
Exploring the Relation between Contextual Social Determinants of Health and COVID-19 Occurrence and Hospitalization
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
2.3. Outcomes
2.4. Exposures
2.5. Covariates
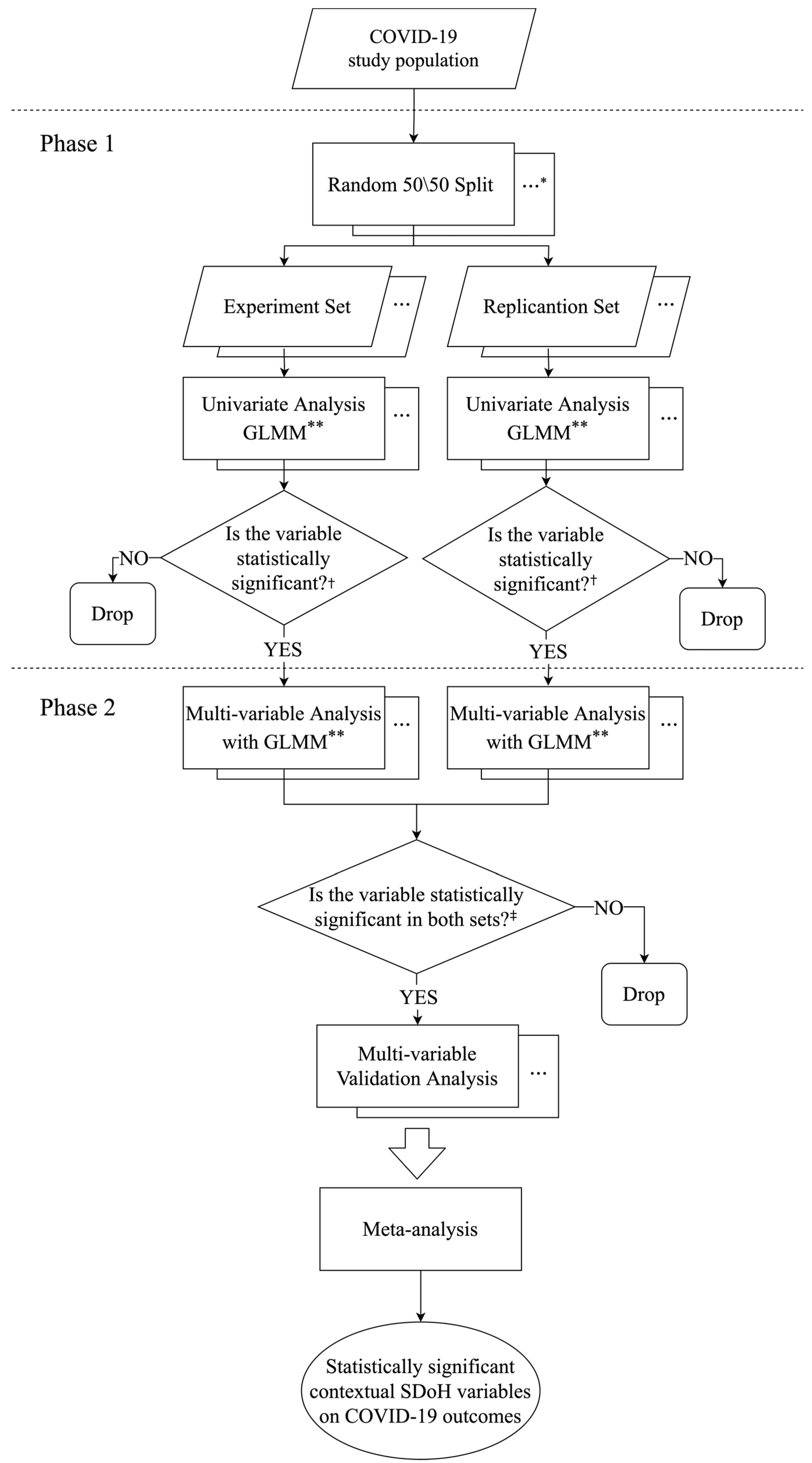
2.6. Data Analysis
3. Results
3.1. Characteristics of COVID-19 and Non-COVID-19 Patients
3.2. Characteristics of COVID-19 Outpatients and Hospitalized COVID-19 Patients
3.3. Associations between Contextual SDoH and COVID-19 Occurrence and Hospitalization
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Missing Imputation in Contextual SDoH Factors and Covariates
References
- Marois, G.; Muttarak, R.; Scherbov, S. Assessing the Potential Impact of COVID-19 on Life Expectancy. PLoS ONE 2020, 15, e0238678. [Google Scholar] [CrossRef]
- WHO. Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 9 December 2022).
- COVID-19 Community Impact Survey. Available online: https://www.mass.gov/resource/covid-19-community-impact-survey (accessed on 9 December 2022).
- Moynihan, R.; Sanders, S.; Michaleff, Z.A.; Scott, A.M.; Clark, J.; To, E.J.; Jones, M.; Kitchener, E.; Fox, M.; Johansson, M.; et al. Impact of COVID-19 Pandemic on Utilisation of Healthcare Services: A Systematic Review. BMJ Open 2021, 11, e045343. [Google Scholar] [CrossRef]
- New Analysis Shows Continued Negative Impact of COVID-19 on Hospital & Health System Financial Health in 2021. Available online: https://www.aha.org/press-releases/2021-03-23-new-analysis-shows-continued-negative-impact-covid-19-hospital-health (accessed on 9 December 2022).
- Social Determinants of Health. Available online: https://health.gov/healthypeople/priority-areas/social-determinants-health (accessed on 9 December 2022).
- Braveman, P.; Gottlieb, L. The Social Determinants of Health: It’s Time to Consider the Causes of the Causes. Public Health Rep. 2014, 129 (Suppl. S2), 19–31. [Google Scholar] [CrossRef] [PubMed]
- de Abreu, M.H.N.G.; Cruz, A.J.S.; Borges-Oliveira, A.C.; de Castro Martins, R.; de Freitas Mattos, F. Perspectives on Social and Environmental Determinants of Oral Health. Int. J. Environ. Res. Public Health 2021, 18, 13429. [Google Scholar] [CrossRef] [PubMed]
- Hynie, M. The Social Determinants of Refugee Mental Health in the Post-Migration Context: A Critical Review. Can. J. Psychiatry 2018, 63, 297–303. [Google Scholar] [CrossRef]
- Walker, R.J.; Smalls, B.L.; Campbell, J.A.; Strom Williams, J.L.; Egede, L.E. Impact of Social Determinants of Health on Outcomes for Type 2 Diabetes: A Systematic Review. Endocrine 2014, 47, 29–48. [Google Scholar] [CrossRef] [PubMed]
- Walker, R.J.; Strom Williams, J.; Egede, L.E. Influence of Race, Ethnicity and Social Determinants of Health on Diabetes Outcomes. Am. J. Med. Sci. 2016, 351, 366–373. [Google Scholar] [CrossRef]
- Jilani, M.H.; Javed, Z.; Yahya, T.; Valero-Elizondo, J.; Khan, S.U.; Kash, B.; Blankstein, R.; Virani, S.S.; Blaha, M.J.; Dubey, P.; et al. Social Determinants of Health and Cardiovascular Disease: Current State and Future Directions towards Healthcare Equity. Curr. Atheroscler. Rep. 2021, 23, 55. [Google Scholar] [CrossRef]
- Cockerham, W.C.; Hamby, B.W.; Oates, G.R. The Social Determinants of Chronic Disease. Am. J. Prev. Med. 2017, 52, S5–S12. [Google Scholar] [CrossRef]
- Li, Y.; Hu, H.; Zheng, Y.; Donahoo, W.T.; Guo, Y.; Xu, J.; Chen, W.-H.; Liu, N.; Shenkman, E.A.; Bian, J.; et al. Impact of Contextual-Level Social Determinants of Health on Newer Antidiabetic Drug Adoption in Patients with Type 2 Diabetes. Int. J. Environ. Res. Public Health 2023, 20, 36. [Google Scholar] [CrossRef]
- Hawkins, D. Social Determinants of COVID-19 in Massachusetts, United States: An Ecological Study. J. Prev. Med. Public Health 2020, 53, 220–227. [Google Scholar] [CrossRef]
- Raifman, M.A.; Raifman, J.R. Disparities in the Population at Risk of Severe Illness from COVID-19 by Race/Ethnicity and Income. Am. J. Prev. Med. 2020, 59, 137–139. [Google Scholar] [CrossRef]
- Baena-Díez, J.M.; Barroso, M.; Cordeiro-Coelho, S.I.; Díaz, J.L.; Grau, M. Impact of COVID-19 Outbreak by Income: Hitting Hardest the Most Deprived. J. Public Health 2020, 42, 698–703. [Google Scholar] [CrossRef] [PubMed]
- Jay, J.; Bor, J.; Nsoesie, E.O.; Lipson, S.K.; Jones, D.K.; Galea, S.; Raifman, J. Neighbourhood Income and Physical Distancing during the COVID-19 Pandemic in the United States. Nat. Hum. Behav. 2020, 4, 1294–1302. [Google Scholar] [CrossRef] [PubMed]
- Dang, H.A.; Huynh, T.L.; Nguyen, M.H. Does the COVID-19 pandemic disproportionately affect the poor? Evidence from a six-country survey. J. Econ. Dev. 2020. [Google Scholar] [CrossRef]
- Pflugeisen, B.M.; Mou, J. Empiric Evidence of Ethnic Disparities in Coronavirus Positivity in Washington State. Ethn. Health 2021, 26, 36–48. [Google Scholar] [CrossRef]
- Pan, D.; Sze, S.; Minhas, J.S.; Bangash, M.N.; Pareek, N.; Divall, P.; Williams, C.M.; Oggioni, M.R.; Squire, I.B.; Nellums, L.B.; et al. The Impact of Ethnicity on Clinical Outcomes in COVID-19: A Systematic Review. EClinicalMedicine 2020, 23, 100404. [Google Scholar] [CrossRef]
- de Souza, C.D.F.; Santos, A.G.G.D.; Cunha, E.J.O.; da Oliveira, T.F.; de Aquino, S.H.S.; Mesquita, R.D.R.; Silva Junior, L.C.F.; Santana, F.M.S.; Alcântara, R.C.; Arnozo, G.M.; et al. Information on Occupation of Patients with COVID-19: Literature Review. Rev. Assoc. Med. Bras. 2020, 66, 866–870. [Google Scholar] [CrossRef]
- Chen, Y.-H.; Glymour, M.; Riley, A.; Balmes, J.; Duchowny, K.; Harrison, R.; Matthay, E.; Bibbins-Domingo, K. Excess Mortality Associated with the COVID-19 Pandemic among Californians 18–65 Years of Age, by Occupational Sector and Occupation: March through November 2020. PLoS ONE 2021, 16, e0252454. [Google Scholar] [CrossRef]
- Hawkins, D.; Davis, L.; Kriebel, D. COVID-19 Deaths by Occupation, Massachusetts, March 1–July 31, 2020. Am. J. Ind. Med. 2021, 64, 238–244. [Google Scholar] [CrossRef]
- Dagliati, A.; Malovini, A.; Tibollo, V.; Bellazzi, R. Health Informatics and EHR to Support Clinical Research in the COVID-19 Pandemic: An Overview. Brief. Bioinform. 2021, 22, 812–822. [Google Scholar] [CrossRef]
- Brat, G.A.; Weber, G.M.; Gehlenborg, N.; Avillach, P.; Palmer, N.P.; Chiovato, L.; Cimino, J.; Waitman, L.R.; Omenn, G.S.; Malovini, A.; et al. International Electronic Health Record-Derived COVID-19 Clinical Course Profiles: The 4CE Consortium. NPJ Digit. Med. 2020, 3, 109. [Google Scholar] [CrossRef] [PubMed]
- Golinelli, D.; Boetto, E.; Carullo, G.; Nuzzolese, A.G.; Landini, M.P.; Fantini, M.P. Adoption of Digital Technologies in Health Care During the COVID-19 Pandemic: Systematic Review of Early Scientific Literature. J. Med. Internet Res. 2020, 22, e22280. [Google Scholar] [CrossRef] [PubMed]
- Adly, A.S.; Adly, A.S.; Adly, M.S. Approaches Based on Artificial Intelligence and the Internet of Intelligent Things to Prevent the Spread of COVID-19: Scoping Review. J. Med. Internet Res. 2020, 22, e19104. [Google Scholar] [CrossRef]
- Osborne, T.F.; Veigulis, Z.P.; Arreola, D.M.; Röösli, E.; Curtin, C.M. Automated EHR Score to Predict COVID-19 Outcomes at US Department of Veterans Affairs. PLoS ONE 2020, 15, e0236554. [Google Scholar] [CrossRef]
- Wagner, T.; Shweta, F.; Murugadoss, K.; Awasthi, S.; Venkatakrishnan, A.J.; Bade, S.; Puranik, A.; Kang, M.; Pickering, B.W.; O’Horo, J.C.; et al. Augmented Curation of Clinical Notes from a Massive EHR System Reveals Symptoms of Impending COVID-19 Diagnosis. Elife 2020, 9, e58227. [Google Scholar] [CrossRef]
- Wang, Q.Q.; Kaelber, D.C.; Xu, R.; Volkow, N.D. COVID-19 Risk and Outcomes in Patients with Substance Use Disorders: Analyses from Electronic Health Records in the United States. Mol. Psychiatry 2021, 26, 30–39. [Google Scholar] [CrossRef]
- Gu, T.; Mack, J.A.; Salvatore, M.; Sankar, S.P.; Valley, T.S.; Singh, K.; Nallamothu, B.K.; Kheterpal, S.; Lisabeth, L.; Fritsche, L.G.; et al. COVID-19 Outcomes, Risk Factors and Associations by Race: A Comprehensive Analysis Using Electronic Health Records Data in Michigan Medicine. medRxiv 2020. [Google Scholar] [CrossRef]
- Wang, Q.; Davis, P.B.; Gurney, M.E.; Xu, R. COVID-19 and Dementia: Analyses of Risk, Disparity, and Outcomes from Electronic Health Records in the US. Alzheimers. Dement. 2021, 17, 1297–1306. [Google Scholar] [CrossRef]
- Buikema, A.R.; Buzinec, P.; Paudel, M.L.; Andrade, K.; Johnson, J.C.; Edmonds, Y.M.; Jhamb, S.K.; Chastek, B.; Raja, H.; Cao, F.; et al. Racial and Ethnic Disparity in Clinical Outcomes among Patients with Confirmed COVID-19 Infection in a Large US Electronic Health Record Database. EClinicalMedicine 2021, 39, 101075. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors Associated with COVID-19-Related Death Using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Xu, R.; Volkow, N.D. Increased Risk of COVID-19 Infection and Mortality in People with Mental Disorders: Analysis from Electronic Health Records in the United States. World Psychiatry 2021, 20, 124–130. [Google Scholar] [CrossRef]
- Owen, R.K.; Conroy, S.P.; Taub, N.; Jones, W.; Bryden, D.; Pareek, M.; Faull, C.; Abrams, K.R.; Davis, D.; Banerjee, J. Comparing Associations between Frailty and Mortality in Hospitalised Older Adults with or without COVID-19 Infection: A Retrospective Observational Study Using Electronic Health Records. Age Ageing 2021, 50, 307–316. [Google Scholar] [CrossRef]
- Yonas, E.; Alwi, I.; Pranata, R.; Huang, I.; Lim, M.A.; Gutierrez, E.J.; Yamin, M.; Siswanto, B.B.; Virani, S.S. Effect of Heart Failure on the Outcome of COVID-19–A Meta Analysis and Systematic Review. Am. J. Emerg. Med. 2021, 46, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Soeroto, A.Y.; Soetedjo, N.N.; Purwiga, A.; Santoso, P.; Kulsum, I.D.; Suryadinata, H.; Ferdian, F. Effect of Increased BMI and Obesity on the Outcome of COVID-19 Adult Patients: A Systematic Review and Meta-Analysis. Diabetes Metab. Syndr. 2020, 14, 1897–1904. [Google Scholar] [CrossRef]
- Sawalha, K.; Abozenah, M.; Kadado, A.J.; Battisha, A.; Al-Akchar, M.; Salerno, C.; Hernandez-Montfort, J.; Islam, A.M. Systematic Review of COVID-19 Related Myocarditis: Insights on Management and Outcome. Cardiovasc. Revasc. Med. 2021, 23, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Palacio, A.; Tamariz, L. Social Determinants of Health Mediate COVID-19 Disparities in South Florida. J. Gen. Intern. Med. 2021, 36, 472–477. [Google Scholar] [CrossRef]
- Abdel Magid, H.S.; Ferguson, J.M.; Van Cleve, R.; Purnell, A.L.; Osborne, T.F. Differences in COVID-19 Risk by Race and County-Level Social Determinants of Health among Veterans. Int. J. Environ. Res. Public Health 2021, 18, 13140. [Google Scholar] [CrossRef]
- Rn, R.C.P.; Hec-C, S.J.M. The Social Determinants of Health, COVID-19, and Structural Competence. Online J. Issues Nurs. 2021, 26, 1–13. [Google Scholar]
- Hogan, W.R.; Shenkman, E.A.; Robinson, T.; Carasquillo, O.; Robinson, P.S.; Essner, R.Z.; Bian, J.; Lipori, G.; Harle, C.; Magoc, T.; et al. The OneFlorida Data Trust: A Centralized, Translational Research Data Infrastructure of Statewide Scope. J. Am. Med. Inform. Assoc. 2022, 29, 686–693. [Google Scholar] [CrossRef]
- Chen, A.; Li, Y.; Woodard, J.N.; Islam, J.Y.; Yang, S.; George, T.J.; Shenkman, E.A.; Bian, J.; Guo, Y. The Impact of Race-Ethnicity and Diagnosis of Alzheimer’s Disease and Related Dementias on Mammography Use. Cancers 2022, 14, 4726. [Google Scholar] [CrossRef]
- Garvin, E.; Branas, C.; Keddem, S.; Sellman, J.; Cannuscio, C. More than Just an Eyesore: Local Insights and Solutions on Vacant Land and Urban Health. J. Urban Health 2013, 90, 412–426. [Google Scholar] [CrossRef] [PubMed]
- CDC/ATSDR Social Vulnerability Index. Available online: https://www.atsdr.cdc.gov/placeandhealth/svi/index.html (accessed on 9 December 2022).
- Kind, A.J.H.; Buckingham, W.R. Making Neighborhood-Disadvantage Metrics Accessible–The Neighborhood Atlas. N. Engl. J. Med. 2018, 378, 2456–2458. [Google Scholar] [CrossRef] [PubMed]
- US Census Bureau County Business Patterns (CBP). Available online: https://www.census.gov/programs-surveys/cbp.html (accessed on 9 December 2022).
- North American Industry Classification System (NAICS) U.S. Census Bureau. Available online: https://www.census.gov/naics/ (accessed on 9 December 2022).
- Crime/Law Enforcement Stats (UCR Program). Available online: https://www.fbi.gov/how-we-can-help-you/need-an-fbi-service-or-more-information/ucr (accessed on 9 December 2022).
- Healthcare Analytics & Provider Data. Available online: https://www.definitivehc.com/ (accessed on 9 December 2022).
- Area Health Resources Files. Available online: https://data.hrsa.gov/topics/health-workforce/ahrf (accessed on 9 December 2022).
- National Walkability Index User Guide and Methodology. Available online: https://www.epa.gov/smartgrowth/national-walkability-index-user-guide-and-methodology (accessed on 12 October 2020).
- Rhone, A. Food Access Research Atlas. Available online: https://www.ers.usda.gov/data-products/food-access-research-atlas/ (accessed on 9 December 2022).
- Rhone, A. Food Environment Atlas. Available online: https://www.ers.usda.gov/data-products/food-environment-atlas/ (accessed on 9 December 2022).
- Measuring Vegetation (NDVI & EVI). Available online: https://earthobservatory.nasa.gov/features/MeasuringVegetation/measuring_vegetation_2.php (accessed on 12 October 2020).
- Hu, H.; Zhao, J.; Savitz, D.A.; Prosperi, M.; Zheng, Y.; Pearson, T.A. An External Exposome-Wide Association Study of Hypertensive Disorders of Pregnancy. Environ. Int. 2020, 141, 105797. [Google Scholar] [CrossRef]
- Azur, M.J.; Stuart, E.A.; Frangakis, C.; Leaf, P.J. Multiple Imputation by Chained Equations: What Is It and How Does It Work? Int. J. Methods Psychiatr. Res. 2011, 20, 40–49. [Google Scholar] [CrossRef]
- BestNormalize Package–RDocumentation. Available online: https://www.rdocumentation.org/packages/bestNormalize/versions/1.5.0 (accessed on 9 December 2022).
- Agier, L.; Portengen, L.; Chadeau-Hyam, M.; Basagaña, X.; Giorgis-Allemand, L.; Siroux, V.; Robinson, O.; Vlaanderen, J.; González, J.R.; Nieuwenhuijsen, M.J.; et al. A Systematic Comparison of Linear Regression-Based Statistical Methods to Assess Exposome-Health Associations. Environ. Health Perspect. 2016, 124, 1848–1856. [Google Scholar] [CrossRef] [PubMed]
- Patel, C.J.; Rehkopf, D.H.; Leppert, J.T.; Bortz, W.M.; Cullen, M.R.; Chertow, G.M.; Ioannidis, J.P. Systematic Evaluation of Environmental and Behavioural Factors Associated with All-Cause Mortality in the United States National Health and Nutrition Examination Survey. Int. J. Epidemiol. 2013, 42, 1795–1810. [Google Scholar] [CrossRef]
- Feise, R.J. Do Multiple Outcome Measures Require P-Value Adjustment? BMC Med. Res. Methodol. 2002, 2, 8. [Google Scholar] [CrossRef]
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair Allocation of Scarce Medical Resources in the Time of COVID-19. N. Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef]
- Quadri, S.A. COVID-19 and Religious Congregations: Implications for Spread of Novel Pathogens. Int. J. Infect. Dis. 2020, 96, 219–221. [Google Scholar] [CrossRef]
- Gaughan, C.H.; Ayoubkhani, D.; Nafilyan, V.; Goldblatt, P.; White, C.; TIngay, K.; Bannister, N. Religious Affiliation and COVID-19-Related Mortality: A Retrospective Cohort Study of Prelockdown and Postlockdown Risks in England and Wales. J. Epidemiol. Community Health 2021, 75, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Rich-Edwards, J.W.; Rocheleau, C.M.; Ding, M.; Hankins, J.A.; Katuska, L.M.; Kumph, X.; Steege, A.L.; Boiano, J.M.; Lawson, C.C. COVID-19 Vaccine Uptake and Factors Affecting Hesitancy among US Nurses, March–June 2021. Am. J. Public Health 2022, 112, 1620–1629. [Google Scholar] [CrossRef] [PubMed]
- Sides, E.; Jones, L.F.; Kamal, A.; Thomas, A.; Syeda, R.; Kaissi, A.; Lecky, D.M.; Patel, M.; Nellums, L.; Greenway, J.; et al. Attitudes towards Coronavirus (COVID-19) Vaccine and Sources of Information across Diverse Ethnic Groups in the UK: A Qualitative Study from June to October 2020. BMJ Open 2022, 12, e060992. [Google Scholar] [CrossRef]
- Wirsiy, F.S.; Nkfusai, C.N.; Ako-Arrey, D.E.; Dongmo, E.K.; Manjong, F.T.; Cumber, S.N. Acceptability of COVID-19 Vaccine in Africa. Int. J. MCH AIDS 2021, 10, 134–138. [Google Scholar] [CrossRef]
- Laliotis, I.; Minos, D. Religion, Social Interactions, and COVID-19 Incidence in Western Germany. Eur. Econ. Rev. 2022, 141, 103992. [Google Scholar] [CrossRef] [PubMed]
- Hipp, J.R. Income Inequality, Race, and Place: Does the Distribution of Race and Class within Neighborhoods affect Crime Rates? Criminology 2007, 45, 665–697. [Google Scholar] [CrossRef]
- Sun, Y.; Huang, Y.; Yuan, K.; Chan, T.O.; Wang, Y. Spatial Patterns of COVID-19 Incidence in Relation to Crime Rate Across London. ISPRS Int. J. Geo-Inf. 2021, 10, 53. [Google Scholar] [CrossRef]
- Singu, S.; Acharya, A.; Challagundla, K.; Byrareddy, S.N. Impact of Social Determinants of Health on the Emerging COVID-19 Pandemic in the United States. Front. Public Health 2020, 8, 406. [Google Scholar] [CrossRef]
- Shah, G.H.; Shankar, P.; Schwind, J.S.; Sittaramane, V. The Detrimental Impact of the COVID-19 Crisis on Health Equity and Social Determinants of Health. J. Public Health Manag. Pract. 2020, 26, 317–319. [Google Scholar] [CrossRef]
- Burström, B.; Tao, W. Social Determinants of Health and Inequalities in COVID-19. Eur. J. Public Health 2020, 30, 617–618. [Google Scholar] [CrossRef]
- Silverman, R.M.; Yin, L.; Patterson, K.L. Dawn of the Dead City: An Exploratory Analysis of Vacant Addresses in Buffalo, NY 2008–2010. J. Urban Aff. 2013, 35, 131–152. [Google Scholar] [CrossRef]
- Keegan, A.D. Hospital Bed Occupancy: More than Queuing for a Bed. Med. J. Aust. 2010, 193, 291–293. [Google Scholar] [CrossRef] [PubMed]
- Alin, A. Multicollinearity. WIREs Comp. Stat. 2010, 2, 370–374. [Google Scholar] [CrossRef]


{kind=link}
| Name | Data Source and Validation Study | Time Range | Spatial Scales | Temporal Scales |
|---|---|---|---|---|
| Vacant land | Aggregated USPS Administrative Data on Address Vacancies, HUD | 2006–2019 | Census tract | 3-month |
| Walkability | Walkability Index, the United States Environment Protection Agency | 2015 | Census block group | Cross-sectional |
| Food Access | USDA Food Access Research Atlas | 2010, 2015 (2011–2014 interpolated) | Census tract | 1-year |
| Food Environment | USDA Food Environment Atlas | 2015 | County | 1-year |
| Green Space | NASA MODIS | 2020 | 250 m/1 KM | 16-day/monthly |
| CDC Social Vulnerability Index | CDC ATSDR SVI | 2000, 2010, 2014, 2016, 2018 | County | 14–18 month |
| Area Deprivation Index | Neighborhood Atlas | 2013, 2015 | County | 20 years |
| Social Capital | United States Census Bureau | 1986–2018 | Zip-code | 1-year |
| Crime and Safety | Uniform Crime Reporting Program, FBI | Offense:1960–2017 Arrest: 1974–2016 | County | 1-year |
| Hospital Utilization | U.S. Department of Health & Human Services | Accessed2020 August | County | Cross-sectional |
| Healthcare Indicator | Health Resources & Services Administration | 2018–2019 | County | 1-year |
| COVID-19 Patients, n = 15,890 | Non-COVID-19 Patients, n = 63,560 | p-Value | |
|---|---|---|---|
| Age | |||
| Mean (SD) | 45.6 (20.9) | 45.7 (20.9) | =0.958 |
| Sex | |||
| Female | 9483 (59.7%) | 37,940 (59.7%) | =0.967 |
| Male | 6407 (40.3%) | 25,620 (40.3%) | |
| Race | |||
| White | 7161 (45.1%) | 26,114 (34.4%) | <0.001 |
| Black | 4444 (28.0%) | 14,235 (18.8%) | |
| Other | 4060 (25.6%) | 18,499 (34.5%) | |
| Unknown | 225 (1.4%) | 4712(8.8%) | |
| Ethnicity | |||
| Hispanic | 5020 (31.6%) | 15,665 (24.6%) | <0.001 |
| Non-Hispanic | 10,304 (64.8%) | 40,650 (64.0%) | |
| Other | 98 (0.6%) | 1981 (3.1%) | |
| Unknown | 468 (3.0%) | 5264(8.3%) | |
| Comorbid Conditions | |||
| ASCVD | 1473 (9.3%) | 5840 (9.2%) | =0.753 |
| Hypertension | 5388 (33.9%) | 23,392 (36.8%) | <0.001 |
| Diabetes | 3070 (19.3%) | 11,637 (18.3%) | =0.004 |
| COPD | 1984 (12.5) | 9980 (15.7%) | <0.001 |
| Cancer | 630 (4.0%) | 2489 (0.39%) | =0.780 |
| Chronic kidney disease | 2819 (17.7%) | 11,158 (17.6%) | =0.587 |
| Myocardial infarction | 310 (2.0%) | 1323 (2.1%) | =0.290 |
| Organ transplant | 283 (1.8%) | 592 (0.9%) | <0.001 |
| Asthma | 117 (0.7%) | 266 (0.4%) | <0.001 |
| Renal disease | 1402 (8.8%) | 5132 (8.1%) | =0.003 |
| Cerebrovascular disease | 299 (1.9%) | 1512 (2.4%) | <0.001 |
| Peripheral vascular disease | 923 (5.8%) | 4608 (7.3%) | <0.001 |
| COVID-19 Outpatients a, n = 12,438 (78.2%) | COVID-19 Hospitalized Patients b, n = 3452 (21.8%) | p-Value | |
|---|---|---|---|
| Age | |||
| Mean (SD) | 41.9 (19.5) | 59.4 (19.8) | <0.001 |
| Sex | |||
| Female | 7603 (61.1%) | 1880 (54.5%) | <0.001 |
| Male | 4855 (38.9%) | 1572 (45.5%) | |
| Race | |||
| White | 5504 (44.3%) | 1657 (48.0%) | <0.001 |
| Black | 3289 (26.4%) | 1155 (33.5%) | |
| Other | 3440 (27.6%) | 619 (17.9%) | |
| Unknown | 205 (1.6%) | 21 (0.6%) | |
| Ethnicity | |||
| Hispanic | 4019 (32.3%) | 1001 (29.3%) | =0.041 |
| Non-Hispanic | 7938 (63.8%) | 2366 (68.3%) | |
| Other | 74 (0.6%) | 24 (0.7%) | |
| Unknown | 407 (3.3%) | 61 (1.7%) | |
| Comorbid Conditions | |||
| ASCVD | 708 (5.7%) | 765 (22.2%) | <0.001 |
| Hypertension | 3165 (25.4%) | 2223 (64.4%) | <0.001 |
| Diabetes | 1619 (13.0%) | 1451 (42.0%) | <0.001 |
| COPD | 1240 (10.0%) | 744 (21.5%) | <0.001 |
| Cancer | 372 (3.0%) | 258 (7.5%) | <0.001 |
| Chronic kidney disease | 1487 (12.0%) | 1332 (38.6%) | <0.001 |
| Myocardial infarction | 133 (1.1%) | 177 (5.1%) | <0.001 |
| Organ transplant | 176 (1.4%) | 107 (3.1%) | <0.001 |
| Asthma | 76 (0.6%) | 41 (1.2%) | <0.001 |
| Renal disease | 641 (5.2%) | 761 (22.1%) | <0.001 |
| Cerebrovascular disease | 147 (1.2%) | 152 (4.4%) | <0.001 |
| Peripheral vascular disease | 478 (3.8%) | 445 (12.9%) | <0.001 |
| Contextual SDoH | OR (95% CI) | p-Value |
|---|---|---|
| Outcome 1: having COVID-19 vs. having no COVID-19 | ||
| Number of pediatric hospital beds (pediatric beds) | 0.86 (0.85, 0.86) | <0.001 |
| Rate of hospital bed utilization (hospital bed utilization) | 0.87 (0.86, 0.88) | <0.001 |
| Percentage of vacant business properties (12 to 24 months) (vacant property) | 0.90 (0.89, 0.91) | <0.001 |
| Number of establishments in golf courses and country clubs (per 10,000 population) (number of golf courses) | 1.05 (1.03, 1.07) | <0.001 |
| Murder rate (per 100 population) | 1.14 (1.13, 1.15) | <0.001 |
| Percentage of minority (all persons except white, non-Hispanic) (percent of minority) | 1.30 (1.29, 1.31) | <0.001 |
| Outcome 2: hospitalized vs. outpatient cared COVID-19 | ||
| Percentage of farmers markets that report selling baked/prepared food products (farmers market) | 0.90 (0.86, 0.93) | <0.001 |
| SNAP households, low access to stores (low access) | 1.14 (1.06, 1.22) | <0.001 |
| Number of establishments in religious organizations (per 10,000 population) (religion) | 1.34 (1.16, 1.54) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, A.; Zhao, Y.; Zheng, Y.; Hu, H.; Hu, X.; Fishe, J.N.; Hogan, W.R.; Shenkman, E.A.; Guo, Y.; Bian, J. Exploring the Relation between Contextual Social Determinants of Health and COVID-19 Occurrence and Hospitalization. Informatics 2024, 11, 4. https://doi.org/10.3390/informatics11010004
Chen A, Zhao Y, Zheng Y, Hu H, Hu X, Fishe JN, Hogan WR, Shenkman EA, Guo Y, Bian J. Exploring the Relation between Contextual Social Determinants of Health and COVID-19 Occurrence and Hospitalization. Informatics. 2024; 11(1):4. https://doi.org/10.3390/informatics11010004
Chicago/Turabian StyleChen, Aokun, Yunpeng Zhao, Yi Zheng, Hui Hu, Xia Hu, Jennifer N. Fishe, William R. Hogan, Elizabeth A. Shenkman, Yi Guo, and Jiang Bian. 2024. "Exploring the Relation between Contextual Social Determinants of Health and COVID-19 Occurrence and Hospitalization" Informatics 11, no. 1: 4. https://doi.org/10.3390/informatics11010004