The Unfavorable Alliance of Pain and Poor Sleep in Children with Life-Limiting Conditions and Severe Psychomotor Impairment


Abstract
:1. Introduction
2. Materials and Methods
2.1. Dataset
- Child is affected by intellectual disability and at least one additional physical disability;
- Parents/caregivers are able to adequately communicate in German;
- Patient is being cared for in one of the participating institutions;
- Parents consented to participation and the use of the patient’s data for study purposes [4].
2.2. Sleep Questionnaire for Children with Severe Psychomotor Impairment (SNAKE)
2.3. Child- and Environment-Related Factors
2.4. Statistical Analyses
3. Results
3.1. Sample Characteristics
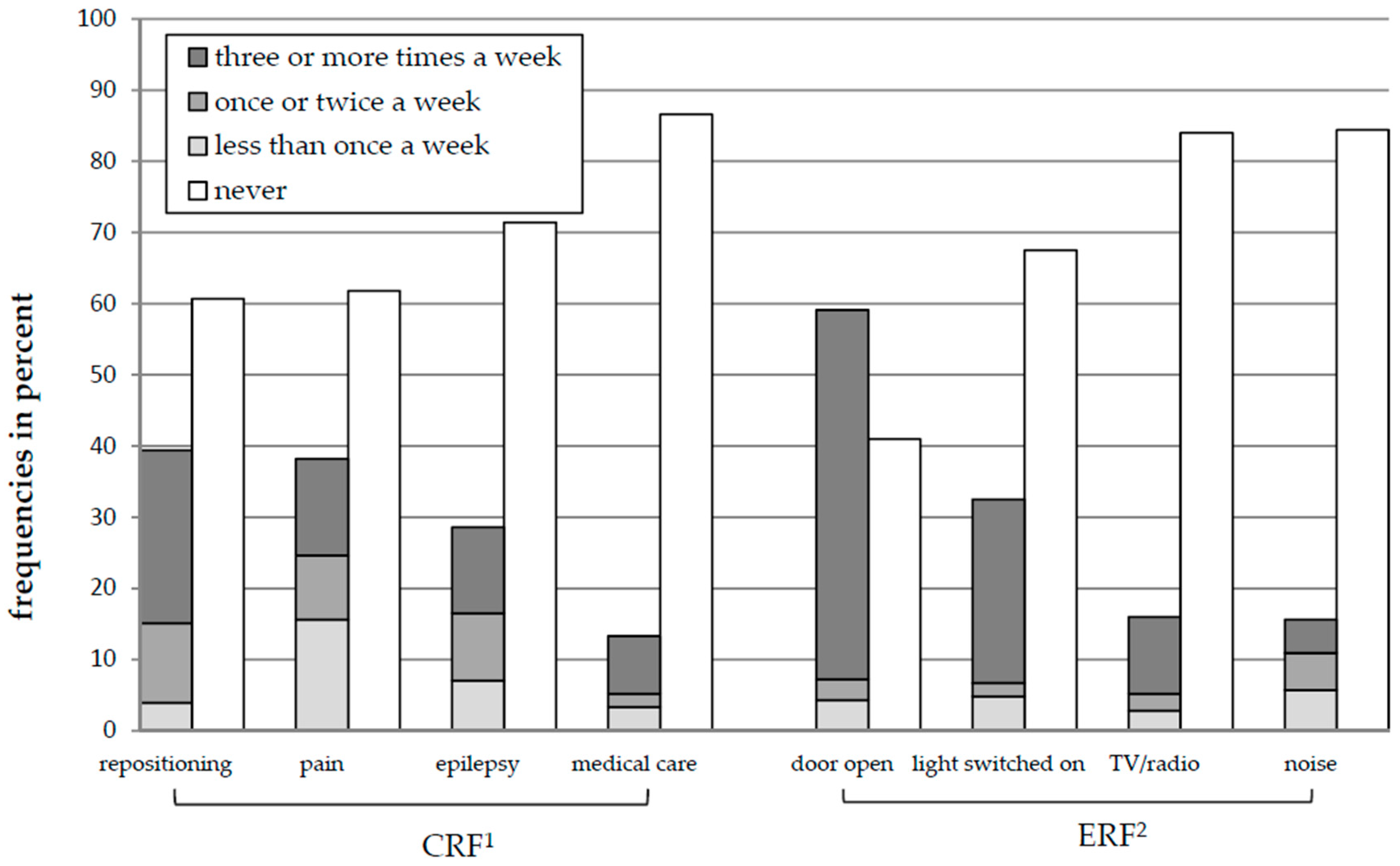
3.2. Frequency of CRF and ERF
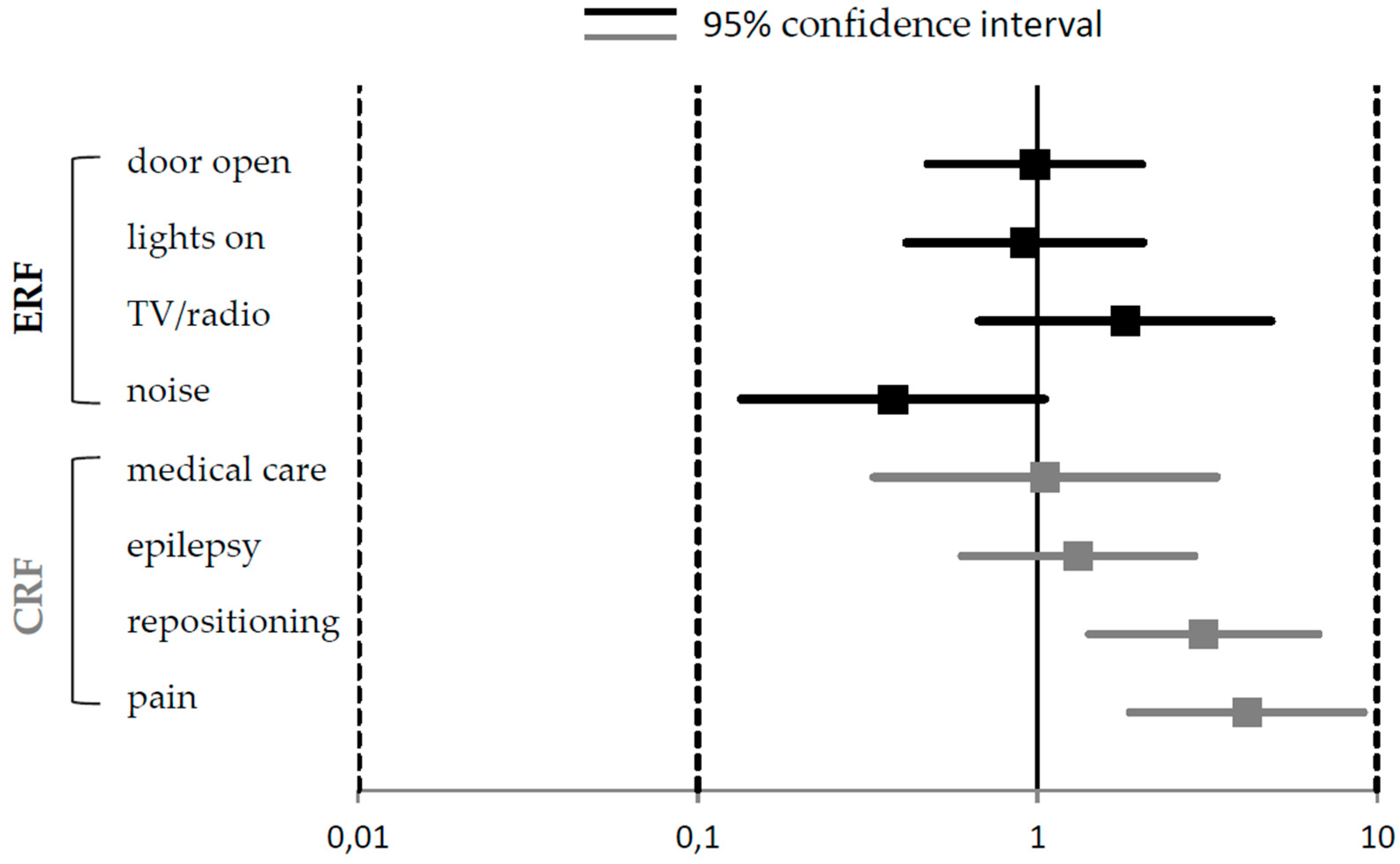
3.3. Influence of CRF and ERF on the Global Ratings of Children’s Sleep
3.4. Influence of CRF and ERF on the SNAKE Scales
3.5. Influence of CRF and ERF on Sleep Duration and Sleep Efficacy
4. Discussion
4.1. Child-Related Factors and their Influence on Sleep
4.2. Environment-Related Factors and their Influence on Sleep
4.3. Clinical Implications
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Thompson, A. Paediatric palliative care. Paediatr. Child Health 2015, 25, 458–462. [Google Scholar] [CrossRef]
- Craig, F.; Abu-Saad Huijer, H.; Benini, F.; Kuttner, L.; Wood, C.; Feraris, P.C.; Zernikow, B. Impacct: Standards of paediatric palliative care. Schmerz 2008, 22, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Zernikow, B. Palliativversorgung von Kindern, Jugendlichen und Jungen Erwachsenen; Springer: Heidelberg, Germany, 2013; Volume 2. [Google Scholar]
- Blankenburg, M.; Tietze, A.L.; Hechler, T.; Hirschfeld, G.; Michel, E.; Koh, M.; Zernikow, B. Snake: The development and validation of a questionnaire on sleep disturbances in children with severe psychomotor impairment. Sleep Med. 2013, 14, 339–351. [Google Scholar] [CrossRef] [PubMed]
- Tietze, A.L.; Blankenburg, M.; Hechler, T.; Michel, E.; Koh, M.; Schluter, B.; Zernikow, B. Sleep disturbances in children with multiple disabilities. Sleep Med. Rev. 2012, 16, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Feudtner, C.; Kang, T.I.; Hexem, K.R.; Friedrichsdorf, S.J.; Osenga, K.; Siden, H.; Friebert, S.E.; Hays, R.M.; Dussel, V.; Wolfe, J. Pediatric palliative care patients: A prospective multicenter cohort study. Pediatrics 2011, 127, 1094–1101. [Google Scholar] [CrossRef] [PubMed]
- Fraser, L.K.; Lidstone, V.; Miller, M.; Aldridge, J.; Norman, P.; McKinney, P.A.; Parslow, R.C. Patterns of diagnoses among children and young adults with life-limiting conditions: A secondary analysis of a national dataset. Palliat. Med. 2014, 28, 513–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Definition of Palliative Care for Children; WHO: Geneva, Switzerland, 1998. [Google Scholar]
- Garske, D.; Schmidt, P.; Hasan, C.; Wager, J.; Zernikow, B. Palliativversorgung auf der pädiatrischen palliativstation “lichtblicke”—Eine retrospektive studie. Palliativmedizin 2016, 17, 302–307. [Google Scholar] [CrossRef]
- Bhatt, M.H.; Podder, N.; Chokroverty, S. Sleep and neurodegenerative diseases. Semin. Neurol. 2005, 25, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Dorris, L.; Scott, N.; Zuberi, S.; Gibson, N.; Espie, C. Sleep problems in children with neurological disorders. Dev. Neurorehabil. 2008, 11, 95–114. [Google Scholar] [CrossRef] [PubMed]
- Adlington, K.; Liu, A.J.; Nanan, R. Sleep disturbances in the disabled child—A case report and literature review. Aust. Fam. Phys. 2006, 35, 711–715. [Google Scholar]
- Kohrman, M.H.; Carney, P.R. Sleep-related disorders in neurologic disease during childhood. Pediat. Neurol. 2000, 23, 107–113. [Google Scholar] [CrossRef]
- Romeo, D.M.; Brogna, C.; Quintiliani, M.; Baranello, G.; Pagliano, E.; Casalino, T.; Sacco, A.; Ricci, D.; Mallardi, M.; Musto, E.; et al. Sleep disorders in children with cerebral palsy: Neurodevelopmental and behavioral correlates. Sleep Med. 2014, 15, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Kothare, S.V.; Kaleyias, J. Sleep and epilepsy in children and adolescents. Sleep Med. 2010, 11, 674–685. [Google Scholar] [CrossRef] [PubMed]
- Sato, H.; Iwasaki, T.; Yokoyama, M.; Inoue, T. Monitoring of body position and motion in children with severe cerebral palsy for 24 hours. Disabil. Rehabil. 2014, 36, 1156–1160. [Google Scholar] [CrossRef] [PubMed]
- Bloetzer, C.; Jeannet, P.Y.; Lynch, B.; Newman, C.J. Sleep disorders in boys with duchenne muscular dystrophy. Acta Paediatr. 2012, 101, 1265–1269. [Google Scholar] [CrossRef] [PubMed]
- Newman, C.J.; O’Regan, M.; Hensey, O. Sleep disorders in children with cerebral palsy. Dev. Med. Child Neurol. 2006, 48, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Vandeleur, M.; Walter, L.M.; Armstrong, D.S.; Robinson, P.; Nixon, G.M.; Horne, R.S.C. What keeps children with cystic fibrosis awake at night? J. Cyst. Fibros. 2017, 16, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Mol, E.M.; Monbaliu, E.; Ven, M.; Vergote, M.; Prinzie, P. The use of night orthoses in cerebral palsy treatment: Sleep disturbance in children and parental burden or not? Res. Dev. Disabil. 2012, 33, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Breau, L.M.; Camfield, C.S. Pain disrupts sleep in children and youth with intellectual and developmental disabilities. Res. Dev. Disabil. 2011, 32, 2829–2840. [Google Scholar] [CrossRef] [PubMed]
- Davis, K.F.; Parker, K.P.; Montgomery, G.L. Sleep in infants and young children: Part two: Common sleep problems. J. Pediat. Health Care 2004, 18, 130–137. [Google Scholar] [CrossRef]
- Stallard, P.; Williams, L.; Lenton, S.; Velleman, R. Pain in cognitively impaired, non-communicating children. Arch. Dis. Child. 2001, 85, 460–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemmingsson, H.; Stenhammar, A.M.; Paulsson, K. Sleep problems and the need for parental night-time attention in children with physical disabilities. Child Care Health Dev. 2009, 35, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Brockmann, P.E.; Diaz, B.; Damiani, F.; Villarroel, L.; Nunez, F.; Bruni, O. Impact of television on the quality of sleep in preschool children. Sleep Med. 2016, 20, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Spruyt, K.; O’Brien, L.M.; Cluydts, R.; Verleye, G.B.; Ferri, R. Odds, prevalence and predictors of sleep problems in school-age normal children. J. Sleep Res. 2005, 14, 163–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dutt, R.; Roduta-Roberts, M.; Brown, C.A. Sleep and children with cerebral palsy: A review of current evidence and environmental non-pharmacological interventions. Children 2015, 2, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Jan, J.E.; Owens, J.A.; Weiss, M.D.; Johnson, K.P.; Wasdell, M.B.; Freeman, R.D.; Ipsiroglu, O.S. Sleep hygiene for children with neurodevelopmental disabilities. Pediatrics 2008, 122, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Jan, J.E.; Freeman, R.D. Melatonin therapy for circadian rhythm sleep disorders in children with multiple disabilities: What have we learned in the last decade? Dev. Med. Child Neurol. 2004, 46, 776–782. [Google Scholar] [CrossRef] [PubMed]
- Angriman, M.; Caravale, B.; Novelli, L.; Ferri, R.; Bruni, O. Sleep in children with neurodevelopmental disabilities. Neuropediatrics 2015, 46, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Fraser, J.; Gason, A.; Wraith, J.; Delatycki, M. Sleep disturbance in sanfilippo syndrome: A parental questionnaire study. Arch. Dis. Child. 2005, 90, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Hoban, T.F. Sleeplessness in children with neurodevelopmental disorders. CNS Drugs 2000, 14, 11–22. [Google Scholar] [CrossRef]
- Didden, R.; Sigafoos, J. A review of the nature and treatment of sleep disorders in individuals with developmental disabilities. Res. Dev. Disabil. 2001, 22, 255–272. [Google Scholar] [CrossRef]
- Tietze, A.L.; Zernikow, B.; Otto, M.; Hirschfeld, G.; Michel, E.; Koh, M.; Blankenburg, M. The development and psychometric assessment of a questionnaire to assess sleep and daily troubles in parents of children and young adults with severe psychomotor impairment. Sleep Med. 2014, 15, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Tietze, A.L.; Zernikow, B.; Michel, E.; Blankenburg, M. Sleep disturbances in children, adolescents, and young adults with severe psychomotor impairment: Impact on parental quality of life and sleep. Dev. Med. Child Neurol. 2014, 56, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Dreier, L.A.; Zernikow, B.; Blankenburg, M.; Wager, J. A sleep questionnaire for children with severe psychomotor impairment (snake)-concordance with a global rating of sleep quality. Children 2018, 5. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders. Diagnostic and Coding Manual, 2nd ed.; American Academy of Sleep Medicine: Westchester, IL, USA, 2005. [Google Scholar]
- WHO. Cancer Pain Relief; WHO: Geneva, Switzerland, 1986. [Google Scholar]
- Lelis, A.L.; Cardoso, M.V.; Hall, W.A. Sleep disorders in children with cerebral palsy: An integrative review. Sleep Med. Rev. 2016, 30, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Reiss, B. Sleeping while disabled, disabled while sleeping. Sleep Health 2016, 2, 187–190. [Google Scholar] [CrossRef] [PubMed]
- McGrath, P.J.; Rosmus, C.; Canfield, C.; Campbell, M.A.; Hennigar, A. Behaviours caregivers use to determine pain in non-verbal, cognitively impaired individuals. Dev. Med. Child Neurol. 1998, 40, 340–343. [Google Scholar] [PubMed]
- Visscher, M.; King, A.; Nie, A.M.; Schaffer, P.; Taylor, T.; Pruitt, D.; Giaccone, M.J.; Ashby, M.; Keswani, S. A quality-improvement collaborative project to reduce pressure ulcers in picus. Pediatrics 2013, 131, e1950–e1960. [Google Scholar] [CrossRef] [PubMed]
- Pallija, G.; Mondozzi, M.; Webb, A.A. Skin care of the pediatric patient. J. Pediat. Nurs. 1999, 14, 80–87. [Google Scholar] [CrossRef]
- Freundlich, K. Pressure injuries in medically complex children: A review. Children 2017, 4, 25. [Google Scholar] [CrossRef] [PubMed]
- Baharestani, M.M.; Ratliff, C.R. Pressure ulcers in neonates and children: An NPUAP white paper. Adv. Skin Wound Care 2007, 20, 208–220. [Google Scholar] [CrossRef] [PubMed]
- Sateia, M.J. International classification of sleep disorders-third edition. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Byars, A.W.; Byars, K.C.; Johnson, C.S.; DeGrauw, T.J.; Fastenau, P.S.; Perkins, S.; Austin, J.K.; Dunn, D.W. The relationship between sleep problems and neuropsychological functioning in children with first recognized seizures. Epilepsy Behav. 2008, 13, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Cortesi, F.; Giannotti, F.; Ottaviano, S. Sleep problems and daytime behavior in childhood idiopathic epilepsy. Epilepsia 1999, 40, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Beattie, J.F.; Koch, S.A.; Bolden, L.B.; Thompson, M.D. Neuropsychological consequences of sleep disturbance in children with epilepsy. Epilepsy Behav. 2016, 57, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Didden, R.; Korzilius, H.; van Aperlo, B.; van Overloop, C.; de Vries, M. Sleep problems and daytime problem behaviours in children with intellectual disability. J. Intellect. Disabil. Res. 2002, 46, 537–547. [Google Scholar] [CrossRef] [PubMed]
- Hill, C.M.; Parker, R.C.; Allen, P.; Paul, A.; Padoa, K.A. Sleep quality and respiratory function in children with severe cerebral palsy using night-time postural equipment: A pilot study. Acta Paediatr. 2009, 98, 1809–1814. [Google Scholar] [CrossRef] [PubMed]
- Read, J.; Simonds, A.; Kinali, M.; Muntoni, F.; Garralda, M.E. Sleep and well-being in young men with neuromuscular disorders receiving non-invasive ventilation and their carers. Neuromuscul. Disord. 2010, 20, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Solodiuk, J.C. Parent described pain responses in nonverbal children with intellectual disability. Int. Journal Nurs. Stud. 2013, 50, 1033–1044. [Google Scholar] [CrossRef] [PubMed]
- Breau, L.M.; Camfield, C.; McGrath, P.J.; Rosmus, C.; Finley, G.A. Measuring pain accurately in children with cognitive impairments: Refinement of a caregiver scale. J. Pediat. 2001, 138, 721–727. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Drug Class 1 | Active Agent | N |
|---|---|---|
| Non-opioid analgesics | Dipyrone | 8 |
| Ibuprofen | 2 | |
| Acetylsalicylic acid | 2 | |
| Paracetamol | 2 | |
| Weak opioids | Tilidine | 2 |
| Strong opioids | Morphine | 4 |
| Opium tincture | 1 | |
| Oxycodone | 1 | |
| Cannabinoids | Delta-9-Tetrahydrocannabinol | 1 |
| 23 |
| Dependant Variables: SNAKE Scales 1–5 | ||||||||||||||||
| Scale 1 (Disturbances Going to Sleep) | Scale 2 (Disturbances Remaining Asleep) | Scale 3 (Arousal and Breathing Disorders) | Scale 4 (Daytime Sleepiness) | Scale 5 (Daytime Behaviour Disorders) | ||||||||||||
| Variable | B (SE) | β | t | B (SE) | β | t | B (SE) | β | t | B (SE) | β | t | B (SE) | β | t | |
| CRF | Pain | 3.10 (0.71) | 0.36 | 4.33 *** | 2.76 (0.74) | 0.28 | 3.70 *** | 2.43 (0.69) | 0.26 | 3.51 ** | 0.24 (0.47) | 0.04 | 0.50 | 1.76 (0.66) | 0.23 | 2.66 ** |
| Repositioning | 0.12 (0.69) | 0.01 | 0.17 | 2.16 (0.72) | 0.22 | 2.98 ** | 2.66 (0.67) | 0.29 | 3.95 *** | 0.98 (0.46) | 0.16 | 2.13 * | 0.08 (0.64) | 0.01 | 0.13 | |
| Epilepsy | −0.81 (0.69) | −0.08 | −1.17 | 1.70 (0.72) | 0.16 | 2.34 * | 0.77 (0.67) | 0.07 | 1.15 | 2.36 (0.46) | 0.37 | 5.13 *** | 0.59 (0.65) | 0.07 | 0.90 | |
| Medical care | 0.86 (1.02) | 0.06 | 0.84 | −0.03 (1.06) | −0.00 | −0.03 | 0.51 (0.98) | 0.03 | 0.52 | −0.34 (0.67) | −0.03 | −0.50 | −0.00 (0.93) | −0.00 | −0.00 | |
| ERF | Noise | −0.16 (0.82) | −0.01 | −0.19 | −0.16 (0.85) | −0.01 | −0.18 | 1.10 (0.79) | 0.09 | 1.38 | 0.51 (0.54) | 0.06 | 0.94 | 0.98 (0.75) | 0.10 | 1.30 |
| TV/Radio | −0.19 (0.85) | −0.01 | −0.23 | 0.83 (0.88) | 0.06 | 0.94 | −1.09 (0.82) | −0.08 | −1.32 | 23 (0.56) | 0.02 | 0.41 | 0.13 (0.78) | 0.01 | 0.17 | |
| Lights on | 0.58 (0.68) | 0.06 | 0.84 | 0.90 (0.71) | 0.09 | 1.27 | 0.47 (0.66) | 0.05 | 0.71 | 0.76 (0.45) | 0.12 | 1.66 | 0.01 (0.63) | 0.00 | 0.02 | |
| Door open | 0.95 (0.61) | 0.11 | 1.54 | 0.23 (0.64) | 0.02 | 0.36 | 0.22 (0.59) | 0.02 | 0.37 | −0.13 (0.40) | −0.02 | −0.33 | 0.15 (0.57) | 0.02 | 0.26 | |
| Dependant Variables: Sleep Duration and Sleep Efficacy | ||||||||||||||||
| Sleep Duration | Sleep Efficacy | |||||||||||||||
| Variable | B (SE) | β | t | B (SE) | β | t | ||||||||||
| CRF | Pain | −0.56 (0.35) | −0.14 | −1.58 | −3.98 (3.25) | −0.11 | −1.22 | |||||||||
| Repositioning | −0.74 (0.34) | −0.18 | −2.15 * | −7.49 (3.19) | −0.21 | −2.34 * | ||||||||||
| Epilepsy | −0.38 (0.34) | −0.08 | −1.11 | −8.53 (3.14) | −0.22 | −2.71 * | ||||||||||
| Medical care | 0.66 (0.50) | 0.10 | 1.31 | 5.25 (4.40) | 0.10 | 1.19 | ||||||||||
| ERF | Noise | 0.40 (0.40) | 0.07 | 1.01 | 5.35 (3.51) | 0.12 | 1.52 | |||||||||
| TV/Radio | −0.32 (0.41) | −0.06 | −0.78 | −4.29 (3.78) | −0.09 | −1.13 | ||||||||||
| Lights on | −0.36 (0.33) | −0.08 | −1.07 | −2.89 (3.05) | −0.08 | −0.94 | ||||||||||
| Door open | −0.16 (0.30) | −0.04 | −0.54 | 1.82 (2.74) | 0.05 | 0.66 | ||||||||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dreier, L.A.; Wager, J.; Blankenburg, M.; Zernikow, B. The Unfavorable Alliance of Pain and Poor Sleep in Children with Life-Limiting Conditions and Severe Psychomotor Impairment. Children 2018, 5, 82. https://doi.org/10.3390/children5070082
Dreier LA, Wager J, Blankenburg M, Zernikow B. The Unfavorable Alliance of Pain and Poor Sleep in Children with Life-Limiting Conditions and Severe Psychomotor Impairment. Children. 2018; 5(7):82. https://doi.org/10.3390/children5070082
Chicago/Turabian StyleDreier, Larissa Alice, Julia Wager, Markus Blankenburg, and Boris Zernikow. 2018. "The Unfavorable Alliance of Pain and Poor Sleep in Children with Life-Limiting Conditions and Severe Psychomotor Impairment" Children 5, no. 7: 82. https://doi.org/10.3390/children5070082