
Application of Augmented Reality Technology for Chest ECG Electrode Placement Practice


1
School of Informatics, Walailak University, Nakhon Si Thammarat 80160, Thailand
2
Informatics Innovative Center of Excellence, Walailak University, Nakhon Si Thammarat 80160, Thailand
3
Biodesign Innovation Center, Department of Parasitology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok 10700, Thailand
4
Department of Mathematics, University at Buffalo, State University of New York, Buffalo, NY 14260-2900, USA
*
Author to whom correspondence should be addressed.
Informatics 2024, 11(1), 5; https://doi.org/10.3390/informatics11010005
Submission received: 9 October 2023
/
Revised: 28 December 2023
/
Accepted: 3 January 2024
/
Published: 15 January 2024
(This article belongs to the Section Human-Computer Interaction)
Abstract
:This study presents an augmented reality application for training chest electrocardiography electrode placement. AR applications featuring augmented object displays and interactions have been developed to facilitate learning and training of electrocardiography (ECG) chest lead placement via smartphones. The AR marker-based technique was used to track the objects. The proposed AR application can project virtual ECG electrode positions onto the mannequin’s chest and provide feedback to trainees. We designed experimental tasks using the pre- and post-tests and practice sessions to verify the efficiency of the proposed AR application. The control group was assigned to learn chest ECG electrode placement using traditional methods, whereas the intervention group was introduced to the proposed AR application for ECG electrode placement. The results indicate that the proposed AR application can encourage learning outcomes, such as chest lead ECG knowledge and skills. Moreover, using AR technology can enhance students’ learning experiences. In the future, we plan to apply the proposed AR technology to improve related courses in medical science education.
1. Introduction
Augmented reality (AR) can immerse users in the real world via supplementation with virtual, computer-generated elements, such as audio, video, and 2D/3D graphics. These virtual overlays are integrated into the physical environment by a different sensory mechanism, enabling users to perceive the real world with virtual objects. AR enables the incorporation of virtual items into actual settings to enhance real-time interaction [1]. AR technology has been developed owing to the advancements in hardware and software, making it accessible on smartphones without requiring specialized equipment [2].
The application of AR as educational technology is a significant area of study in today’s era. AR application research in education has been developed for several fields, including medicine and engineering [3,4,5,6,7,8,9,10]. In addition to designing AR applications, verifying their efficiency, usability, and user experience is crucial. Moreover, AR applications for educational purposes have been developed, leveraging mobile technologies. Some studies [11,12,13,14,15] have shown that AR technology can motivate students and improve their learning experiences. For example, a study suggested an AR learning system based on image schemas and AR animations for smartphone-based AR markers with interactive animations. Furthermore, AR-based instruction was shown to aid students in strengthening their programming skills, increasing their learning motivation, and decreasing their cognitive load. Additionally, students exhibited a favorable attitude toward the AR learning approach [16]. The researchers created an AR-based learning system to make programming ideas more concrete. Specifically, they used a highly interactive AR mode that enabled students to freely create puzzle cards to compare diverse 3D animation programming outcomes. The AR learning system significantly aided students in acquiring complex verb combinations, with those who used picture schema materials re-calling verb meanings more effectively [17]. Moreover, Bujak et al. [18] explore an AR application designed by researchers with a specific emphasis on psychological variables. Their work presents a comprehensive framework to elucidate the advantages and limitations of augmented reality learning experiences within the mathematics classroom, focusing on physical, cognitive, and contextual dimensions. The paper focuses on how AR can stimulate embodied representations, support symbolic understanding, and foster collaborative learning. This framework underscores the potential benefits of AR in boosting student motivation while addressing practical and technological considerations, offering valuable insights that inform our ongoing investigation. Furthermore, Lee [19] observed the transformative impact of AR technology on education and training. The findings emphasize the potential of AR for traditional educational approaches by shifting the location and timing of learning experiences, offering contextual on-site learning, and encouraging exploration of real-world information. The study reports that the contribution of AR to immersive, interactive learning experiences aims to enhance educational realism and strengthen learners’ motivation. By unlocking new avenues for learning and fostering increased engagement, AR can revolutionize education, aligning with contemporary needs and paving the way for a future where learning extends beyond conventional boundaries.
In medical education, significant strides have been made in harnessing the potential of AR, as highlighted by the research findings from various studies. Emphasizing immersive technologies [20] like AR, virtual reality (VR), mixed reality (MR), and extended reality (XR), the research particularly underscores their applications in surgery and anatomy, proving beneficial for doctors and medical students. The study stresses the importance of diversifying research topics to fully leverage immersive technology in medical education, focusing on collaborative learning experiences through group experiments. Dhar et al. [21] propose that integrating digitally generated 3D representations with real-world stimuli is increasingly integral to medical education. Offering advantages such as remote learning, interactive simulations, and improved comprehension, AR enhances medical students’ knowledge, practical skills, and social skills. The paper identifies specific AR programs, such as HoloHuman and OculAR SIM, designed for this purpose, especially relevant during the COVID-19 pandemic.
Parsons et al. [22] examine current trends in AR usage in medical education and identify areas for further exploration from twenty-one peer-reviewed journal articles from 2015 to 2020; the study indicates that AR is more effective in supporting skill development than knowledge gain in medical education. Key affordances include enhancing practical skills in a spatial context, device portability, and situated learning, with a growing exploration into other practice areas beyond anatomy and surgery. Simultaneously, ref. [23] explores the emergence of VR, AR, and alternate reality technologies in simulation-based education, highlighting how these technologies expand the applications of simulation-based education, providing asynchronous and geographically diverse learning opportunities. In a parallel endeavor, ref. [24] emphasizes the revolutionary potential of VR and AR technologies in medical education, focusing on their capacity to provide an extensive array of anatomical models. Furthermore, Kugelmann et al. [25] introduce an innovative AR Magic Mirror technology for interactive anatomy learning, showcasing improvements in students’ enthusiasm and understanding of anatomy. Additionally, two noteworthy studies present the REFLECT system [26] and an AR-based learning intervention for clinical anatomy [27] and examine the value of a mobile AR ultrasound simulator for ultrasound training. The REFLECT system demonstrates enhanced learning of the musculoskeletal system, while the mobile AR ultrasound simulator exhibits improved accuracy in kidney measurements compared to traditional textbooks. These findings collectively highlight the transformative impact of AR and related technologies in advancing medical education.
Healthcare professionals, including nurses, paramedics, and those in emergency medicine or cardiology, are trained in chest electrocardiography or ECG lead placement. This refers to the process of attaching electrodes to a patient’s chest at specific locations to measure the electrical activity of the heart [28]. ECG signal measurement, which is a diagnostic test that records the electrical activity of the heart, involves attaching electrodes to the patient’s chest, arms, and legs, through which the electrical activity of the heart is recorded. The ECG machine produces a graph, called an ECG trace, depicting the electrical activity of the heart. Proper lead placement is important for accurate ECG readings and proper diagnosis of cardiac conditions. Learning ECG chest placement commonly begins with a comprehensive study of educational materials, encompassing textbooks and guidelines. Establishing a solid foundation for accurate electrode placement involves understanding the anatomy of the chest and key landmarks, including the sternal notch and midclavicular line. It is imperative for learners to grasp the specific locations for each lead (V1 to V6) to ensure precision in recording. Hence, the implementation of ECG electrode placement training has been suggested [29]. Bifulco et al. [30] proposed an augmented reality (AR) application that served as an interactive guide through a head-mounted display (HMD), aiding untrained individuals by displaying a virtual ECG position on a mannequin’s chest. Users could interact through a red circle augmented on the chest, guiding them to the correct electrode position. Results demonstrated that ten unskilled volunteers successfully performed an ECG test on a mannequin and a patient within a respectable timeframe (approximately 8 min). The average error distance was less than 3 mm for the mannequin and 7 mm for the patient. However, a limitation of this proposed method was the requirement for an HMD, which is not commonly used in daily life. To address this concern, there is a challenge to introduce an AR application approach as a supportive learning tool through mobile devices, making it more accessible for the common learner.
In this study, we propose an AR application on a smartphone to enhance the learning experience in ECG chest electrode placement. Two primary objectives guided our investigation: (1) verifying the impact of the AR application on students’ learning efficiency, encompassing background theoretical knowledge and ECG electrode placement skills, and (2) proving optimization of the utilization of the AR application for ECG electrode placement training. The latter involves an in-depth examination of specific factors contributing to the effectiveness and usability of the AR-based approach. The remainder of this paper is organized into six sections. Section 2 introduces ECG placement and AR technology. The AR application setup is detailed in Section 3, with the methodology presented in Section 4. Section 5 presents the experimental results and discussion, and the conclusion is provided in Section 6.
2. Materials and Methods
2.1. Chest Lead ECG Positioning
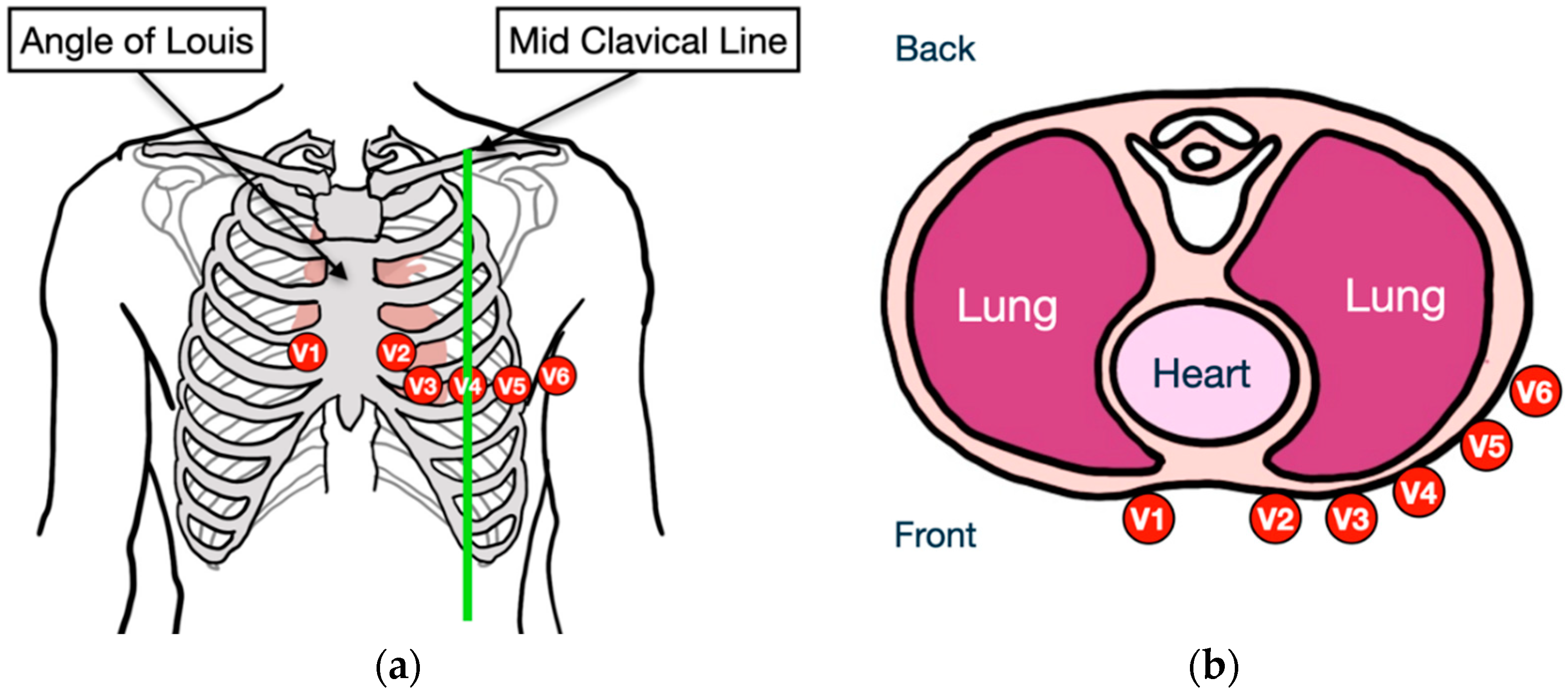
The traditional electrocardiogram (ECG) method involves two crucial steps. First, it is imperative to accurately identify the ribs and chest position to precisely determine the heart’s location (refer to Figure 1). Second, electrodes are strategically placed on the chest to record the heart’s electrical activity. Specifically, six positive electrodes—V1, V2, V3, V4, V5, and V6—are positioned based on specific arrangements [30]. In the context of ECG, the “V” in V1 through V6 stands for “Voltage”. Each lead is associated with a specific electrode placement on the chest, measuring electrical activity from different perspectives.
To ensure accurate electrode placement, learners tactually explore the chest by first locating the angle of Louis, which is the angle formed by the articulation of the manubrium (the uppermost part of the sternum), and the body of the sternum, identified when the subject is reclined due to the tighter surrounding tissue on the rib cage. Proceeding from the angle of Louis, learners move to the right, carefully navigating the rifts between the ribs for optimal electrode contact. This rift, located in the second intercostal space, serves as the starting point. Learners then move down, crossing the ribs, reaching the fourth intercostal space for V1 and opposite on the left side for V2. V4 is placed after moving further down to the 5th intercostal space and aligning with the middle of the clavicle. V3, situated between V2 and V4, follows the 5th intercostal space to the left, reaching below the origin of the axilla. This corresponds to the position of V5. Moving further along this line, slightly below the center point of the axilla, is where V6 is placed (Figure 1).
2.2. Overview Architecture of Proposed System
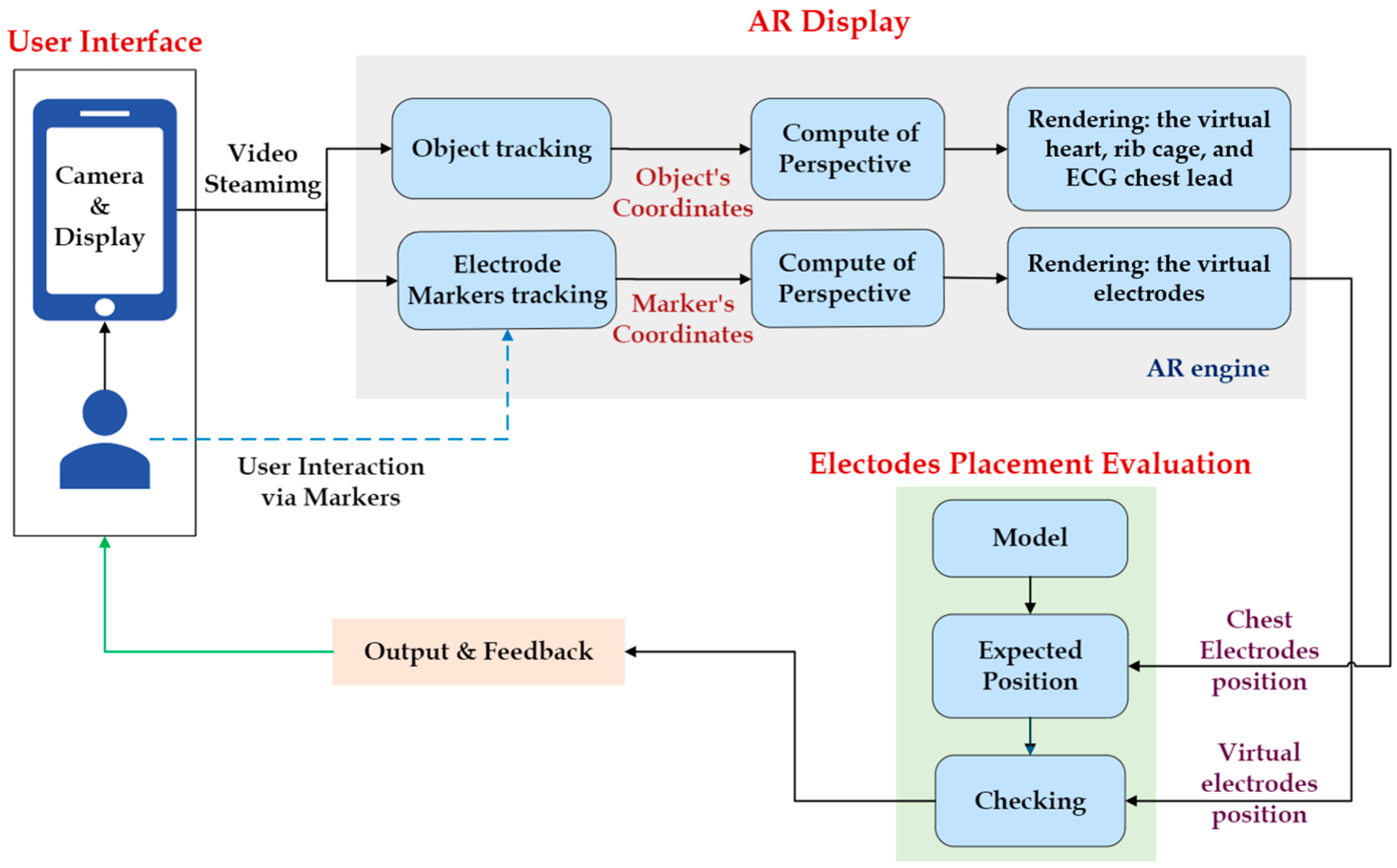
The proposed augmented reality consists of the following: (1) displaying, in which a smartphone running our augmented reality software projects an image of a virtual heart, ribcage, and chest lead onto a mannequin to demonstrate chest lead placement, and (2) training, in which the user may practice placing a virtual electrode on the mannequin, which interacts with an object-based marker base. The architecture of the proposed AR system for chest ECG electrode placement is illustrated in Figure 2.
In this section, we explain how to set each component in the AR application. We developed AR applications using the Unity 3D engine 2020.3, a Long-Term Support (LTS) release with an AR base. Unity is a game engine that can generate 2D and 3D graphics, offering drag-and-drop capabilities and supporting C# code. Unity can create a virtual world with three-dimensional qualities that replicate the real world. The AR Foundation within Unity allows us to manage augmented reality systems across several platforms (e.g., iOS, Android, OSX, and Windows).
2.2.1. AR Tracking
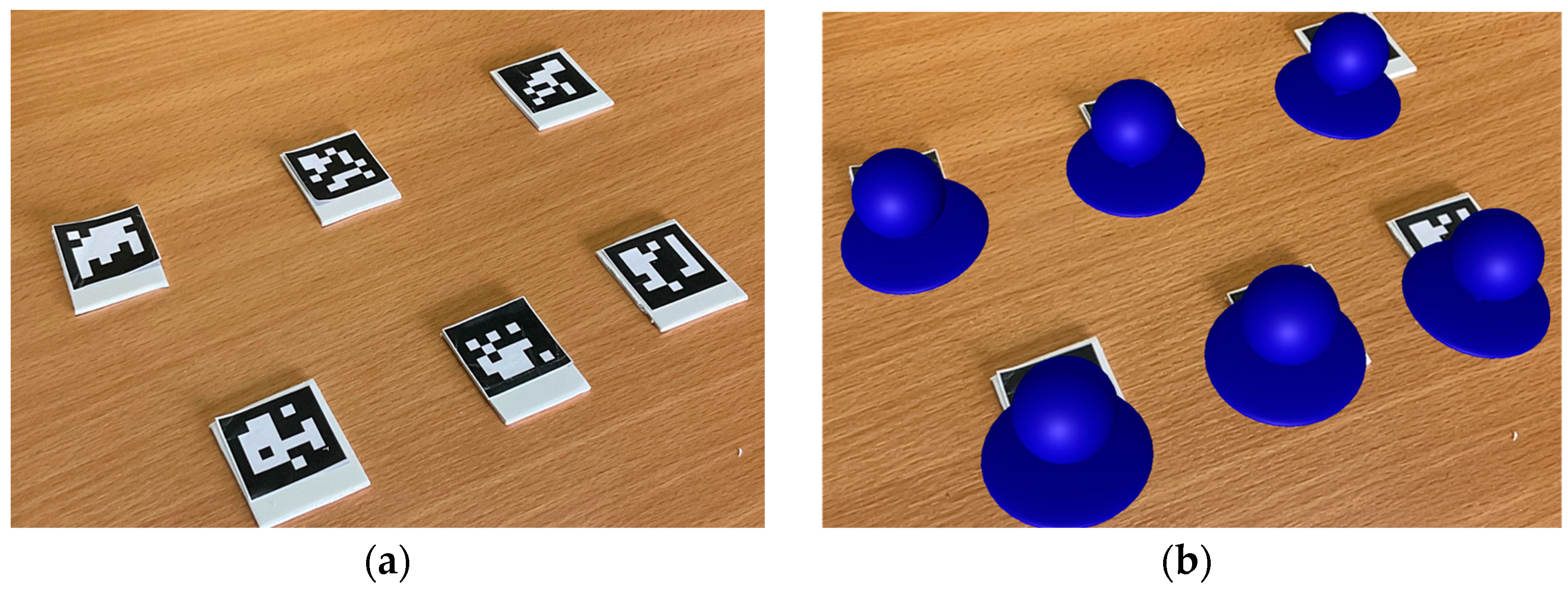
A marker-based technique is employed, using the image tracking feature in AR Foundation to identify the position and rotation of virtual ECG electrodes superimposed in the real world. In this technique, the input image includes a recognized pattern (fiducial marker) in the picture, which can detect and locate the marker [31,32]. The 2 × 2 cm square marker (Figure 3a) was used as a representative for a virtual electrode that matches the dimensions and shapes of real electrodes (2.5 × 2.5 cm) (Figure 3b). Typically, computer vision methods, feature detection, and pattern recognition are used for this operation. The output of marker-based AR is the marker’s 3D position and orientation in the virtual environment, along with any data contained in the marker. This information is utilized to create the appearance of augmented reality by aligning virtual electrodes with real-world markers, as shown in Figure 3.
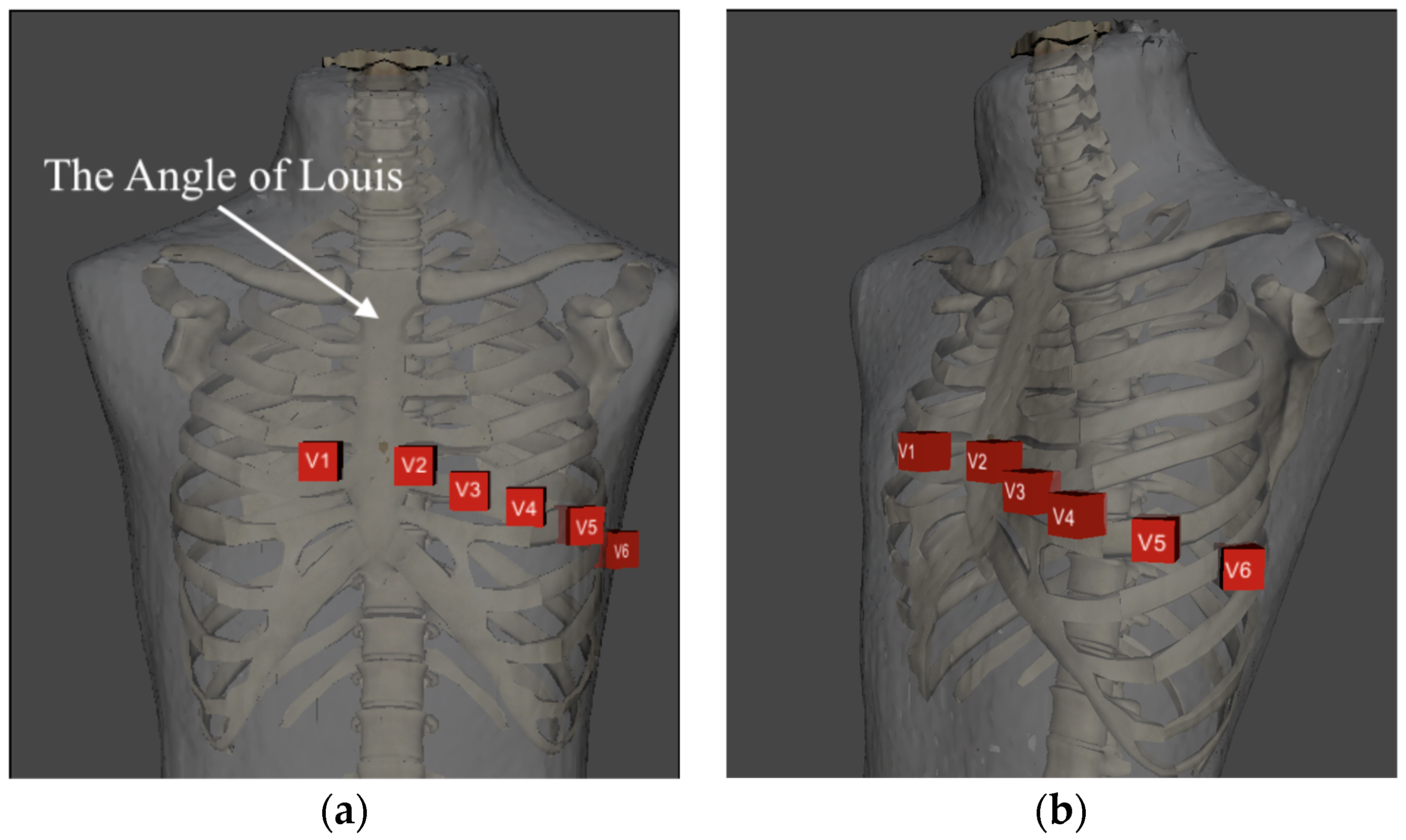
Object-based or object recognition techniques require a reference point to create the mannequin’s virtual rib cage and ECG chest lead locations (V1–V6). Recognizing the limitations of marker-based AR, which can detect only one plane of an object [33], we endeavored to showcase object detection in multiple planes, encompassing all dimensions. Object identification and tracking employ various methods for identifying and tracking positions and orientations, typically utilized in computer vision [34,35,36]. Using the Object Tracking feature of AR Foundation, we expanded our capabilities. This feature enables the recognition and continuous tracking of objects in the real world, facilitating a more dynamic and immersive augmented reality experience. Object tracking results display a 3D model of the mannequin, providing a dynamic and real-time representation of its position and orientation. This 3D model becomes the foundation upon which we can seamlessly overlay and place a virtual ECG chest lead, enhancing the accuracy and realism of the augmented reality experience. Point clouds emerge as a frequent and effective method for storing and visualizing virtual rib cages and ECG chest lead locations. Additionally, point clouds serve as the default format for acquisition devices to collect a scene’s depth, such as 3D scanners and depth sensors. A point cloud is a collection of three-dimensional spatial points representing an object’s external surface. Each sample is specified by its position, determined by the x-, y-, and z-coordinates, which can be tracked by the mannequin’s location for real-time display. Integrating the Object Tracking feature of AR Foundation enhances the accuracy and robustness of object identification and tracking, providing a comprehensive solution for creating and maintaining virtual elements within the augmented reality environment. Figure 4 illustrates the setting of the ECG chest lead position in Unity3d.
2.2.2. Integrated AR Display and Expert Confirmation
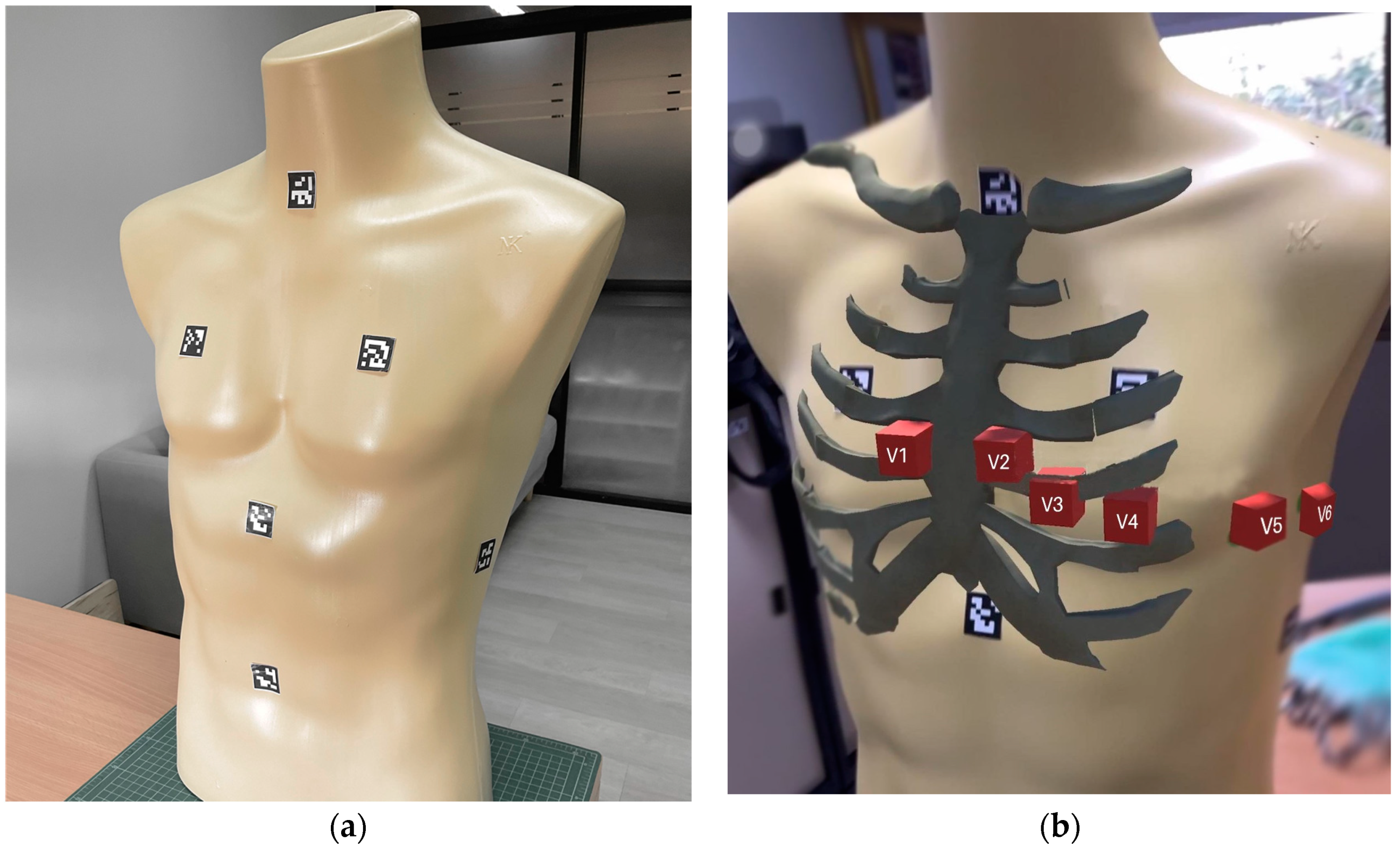
This study utilized AR technology on an iPad Pro with a LiDAR sensor and camera to offer real-time ECG chest lead placement training feedback. Acknowledging the inherent limitations of AR display that may lead to slight inaccuracies in rendering virtual ECG chest leads. We addressed this challenge by conducting a comprehensive confirmation process. Each nurse performed the procedure independently three times for verification. Three nursing experts, also lecturers from the School of Nursing at Walailak University, carried out the confirmation process. During each instance, a nurse affixed a sticker on each V to mark the true positions of the ECG chest leads on the mannequin. Subsequently, the augmented reality application displayed virtual ECG chest leads, and the center of the stickers was measured against the virtual leads. We used a Digital Vernier caliper to determine the error distance of the proposed AR application. The average error distance of the proposed AR application is presented in Table 1 and is derived from the measurements taken during the confirmation process.
In our setup, the virtual ECG chest lead was designed to be 3 × 3 cm for each V, accounting for the size of the real ECG electrode (2.5 cm) plus an average error distance of 0.44 cm identified during each of the three confirmation rounds. This sizing approach aims to provide a more accurate representation and account for potential variations in AR display accuracy. The associated results, as illustrated in Figure 5, showcase the dynamic and real-time representation of the virtual ECG chest lead positions aligned with the mannequin.
2.2.3. Electrode Placement Evaluation
Marker-based techniques for user interaction have been widely used in education and medicine [37,38]. This study examines the interaction between marker-based and object-based approaches in providing real-time feedback for ECG chest lead placement training. Following the AR display, the position of the virtual ECG electrode was compared to the virtual ECG lead positions to provide real-time feedback on their alignment.
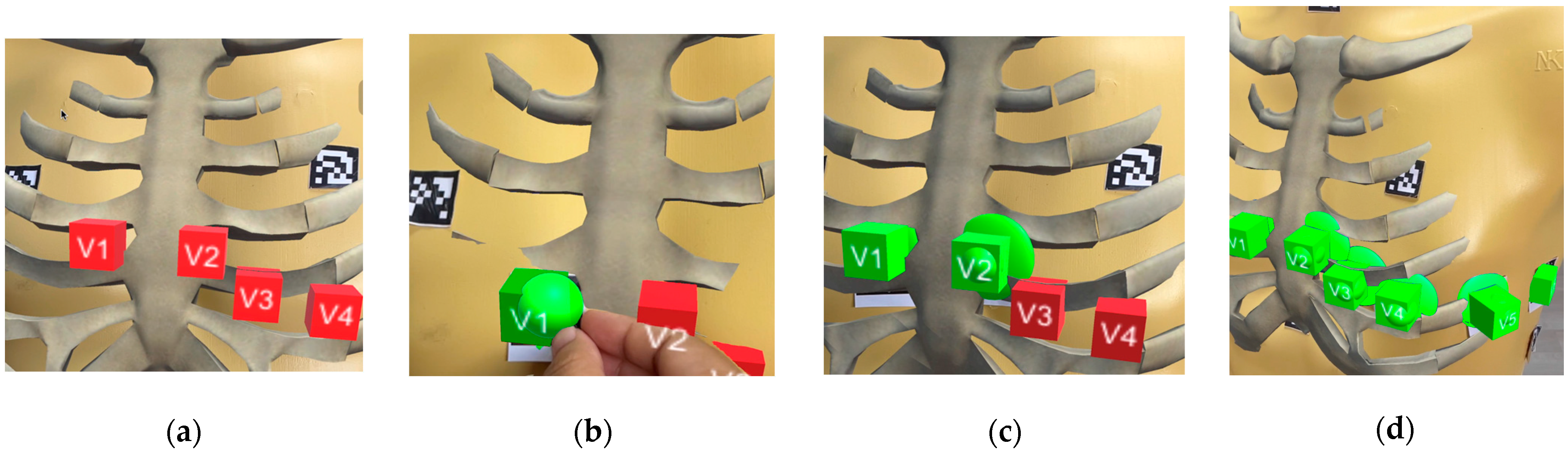
In Unity, we implemented a robust feedback mechanism by utilizing the Collider component to define the physical shape of the virtual ECG electrode and detect collisions with the ECG lead positions. To ensure precision, we set the size of the collision detection to match the size of the virtual ECG chest lead. Additionally, we specified the collision area settings: if the center of the virtual electrode comes into contact with the boundary of the ECG lead positions, both turn green; otherwise, they turn red, as shown in Figure 6. The Collider component serves as a boundary, outlining the contours of the virtual ECG electrodes. Unity uses this boundary to determine precisely when the electrodes come into contact with the designated lead positions. Upon collision detection, a key element of the interaction design, we initiated a response mechanism. Specifically, we dynamically changed the color of the ECG lead positions and the virtual ECG electrode. This visual cue served as an immediate indicator that the virtual ECG electrode had been correctly aligned with the electrode positions. Setting the size of collision detection to match the virtual electrode size enhances the realism of the training scenario. It provides valuable real-time feedback to users, reinforcing correct placement techniques during ECG chest lead training. Following this feedback process, the AR system displays the feedback on the user’s devices, offering a comprehensive and immediate overview of the training outcomes. The proposed AR system, developed and optimized, has been seamlessly integrated into an application designed to run on iPad Pro. Users can now experience the interactive ECG chest lead placement training with real-time feedback conveniently on their iPad Pro devices, ensuring a portable and user-friendly learning experience.
3. Experiments
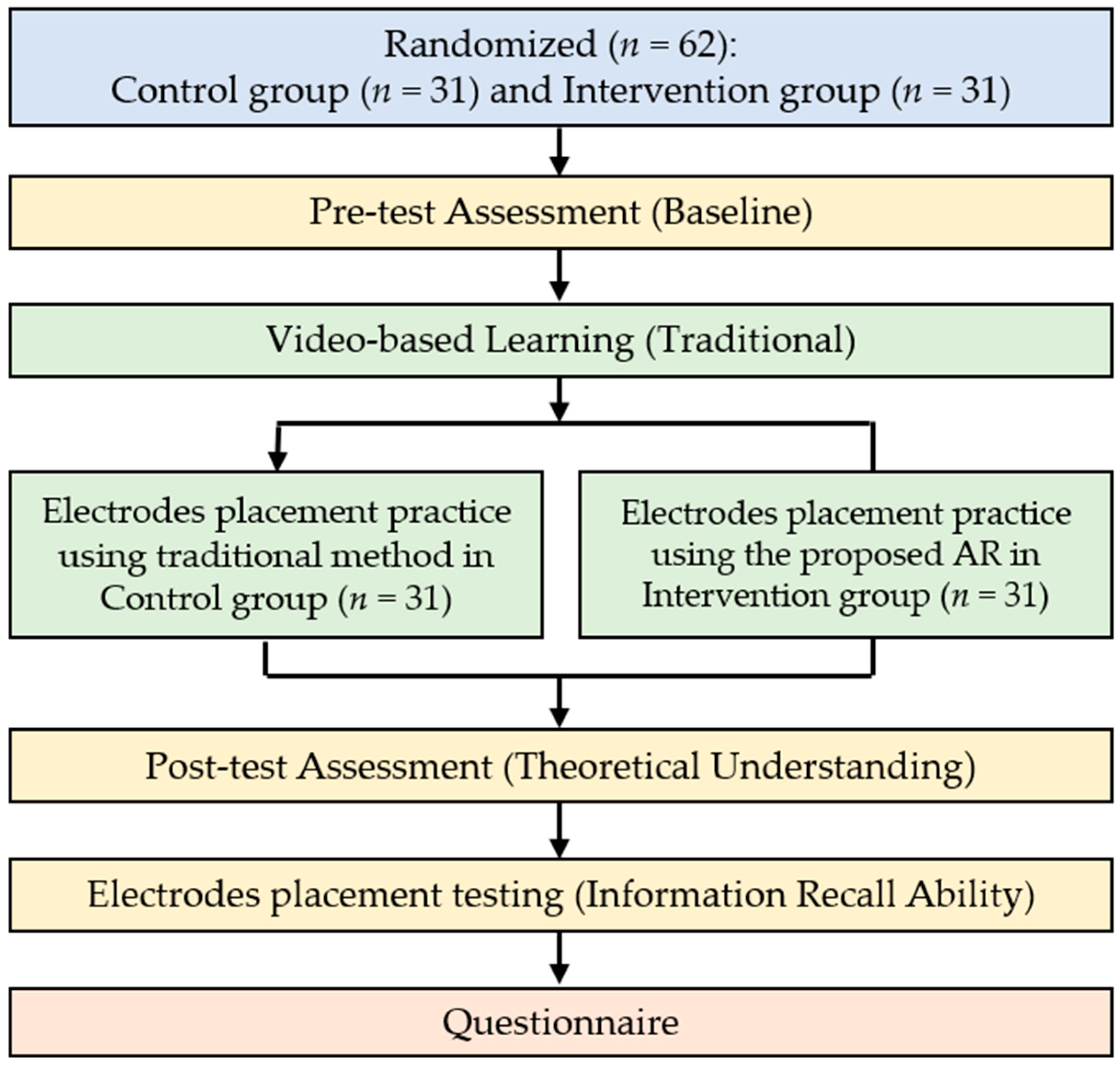
In this section, we provide a detailed description of the experiment employed in our study. We evaluated the effectiveness of the proposed AR application with a group of participants, specifically sixty-two students studying health science and technology (average age: 18 ± 1.6 years; 56 females and 6 males). None of the participants had any experience with chest ECG electrode placement. The experiments involving human subjects were approved by the Office of the Human Research Ethics Committee of Walailak University (WU-EC-IN-2-005-65, approval date: 7 February 2021), which acknowledges the Ethical Declaration of Helsinki, Council for International Organization of Medical Sciences and the World Health Organization guidelines. After receiving detailed information and reading the documentation, all participants provided written informed consent, which was kept confidential. The participants were randomly and equally divided into control and intervention groups. The learning and testing procedures are illustrated in Figure 7.
3.1. Experimental Objectives
Our primary research objectives:
- Verifying impact: This objective involved assessing the impact of the AR application on students’ learning efficiency, covering background theoretical knowledge and ECG electrode placement skills. The study was initiated with a pre-test, a crucial component of our learning assessment, to evaluate the participants’ baseline theoretical comprehension in the control and intervention groups. Subsequently, a post-test, another facet of our learning assessment, measured the increase in theoretical understanding after exposure to the AR application.
- Proving optimization: This study sought to demonstrate the application’s capacity to optimize the practice of positioning ECG electrodes on the chest. This entailed evaluating the operational efficiency of ECG electrode placement by assessing the accuracy of electrode positioning. To achieve this and further contribute to our optimization assessment, we conducted tests to measure participants’ information recall ability.
In addition, the final section of our study involved a questionnaire designed to gauge participants’ satisfaction with the learning methods. By delving into these objectives and incorporating participant feedback, the research aimed to verify the AR application’s impact on learning efficiency and prove its effectiveness in optimizing the practical aspect of ECG electrode placement on the chest.
3.2. Learning Assessment
We employed pre-tests and post-tests, each consisting of ten multiple-choice questions in Appendix A, to assess participants’ recall of specific details related to the placement sites of leads and their understanding of the significance and function of chest leads in an ECG. The assessment comprised two sections: pre-test and post-test. Both were administered through a Google Form. Although the questions were the same in both sections, they were presented in a different order, and the answers varied.
Before instruction or training, the pre-test established a baseline for participants’ knowledge and comprehension of ECG placement theory and procedures. Simultaneously, as part of our study on the effectiveness of an AR application, we verified the impact of the pre-test on participants’ learning efficiency, covering background theoretical knowledge and ECG electrode placement skills. In contrast, the post-test evaluated the extent to which participants’ knowledge and comprehension improved after instruction and practice. Scores for the pre-test and post-test were determined based on the number of correct responses provided.
3.3. Learning Materials and Practice Session
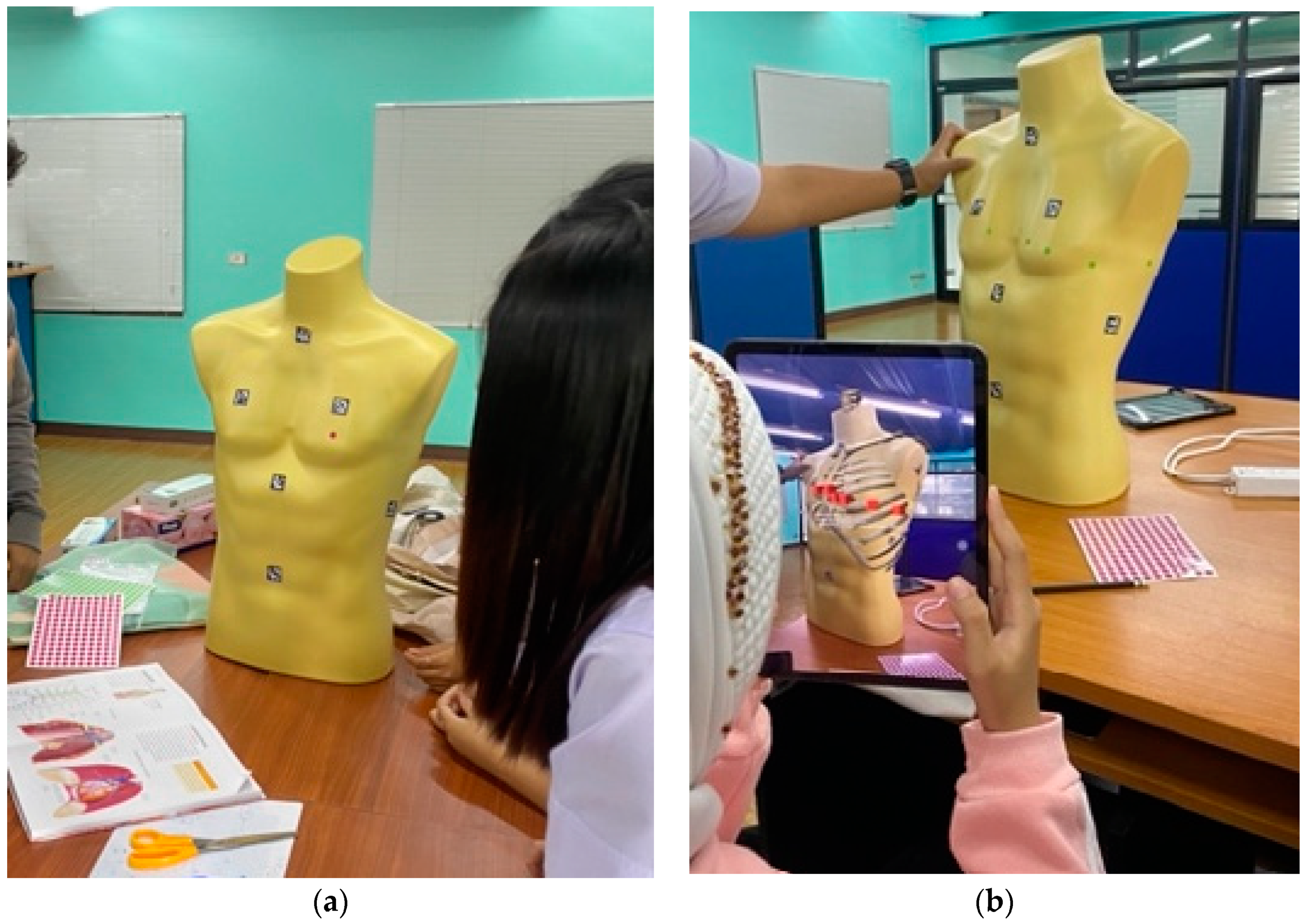
Regarding theoretical learning, our instructional approach involved providing two videos covering the content, importance, and factors of ECG signal data collection. The first video provided an overview of the ECG signal-collection process, whereas the second video explained the placement of electrodes on the chest and limbs and recommendations for using the equipment for detecting ECG signals. The total time for the participants to view both videos was approximately 15–20 min. Following the video presentations, the participants were divided into two groups for practical applications. The control group practiced placing ECG electrodes on a mannequin, whereas the intervention group used an AR app to practice electrode placement. For the electrode placement practice methods, as shown in Figure 8, we used a mannequin that resembled humans (22 × 45 × 65 cm) to locate the V1–V6 positions and placed the ECG electrodes in the correct position for an hour before testing. The students were grouped into ten small groups, each with six people. These groups were randomly divided into five control groups and five intervention groups. The control group employed the traditional methods of group discussion, knowledge-sharing, and practice (Figure 8a). The intervention group used the proposed AR application to practice ECG electrode placement (Figure 8b).
3.4. Testing of Information Recall Ability
Moreover, we assessed the chest ECG electrode placement proficiency in both participant groups to evaluate the information recall ability of traditional methods and the impact of the proposed AR application for practice. For this purpose, we conducted the ECG electrode positioning test individually for each participant. This test involved placing circular stickers measuring 2.5 cm on all six ECG locations on the mannequin’s chest. After each participant completed the test, we measured the distance error of electrode placement by assessing the space between the center of the sticker and the edge of the virtual ECG chest lead, with the simulation confirmed by the nurses. This method was applied to all participants in the study.
3.5. Satisfaction
The satisfaction questionnaire, comprising ten questions addressing various aspects for all group participants, was designed based on insights from an instructional material motivation survey [39] and guided by the proposed design [40]. In selecting a tailored approach, we aimed to ensure the questionnaire’s relevance to the unique context of ECG placement practice. Each question was evaluated using a five-point psychometric response scale, ranging from “Strongly Disagree” (1) to “Strongly Agree” (5). As detailed in Table 2, the specific pairing of questions (Q1 and Q7, Q2 and Q6, Q4 and Q8, Q5 and Q10, and Q3 and Q9) was instrumental in assessing learning interest, assembly task complexity, academic results, confidence factors, and satisfaction factors, respectively. This approach was chosen to better capture the intricacies of our study objectives and participants’ experiences.
4. Results
In this section, we present and compare the learning outcomes achieved using our applications and traditional methods. We assess theoretical knowledge through learning assessments and evaluate practical knowledge using information recall ability. Our analysis investigates whether there is a significant difference between the two groups regarding learning the theory of positioning the front ECG, the training results, and learning outcomes in terms of satisfaction. The statistical examination provides insights into the effectiveness of each approach and highlights potential distinctions between the two methodologies.
4.1. Theoretical Understanding
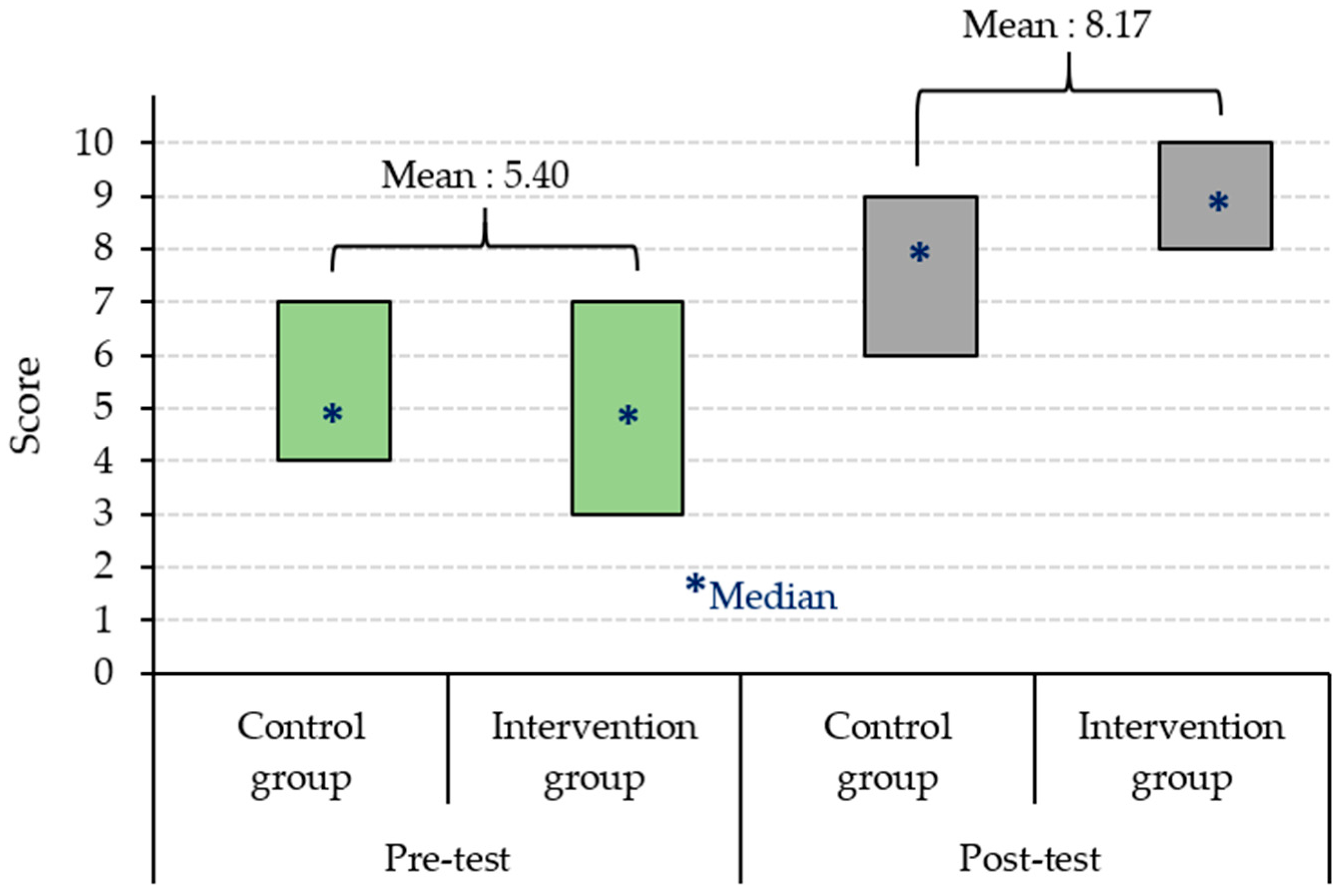
Table 3 and Table 4 show the mean scores obtained from the pre-test and post-test assessments, respectively, for the control and intervention groups. The unpaired t-test (n = 62) indicated no significant difference at the significance level of 0.05 between the control and intervention groups in the pre-test. Both groups exhibited similar levels of basic knowledge (baseline). However, the unpaired t-test indicated a significant difference in the post-test at the significance level of 0.05 between the control and intervention groups. Figure 9 compares the quartile range between the Control group and the Intervention group, revealing that the post-test score of the Control group had a quartile in the range of 7–8 points, and the intervention group had a quartile in the range of 8–9 points.
4.2. Information Recall Ability
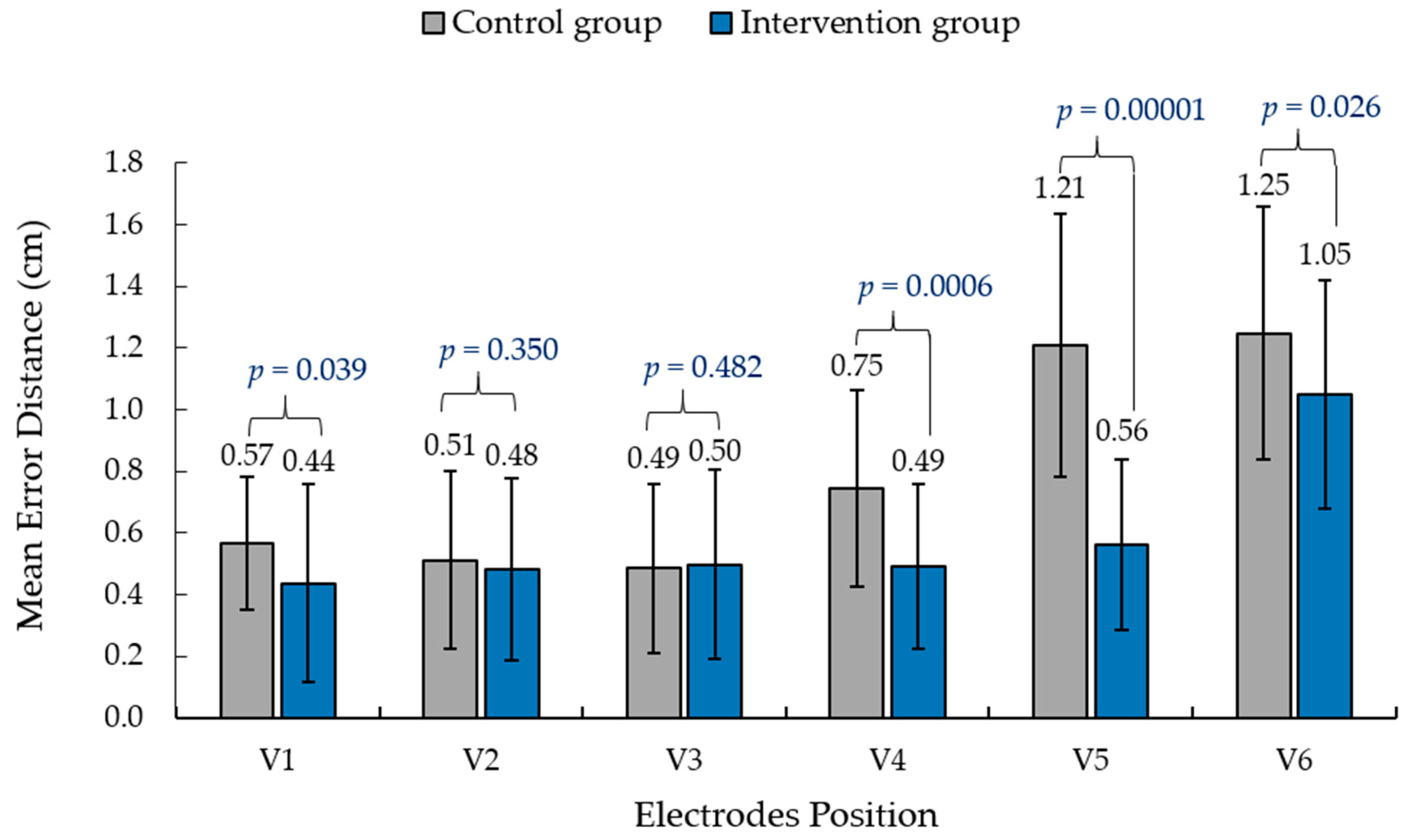
Figure 10 shows the average distance error and the standard deviation of electrode placement between the two groups. Prior to conducting t-tests, normality assumptions were checked using the Shapiro-Wilk test. Despite efforts to meet the normality assumption, the data did not exhibit a normal distribution. Therefore, the Mann-Whitney U-test, a non-parametric alternative, was chosen to compare the control and intervention groups. The average distance error for the AR application (intervention group) ranged from 0.44 cm to 1.03 cm, whereas that using the traditional method (control group) ranged from 0.49 cm to 1.25 cm. The unpaired t-test (n = 62) indicated significant differences at the significance level of 0.05 between the control and intervention groups for ECG chest lead electrodes at V1, V4, V5, and V6. The unpaired t-test (n = 62) indicated no significant differences at the significance level of 0.05 between the Control and Intervention groups for ECG chest lead electrodes at V2 and V3.
4.3. Satisfaction with Learning Methods
Table 5 presents the responses to the questionnaire. In evaluating the satisfaction levels derived from our augmented reality (AR) applications compared to traditional methods, our analysis focused on critical factors gauging student engagement and perceptions. First, regarding learning interest, the intervention group exhibited a significantly higher mean score (4.52 ± 0.57; range: 3–5) than the control group (3.32 ± 0.54; range: 2–4), indicating heightened interest in learning about the ECG chest lead. This trend was consistent with the task difficulty factor, where the intervention group perceived the ECG placement tasks as less difficult (3.94 ± 0.57; range: 3–5) compared to the control group (2.77 ± 0.67; range: 2–4). In assessing academic outcomes, the intervention group demonstrated superior performance (3.68 ± 0.65; range: 3–5) compared to the control group (2.97 ± 0.80; range: 2–4) regarding the structural composition and relative locations of ECG placements. Regarding confidence and mastery, the intervention group reported a significantly higher confidence level (4.65 ± 0.49; range: 4–5) than the control group (3.61 ± 0.50; range: 3–4) in their ability to place ECG electrodes. Additionally, the intervention group displayed enhanced mastery of the electrode placement order (4.10 ± 0.65; range: 3–5) compared to the control group (3.45 ± 0.57; range: 2–4). Overall satisfaction with the learning methods revealed substantial differences, with the intervention group reporting a significantly higher mean score (4.68 ± 0.48; range: 4–5) compared to the control group (2.87 ± 0.67; range: 1–4). Furthermore, the intervention group expressed greater eagerness to learn (4.55 ± 0.51; range: 4–5) compared to the control group (3.65 ± 0.75; range: 3–5).
5. Discussion
This section examines the learning outcomes arising from our AR applications compared to traditional methods. Our primary focus revolves around addressing fundamental research inquiries to provide essential insights.
In our comprehensive investigation into the impact of the AR application on students’ learning efficiency, encompassing theoretical knowledge and ECG electrode placement skills, conventional study methods demonstrated an increase in participants’ theoretical understanding. The average pre-test score was 5.45 and 7–8 points for the post-test, indicating a positive effect. Despite the Intervention group initially sharing a similar mean pre-test score with the Control group, the application significantly contributed to increasing the participants’ theoretical knowledge. Specifically, the intervention group’s average pre-test score was 5.32, and the post-test score showed a mean within the 8–9 range. This heightened interest and satisfaction can be attributed to the novelty of AR applications, as participants had no prior experience with such technology. The introduction of AR applications generated excitement and motivation, fostering a positive learning environment [18,41]. Consequently, the theory comprehension test showed that the intervention group answered more questions correctly than the control group. These findings align with our goal of enhancing learning efficiency through innovative educational technologies, confirming the positive impact on theoretical knowledge and emphasizing the app’s role in optimizing the learning experience. Additionally, in assessing learning interest and task difficulty, the intervention group exposed to AR demonstrated significantly higher learning interest, indicating the engaging nature of AR in learning about ECG chest leads. They perceived ECG placement tasks as less difficult than the control group, highlighting AR’s potential to reduce task difficulty.
In the context of optimizing ECG electrode placement training, our investigation highlights that the AR application’s utilization significantly improves electrode positioning precision, surpassing traditional methods. The outcomes of the practical knowledge test emphasize this enhancement, revealing that the intervention group consistently achieved greater accuracy in electrode placement across all positions compared to the control group. This positive trend aligns seamlessly with the satisfaction evaluation results, suggesting that the intervention group not only acquired a better understanding of the content but also demonstrated enhanced recall of electrode positions. Figure 10 visually represents the average distance error of electrode placement between the two groups of participants. The AR application (intervention group) exhibited superior precision, with an average distance error ranging from 0.44 cm to 1.03 cm. In comparison, the traditional method (control group) ranged from 0.49 cm to 1.25 cm. Statistical analysis, using an unpaired t-test (n = 62), identified a significant difference at the 0.05 significance level between the control and intervention groups for ECG chest lead electrodes at V1, V4, V5, and V6. However, no significant difference was observed for ECG chest lead electrodes at V2 and V3. These findings collectively underscore the AR application’s efficacy in enhancing theoretical knowledge and improving the precision of electrode placement in practical scenarios. The immersive experience facilitated by AR technology, simulating a virtual chest ECG, plays a key role in this optimization process [42]. The visual overlay of virtual ECG chest lead positions on the mannequin enhances participants’ understanding of ECG chest lead placement. This augmented comprehension supports participants’ confidence, particularly in positions V1 to V3. Despite these advancements, challenges arise for positions V4, V5, and V6, where positioning errors tend to escalate. The sideways placement of these electrodes introduces complexity, making observation challenging and contributing to sequential errors in electrode placement. Notably, in position V6, both groups exhibited an average positioning deviation of 1 cm from the actual location. This difference emphasizes the complications of positioning. To place the ECG chest lead position V6, it is necessary to align with position V5 in the same horizontal plane and place it precisely in the center of the left midaxillary line.
The overall findings accentuate the optimized learning and training outcomes achieved through the integration of the AR application for ECG electrode placement, supporting the second objective of optimization. Furthermore, in terms of confidence and mastery, students in the intervention group reported significantly higher confidence levels, signifying the contribution of AR applications to increased confidence in accurate electrode placement. Enhanced mastery of the electrode placement order in the intervention group suggests that AR technology aids in learning procedural aspects. Overall satisfaction and eagerness to learn were significantly higher in the intervention group, emphasizing the positive impact of AR applications on the overall learning experience, creating a more engaging and enjoyable learning environment than traditional methods [20,21].
6. Conclusions
This study evaluated the effectiveness of an AR application in enhancing the learning efficiency and accuracy of ECG chest lead placements. The results revealed that AR technology can enhance students’ comprehension of ECG chest lead placement. The post-test scores of the intervention group, which utilized the AR application, were significantly higher than those of the control group, which received traditional teaching materials. Additionally, the placement accuracy of ECG chest leads was significantly affected by position, and the AR application improved the accuracy in specific regions. The results of the questionnaire showed that students in the intervention group exhibited a greater level of interest and excitement in learning about ECG chest leads than those in the control group. Furthermore, the AR application facilitated active learning and increased the participants’ confidence in the ECG chest lead placement. Overall, this study suggests that incorporating AR technology into teaching ECG chest lead placement can improve accuracy and enhance learning efficiency. This research has significant implications for educators and healthcare professionals who aim to improve the training of ECG chest lead placement.
However, a critical consideration lies in the limitations inherent in our current analysis. The absence of corrections for multiple comparisons poses a potential challenge to interpreting our results. Recognizing this, we emphasize that addressing this limitation is not merely a future development but an imperative facet of ensuring the validity of our statistical analysis. Consequently, our commitment to implementing appropriate statistical methods to rectify this shortfall remains a priority in future research endeavors. This correction will undoubtedly contribute to fortifying the robustness and reliability of our findings, securing a more nuanced understanding of the impact of AR technology on ECG chest lead placement training.
Future developments of the AR application should focus on advanced functionalities, including simulating virtual chest ECG positions on real people, both male and female. Additionally, expanding the participant pool, conducting longitudinal studies, and exploring cross-disciplinary applications will contribute to a more comprehensive understanding of the AR technology’s potential. Moreover, further studies are required to explore the long-term impact of AR technology on ECG chest lead placement training and its potential use in other healthcare fields.
Author Contributions
Conceptualization, C.K., D.A., S.T.A. and Y.P.; methodology, C.K. and Y.P.; software, C.K. and Y.P.; validation, C.K., D.A., S.T.A. and Y.P.; formal analysis, C.K., D.A., S.T.A. and Y.P.; investigation, C.K. and Y.P.; resources, C.K. and Y.P.; data curation, C.K. and Y.P.; writing—original draft preparation, C.K. and Y.P.; writing—review and editing, C.K., D.A., S.T.A. and Y.P.; visualization, C.K. and Y.P.; supervision, C.K. and Y.P.; project administration, C.K. and Y.P.; funding acquisition, C.K. and Y.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was partially supported by Walailak University, Thailand.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Office of the Human Research Ethics Committee of Walailak University (WU-EC-IN-2-005-65, approval date: 7 February 2021).
Informed Consent Statement
Informed consent was obtained from all the participants involved in the study.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
This section presents the questions posed in the pre-test and post-test. The questions were the same in both sections, they were presented in a different order, and the position of the answer choices for each question was altered between the two tests. This adjustment was made to eliminate the possibility of participants relying on memorization of the order and to ensure a fair assessment of their knowledge. The questions are as follows:
- 1.
- How many chest leads are there in total?
- A)
- 4
- B)
- 6
- C)
- 8
- D)
- 10
- 2.
- Which chest lead is placed in the fourth intercostal space to the right of the sternum?
- A)
- V1
- B)
- V2
- C)
- V3
- D)
- V4
- 3.
- Which lead placement provides a view of the electrical activity in the left ventricle?
- A)
- V1 and V2
- B)
- V3 and V4
- C)
- V5 and V6
- D)
- None of the above
- 4.
- In which intercostal space is the V4 lead placed?
- A)
- Fourth intercostal space
- B)
- Fifth intercostal space
- C)
- Sixth intercostal space
- D)
- Seventh intercostal space
- 5.
- Which lead placement provides a view of the electrical activity in the right ventricle?
- A)
- V1 and V2
- B)
- V3 and V4
- C)
- V5 and V6
- D)
- None of the above
- 6.
- Which lead placement is used to diagnose hypertrophy of the left ventricle?
- A)
- V1
- B)
- V2
- C)
- V3
- D)
- V4
- 7.
- Which lead placement provides the inferior view of the heart?
- A)
- V1 and V2
- B)
- V3 and V4
- C)
- V5 and V6
- D)
- None of the above
- 8.
- Which lead placement provides the lateral view of the heart?
- A)
- V1 and V2
- B)
- V3 and V4
- C)
- V5 and V6
- D)
- None of the above
- 9.
- In which lead placement should the electrode be placed closest to the heart?
- A)
- V1
- B)
- V2
- C)
- V3
- D)
- V4
- 10.
- Which lead placement provides a view of the electrical activity in the mid-axillary line?
- A)
- V1
- B)
- V2
- C)
- V3
- D)
- V6
References
- Sirakaya, M.; Alsancak Sirakaya, D. Trends in educational augmented reality studies: A systematic review. Malays. Online J. Educ. Technol. 2018, 6, 60–74. [Google Scholar] [CrossRef]
- Pelet, J.E. (Ed.) Mobile Platforms, Design, and Apps for Social Commerce; IGI Global: Hershey, PA, USA, 2017. [Google Scholar]
- Eckert, M.; Volmerg, J.S.; Friedrich, C.M. Augmented reality in medicine: Systematic and bibliographic review. JMIR Mhealth Uhealth 2019, 7, e10967. [Google Scholar] [CrossRef] [PubMed]
- Bin, S.; Masood, S.; Jung, Y. Virtual and augmented reality in medicine. In Biomedical Information Technology; Elsevier: Amsterdam, The Netherlands, 2020; pp. 673–686. [Google Scholar] [CrossRef]
- Ferrari, V.; Klinker, G.; Cutolo, F. Augmented reality in healthcare. J. Healthc. Eng. 2019, 2019, 9321535. [Google Scholar] [CrossRef]
- Gerup, J.; Soerensen, C.B.; Dieckmann, P. Augmented reality and mixed reality for healthcare education beyond surgery: An integrative review. Int. J. Med. Educ. 2020, 11, 1–18. [Google Scholar] [CrossRef]
- Bui, D.T.; Barnett, T.; Hoang, H.T.; Chinthammit, W. Tele-mentoring using augmented reality technology in healthcare: A systematic review. Australas. J. Educ. Technol. 2021, 37, 68–88. [Google Scholar] [CrossRef]
- Aung, Y.M.; Al-Jumaily, A. AR based upper limb rehabilitation system. In Proceedings of the 2012 4th IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob), Rome, Italy, 24–27 June 2012; pp. 213–218. [Google Scholar] [CrossRef]
- Hondori, H.M.; Khademi, M.; McKenzie, A.; Dodakian, L.; Lopes, C.V.; Cramer, S.C. Abstract T MP43: Utility of augmented reality in relation to virtual reality in stroke rehabilitation. Stroke 2018, 45, 1. [Google Scholar] [CrossRef]
- Martín-Gutiérrez, J.; Saorín, J.L.; Contero, M.; Alcañiz, M.; Pérez-López, D.C.; Ortega, M. Design and validation of an augmented book for spatial abilities development in engineering students. Comput. Graph. 2010, 34, 77–91. [Google Scholar] [CrossRef]
- Akçayir, M.; Akçayir, G. Advantages and challenges associated with AR for education: A systematic review of the literature. Educ. Res. Rev. 2016, 20, 1–11. [Google Scholar] [CrossRef]
- Martín-Gutiérrez, J.; Fabiani, P.; Benesova, W.; Meneses, M.D.; Mora, C.E. Augmented reality to promote collaborative and autonomous learning in higher education. Comput. Hum. Behav. 2015, 51, 752–761. [Google Scholar] [CrossRef]
- Kamińska, D.; Zwoliński, G.; Laska-Leśniewicz, A.; Raposo, R.; Vairinhos, M.; Pereira, E.; Urem, F.; Ljubić Hinić, M.; Haamer, R.E.; Anbarjafari, G. Augmented Reality: Current and New Trends in Education. Electronics 2023, 12, 3531. [Google Scholar] [CrossRef]
- Di Serio, Á.; Ibáñez, M.B.; Kloos, C.D. Impact of an augmented reality system on students’ motivation for a visual art course. Comput. Educ. 2013, 68, 586–596. [Google Scholar] [CrossRef]
- Wu, H.K.; Lee, S.W.Y.; Chang, H.Y.; Liang, J.C. Current status, opportunities and challenges of augmented reality in education. Comput. Educ. 2013, 62, 41–49. [Google Scholar] [CrossRef]
- Kao, G.Y.M.; Ruan, C.A. Designing and evaluating a high interactive augmented reality system for programming learning. Comput. Hum. Behav. 2022, 132, 107245. [Google Scholar]
- Geng, X.; Yamada, M. An augmented reality learning system for Japanese compound verbs: Study of learning performance and cognitive load. Smart Learn. Environ. 2020, 7, 27. [Google Scholar] [CrossRef]
- Bujak, K.R.; Radu, I.; Catrambone, R.; MacIntyre, B.; Zheng, R.; Golubski, G. A psychological perspective on augmented reality in the mathematics classroom. Comput. Educ. 2013, 68, 536–544. [Google Scholar] [CrossRef]
- Lee, K. Augmented reality in education and training. TechTrends 2012, 56, 13–21. [Google Scholar] [CrossRef]
- Tang, Y.M.; Chau, K.Y.; Kwok, A.P.K.; Zhu, T.; Ma, X. A systematic review of immersive technology applications for medical practice and education-trends, application areas, recipients, teaching contents, evaluation methods, and performance. Educ. Res. Rev. 2022, 35, 100429. [Google Scholar] [CrossRef]
- Dhar, P.; Rocks, T.; Samarasinghe, R.M.; Stephenson, G.; Smith, C. Augmented reality in medical education: Students’ experiences and learning outcomes. Med. Educ. Online 2021, 26, 1953953. [Google Scholar] [CrossRef]
- Parsons, D.; MacCallum, K. Current perspectives on augmented reality in medical education: Applications, affordances and limitations. Adv. Med. Educ. Pract. 2021, 12, 77–91. [Google Scholar] [CrossRef]
- Kassutto, S.M.; Baston, C.; Clancy, C. Virtual, augmented, and alternate reality in medical education: Socially distanced but fully immersed. ATS Sch. 2021, 2, 651–664. [Google Scholar] [CrossRef]
- Xu, X.; Mangina, E.; Campbell, A.G. HMD-based virtual and augmented reality in medical education: A systematic review. Front. Virtual Real. 2021, 2, 692103. [Google Scholar] [CrossRef]
- Kugelmann, D.; Stratmann, L.; Nühlen, N.; Bork, F.; Hoffmann, S.; Samarbarksh, G.; Waschke, J. An augmented reality magic mirror as additive teaching device for gross anatomy. Ann. Anat. Anz. 2018, 215, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Gsaxner, C.; Pepe, A.; Wallner, J.; Schmalstieg, D.; Egger, J. Markerless image-to-face registration for untethered augmented reality in head and neck surgery. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Shenzhen, China, 13–17 October 2019; Springer: Cham, Switzerland, 2019; pp. 236–244. [Google Scholar]
- Barmaki, R.; Yu, K.; Pearlman, R.; Shingles, R.; Bork, F.; Osgood, G.M.; Navab, N. Enhancement of anatomical education using augmented reality: An empirical study of body painting. Anat. Sci. Educ. 2019, 12, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Ebner, F.; De Gregorio, A.; Schochter, F.; Bekes, I.; Janni, W.; Lato, K. Effect of an augmented reality ultrasound trainer app on the motor skills needed for a kidney ultrasound: Prospective trial. JMIR Serious Games 2019, 7, e12713. [Google Scholar] [CrossRef] [PubMed]
- McCann, K.; Holdgate, A.; Mahammad, R.; Waddington, A. Accuracy of ECG electrode placement by emergency department clinicians. Emerg. Med. Australas. 2007, 19, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Bifulco, P.; Narducci, F.; Vertucci, R.; Ambruosi, P.; Cesarelli, M.; Romano, M. Telemedicine supported by Augmented Reality: An interactive guide for untrained people in performing an ECG test. Biomed. Eng. Online 2014, 13, 153. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, A.L.; Goldberger, Z.D.; Shvilkin, A. Clinical Electrocardiography: A Simplified Approach E-Book; Elsevier Health Sciences: Philadelphia, PA, USA, 2017. [Google Scholar]
- Kato, H.; Billinghurst, M. Marker tracking and hmd calibration for a video-based augmented reality conferencing system. In Proceedings of the 2nd IEEE and ACM International Workshop on Augmented Reality (IWAR’99), San Francisco, CA, USA, 20–21 October 1999; pp. 85–94. [Google Scholar]
- Neumann, U.; You, S. Natural feature tracking for augmented reality. IEEE Trans. Multimed. 1999, 1, 53–64. [Google Scholar] [CrossRef]
- Alexiou, E.; Upenik, E.; Ebrahimi, T. Towards subjective quality assessment of point cloud imaging in augmented reality. In Proceedings of the 2017 IEEE 19th International Workshop on Multimedia Signal Processing (MMSP), Luton, UK, 16–18 October 2017; pp. 1–6. [Google Scholar]
- Dinayusadewi, N.P.; Agustika, G.N.S. Development of augmented reality application as a mathematics learning media in elementary school geometry materials. J. Educ. Technol. 2020, 4, 204–210. [Google Scholar] [CrossRef]
- Wake, N.; Rosenkrantz, A.B.; Huang, R.; Park, K.U.; Wysock, J.S.; Taneja, S.S.; Chandarana, H. Patient-specific 3D printed and augmented reality kidney and prostate cancer models: Impact on patient education. 3D Print. Med. 2019, 5, 4. [Google Scholar] [CrossRef]
- Rahmat, R.F.; Akbar, F.; Syahputra, M.F.; Budiman, M.A.; Hizriadi, A. Interactive augmented reality implementation of hijaiyah alphabet for children education. J. Phys. Conf. Ser. 2018, 978, 012102. [Google Scholar] [CrossRef]
- Muñoz-Saavedra, L.; Miró-Amarante, L.; Domínguez-Morales, M. Augmented and virtual reality evolution and future tendency. Appl. Sci. 2020, 10, 322. [Google Scholar] [CrossRef]
- Albertazzi, D.; Okimoto, M.L.; Ferreira, M.G.G. Developing an usability test to evaluate the use of augmented reality to improve the first interaction with a product. Work 2012, 41 (Suppl. S1), 1160–1163. [Google Scholar] [CrossRef] [PubMed]
- Bakri, F.; Marsal, O.; Muliyati, D. Textbooks equipped with augmented reality technology for physics topic in high-school. J. Penelit. Pengemb. Pendidik. Fis. 2019, 5, 113–122. [Google Scholar] [CrossRef]
- Fidan, M.; Tuncel, M. Integrating Augmented Reality into Problem Based Learning: The Effects on Learning Achievement and Attitude in Physics Education. Comput. Educ. 2019, 142, 103635. [Google Scholar] [CrossRef]
- Boonbrahm, P.; Kaewrat, C.; Boonbrahm, S. Interactive marker-based augmented reality for CPR training. Int. J. Technol. 2019, 10, 291–319. [Google Scholar] [CrossRef]
Figure 1.
Chest lead position of V1–V6. (a) Front view; (b) cross section of chest leads.

Figure 2.
System architecture of the proposed AR for the chest ECG electrode placement system.

Figure 3.
Virtual electrodes. (a) Markers used for the virtual display of electrodes; (b) virtual electrodes displayed on the marker via AR application.
Figure 3.
Virtual electrodes. (a) Markers used for the virtual display of electrodes; (b) virtual electrodes displayed on the marker via AR application.

Figure 4.
Virtual rib cage overlay on a mannequin. (a) Positioning the angle of Louis from the virtual rib; (b) display of virtual ECG chest lead (V1–V6).
Figure 4.
Virtual rib cage overlay on a mannequin. (a) Positioning the angle of Louis from the virtual rib; (b) display of virtual ECG chest lead (V1–V6).

Figure 5.
AR display. (a) Mannequin for object tracking; (b) AR display showing a virtual rib cage and the ECG chest lead positions (V1–V6).
Figure 5.
AR display. (a) Mannequin for object tracking; (b) AR display showing a virtual rib cage and the ECG chest lead positions (V1–V6).

Figure 6.
Example of the AR interaction sequence. (a) AR displays the virtual rib cage and ECG chest leads; (b) Placing the correct positioning of V1; (c) Correct ECG placement of V1 and V2 in green color and incorrect correct positioning of V3 and V4 in red color; (d) Correct ECG placement of all positions.
Figure 6.
Example of the AR interaction sequence. (a) AR displays the virtual rib cage and ECG chest leads; (b) Placing the correct positioning of V1; (c) Correct ECG placement of V1 and V2 in green color and incorrect correct positioning of V3 and V4 in red color; (d) Correct ECG placement of all positions.

Figure 7.
Process diagram of the learning methods and assessments.

Figure 8.
Example scenario during electrode placement practice. (a) Traditional method for the control group; (b) proposed AR for the intervention group.
Figure 8.
Example scenario during electrode placement practice. (a) Traditional method for the control group; (b) proposed AR for the intervention group.

Figure 9.
Comparison of the quartile range between the Control and Intervention groups.

Figure 10.
Average distance error for electrodes placement between the two groups of participants.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Average error distance for the proposed AR application.
| ECG Chest Lead Position | Average Error Distance ± SD (cm) |
|---|---|
| V1 | 0.31 ± 0.03 |
| V2 | 0.30 ± 0.03 |
| V3 | 0.21 ± 0.03 |
| V4 | 0.23 ± 0.03 |
| V5 | 0.44 ± 0.03 |
| V6 | 0.40 ± 0.04 |
| Mean | 0.31 ± 0.03 |
Table 2.
Satisfaction questionnaire.
| No. | Question |
|---|---|
| Q1 | My attention was quickly captured by the materials. |
| Q2 | I could easily complete the ECG placement tasks with guidance. |
| Q3 | I enjoy this method of learning. |
| Q4 | I have learned the ’structural composition and relative locations of ECG placements. |
| Q5 | I am confident that I can place all electrodes in the future. |
| Q6 | The ECG placement tasks were not difficult for me at all. |
| Q7 | I did not bored at the conclusion of the course. |
| Q8 | I have mastered the order of electrode placement for ECG chest leads. |
| Q9 | I am eager to learn more about the ECG placement through this course. |
| Q10 | I was confident in my knowledge of the course material. |
Table 3.
Mean scores obtained from the pre-test.
| Participants | Mean Score | SD | Z-Score | p-Value | Result |
|---|---|---|---|---|---|
| Control group | 5.45 | 0.97 | 0.640 | 0.32 | Not significant |
| Intervention group | 5.32 | 1.21 |
Table 4.
Mean scores obtained from the post-test.
| Participants | Mean Score | SD | Z-Score | p-Value | Result |
|---|---|---|---|---|---|
| Control group | 7.61 | 0.76 | −4.476 | 0.00001 | Significant |
| Intervention group | 8.74 | 0.77 |
Table 5.
Average satisfaction score of ECG electrode placement practice from each group of participants.
Table 5.
Average satisfaction score of ECG electrode placement practice from each group of participants.
| Factor | Question No. | Group | Range | Median | Mean ± SD |
|---|---|---|---|---|---|
| Learning Interest | Q1 | Control | 2–4 | 3 | 3.32 ± 0.54 |
| Intervention | 3–5 | 5 | 4.52 ± 0.57 | ||
| Q7 | Control | 1–3 | 2 | 2.32 ± 0.70 | |
| Intervention | 4–5 | 5 | 4.58 ± 0.50 | ||
| Task Difficulty | Q2 | Control | 2–4 | 3 | 2.77 ± 0.67 |
| Intervention | 3–5 | 4 | 3.94 ± 0.57 | ||
| Q6 | Control | 3–5 | 3 | 3.52 ± 0.57 | |
| Intervention | 3–5 | 4 | 3.71 ± 0.59 | ||
| Academic Outcome | Q4 | Control | 2–4 | 3 | 2.97 ± 0.80 |
| Intervention | 3–5 | 4 | 3.68 ± 0.65 | ||
| Q8 | Control | 2–4 | 3 | 3.45 ± 0.57 | |
| Intervention | 3–5 | 4 | 4.10 ± 0.65 | ||
| Confidence | Q5 | Control | 3–4 | 4 | 3.61 ± 0.50 |
| Intervention | 4–5 | 5 | 4.65 ± 0.49 | ||
| Q10 | Control | 2–5 | 3 | 3.65 ± 0.91 | |
| Intervention | 3–5 | 4 | 3.94 ± 0.68 | ||
| Satisfaction | Q3 | Control | 1–4 | 3 | 2.87 ± 0.67 |
| Intervention | 4–5 | 5 | 4.68 ± 0.48 | ||
| Q9 | Control | 3–5 | 3 | 3.65 ± 0.75 | |
| Intervention | 4–5 | 5 | 4.55 ± 0.51 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kaewrat, C.; Anopas, D.; Aung, S.T.; Punsawad, Y. Application of Augmented Reality Technology for Chest ECG Electrode Placement Practice. Informatics 2024, 11, 5. https://doi.org/10.3390/informatics11010005
AMA Style
Kaewrat C, Anopas D, Aung ST, Punsawad Y. Application of Augmented Reality Technology for Chest ECG Electrode Placement Practice. Informatics. 2024; 11(1):5. https://doi.org/10.3390/informatics11010005
Chicago/Turabian StyleKaewrat, Charlee, Dollaporn Anopas, Si Thu Aung, and Yunyong Punsawad. 2024. "Application of Augmented Reality Technology for Chest ECG Electrode Placement Practice" Informatics 11, no. 1: 5. https://doi.org/10.3390/informatics11010005
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.