Temporal and Atemporal Provider Network Analysis in a Breast Cancer Cohort from an Academic Medical Center (USA)

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Network Representation
2.3. Network Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- van Beek, A.P. Communication, advice exchange and job satisfaction of nursing staff: A social network analyses of 35 long-term care units. BMC Health Serv. Res. 2011, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Creswick, N.; Westbrook, J.I.; Braithwaite, J. Understanding communication networks in the emergency department. BMC Health Serv. Res. 2009, 9, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Alexander, G.L.; Steege, L.M.; Pasupathy, K.S.; Wise, K. Case studies of IT sophistication in nursing homes: A mixed method approach to examine communication strategies about pressure ulcer prevention practices. Int. J. Ind. Ergon. 2015, 49, 156–166. [Google Scholar] [CrossRef]
- Alexander, G.L.; Pasupathy, K.S.; Steege, L.M.; Strecker, E.B.; Carley, K.M. Multi-disciplinary communication networks for skin risk assessment in nursing homes with high IT sophistication. Int. J. Ind. Ergon. 2014, 83, 581–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steitz, B.D.; Levy, M.A. A social network analysis of cancer provider collaboration. AMIA Annu. Symp. Proc. 2016, 2016, 1987–1996. [Google Scholar] [PubMed]
- Barnett, M.L.; Landon, B.E.; O’Malley, A.J.; Keating, N.L.; Christakis, N.A. Mapping physician networks with self-reported and administrative data. Health Serv. Res. 2011, 46, 1592–1609. [Google Scholar] [CrossRef] [PubMed]
- Boyer, L.; Belzeaux, R.; Maurel, O.; Baumstarck Barrau, K.; Samuelian, J.C. A social network analysis of healthcare professional relationships in a French hospital. Int. J. Health Care Qual. Assur. 2010, 23, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Rangachari, P. Knowledge sharing networks related to hospital quality measurement and reporting. Health Care Manag. Rev. 2008, 33, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Wiemken, T.L.W.P.M.; Ramirez, J.A.R.M.; Polgreen, P.P.M.; Peyrani, P.P.; Carrico, R.M.C.P.R.F. Evaluation of the knowledge-sharing social network of hospital-based infection preventionists in Kentucky. Am. J. Infect. Control 2012, 40, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Menchik, D.A.; Meltzer, D.O. The cultivation of esteem and retrieval of scientific knowledge in physician networks. J. Health Soc. Behav. 2010, 51, 137–152. [Google Scholar] [CrossRef] [PubMed]
- Creswick, N.; Westbrook, J.I. Social network analysis of medication advice-seeking interactions among staff in an Australian hospital. Int. J. Med. Inform. 2010, 79, e116–e125. [Google Scholar] [CrossRef] [PubMed]
- Sabot, K.; Wickremasinghe, D.; Blanchet, K.; Avan, B.; Schellenberg, J. Use of social network analysis methods to study professional advice and performance among healthcare providers: A systematic review. Syst. Rev. 2017, 6, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Barnett, M.L.; Christakis, N.A.; O’Malley, J.; Onnela, J.-P.; Keating, N.L.; Landon, B.E. Physician patient-sharing networks and the cost and intensity of care in US hospitals. Med. Care 2012, 50, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Bridewell, W.; Das, A.K. Social network analysis of physician interactions: The effect of institutional boundaries on breast cancer care. AMIA Annu. Symp. Proc. 2011, 2011, 152–160. [Google Scholar]
- Iwashyna, T.J.; Christie, J.D.; Moody, J.; Kahn, J.M.; Asch, D.A. The structure of critical care transfer networks. Med. Care 2009, 47, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Chambers, D.; Wilson, P.; Thompson, C.; Harden, M. Social network analysis in healthcare settings: A systematic scoping review. PLoS ONE 2012, 7, e41911. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, S.; Faust, K. Social Network Analysis: Methods and Applications; Cambridge University Press: New York, NY, USA, 1994. [Google Scholar]
- O’Malley, A.J.; Marsden, P.V. The analysis of social networks. Health Serv. Outcomes Res. Method 2008, 8, 222–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, D.; Rosen, D.W.; Wang, L.; Schaefer, D. Cloud-based design and manufacturing: A new paradigm in digital manufacturing and design innovation. Comput. Aided Des. 2015, 59, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Casper, S. How do technology clusters emerge and become sustainable? Res. Policy 2007, 36, 438–455. [Google Scholar] [CrossRef]
- Cross, R.; Borgatti, S.P.; Parker, A. Making invisible work visible: Using social network analysis to support strategic collaboration. Calif. Manag. Rev. 2002, 44, 25–46. [Google Scholar] [CrossRef]
- Bonchi, F.; Castillo, C.; Gionis, A.; Jaimes, A. Social network analysis and mining for business applications. ACM Trans. Intell. Syst. Technol. 2011, 2, 1–37. [Google Scholar] [CrossRef]
- Larruscain, J.; Río-Belver, R.; Arraibi, J.R.; Garechana, G. Efficiency in knowledge transmission in R&D project networks: European renewable energy sector. J. Renew. Sustain. Energy 2017, 9, 065908. [Google Scholar]
- Latora, V.; Marchiori, M. Is the Boston subway a small-world network? Phys. A Stat. Mech. Appl. 2002, 314, 109–113. [Google Scholar] [CrossRef] [Green Version]
- Tichy, N.M.; Tushman, M.L.; Fombrun, C. Social network analysis for organizations. Acad. Manag. Rev. 1979, 4, 507–519. [Google Scholar] [CrossRef]
- Oborn, E.; Dawson, S. Knowledge and practice in multidisciplinary teams: Struggle, accommodation and privilege. Hum. Relat. 2010, 63, 1835–1857. [Google Scholar] [CrossRef]
- Hartgerink, J.M.; Cramm, J.M.; Bakker, T.J.E.M.; van Eijsden, A.M.; Mackenbach, J.P.; Nieboer, A.P. The importance of multidisciplinary teamwork and team climate for relational coordination among teams delivering care to older patients. J. Adv. Nurs. 2013, 70, 791–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schepman, S.; Hansen, J.; de Putter, I.D.; Batenburg, R.S.; de Bakker, D.H. The common characteristics and outcomes of multidisciplinary collaboration in primary health care: A systematic literature review. Int. J. Integr. Care 2015, 15, e027. [Google Scholar] [CrossRef] [PubMed]
- Committee on Quality of Health Care in America, Institute of Medicine (US). Crossing the Quality Chasm: A New Health System for the 21st Century; The National Academies Press: Washington, DC, USA, 2001.
- Shannon, D. Effective physician-to-physician communication: An essential ingredient for care coordination. Phys. Exec. 2012, 38, 16–21. [Google Scholar]
- Kesson, E.M.; Allardice, G.M.; George, W.D.; Burns, H.J.G.; Morrison, D.S. Effects of multidisciplinary team working on breast cancer survival: Retrospective, comparative, interventional cohort study of 13,722 women. BMJ 2012, 344, e2718. [Google Scholar] [CrossRef] [PubMed]
- McDonald, K.M.; Sundaram, V.; Bravata, D.M.; Lewis, R.; Lin, N.; Kraft, S.A.; McKinnon, M.; Paguntalan, H.; Owens, D.K. Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies; Agency for Healthcare Research and Quality (AHRQ): Rockville, MD, USA, 2007; Volume 7.
- Peikes, D.; Chen, A.; Schore, J.; Brown, R. Effects of care coordination on hospitalization, quality of care, and health care expenditures among medicare beneficiaries. JAMA 2009, 301, 603–616. [Google Scholar] [CrossRef] [PubMed]
- Forster, A.J. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann. Intern. Med. 2003, 138, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Casteigts, A.; Flocchini, P.; Quattrociocchi, W.; Santoro, N. Time-varying graphs and dynamic networks. Int. J. Parallel Emerg. Distrib. Syst. 2012, 27, 387–408. [Google Scholar] [CrossRef] [Green Version]
- Cancer Registry. Available online: https://seer.cancer.gov/registries/cancer_registry/cancer_registry.html (accessed on 30 July 2018).
- Tennessee Cancer Registry. Available online: https://www.tn.gov/health/health-program-areas/tcr.html (accessed on 30 July 2018).
- Pollack, C.E.; Weissman, G.E.; Lemke, K.W.; Hussey, P.S.; Weiner, J.P. Patient sharing among physicians and costs of care: A network analytic approach to care coordination using claims data. J. Gen. Intern. Med. 2012, 28, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Csardi, G.; Nepusz, T. The igraph software package for complex network research. InterJournal Complex Syst. 2006, 1695, 1–9. [Google Scholar]
- Team, R.C. R: A Language and Environment for Statistical Computing, version 3.0; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Samarth, C.N.; Gloor, P.A. Process efficiency. Redesigning social networks to improve surgery patient flow. J. Healthc. Inf. Manag. 2009, 23, 20–26. [Google Scholar] [PubMed]
- Merrill, J.A.; Sheehan, B.M.; Carley, K.M.; Stetson, P.D. Transition networks in a cohort of patients with congestive heart failure. Appl. Clin. Inform. 2015, 6, 548–564. [Google Scholar] [PubMed]
- Chen, Y.; Kho, A.N.; Liebovitz, D.; Ivory, C.; Osmundson, S.; Bian, J.; Malin, B.A. Learning bundled care opportunities from electronic medical records. J. Biomed. Inform. 2018, 77, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Xie, W.; Gunter, C.A.; Liebovitz, D.; Mehrotra, S.; Zhang, H.; Malin, B. Inferring clinical workflow efficiency via electronic medical record utilization. AMIA Annu. Symp. Proc. 2015, 2015, 416–425. [Google Scholar] [PubMed]
- Fowler, J.H.; Christakis, N.A. Dynamic spread of happiness in a large social network: Longitudinal analysis over 20 years in the Framingham Heart Study. BMJ 2008, 337, a2338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christakis, N.A.; Fowler, J.H. The collective dynamics of smoking in a large social network. N. Engl. J. Med. 2008, 358, 2249–2258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christakis, N.A.; Fowler, J.H. Social contagion theory: Examining dynamic social networks and human behavior. Stat. Med. 2012, 32, 556–577. [Google Scholar] [CrossRef] [PubMed]
- Blanchet, K.; James, P. How to do (or not to do) … a social network analysis in health systems research. Health Policy Plan. 2012, 27, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Srinivasan, U.; Uddin, S.; Chawla, S. Application of network analysis on healthcare. In Proceedings of the IEEE/ACM International Conference on Advances in Social Network Analysis and Mining, Beijing, China, 17–20 August 2014; pp. 596–603. [Google Scholar]
- Steitz, B.D.; Weinberg, S.T.; Danciu, I.; Unertl, K.M. Managing and communicating operational workflow. Appl. Clin. Inform. 2016, 7, 59–68. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Calculation | Definition | Interpretation | |
|---|---|---|---|
| Network Density | The percentage of potential connections in a network that are actual connections. | A measure to quantify the relative degree of connectivity within a network. | |
| Network Care Density | The average number of patients shared per provider connection. | A measure to quantify the amount of patient sharing between providers in a network. | |
| Degree Centrality | The sum of unique connections adjacent to a single node. | The total number of connections associated with a single node. | The number of providers who share a patient with a single provider of interest. |
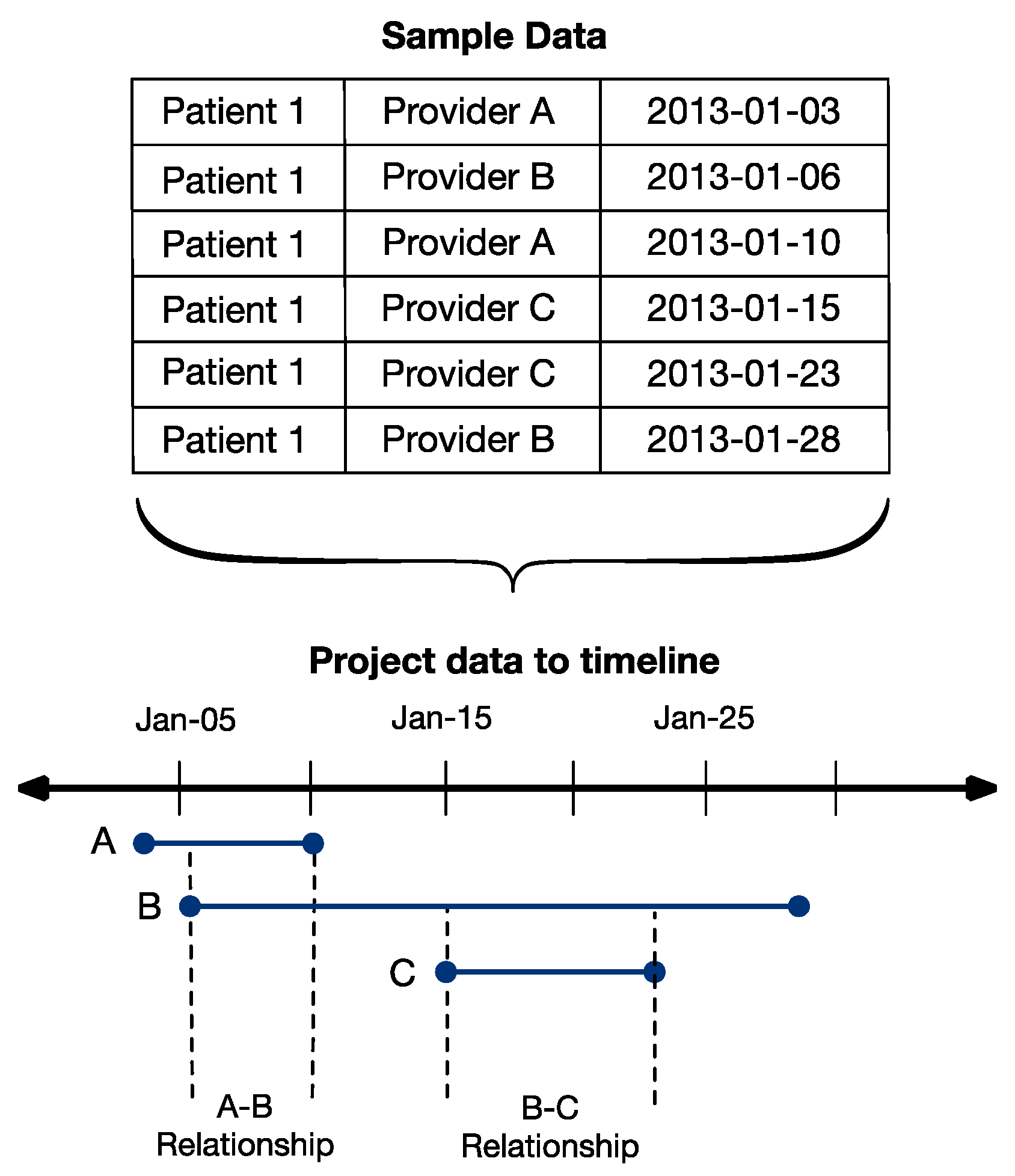
| Temporal Edge | Pair of providers associated with overlapping treatment of a single patient. | Connection between nodes relative to time at which each node was present in the network. | Provider–provider connections that represent instances in which care was likely coordinated. |
| Atemporal Edge | Pairwise combination of providers associated with treatment of a single patient. | Connection between nodes, irrespective of time when node was present in the network. | Provider–provider connections that represent potential connections based on caring for a shared patient. |
| Stage I | Stage II | Stage III | Stage I–III | |
|---|---|---|---|---|
| Number of Patients | 2116 | 1452 | 514 | 4082 |
| Number of Providers | 1090 | 948 | 503 | 2190 |
| Unique Temporal Edges | 35,402 | 23,265 | 9789 | 54,695 |
| Unique Atemporal Edges | 167,318 | 107,018 | 41,686 | 249,075 |
| Node Size | ||||
| Mean (range) | 16.3 (1, 1084) | 10.7 (1, 675) | 5.6 (1, 164) | 31.4 (1, 2351) |
| Median | 4 | 3 | 2 | 179 |
| Temporal Edge Size | ||||
| Mean (range) | 3.4 (1, 371) | 3.5 (1, 400) | 3.1 (1, 164) | 4.2 (1, 838) |
| Median | 2 | 2 | 2 | 2 |
| Atemporal Edge Size | ||||
| Mean (range) | 1.8 (1, 467) | 1.7 (1, 306) | 1.5 (1, 157) | 2.2 (1, 908) |
| Median | 1 | 1 | 1 | 1 |
| Providers per Patient | ||||
| Mean (range) | 15.3 (1, 414) | 15.1 (1, 64) | 15.7 (1, 44) | 15.3 (1, 74) |
| Median | 12 | 12 | 13 | 12 |
| Appointments per Patient | ||||
| Mean (range) | 70.5 (1, 414) | 72.8 (1, 498) | 80.4 (1, 363) | 72.7 (1, 498) |
| Median | 50 | 56 | 65 | 54 |
| Number of Diagnoses | Number of Patients | Number of Providers | Number of Temporal Edges | Number of Atemporal Edges | Sum of Temporal Edge Weights | Sum of Atemporal Edge Weights | Temporal Network Density | Atemporal Network Density | |
|---|---|---|---|---|---|---|---|---|---|
| 2002 | 155 | 1424 | 458 | 596 | 2033 | 1814 | 2831 | 1.56 | 1.57 |
| 2003 | 156 | 1678 | 533 | 1309 | 3355 | 4425 | 4843 | 1.52 | 1.62 |
| 2004 | 174 | 1840 | 569 | 1919 | 4273 | 6575 | 6239 | 1.7 | 1.76 |
| 2005 | 173 | 2023 | 631 | 2748 | 5095 | 9714 | 7550 | 1.73 | 1.7 |
| 2006 | 202 | 2249 | 682 | 3378 | 5340 | 12,082 | 8078 | 1.69 | 1.53 |
| 2007 | 205 | 2461 | 753 | 4372 | 6625 | 15,408 | 9993 | 1.63 | 1.6 |
| 2008 | 256 | 2625 | 786 | 5455 | 7962 | 18,805 | 12,177 | 1.66 | 1.63 |
| 2009 | 276 | 2799 | 790 | 7055 | 9453 | 24,153 | 14,800 | 1.85 | 1.79 |
| 2010 | 271 | 2989 | 863 | 9658 | 11,841 | 33,066 | 19,188 | 1.88 | 1.94 |
| 2011 | 303 | 3127 | 945 | 11,581 | 13,614 | 40,552 | 22,146 | 1.82 | 1.84 |
| 2012 | 331 | 3366 | 995 | 13,016 | 14,601 | 44,778 | 23,394 | 1.8 | 1.69 |
| 2013 | 406 | 3593 | 1038 | 14,663 | 16,387 | 51,366 | 27,015 | 1.84 | 1.74 |
| 2014 | 356 | 3711 | 1034 | 14,729 | 16,212 | 52,382 | 26,794 | 1.83 | 1.83 |
| 2015 | 418 | 3775 | 1074 | 15,366 | 17,493 | 52,505 | 28,240 | 1.66 | 1.76 |
| 2016 | 400 | 3826 | 1076 | 14,142 | 17,025 | 49,263 | 29,263 | 1.5 | 1.74 |
| Full-Time | Part-Time | |||||
|---|---|---|---|---|---|---|
| Medical Oncologist 1 | Medical Oncologist 2 | Medical Oncologist 3 | Medical Oncologist 4 | Medical Oncologist 5 | Medical Oncologist 6 | |
| Overall Degree Centrality | ||||||
| Temporal | 1159 | 1034 | 950 | 423 | 517 | 342 |
| Atemporal | 1963 | 1979 | 1864 | 994 | 1493 | 836 |
| Overall Care Density | ||||||
| Temporal | 12.3 | 12.3 | 14.2 | 6.9 | 7.8 | 5.4 |
| Atemporal | 7.2 | 6.4 | 7.2 | 2.9 | 2.7 | 2.2 |
| Yearly Temporal Care Density | ||||||
| Year 1 | 4.1 | 4.86 | 6.4 | 3.77 | 2 | 3.74 |
| Year 2 | 6.64 | 6.69 | 7.07 | 4.49 | 4 | 4.11 |
| Year 3 | 5.95 | 7.72 | 6.96 | 4.47 | 5.04 | 4.34 |
| Year 4 | 6.94 | 7.69 | 7.6 | 5.11 | 5.16 | 4.2 |
| Year 5 | 6.76 | 7.51 | 8.79 | 4.97 | 5.84 | 4.22 |
| Year 6 | 6.69 | 7.46 | 9.34 | 5.03 | 6.19 | |
| Year 7 | 6.76 | 6.86 | 9.33 | 5.49 | ||
| Year 8 | 7.38 | 7.23 | 9.36 | |||
| Year 9 | 7.64 | 7.24 | ||||
| Year 10 | 7.17 | 7.28 | ||||
| Year 11 | 7.23 | 6.74 | ||||
| Year 12 | 7.25 | |||||
| Year 13 | 6.68 | |||||
| Year 14 | 6.66 | |||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steitz, B.D.; Levy, M.A. Temporal and Atemporal Provider Network Analysis in a Breast Cancer Cohort from an Academic Medical Center (USA). Informatics 2018, 5, 34. https://doi.org/10.3390/informatics5030034
Steitz BD, Levy MA. Temporal and Atemporal Provider Network Analysis in a Breast Cancer Cohort from an Academic Medical Center (USA). Informatics. 2018; 5(3):34. https://doi.org/10.3390/informatics5030034
Chicago/Turabian StyleSteitz, Bryan D., and Mia A. Levy. 2018. "Temporal and Atemporal Provider Network Analysis in a Breast Cancer Cohort from an Academic Medical Center (USA)" Informatics 5, no. 3: 34. https://doi.org/10.3390/informatics5030034