Abstract
Regular physical activity during childhood and adolescence is associated with health benefits. Consequently, numerous health promotion programs for children and adolescents emphasize the enhancement of physical activity. However, the ActivityStat hypothesis states that increases in physical activity in one domain are compensated for by decreasing physical activity in another domain. Currently, little is known about how physical activity varies in children and adolescents within intervals of one day or multiple days. This systematic review provides an overview of studies that analyzed changes in (overall) physical activity, which were assessed with objective measurements, or compensatory mechanisms caused by increases or decreases in physical activity in a specific domain in children and adolescents. A systematic search of electronic databases (PubMed, Scopus, Web of Science, SportDiscus) was performed with a priori defined inclusion criteria. Two independent researchers screened the literature and identified and rated the methodological quality of the studies. A total of 77 peer-reviewed articles were included that analyzed changes in overall physical activity with multiple methodological approaches resulting in compensation or displacement. Of 40,829 participants, 16,265 indicated compensation associated with physical activity. Subgroup analyses separated by study design, participants, measurement instrument, physical activity context, and intervention duration also showed mixed results toward an indication of compensation. Quality assessment of the included studies revealed that they were of high quality (mean = 0.866). This review provides inconclusive results about compensation in relation to physical activity. A trend toward increased compensation in interventional studies and in interventions of longer duration have been observed.
1. Introduction
1.1. Health Benefits of Physical Activity
Regular physical activity (PA) during childhood and adolescence is associated with numerous health benefits []. As a result of regular PA, physical fitness in children increases, and is associated with improvements in cardiovascular [] and cardiometabolic [,] health, as well as with a reduction in obesity risk [,,]. Additionally, PA is associated with better mental health in children and adolescents [,].
In line with these findings, the World Health Organization (WHO) [,] developed PA recommendations for children and adolescents. Briefly, it is recommended for children 5 to 17 years of age to accumulate at least 60 min of moderate-to-vigorous PA (MVPA) daily []. However, recent analyses have demonstrated that PA levels of children and adolescents in many regions worldwide are not meeting the WHO recommendations [,,].
1.2. ActivityStat Hypothesis and Compensatory Mechanisms
PA promotion serves as a preventive health strategy [,], and there are numerous efforts to promote PA in children and adolescents to develop more active lifestyles [,,,]. To succeed with the health benefits of PA, it is essential to fully understand the PA determinants. Most research thus far has focused on the psychosociological, social, and environmental issues that affect PA levels []. In contrast, the potential effect of intrinsic biological control on regular activity has received little attention [].
With Rowland’s “ActivityStat” hypothesis [], the research on biological control that underpins PA and energy expenditure has gained momentum in the literature []. Briefly, the ActivityStat hypothesis suggests that an imposed increase or decrease in PA in one domain might induce a compensatory change in the opposite direction in another domain in order to maintain a level of PA or energy expenditure that is overall stable over time []. Thus, based on the ActivityStat concept, human beings maintain their total PA at a constant level by adapting various mechanisms, such as increasing or decreasing the frequency, intensity, or duration of time spent engaged in PA []. By such adapting mechanisms, their actual energy expenditure can either be increased or decreased so that the overall energy expenditure is stable over a certain period of time. For example, on a day when a child has physical education (PE) classes at school, the child may experience an increase in PA in the morning. However, the child may subsequently increase the time that they spend being sedentary in the afternoon, resulting in an overall PA level that is not increased for this day.
This compensatory mechanism has been observed in some interventional studies: school-based interventions [,,,,,,,] demonstrated small or moderate effects on increasing PA within the school setting, but little to no changes in terms of overall PA levels as a result of compensatory mechanisms employed outside of the school setting. Nevertheless, in order to obtain evidence regarding the general effectiveness of interventions on overall PA levels, a holistic approach is important—one that analyzes different domains and time periods of a day (e.g., physical activities in school and outside of school) in addition to overall PA. Such analyses could provide insights into the potential compensatory mechanisms and rearrangements mentioned in the ActivityStat hypothesis.
1.3. Displacement Hypothesis
The original displacement hypothesis postulates a mechanism that opposes the ActivityStat hypothesis, stating that watching television and other sedentary behaviors may displace PA []. Different studies have suggested that an increased amount of time spent being sedentary is the primary factor contributing to the current increase in obesity seen in adolescents [,,,,]. Due to its inverse relationship, this original hypothesis can also be used to justify the displacement of inactivity with PA. However, little evidence exists that supports this assumption in children and adolescents under 18 years of age [,,]. However, a Cochrane systematic review of school-based PA programs has concluded that there is solid evidence that school-based interventions have a positive impact on the duration of PA, with generally no effects on leisure time PA []. The review implies no substantial evidence that compensation is being made for PA imposed through interventions by having the PA decrease in another domain [].
1.4. Previous Reviews Analyzing Compensatory Mechanisms in Children and Adolescents
Little is known about how PA varies in children and adolescents within intervals of one and multiple days [,]. Additionally, the question arises as to whether and how inactive or sedentary time can be displaced by PA within one day or over a period of several days in children and adolescents. For children and adults, a systematic review by Gomersall, Rowlands, English, Maher, and Olds [] found inconclusive results with regard to the ActivityStat hypothesis. This review was limited in its scope because it exclusively considered studies that made explicit reference to compensation. Additionally, in the previous review, both children and adults were assessed, and objective as well as subjective measurement methods were used. Overall, to the best of our knowledge, no review has yet analyzed PA compensation in children and adolescents only within intervals of one and multiple days with objective measurement methods.
1.5. Aims of the Present Review
Starting from this state of research, this systematic review aims to provide a synthesis of studies that analyzed changes in overall PA among children and adolescents within various contexts of PA. Specifically, the present review aims: (i) to provide an overview and analysis of studies that examined changes in (overall) PA, assessed with objective measurements, in children and adolescents; and (ii) to identify the displacement of PA or whether compensatory mechanisms following PA increase or decrease in one domain or during a timespan of the day (e.g., at school, in the morning) or in terms of the amount at a specific intensity level (e.g., light, moderate, or vigorous PA).
2. Methods
This systematic review was performed and is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [].
2.1. Eligibility Criteria
Studies were deemed to be eligible if they met the following inclusion criteria and were excluded for the review if one or more exclusion criteria applies (Table 1).

Table 1.
Inclusion and exclusion criteria for the systematic review.
We decided to focus on objective measurement methods due to the advantages over subjective methods. These are limited to poorer reliability and validity, as well as participants recall bias []. Objective measurements are able to directly assess one or more dimensions of PA (intensity, frequency, time and type) and a variety of metrics such as step numbers, minutes or intensity [].
We included interventional as well as non-interventional studies. Interventional studies offered the opportunity to obtain information about “ActivityStat” by investigating within-subject changes in PA levels in response to an intervention stimulus. Non-interventional studies were included if they investigated PA levels of individuals during different timespans or in different domains over a period of several days.
2.2. Search Strategy
The search was performed on 31 March 2020 using the electronic databases PubMed, Scopus, Web of Science, and SportDiscus. In contrast to Gomersall, Rowlands, English, Maher, and Olds [], the search term in the present review was not limited to the term compensation: the search strategy included using a combination of terms related to children and youth (child* OR youth* OR adolescen* OR boy* OR girl* OR student* OR pupil*), terms related to PA compensation (increas* OR decreas* OR “more activ*” OR improve* OR “less activ*” OR compensat* OR displace* OR change* OR activitystat), terms related to measurement methods (“objective* measure*” OR acceleromet* OR pedomet* OR “heart rate monitor*” OR “doubly labeled water” OR calorimet* OR “direct* observ*”), and outcome-related terms (“physical activ*” OR “energy expenditure”). Two filters were used to refine the results and to obtain the final reference sample for screening. In accordance with the set inclusion criteria, studies published between 2000 and 2020 were selected. The publication type was filtered for journal articles (PubMed: “journal article”; SportDiscus: “academic journal”, “peer reviewed”; Scopus: “articles”; Web of Science: “Article”). In accordance with recommendations for systematic reviews [], we screened the reference lists and citations of included articles in order to identify additional relevant studies.
2.3. Study Selection
Identified references were imported into Endnote X9, a reference management software []. Subsequently, the citations were imported into Covidence, a systematic review software []. Within this program, all duplicates were removed. This step was followed by a three-step study selection process, comprising (1) title-screening, (2) abstract-screening, and (3) full-text-screening for inclusion criteria by two independent reviewers (F.B. and a trained student assistant). During each step of the screening process, all references that could not conclusively be excluded were kept for further screening in the next step. Disagreements between the two reviewers in relation to final inclusion were resolved through discussion with a third researcher (A.K.R.).
2.4. Data Extraction
The following data were extracted from each article: author(s); country; study design; sample description (number of participants, age, sex); aim/purpose of the study; measurement and instrument of measurement as well as duration of measurement; context of PA, main study results on the relationship between PA in one domain and PA in another domain/overall PA; and statistical indicators for compensation. In particular, this was referred to as the p-value for between- and within-group comparisons of PA or energy expenditure levels in one domain/timespan and the following domain/timespan (see also Electronic Supplementary Material File S1).
Studies were also classified by taking into consideration different settings or contexts in which PA was measured. In relation to the main objectives of the study, six settings were defined (school-based PA, physical education, active commuting to school, daily pattern, sport clubs, and others). All included studies were allocated to one of these categories.
2.5. Quality Assessment
The methodological quality of the included studies was rated by two independent reviewers (F.B. and a trained student assistant). To assess the quality of each study, criteria for evaluating primary research articles, developed by Kmet et al. [], were applied. We decided to use this tool because it is appropriate for a variety of different study designs. The “QualSyst” scoring system is based on existing tools and particularly relies upon the instruments developed by Cho and Bero [] and Timmer et al. [] for quantitative studies. A series of 14 items was used to assess quality. These items included questions related to study design, methods of participant selection, random allocation procedure, blinding, outcome measures, sample size, estimate of variance, confounding, reporting of results, and the evidence base for the conclusion. The items were scored depending on the degree to which each criterion was met (“yes” = 2, “partial” = 1, “no” = 0). If an item was not applicable to a particular study design, it was coded with “N/A” and was excluded from the calculation of the summative score. Randomization was only scored in interventional studies. The following equation was applied for estimating quality scores: 28 − (number of N/A × 2). Consequently, 28 was the maximum score that could be obtained for the 14 questions. The risk of bias was evaluated with its summary score (range 0–1), whereas higher scores indicated better methodological quality.
2.6. Synthesis of Results
It was anticipated that the studies included in this systematic review would exhibit a diverse range of research methods (e.g., study design, intervention characteristics, setting, measurements, participant characteristics, and outcome measures). Therefore, it was not appropriate to use meta-analysis to integrate and summarize the included studies. Instead, a narrative synthesis of results was performed. Summary tables describing the detailed characteristics of included studies and the visualization of statistical indicators, describing the probability for compensation related to these characteristics, were provided. The included studies and their findings were grouped according to the study design, sample size, target group, dependent variable, geographic origin, PA context, measurement instrument, duration of intervention (if this information was provided), intervention type, and the timespan in which compensation was measured. Analyses of compensatory mechanisms were performed for different categories, which seemed to be helpful for understanding compensation. In this respect, the aim was to determine which study design, target group, measurement instrument, PA context, timespan, and intervention duration, as well as type, was susceptible to compensation. A study was voted to be “supporting compensation” if the overall PA did not change with respect to different time points, or if it did not differ between intervention group(s) and control group(s), or if there was a significant increase in PA in one domain or timespan and a significant decrease in PA in another domain or timespan.
3. Results
3.1. Flow Chart
A total of 5917 potentially relevant articles (or 10,946 including duplicates) were identified through database searches, and their titles and abstracts were screened. In the next step, the full texts of 95 studies were retrieved for in-depth screening. Since 20 articles were excluded due to inappropriate aims of study, statistical analysis, participants, or multiple reasons, a total of 75 articles were identified as eligible and were included in this systematic review. Subsequently, 2 additional relevant publications were identified through backward reference tracking, yielding a total of 77 articles reporting on 74 unique studies included in this systematic review (Figure 1). PA as a Civil Skill Program was published in two studies that focused on LPA [] and moderate PA (MPA) [], respectively. The PHASE-Study was also reported in two separate articles. Ridgers et al. [] focused on the association between daily PA on two following days, whereas Ridgers et al. [] analyzed the correlations between the amount of sitting, standing, and stepping time within and between days in primary schoolchildren. Furthermore, two articles included in this review were part of the TEACHOUT-Study and investigated general effects of education outside the classroom [] and effects of education outside the classroom in different domains [].
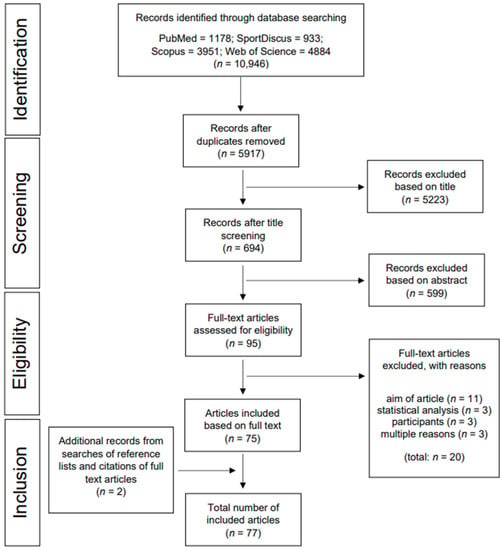
Figure 1.
Flow chart.
3.2. Characteristics of Included Studies
A complete data extraction table for each included study can be found in Electronic Supplementary Material File S1. A synthesis of the characteristics of the included articles is presented in Table 2. The majority of included articles (n = 49; 64%) presented non-interventional studies and 36% presented interventional studies. The sample size ranged from 13 [] to 6916 participants [], with a mean sample size of 532 participants. The geographical origin of the studies was as follows: n = 40 Europe, n = 21 North/Mid America, n = 10 Australia/New Zealand, and n = 6 Asia. Most studies (76%) were published between 2011 and 2020, with the earliest being published in 2000. The main focus of 65 studies (84%) were schoolchildren, whereas 12 (16%) studies focused on preschoolers. There were 4 studies that targeted only girls [,,,], and 2 only targeted boys [,]. Only 10 studies explicitly stated that their aim was to test compensation [,,,,,,,,,], and of these studies, 2 specifically mentioned the ActivityStat hypothesis [,]. There were 63 studies that used accelerometry to objectively assess PA, 13 used pedometers, and 1 used a heart rate monitor. A SenseWear Armband was used in 2 studies, in addition to an accelerometer, to assess energy expenditure [,]. Included studies were assigned to one of six contexts/settings: school-based PA in children and adolescents (n = 28), active commuting to school (n = 9), daily PA pattern (n = 15), physical education lessons (n = 16), organized sports (n = 5), or others (n = 4). With respect to interventional studies, the duration of the intervention varied from one week [,] to two years [,,,,]. The average duration of the interventions was 36 weeks (standard deviation (SD) = 37 weeks). Investigation of 3 intervention types found that 50% (n = 14) were educational, 29% (n = 8) were environmental, and 21% (n = 6) were multicomponent. Regardless of their study design (interventional or non-interventional), most studies (85%) examined changes in PA within a one-day period.
A total of 39 of the 77 studies, representing 16,297 (40%) children and adolescents, reported statistical indicators that emphasize the probability of compensation. From these 39 studies, 5 reported inconsistent findings in relation to compensation within the sample [,,,,]. Furthermore, some studies indicated compensation in one interventional group (higher amount of PA during intervention) but not in the other [,]—in girls but not in boys [,,,], or in boys but not in girls []. In Table 2, an overview of all studies supporting compensation (n = 39) is presented. With respect to study design, interventional studies indicated compensatory behavior in 75% of studies (representing 76% of participants; n = 6477), whereas non-interventional studies supported compensation in only 30% of studies (representing 30% of participants; n = 9820) [,,,,,,,,,,,,,,,,,]. Furthermore, 42% of preschoolers and 40% of schoolchildren showed indicators for compensatory behavior. Measurements conducted with a pedometer indicated compensation in 6938 participants (72%), whereas accelerometer measurements showed indicators for compensation in 9309 participants (30%). In relation to the PA context, school-based PA revealed compensation indicators in 5350 participants, which corresponded to 72% of all participants in this context, followed by active commuting to school (6095 participants; 56%). No compensation was indicated in the sport club context (0%). With respect to intervention duration, in studies with a duration ≥1 year, 100% of participants indicated compensatory behavior. Compensation was supported in all multicomponent interventions (n = 2074 participants) and in 64% of all educational interventions (n = 2295 participants).
Table 2.
Characteristics and compensation or displacement voting of all included articles.
Table 2.
Characteristics and compensation or displacement voting of all included articles.
| Characteristics | n Studies (% of All Studies) | n Participants (% of All Participants) | n Studies to Support Compensation | n Participants to Support Compensation | n Studies to Support Displacement | n Participants to Support Displacement | All Sources | Compensation Sources |
|---|---|---|---|---|---|---|---|---|
| Study design | ||||||||
| Non-interventional studies | 49 (64%) | 32,310 (79%) | 18 (37%) | 9820 (30%) | 35 (71%) | 22,490 (70%) | [,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,] | [,,,,,,,,,,,,,,,,] |
| Interventional studies | 28 (36%) | 8519 (21%) | 21 (75%) | 6477 (76%) | 10 (36%) | 2042 (24%) | [,,,,,,,,,,,,,,,,,,,,,,,,,,,] | [,,,,,,,,,,,,,,,,,,,] |
| Sample Size | ||||||||
| <500 | 57 (74%) | 10,980 (27%) | [,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,] | |||||
| >500 | 20 (26%) | 29,849 (73) | [,,,,,,,,,,,,,,,,,,,] | |||||
| Target group | ||||||||
| Preschool children (3–6 years) | 12 (16%) | 2188 (5%) | 5 (42%) | 919 (42%) | 7 (58%) | 38 (58%) | [,,,,,,,,,,,] | [,,,,] |
| School children (>6 years) | 65 (84%) | 38,641 (95%) | 34 (52%) | 15,378 (40%) | 1269 (58%) | 23,263 (60%) | [,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,] | [,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,] |
| Dependent Variable | ||||||||
| Physical Activity | 76 (96%) | 40,779 (99%) | [,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,] | |||||
| Energy Expenditure | 3 (4%) | 333 (1%) | [,,] | |||||
| Geographic origin | ||||||||
| Europe | 40 (52%) | 16,881 (41%) | [,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,] | |||||
| North America | 21 (27%) | 14,256 (35%) | [,,,,,,,,,,,,,,,,,,,,] | |||||
| Australia/New Zealand | 10 (13%) | 3548 (9%) | [,,,,,,,,,] | |||||
| Asia | 6 (8%) | 6144 (15%) | [,,,,,] | |||||
| PA measurement instrument | ||||||||
| Accelerometer | 63 (79%) | 31,150 (76%) | 32 (51%) | 9309 (30%) | 36 (57%) | 21,841 (70%) | [,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,] | [,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,] |
| Pedometer | 13 (16%) | 9629 (23%) | 6 (46%) | 6938 (72%) | 10 (77%) | 2691 (28%) | [,,,,,,,,,,,,] | [,,,,,] |
| Heart Rate Monitor | 1 (1%) | 50 (0.1%) | 1 (100%) | 50 (100%) | 0 | 0 | [] | [] |
| Context of PA measures | ||||||||
| School-based PA | 26 (34%) | 7392 (18%) | 19 (72%) | 5350 (72%) | 10 (36%) | 2042 (28%) | [,,,,,,,,,,,,,,,,,,,,,,,,,] | [,,,,,,,,,,,,,,,,,,] |
| Active commuting to school | 10 (13%) | 10,733 (26%) | 5 (50%) | 6175 (58%) | 7 (70%) | 4558 (43%) | [,,,,,,,,,] | [,,,,] |
| Daily PA Pattern | 15 (19%) | 12,499 (31%) | 7 (47%) | 1677 (13%) | 8 (53%) | 10,822 (87%) | [,,,,,,,,,,,,,,] | [,,,,,,] |
| Physical Education | 17 (22%) | 5814 (14%) | 7 (41%) | 2567 (44%) | 12 (75%) | 3247 (56%) | [,,,,,,,,,,,,,,,] | [,,,,,,] |
| Sports Club | 5 (6%) | 2583 (6%) | 0 (0%) | 0 (0%) | 5 (100%) | 2583 (100%) | [,,,,] | |
| Others (Locations/Active play) | 4 (5%) | 1808 (4%) | 1 (25%) | 528 (29%) | 3 (75%) | 1280 (71%) | [,,,] | [] |
| Duration of Intervention | ||||||||
| ≤one week | 2 (7%) | 207 (2%) | 1 (50%) | 51 (25%) | 1 (50%) | 156 (75%) | [,] | [] |
| ≤one month | 1 (4%) | 67 (1%) | 0 (0%) | 0 (0%) | 1 (100%) | 67 (100%) | [] | |
| ≤1–2 months | 6 (21%) | 869 (12%) | 5 (83) | 573 (66%) | 2 (33%) | 296 (34%) | [,,,,,] | [,,,,] |
| ≤3–4 months | 3 (11%) | 144 (2%) | 3 (100%) | 144 (100%) | 0 | 0 | [,,] | [,,] |
| ≤5–6 months | 6 (21%) | 2241 (38%) | 3 (50%) | 1520 (68%) | 4 (67%) | 721 (32%) | [,,,,,] | [,,] |
| ≤one year | 4 (14%) | 2450 (28%) | 3 (75%) | 1648 (58%) | 2 (50%) | 802 (32%) | [,,,] | [,,] |
| >one year | 6 (21%) | 2541 (31%) | 6 (100%) | 2541 (100%) | 0 | 0 | [,,,,,] | [,,,,,] |
| Intervention type | ||||||||
| Educational | 14 (50%) | 3593 (42%) | 9 (64%) | 2295 (64%) | 7 (50%) | 1145 (32%) | [,,,,,,,,,,,,] | [,,,,,,,,] |
| Environmental | 8 (29%) | 2393 (28%) | 6 (75%) | 2108 (88%) | 2 (25%) | 285 (12%) | [,,,,,,,] | [,,,,,] |
| Multicomponent | 6 (21%) | 2533 (30%) | 6 (100%) | 2074 (82%) | 1 (17%) | 459 (18%) | [,,,,,] | [,,,,,] |
| Timespan measuring compensation | ||||||||
| Within a day | 65 (85%) | 37,198 (91%) | 35 (54%) | 15,567 (42%) | 36 (55%) | 21,631 (58%) | [,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,] | [,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,] |
| Between two consecutive days | 4 (5%) | 904 (2%) | 3 (75%) | 610 (67%) | 1 (25%) | 294 (33%) | [,,,] | [,,] |
| Across several days | 8 (10%) | 2727 (7%) | 1 (13%) | 120 (4%) | 8 (100%) | 2607 (96%) | [,,,,,,,] | [] |
3.3. Results of Methodological Quality Assessment
For quality assessment, we applied the “QualSyst” scoring system with a scoring range of 0–1 []. The mean quality score of the included articles was rated as high by both raters (mean = 0.87, SD = 0.10, range 0.5–1). The methodological quality criteria and the proportion of studies fulfilling the criteria are presented in Table 3; more detailed quality assessments of each included article are presented in Electronic Supplementary File S2. Items 5, 6, and 7 were only scored for randomized controlled trials (RCTs).
Table 3.
Criteria for the methodological quality assessment and the number (%) of studies that scored points or each criterion.
In RCTs, the mean quality score was 0.76 (SD = 0.11) (range 0.5–0.89). In all RCTs, poor blinding of the treatment was evident for both investigators and participants. Overall, the included studies revealed a high quality, and only few studies exhibited a higher risk of bias [,,,].
4. Discussion
The present systematic review aims to provide a synthesis of studies that have analyzed changes in overall PA, assessed using objective measurements, or compensatory behavior caused by PA increases or decreases in a specific PA domain or during the timespan of one day in children and adolescents.
A total of 77 articles were included that investigated compensation or displacement across various contexts in children and adolescents. Overall, approximately 50% of the included articles found indicators suggesting compensation, and 50% refuted compensational behavior and supported the displacement of inactive time with bouts of activity. Detailed analyses based on study design, target group, instruments, context, intervention duration, and measurement duration were performed, revealing differences in compensation depending on categories. The analyses showed tendencies toward compensation in school interventions (especially with durations lasting longer than 1 year) and tendencies of displacement in the context of weekly organized participation in sport clubs.
It is hypothesized that when PA in one domain or timespan increases, PA in another domain or timespan decreases in order to maintain the constant PA level, as postulated by the ActivityStat hypothesis []. In the present analysis, 38 of 77 articles, involving a total of 24,532 participants, refuted the ActivityStat hypothesis and showed an increase in overall PA that resulted from imposed PA in one domain or timespan and absence of a reduction in PA in other domains or timespans. Sustained displacement of inactivity with PA led to an overall increased PA level, as described in the displacement hypothesis. One possible explanation for these increases in overall PA could be that imposed PA stimuli serve as some kind of trigger: PA opportunities in different contexts may stimulate children and adolescents to engage more in physical activities during the entire day [,,,,,].
In our review, we distinguished between interventional and non-interventional studies. A total of 21 interventional studies (n = 6477 participants) showed indicators for compensation, whereas only 18 non-interventional studies (n = 9820 participants) indicated compensatory behavior. This suggests that when the PA of children and adolescents is promoted in an intervention, the participants tend to compensate for the additional bouts of PA within the intervention by decreasing their activity levels during other parts of the day or in other domains so that they maintain their overall PA at a stable level. On the other hand, when children increase their PA levels on their own, without participating in an intervention program (in non-interventional studies), it seems that they do not compensate for this, and ultimately increase their overall PA level. This could be due to the fact that, in these cases, their PA is more likely based on intrinsic motivation that external influences. Furthermore, interventions were mostly offered and performed in (pre)school contexts. Improvements in (pre)school PA can be compensated for by less PA outside of (pre)school [,,,,,,,,,,,,,,,,,,]. “It is possible that school-based interventions are too focused on school setting and children and adolescents do not translate the health message on the importance of physical activity at home or in the community” []. For school interventions, it has been suggested that the focus should also be placed on changing parental behaviors and awareness for the sake of adopting a sustainable active lifestyle. In addition, multicomponent interventions or interventions that include schools together with families or communities are most effective in changing PA levels [,]. In general, interventions are most efficient when they operate on multiple levels []. “According to ecological models, the most powerful interventions should (a) ensure safe, attractive, and convenient places for physical activity, (b) implement motivational and educational programs to encourage use of those places, and (c) use mass media and community organization to change social norms and culture.” []. Intrapersonal, interpersonal, organizational, community, and public policy factors can influence health behaviors; thus, they consequently counteract compensatory behavior. Even though the literature suggests that multicomponent interventions have been shown to be useful for changing PA behavior, our results contradict this assumption, with the findings of compensatory behavior in all multicomponent studies [,,,,,].
Analysis of interventions pointed out a wide range in terms of intervention duration. All six studies (n = 2541 participants) in which interventions lasted for over one year supported compensation behavior in children and adolescents [,,,,,]. Nevertheless, compensatory behavior in children and adolescents was also identified in interventions that had a duration between one month and one year [,,,,,,,,,,]. A possible explanation for this finding could be that interventions which last for a shorter period of time may have little or no effect in changing the PA behavior of children and adolescents due to a lack of time needed to progress through the six stages of change, according to the trans-theoretical model []. This means that children and adolescents who accumulate more MVPA during an intervention might continue to be as physically active in their leisure time as they were before the intervention. The longer an intervention lasts, the greater the probability that children and adolescents adapt their PA and become less active in their leisure time; hence, maintaining their overall PA at a stable level.
Almost all studies included in our review captured PA data using pedometers or accelerometers. Only 6 pedometer studies (n = 6938 children and adolescents) reported compensatory mechanisms [,,,,,], whereas children and adolescents (n = 9309) showed compensatory behavior in 32 accelerometer studies [,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,]. One explanation for this finding could be that pedometers only capture step counts—an index of the number of steps a person took—whereas the overall PA levels for participating individuals remained unknown. Hence, it is likely that compensation is diagnosed through a measured reduction in steps, whereas other shifts in PA levels (e.g., overall MVPA) remain unconsidered. Furthermore, only 1 study out of the 77 analyzed studies investigated energy expenditure using a heart rate monitor and indicated compensation [].
In addition to interventions in a school context, there are two other settings in which children and adolescents are physically active. Only 57% of children and adolescents who actively commute to school showed indicators for compensation [,,,]. Active commuting and the independent mobility of children provide additional opportunities for spontaneous play [] and enable other active behaviors [,]. This can lead to an increase in overall PA, which therefore supports the displacement theory.
In the PE context, only 32% of the participants indicated compensatory behavior [,,,,,]. PE classes should provide an opportunity for children and adolescents to engage in PA and to develop knowledge about and attitudes toward developing an active lifestyle [], which could lead to displacing inactivity with active behavior. Interestingly, two articles, involving 365 participants, investigated the impact of different amounts of PE per week on overall PA levels in children and adolescents. From their findings, it can be summarized that more PE per week is not necessarily effective for increasing the total PA, because the PA in PE classes is often compensated for by less activity outside of the school setting [,]. Consequently, future studies should assess what the right amounts and intensities of PA during PE classes would be in order to avoid compensation outside of school.
Finally, our detailed analyses revealed one PA domain in which an increase in activity levels was not found to lead to compensation, but instead, to displacement: when engaging in organized sport clubs, children and adolescents do not compensate their PA levels by being less active after the training sessions [,,,,]. Sport clubs represent a health-promoting setting and support children and adolescents in living an active lifestyle outside sport clubs []. Furthermore, sport programs can provide beneficial access to and resources for recreational activities []. Thus, participation in sport clubs serves as an additional factor for increasing overall PA and can displace sedentary behavior.
Compensatory behavior occurs after a PA increase or decrease in one domain or timespan in order to maintain a stable overall PA level. Almost all studies in this review revealed that a PA increase in one domain or timespan is followed by a PA decrease in another domain or timespan, which is negatively connoted. Nevertheless, there exists one study [] in our review, where compensatory behavior was found to occur after a PA reduction—leading to compensation being positively connoted.
4.1. Implications
This review of compensation for PA in children and adolescents provides inconsistent results relating to compensation. Consequently, further research is needed to better understand compensatory mechanisms, and a recommendation is made for future studies to investigate PA behavior over a period of a few days using an objective measurement method. In addition, participants should complete a questionnaire or keep a diary in order to terminate and locate their activities and to obtain information about the reasons for their PA behavior. Social support plays an important role for sufficient PA in children and adolescents. Thus, PA behavior and attitudes of family and friends can influence one’s own PA and determine compensatory behavior. Additional subgroup analysis, including an examination of differences in PA by gender, age, weight status, socio-economic status (SES), and ethnicity, could provide more information about compensatory behavior. Gender differences have already been seen in a few of the included studies with inconclusive results [,,,]. Additionally, various SES analyses indicate different environmental, social, and educational circumstances [,]. Hence, SES is an important predictor of PA in children and adolescents [] and can influence compensatory behavior. Unfortunately, none of the included studies investigated compensatory behavior separately for different SES. It is hypothesized that children and adolescents with lower SES compensate more often than individuals with higher SES. It would also be interesting to further investigate the setpoint for “ActivityStat” or possible differences depending on age, season, or energy intake. Through an experimental design, future studies could investigate when this setpoint is reached and whether there are differences. Furthermore, there are currently no existing theories that deal with the timeframe for compensation. It is hypothesized that the timeframe for compensation is unlikely to be day-to-day []. Currently, the timeframes in the studies examined in our review are random. Finally, combined measurements of energy expenditure and PA should be used to obtain more detailed and reliable information about compensatory mechanisms.
Practical implications refer to interventional studies: in addition to active PA promotion, it is important to improve awareness in children and adolescents, as well as in their parents, regarding the importance of PA, as well as to encourage them to be physically active at home during their leisure time. This is necessary in order to avoid compensation that occurs when PA at home and/or in the family environment is reduced after increases in PA levels take place during interventions in, for example, the school setting.
4.2. Strengths and Limitations
The main strength of this review is that we exclusively included studies that objectively measured PA, including measures that directly assessed one or more PA dimension (e.g., frequency, intensity, time, and type) and captured a variety of measures, such as step counts, activity minutes, and PA intensity []. An additional strength lies in the fact that the systematic search of relevant primary studies employed several electronic databases and a comprehensive list of search strings. Furthermore, the reference lists of all included studies were manually checked in the search for additional relevant studies. Our search strategy was broad enough to enable us to identify relevant studies as well as to include those studies that did not analyze PA compensation as their main objective. In contrast to Gomersall, Rowlands, English, Maher, and Olds [], we did not only include studies that made explicit reference to compensation. Instead, we analyzed studies investigating changes in overall PA and in different domains or time segments for compensatory mechanisms. Another strength is the inclusion of a wide range of different settings in which PA plays an important role.
A limitation of this review relates to the variety in the study designs of the included studies, which made a comparison of the results difficult. Additionally, some studies only allowed between-subject analyses, which, in turn, only enabled conclusions about compensation to be obtained from a comparison of PA levels between two groups. For better understanding of compensatory mechanisms, within-subject analyses could provide stronger results. Another limitation is that there were different PA segments in the reviewed studies, which made it difficult to compare them all.
5. Conclusions
This systematic review provided inconclusive results regarding potential compensatory activity behavior after changes in PA levels in one domain or during a timespan in children and adolescents. Overall, 39 studies (n = 16,297 children and adolescents) that were included in this review did exhibit indicators of compensation. In summary, the synthesis of the included studies revealed a tendency for compensatory behavior in the context of interventions, especially in interventions with a long duration (<1 year). Furthermore, children and adolescents who regularly participated in organized sports showed no indicators for compensatory behavior. In order to verify the results of the present review, further investigations are needed.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/children9030351/s1, Table S1: Data extraction of included studies, Table S2: Quality Assessment of included studies.
Author Contributions
Conceptualization, F.B., F.A.E. and A.K.R.; methodology, F.B., F.A.E. and A.K.R.; writing—original draft preparation, F.B.; writing—review and editing, F.B., F.A.E. and A.K.R.; supervision, A.K.R. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the Federal and State Program for Women Professors (Pro-fessorinnenprogramm) (third phase; 2018–2022) that is funded by the Federal Ministry of Education and Research (BMBF) together with the German states.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors thank Susan Faizy and Ralf Winderl for their assistance in the processes of literature screening and methodological quality rating. Additionally, we acknowledge financial support by Deutsche Forschungsgemeinschaft and Friedrich-Alexander-Universität Erlangen-Nürnberg within the funding programme “Open Access Publication Funding”.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Gorber, S.C.; Kho, M.E.; et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S197–S239. [Google Scholar] [CrossRef]
- Ekelund, U.; Luan, J.; Sherar, L.B.; Esliger, D.W.; Griew, P.; Cooper, A. Moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents. JAMA 2012, 307, 704–712. [Google Scholar] [CrossRef]
- Committee, P.A.G.A.A. Physical Activity Guidelines Advisory and Committee Report; United States Department of Health and Human Services: Washington, DC, USA, 2008. [Google Scholar]
- World Health Organization. Global Health Risks. Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Hong, I.; Coker-Bolt, P.; Anderson, K.R.; Lee, D.; Velozo, C.A. Relationship Between Physical Activity and Overweight and Obesity in Children: Findings From the 2012 National Health and Nutrition Examination Survey National Youth Fitness Survey. Am. J. Occup. Ther. 2016, 70, 7005180060p1–7005180060p8. [Google Scholar] [CrossRef]
- Rodriguez-Ayllon, M.; Cadenas-Sanchez, C.; Estevez-Lopez, F.; Munoz, N.E.; Mora-Gonzalez, J.; Migueles, J.H.; Molina-Garcia, P.; Henriksson, H.; Mena-Molina, A.; Martinez-Vizcaino, V.; et al. Role of Physical Activity and Sedentary Behavior in the Mental Health of Preschoolers, Children and Adolescents: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 1383–1410. [Google Scholar] [CrossRef]
- Biddle, S.J.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. Br. J. Sports Med. 2011, 45, 886–895. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations of Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- World Health Organization. Guidelines on Physical Activity, Sedentary Behavior and Sleep for Children under 5 Years of Age; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Van Hecke, L.; Loyen, A.; Verloigne, M.; van der Ploeg, H.P.; Lakerveld, J.; Brug, J.; De Bourdeaudhuij, I.; Ekelund, U.; Donnelly, A.; Hendriksen, I.; et al. Variation in population levels of physical activity in European children and adolescents according to cross-European studies: A systematic literature review within DEDIPAC. Int. J. Behav. Nutr. Phys. Act 2016, 13, 1–22. [Google Scholar] [CrossRef]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Barnes, J.D.; Gonzalez, S.A.; Katzmarzyk, P.T.; Onywera, V.O.; Reilly, J.J.; Tomkinson, G.R. Global Matrix 2.0: Report Card Grades on the Physical Activity of Children and Youth Comparing 38 Countries. J. Phys. Act Health 2016, 13, S343–S366. [Google Scholar] [CrossRef]
- Janssen, I.; Leblanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act 2010, 7, 40. [Google Scholar] [CrossRef]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef]
- Messing, S.; Rutten, A.; Abu-Omar, K.; Ungerer-Rohrich, U.; Goodwin, L.; Burlacu, I.; Gediga, G. How Can Physical Activity Be Promoted Among Children and Adolescents? A Systematic Review of Reviews Across Settings. Front. Public Health 2019, 7, 55. [Google Scholar] [CrossRef]
- Dobbins, M.; Husson, H.; DeCorby, K.; LaRocca, R.L. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst. Rev. 2013, Cd007651. [Google Scholar] [CrossRef]
- Owen, M.B.; Curry, W.B.; Kerner, C.; Newson, L.; Fairclough, S.J. The effectiveness of school-based physical activity interventions for adolescent girls: A systematic review and meta-analysis. Prev. Med. 2017, 105, 237–249. [Google Scholar] [CrossRef]
- Gorga, E.; Regazzoni, V.; Bansilal, S.; Carubelli, V.; Trichaki, E.; Gavazzoni, M.; Lombardi, C.; Raddino, R.; Metra, M. School and family-based interventions for promoting a healthy lifestyle among children and adolescents in Italy: A systematic review. J. Cardiovasc. Med. 2016, 17, 547–555. [Google Scholar] [CrossRef]
- Sallis, J.F.; Hovell, M.F. Determinants of exercise behavior. Exerc. Sport Sci. Rev. 1990, 18, 307–330. [Google Scholar] [CrossRef]
- Thorburn, A.W.; Proietto, J. Biological determinants of spontaneous physical activity. Obes. Rev. 2000, 1, 87–94. [Google Scholar] [CrossRef]
- Rowland, T.W. The biological basis of physical activity. Med. Sci. Sports Exerc. 1998, 30, 392–399. [Google Scholar] [CrossRef]
- Gomersall, S.R.; Rowlands, A.V.; English, C.; Maher, C.; Olds, T.S. The ActivityStat hypothesis: The concept, the evidence and the methodologies. Sports Med. 2013, 43, 135–149. [Google Scholar] [CrossRef]
- Baggett, C.D.; Stevens, J.; Catellier, D.J.; Evenson, K.R.; McMurray, R.G.; He, K.; Treuth, M.S. Compensation or displacement of physical activity in middle-school girls: The Trial of Activity for Adolescent Girls. Int. J. Obes. 2010, 34, 1193–1199. [Google Scholar] [CrossRef]
- Baranowski, T.; Anderson, C.A.M.; Carmark, C. Mediating variables framework in physical activity interventions. How are we doing? How might we do better? Am. J. Prev. Med. 1998, 15, 266–297. [Google Scholar] [CrossRef]
- Gortmaker, S.L.; Peterson, K.; Wiecha, J.; Sobol, A.M.; Dixit, S.; Fox, M.K.; Laird, N. Reducing obesity via a school-based interdisciplinary intervention among youth: Planet Health. Arch. Pediatr. Adolesc. Med. 1999, 153, 409–418. [Google Scholar] [CrossRef]
- Kelder, S.H.; Perry, C.L.; Klepp, K.I. Community-wide youth exercise promotion: Long-term outcomes of the Minnesota Heart Health Program and the Class of 1989 Study. J. Sch. Health 1993, 63, 218–223. [Google Scholar] [CrossRef]
- Killen, J.D.; Telch, M.J.; Robinson, T.N.; Maccoby, N.; Taylor, C.B.; Farquhar, J.W. Cardiovascular disease risk reduction for tenth graders. A multiple-factor school-based approach. JAMA 1988, 260, 1728–1733. [Google Scholar] [CrossRef]
- Saunders, R.P.; Ward, D.; Felton, G.M.; Dowda, M.; Pate, R.R. Examining the link between program implementation and behavior outcomes in the lifestyle education for activity program (LEAP). Eval. Program Plan. 2006, 29, 352–364. [Google Scholar] [CrossRef]
- van Sluijs, E.M.; McMinn, A.M.; Griffin, S.J. Effectiveness of interventions to promote physical activity in children and adolescents: Systematic review of controlled trials. BMJ 2007, 335, 703. [Google Scholar] [CrossRef]
- Haapala, H.L.; Hirvensalo, M.H.; Kulmala, J.; Hakonen, H.; Kankaanpaa, A.; Laine, K.; Laakso, L.; Tammelin, T.H. Changes in physical activity and sedentary time in the Finnish Schools on the Move program: A quasi-experimental study. Scand. J. Med. Sci. Sports 2017, 27, 1442–1453. [Google Scholar] [CrossRef]
- Aburto, N.J.; Fulton, J.E.; Safdie, M.; Duque, T.; Bonvecchio, A.; Rivera, J.A. Effect of a School-Based Intervention on Physical Activity: Cluster-Randomized Trial. Med. Sci. Sports Exerc. 2011, 43, 1898–1906. [Google Scholar] [CrossRef]
- Mutz, D.C.; Roberts, D.F.; Van Vuuren, D.P. Reconsidering the Displacement Hypothesis. Television’s influence on Children’s Time use. Commun. Res. 1993, 20, 51–75. [Google Scholar] [CrossRef]
- Gortmaker, S.L.; Must, A.; Sobol, A.M.; Peterson, K.; Colditz, G.A.; Dietz, W.H. Television Viewing as a Cause of Increasing Obesity Among Children in the United States, 1986–1990. Arch. Pediatr. Adolesc. Med. 1996, 150, 356–362. [Google Scholar] [CrossRef]
- Dietz, W.J.; Gortmaker, S.L. Do we fatten our children at the television set? Obesity and television viewing in children and adolescents. Pediatrics 1985, 75, 807–812. [Google Scholar] [CrossRef]
- Klesges, R.C.; Shelton, M.L.; Klesges, L.M. Effects of television on metabolic rate: Potential implications for childhood obesity. Pediatrics 1993, 91, 281–286. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Barreira, T.V.; Broyles, S.T.; Champagne, C.M.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Johnson, W.D.; Kuriyan, R.; Kurpad, A.; et al. Physical Activity, Sedentary Time, and Obesity in an International Sample of Children. Med. Sci. Sports Exerc. 2015, 47, 2062–2069. [Google Scholar] [CrossRef]
- Jago, R.; Salway, R.; Emm-Collison, L.; Sebire, S.J.; Thompson, J.L.; Lawlor, D.A. Association of BMI category with change in children’s physical activity between ages 6 and 11 years: A longitudinal study. Int. J. Obes. 2020, 44, 104–113. [Google Scholar] [CrossRef]
- Marshall, S.J.; Biddle, S.J.; Gorely, T.; Cameron, N.; Murdey, I. Relationships between media use, body fatness and physical activity in children and youth: A meta-analysis. Int. J. Obes. Relat. Metab. Disord. 2004, 28, 1238–1246. [Google Scholar] [CrossRef]
- Lees, B.; Squeglia, L.M.; Breslin, F.J.; Thompson, W.K.; Tapert, S.F.; Paulus, M.P. Screen media activity does not displace other recreational activities among 9–10 year-old youth: A cross-sectional ABCD study®. BMC Public Health 2020, 20, 1783. [Google Scholar] [CrossRef]
- Spengler, S.; Mess, F.; Woll, A. Do Media Use and Physical Activity Compete in Adolescents? Results of the MoMo Study. PLoS ONE 2015, 10, e0142544. [Google Scholar] [CrossRef]
- Wilkin, T.J.; Mallam, K.M.; Metcalf, B.S.; Jeffery, A.N.; Voss, L.D. Variation in physical activity lies with the child, not his environment: Evidence for an ‘activitystat’ in young children (EarlyBird 16). Int. J. Obes. 2006, 30, 1050–1055. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The Prisam Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Word Health Organization. Adolescent Health. Available online: https://www.who.int/health-topics/adolescent-health#tab=tab_1 (accessed on 5 December 2021).
- Prince, S.A.; Adamo, K.B.; Hamel, M.E.; Hardt, J.; Gorber, S.C.; Tremblay, M. A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. Int. J. Behav. Med. Phys. Act. 2008, 5, 56. [Google Scholar] [CrossRef]
- Strath, S.J.; Kaminsky, L.A.; Ainsworth, B.E.; Ekelund, U.; Freedson, P.S.; Gary, R.A.; Richardson, C.R.; Smith, D.T.; Swartz, A.M. Guide to the assessment of physical activity: Clinical and research applications: A scientific statement from the American Heart Association. Circulation 2013, 128, 2259–2279. [Google Scholar] [CrossRef]
- Briscoe, S.; Bethel, A.; Rogers, M. Conduct and reporting of citation searching in Cochrane systematic reviews: A cross-sectional study. Res. Synth. Methods 2020, 11, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Endnote X9; Analytics Clarivate; Clarivate Analytics: Philadelphia, PE, USA, 2020.
- Covidence Systematic Review Software Melbourne; Veritas Health Innovation: Melbourne, Australia, 2020.
- Kmet, L.M.; Lee, R.C.; Cook, L.S. Standard Quality Assessment Criteria for Evaluating Primary Research Paper from a Variety of Fields; Alberta Heritage Foundation for Medical Research (AHFMR): Edmonton, AB, Canada, 2004. [Google Scholar]
- Cho, M.K.; Bero, L.A. Instruments for assessing the quality of drug studies published in the medical literature. JAMA 1994, 272, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Timmer, A.; Sutherland, L.R.; Hilsden, R.J. Development and evaluation of a quality score for abstracts. BMC Med. Res. Methodol. 2003, 3, 2. [Google Scholar] [CrossRef] [PubMed]
- Grasten, A. Children’s segment specific light physical activity across two years of school-based program. J. Phys. Educ. Sport 2015, 15, 88–95. [Google Scholar] [CrossRef]
- Grasten, A. Children’s segment specific moderate to vigorous physical activity through a school-initiated physical activity program. Balt. J. Health Phys. Act. 2015, 7, 19–32. [Google Scholar] [CrossRef]
- Ridgers, N.D.; Timperio, A.; Cerin, E.; Salmon, J. Compensation of physical activity and sedentary time in primary school children. Med. Sci. Sports Exerc. 2014, 46, 1564–1569. [Google Scholar] [CrossRef]
- Ridgers, N.D.; Timperio, A.; Cerin, E.; Salmon, J. Within- and between-day associations between children’s sitting and physical activity time. BMC Public Health 2015, 15, 950. [Google Scholar] [CrossRef]
- Schneller, M.B.; Duncan, S.; Schipperijn, J.; Nielsen, G.; Mygind, E.; Bentsen, P. Are children participating in a quasi-experimental education outside the classroom intervention more physically active? BMC Public Health 2017, 17, 1–13. [Google Scholar] [CrossRef]
- Schneller, M.B.; Schipperijn, J.; Nielsen, G.; Bentsen, P. Children’s physical activity during a segmented school week: Results from a quasi-experimental education outside the classroom intervention. Int. J. Behav. Med. Phys. Act. 2017, 14, 80. [Google Scholar] [CrossRef]
- Pelclova, J.; El Ansari, W.; Vasickova, J. Is Participation in After-School Physical Activity Associated with Increased Total Physical Activity? A Study of High School Pupils in the Czech Republic. Int. J. Environ. Res. Public Health 2010, 7, 2853–2865. [Google Scholar] [CrossRef]
- Alhassan, S.; Nwaokelemeh, O.; Greever, C.J.; Burkart, S.; Ahmadi, M.; St Laurent, C.W.; Barr-Anderson, D.J. Effect of a culturally-tailored mother-daughter physical activity intervention on pre-adolescent African-American girls’ physical activity levels. Prev. Med. Rep. 2018, 11, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Fromel, K.; Pelclova, J.; Skalik, K.; Novakova Lokvencova, P.; Mitas, J. The association between participation in organised physical activity and level of physical activity and inactivity in adolescent girls. Acta Gymnica 2012, 42, 7–16. [Google Scholar] [CrossRef]
- Harrington, D.M.; Davies, M.J.; Bodicoat, D.H.; Charles, J.M.; Chudasama, Y.V.; Gorely, T.; Khunti, K.; Plekhanova, T.; Rowlands, A.V.; Sherar, L.B.; et al. Effectiveness of the ‘Girls Active’ school-based physical activity programme: A cluster randomised controlled trial. Int. J. Behav. Med. Phys. Act. 2018, 15, 40. [Google Scholar] [CrossRef] [PubMed]
- Aljuhani, O.; Sandercock, G. Contribution of Physical Education to the Daily Physical Activity of Schoolchildren in Saudi Arabia. Int. J. Environ. Res. Public Health 2019, 16, 2397. [Google Scholar] [CrossRef]
- Wilson, A.N.; Olds, T.; Lushington, K.; Parvazian, S.; Dollman, J. Active School Lesson Breaks Increase Daily Vigorous Physical Activity, but Not Daily Moderate to Vigorous Physical Activity in Elementary School Boys. Pediatr. Exerc. Sci. 2017, 29, 145–152. [Google Scholar] [CrossRef]
- Alderman, B.L.; Benham-Deal, T.; Beighle, A.; Erwin, H.E.; Olson, R.L. Physical education’s contribution to daily physical activity among middle school youth. Pediatr Exerc. Sci. 2012, 24, 634–648. [Google Scholar] [CrossRef]
- Alhassan, S.; Sirard, J.R.; Robinson, T.N. The effects of increasing outdoor play time on physical activity in Latino preschool children. Int. J. Pediatr. Obes. 2007, 2, 153–158. [Google Scholar] [CrossRef]
- Carlson, J.A.; Mitchell, T.B.; Saelens, B.E.; Staggs, V.S.; Kerr, J.; Frank, L.D.; Schipperijn, J.; Conway, T.L.; Glanz, K.; Chapman, J.E.; et al. Within-person associations of young adolescents’ physical activity across five primary locations: Is there evidence of cross-location compensation? Int. J. Behav. Nutr. Phys. Act. 2017, 14, 50. [Google Scholar] [CrossRef]
- Dale, D.; Corbin, C.B.; Dale, K.S. Restricting opportunities to be active during school time: Do children compensate by increasing physical activity levels after school? Res. Q. Exerc. Sport 2000, 71, 240–248. [Google Scholar] [CrossRef]
- Fremeaux, A.E.; Mallam, K.M.; Metcalf, B.S.; Hosking, J.; Voss, L.D.; Wilkin, T.J. The impact of school-time activity on total physical activity: The activitystat hypothesis (EarlyBird 46). Int. J. Obes. 2011, 35, 1277–1283. [Google Scholar] [CrossRef]
- Long, M.W.; Sobol, A.M.; Cradock, A.L.; Subramanian, S.V.; Blendon, R.J.; Gortmaker, S.L. School-day and overall physical activity among youth. Am. J. Prev. Med. 2013, 45, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Morgan, C.F.; Beighle, A.; Pangrazi, R.P. What are the contributory and compensatory relationships between physical education and physical activity in children? Res. Q. Exerc. Sport 2007, 78, 407–412. [Google Scholar] [CrossRef]
- Ridgers, N.D.; Lamb, K.E.; Timperio, A.; Brown, H.; Salmon, J. Investigating children’s short-term responses to imposed or restricted physical activity. J. Phys. Act. Health 2018, 15, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Stylianou, M.; van der Mars, H.; Kulinna, P.H.; Adams, M.A.; Mahar, M.; Amazeen, E. Before-School Running/Walking Club and Student Physical Activity Levels: An Efficacy Study. Res. Q. Exerc. Sport 2016, 87, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Ridgers, N.D.; Barnett, L.M.; Lubans, D.R.; Timperio, A.; Cerin, E.; Salmon, J. Potential moderators of day-to-day variability in children’s physical activity patterns. J. Sport Sci. 2018, 36, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, K.T.; Sigurgeirsson, I.; Sveinsson, T.; Johannsson, E. Assessment of a two-year school-based physical activity intervention among 7–9-year-old children. Int. J. Behav. Med. Phys. Act. 2011, 8, 1–13. [Google Scholar] [CrossRef]
- Toftager, M.; Christiansen, L.B.; Ersboll, A.K.; Kristensen, P.L.; Due, P.; Troelsen, J. Intervention Effects on Adolescent Physical Activity in the Multicomponent SPACE Study: A Cluster Randomized Controlled Trial. PLoS ONE 2014, 9, e99369. [Google Scholar] [CrossRef]
- Eyre, E.L.J.; Cox, V.M.; Birch, S.L.; Duncan, M.J. An integrated curriculum approach to increasing habitual physical activity in deprived South Asian children. Eur. J. Sport Sci. 2016, 16, 381–390. [Google Scholar] [CrossRef]
- Goodman, A.; Mackett, R.L.; Paskins, J. Activity compensation and activity synergy in British 8–13 year olds. Prev. Med. 2011, 53, 293–298. [Google Scholar] [CrossRef]
- Cooper, A.R.; Page, A.S.; Foster, L.J.; Qahwaji, D. Commuting to school. Am. J. Prev. Med. 2003, 25, 273–276. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Lee, S.M.; Morgan, C.F.; Beighle, A.; Pangrazi, R.P. Children’s pedometer-determined physical activity during the segmented school day. Med. Sci. Sports Exerc. 2006, 38, 1732–1738. [Google Scholar] [CrossRef] [PubMed]
- Jago, R.; Wood, L.; Sebire, S.J.; Edwards, M.J.; Davies, B.; Banfield, K.; Fox, K.R.; Thompson, J.L.; Cooper, A.R.; Montgomery, A.A. School travel mode, parenting practices and physical activity among UK Year 5 and 6 children. BMC Public Health 2014, 14, 370. [Google Scholar] [CrossRef] [PubMed]
- Bin Tan, S.; Zegras, P.C.; Wilhelm, E.; Arcaya, M.C. Evaluating the effects of active morning commutes on students’ overall daily walking activity in Singapore: Do walkers walk more? J. Transport Health 2018, 8, 220–243. [Google Scholar] [CrossRef]
- Bringolf-Isler, B.; Grize, L.; Maeder, U.; Ruch, N.; Sennhauser, F.H.; Braun-Fahrlaender, C. Assessment of intensity, prevalence and duration of everyday activities in Swiss school children: A cross-sectional analysis of accelerometer and diary data. Int. J. Behav. Med. Phys. Act. 2009, 6, 50. [Google Scholar] [CrossRef]
- Ford, P.; Bailey, R.; Coleman, D.; Woolf-May, K.; Swaine, I. Activity levels, dietary energy intake, and body composition in children who walk to school. Pediatr. Exerc. Sci. 2007, 19, 393–407. [Google Scholar] [CrossRef]
- Gidlow, C.J.; Cochrane, T.; Davey, R.; Smith, H. In-school and out-of-school physical activity in primary and secondary school children. J. Sports Sci. 2008, 26, 1411–1419. [Google Scholar] [CrossRef]
- Groffik, D.; Mitas, J.; Jakubec, L.; Svozil, Z.; Fromel, K. Adolescents’ Physical Activity in Education Systems Varying in the Number of Weekly Physical Education Lessons. Res. Q. Exerc. Sport 2020, 91, 551–561. [Google Scholar] [CrossRef]
- Mallam, K.M.; Metcalf, B.S.; Kirkby, J.; Voss, L.D.; Wilkin, T.J. Contribution of timetabled physical education to total physical activity in primary school children: Cross sectional study. BMJ 2003, 327, 592–593. [Google Scholar] [CrossRef]
- Ribeyre, J.; Fellmann, N.; Vernet, J.; Delaître, M.; Chamoux, A.; Coudert, J.; Vermorel, M. Components and variations in daily energy expenditure of athletic and non-athletic adolescents in free-living conditions. Br. J. Nutr. 2007, 84, 531–539. [Google Scholar] [CrossRef][Green Version]
- Rooney, L.; McKee, D. Contribution of Physical Education and Recess towards the overall Physical Activity of 8-11 year old children. J. Sport Health Res. 2018, 10, 302–313. [Google Scholar]
- Brockman, R.; Jago, R.; Fox, K.R. The contribution of active play to the physical activity of primary school children. Prev. Med. 2010, 51, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Brusseau, T.; Kulinna, P.H.; Tudor-Locke, C.; Van der Mars, H.; Darst, P.W. Children’s step counts on weekend, physical education and non-physical education days. J. Hum. Kinet. 2011, 27, 125–135. [Google Scholar] [CrossRef]
- Cheung, P. School-based physical activity opportunities in PE lessons and after-school hours: Are they associated with children’s daily physical activity? Eur. Phys. Educ. Rev. 2019, 25, 65–75. [Google Scholar] [CrossRef]
- Gao, Y.; Wang, J.-J.; Lau, P.W.C.; Ransdell, L. Pedometer-determined physical activity patterns in a segmented school day among Hong Kong primary school children. J. Exerc. Sci. Fit. 2015, 13, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Hardman, C.A.; Horne, P.J.; Rowlands, A.V. Children’s pedometer-determined physical activity during school-time and leisure time. J. Exerc. Sci. Fit. 2009, 7, 129–134. [Google Scholar] [CrossRef]
- Jago, R.; Macdonald-Wallis, C.; Solomon-Moore, E.; Thompson, A.L.; Lawlor, D.A.; Sebire, S.J. Associations between participation in organised physical activity in the school or community outside school hours and neighbourhood play with child physical activity and sedentary time: A cross-sectional analysis of primary school-aged children from the UK. BMJ Open 2017, 7, e017588. [Google Scholar] [CrossRef]
- Kek, C.C.; Bengoechea, E.G.; Spence, J.C.; Mandic, S. The relationship between transport-to-school habits and physical activity in a sample of New Zealand adolescents. J. Sport Health Sci. 2019, 8, 463–470. [Google Scholar] [CrossRef]
- Kippe, K.O.; Lagestad, P.A. Kindergarten: Producer or Reducer of Inequality Regarding Physical Activity Levels of Preschool Children. Front. Public Health 2018, 6, 361. [Google Scholar] [CrossRef]
- Kobel, S.; Kettner, S.; Lammle, C.; Steinacker, J.M. Physical activity of German children during different segments of the school day. Z. Gesundh. Wiss. 2017, 25, 29–35. [Google Scholar] [CrossRef]
- Koorts, H.; Timperio, A.; Arundell, L.; Parker, K.; Abbott, G.; Salmon, J. Is sport enough? Contribution of sport to overall moderate- to vigorous-intensity physical activity among adolescents. J. Sci. Med. Sport 2019, 22, 1119–1124. [Google Scholar] [CrossRef]
- Mayorga-Vega, D.; Martinez-Baena, A.; Viciana, J. Does school physical education really contribute to accelerometer-measured daily physical activity and non sedentary behaviour in high school students? J. Sports Sci. 2018, 36, 1913–1922. [Google Scholar] [CrossRef] [PubMed]
- Meyer, U.; Roth, R.; Zahner, L.; Gerber, M.; Puder, J.J.; Hebestreit, H.; Kriemler, S. Contribution of physical education to overall physical activity. Scand. J. Med. Sci. Sports 2013, 23, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Mooses, K.; Kull, M. The participation in organised sport doubles the odds of meeting physical activity recommendations in 7–12-year-old children. Eur. J. Sport Sci. 2019, 20, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, G.; Bugge, A.; Hermansen, B.; Svensson, J.; Anderson, L.B. School Playground Facilities as a Determinant of Children’s Daily Activity: A Cross-Sectional Study of Danish Primary School Children. J. Phys. Act Health 2012, 9, 104–114. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J.R.; Pfeiffer, K.A.; Dowda, M.; Pate, R.R. In-school and out-of-school physical activity in preschool children. J. Phys. Act. Health 2016, 13, 606–610. [Google Scholar] [CrossRef]
- Owen, C.G.; Nightingale, C.M.; Rudnicka, A.R.; van Sluijs, E.M.F.; Ekelund, U.; Cook, D.G.; Whincup, P.H. Travel to school and physical activity levels in 9–10 year-old UK children of different ethnic origin; child heart and health study in England (CHASE). PLoS ONE 2012, 7, e30932. [Google Scholar] [CrossRef]
- Pesola, A.J.; Melin, M.; Vanhala, A.; Gao, Y.; Finni, T. Does SuperPark Make Children Less Sedentary? How Visiting a Commercial Indoor Activity Park Affects 7 to 12 Years Old Children’s Daily Sitting and Physical Activity Time. Int. J. Environ. Res. Public Health 2018, 15, 1595. [Google Scholar] [CrossRef]
- Sigmund, E.; Sigmundova, D.; Hamrik, Z.; Geckova, A.M. Does Participation in Physical Education Reduce Sedentary Behaviour in School and throughout the Day among Normal-Weight and Overweight-to-Obese Czech Children Aged 9–11 Years? Int. J. Environ. Res. Public Health 2014, 11, 1076–1093. [Google Scholar] [CrossRef]
- Smith, L.; Sahlqvist, S.; Ogilvie, D.; Jones, A.; Corder, K.; Griffin, S.J.; van Sluijs, E. Is a change in mode of travel to school associated with a change in overall physical activity levels in children? Longitudinal results from the SPEEDY study. Int. J. Behav. Med. Phys. Act. 2012, 9, 134–141. [Google Scholar] [CrossRef]
- Stewart, T.; Duncan, S.; Schipperijn, J. Adolescents who engage in active school transport are also more active in other contexts: A space-time investigation. Health Place 2017, 43, 25–32. [Google Scholar] [CrossRef]
- Trapp, G.; Giles-Corti, B.; Christian, H.; Timperio, A.; McCormack, G.; Bulsara, M.; Villanueva, K. Driving Down Daily Step Counts: The Impact of Being Driven to School on Physical Activity and Sedentary Behavior. Pediatr. Exerc. Sci. 2013, 25, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Vale, S.; Santos, R.; Soares-Miranda, L.; Silva, P.; Mota, J. The importance of physical education classes in pre-school children. J. Paediatr. Child Health 2011, 47, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Van Cauwenberghe, E.; De Craemer, M.; De Decker, E.; De Bourdeaudhuij, I.; Cardon, G. The impact of a teacher-led structured physical activity session on preschoolers’ sedentary and physical activity levels. J. Sci. Med. Sport 2013, 16, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Herman, K.M.; Paradis, G.; Mathieu, M.-E.; O’Loughlin, J.; Tremblay, A.; Lambert, M. Association Between Accelerometer-Measured Physical Activity Intensities and Sedentary Time in 8-to 10-Year-Old Children. Pediatr. Exerc. Sci. 2014, 26, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Adamo, K.B.; Wasenius, N.S.; Grattan, K.P.; Harvey, A.L.J.; Naylor, L.H.; Barrowman, N.J.; Goldfield, G.S. Effects of a Preschool Intervention on Physical Activity and Body Composition. J. Pediatr. 2017, 188, 42–49. [Google Scholar] [CrossRef]
- Adkins, M.; Brown, G.A.; Heelan, K.; Ansorge, C. Can dance exergaming contribute to improving physical activity levels in elementary school children? Afr. J. Phys. Health Educ. Recreat. Dance 2013, 19, 576–585. [Google Scholar]
- Alhassan, S.; Nwaokelemeh, O.; Ghazarian, M.; Roberts, J.; Mendoza, A.; Shitole, S. Effects of Locomotor Skill Program on Minority Preschoolers’ Physical Activity Levels. Pediatr. Exerc. Sci. 2012, 24, 435–449. [Google Scholar] [CrossRef]
- Alhassan, S.; Nwaokelemeh, O.; Ghazarian, M.; Shitole, S.; Puleo, E.; Pfeiffer, K.A.; Whitt-Clover, M.C. Feasibility and Effects of Short Activity Breaks for Increasing Preschool-Age Children’s Physical Activity Levels. J. Sch. Health 2016, 86, 526–533. [Google Scholar] [CrossRef]
- Alhassan, S.; Nwaokelemeh, O.; Lyden, K.; Goldsby, T.; Mendoza, A. A Pilot Study to Examine the Effect of Additional Structured Outdoor Playtime on Preschoolers’ Physical Activity Levels. Child Care Pract. 2013, 19, 23–35. [Google Scholar] [CrossRef]
- Coombes, E.; Jones, A. Gamification of active travel to school: A pilot evaluation of the Beat the Street physical activity intervention. Health Place 2016, 39, 62–69. [Google Scholar] [CrossRef]
- Kidokoro, T.; Shimizu, Y.; Edamoto, K.; Annear, M. Classroom Standing Desks and Time-Series Variation in Sedentary Behavior and Physical Activity among Primary School Children. Int. J. Environ. Res. Public Health 2019, 16, 1892. [Google Scholar] [CrossRef]
- Loucaides, C.A.; Jago, R.; Charalambous, I. Promoting physical activity during school break times: Piloting a simple, low cost intervention. Prev. Med. 2009, 48, 332–334. [Google Scholar] [CrossRef] [PubMed]
- Møller, N.C.; Tarp, J.; Kamelarczyk, E.F.; Brønd, J.; Klakk, H.; Wedderkopp, N. Do extra compulsory physical education lessons mean more physically active children—Findings from the childhood health, activity, and motor performance school study Denmark (The CHAMPS-study DK). Int. J. Behav. Med. Phys. Act. 2014, 11, 121. [Google Scholar] [CrossRef] [PubMed]
- O’Dwyer, M.V.; Fairclough, S.J.; Ridgers, N.D.; Knowles, Z.R.; Foweather, L.; Stratton, G. Effect of a school-based active play intervention on sedentary time and physical activity in preschool children. Health Educ. Res. 2013, 28, 931–942. [Google Scholar] [CrossRef] [PubMed]
- Palmer, K.K.; Chinn, K.M.; Robinson, L.E. The effect of the CHAMP intervention on fundamental motor skills and outdoor physical activity in preschoolers. J. Sport Health Sci. 2019, 8, 98–105. [Google Scholar] [CrossRef]
- Pate, R.R.; Brown, W.H.; Pfeiffer, K.A.; Howie, E.K.; Saunders, R.P.; Addy, C.L.; Dowda, M. An Intervention to Increase Physical Activity in Children A Randomized Controlled Trial With 4-Year-Olds in Preschools. Am. J. Prev. Med. 2016, 51, 12–22. [Google Scholar] [CrossRef]
- Sutherland, R.L.; Nathan, N.K.; Lubans, D.R.; Cohen, K.; Davies, L.J.; Desmet, C.; Cohen, J.; McCarthy, N.J.; Butler, P.; Wiggers, J.; et al. An RCT to Facilitate Implementation of School Practices Known to Increase Physical Activity. Am. J. Prev. Med. 2017, 53, 818–828. [Google Scholar] [CrossRef]
- Sallis, J.F.; Owen, N.; Fisher, E.B. Ecological Models of Health Behavior. In Health Behavior and Health Education: Theory, Research and Practice, 4th ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 465–486. [Google Scholar]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Velicer, W.F. The transtheoretical model of health behavior change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef]
- Page, A.S.; Cooper, A.R.; Griew, P.; Jago, R. Independent mobility, perceptions of the built environment and children’s participation in play, active travel and structured exercise and sport: The PEACH Project. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 17. [Google Scholar] [CrossRef]
- Wen, L.M.; Kite, J.; Merom, D.; Rissel, C. Time spent playing outdoors after school and its relationship with independent mobility: A cross-sectional survey of children aged 10–12 years in Sydney, Australia. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 15. [Google Scholar] [CrossRef] [PubMed]
- Hills, A.P.; Dengel, D.R.; Lubans, D.R. Supporting public health priorities: Recommendations for physical education and physical activity promotion in schools. Prog. Cardiovasc. Dis. 2015, 57, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Geidne, S.; Quennerstedt, M.; Eriksson, C. The youth sports club as a health-promoting setting: An integrative review of research. Scand. J. Public Health 2013, 41, 269–283. [Google Scholar] [CrossRef] [PubMed]
- Gidlow, C.; Johnston, L.H.; Crone, D.; Ellis, N.; James, D. A systematic review of the relationship between socio-economic position and physical activity. Health Educ. J. 2016, 65, 338–367. [Google Scholar] [CrossRef]
- Schmidt, S.C.E.; Anedda, B.; Burchartz, A.; Oriwol, D.; Kolb, S.; Wasche, H.; Niessner, C.; Woll, A. The physical activity of children and adolescents in Germany 2003-2017: The MoMo-study. PLoS ONE 2020, 15, e0236117. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).