/Turabian StyleMößle, Thomas, Sören Kliem, Anna Lohmann, Marie Christine Bergmann, and Dirk Baier. 2017. "Differential Influences of Parenting Dimensions and Parental Physical Abuse during Childhood on Overweight and Obesity in Adolescents" Children 4, no. 3: 17. https://doi.org/10.3390/children4030017
APA StyleMößle, T., Kliem, S., Lohmann, A., Bergmann, M. C., & Baier, D. (2017). Differential Influences of Parenting Dimensions and Parental Physical Abuse during Childhood on Overweight and Obesity in Adolescents. Children, 4(3), 17. https://doi.org/10.3390/children4030017