
Personalized Medicine for the Critically Ill Patient: A Narrative Review

Department of Anesthesiology and Intensive Care, George Emil Palade University of Medicine, Pharmacy, Science and Technology of Targu Mures, 540139 Targu Mures, Romania
*
Author to whom correspondence should be addressed.
Processes 2022, 10(6), 1200; https://doi.org/10.3390/pr10061200
Submission received: 30 May 2022
/
Revised: 12 June 2022
/
Accepted: 14 June 2022
/
Published: 16 June 2022
(This article belongs to the Special Issue New Advances in Materials and Procedures for Precision Medicine)
Abstract
:Personalized Medicine (PM) is rapidly advancing in everyday medical practice. Technological advances allow researchers to reach patients more than ever with their discoveries. The critically ill patient is probably the most complex of all, and personalized medicine must make serious efforts to fulfill the desire to “treat the individual, not the disease”. The complexity of critically ill pathologies arises from the severe state these patients and from the deranged pathways of their diseases. PM constitutes the integration of basic research into clinical practice; however, to make this possible complex and voluminous data require processing through even more complex mathematical models. The result of processing biodata is a digitized individual, from which fragments of information can be extracted for specific purposes. With this review, we aim to describe the current state of PM technologies and methods and explore its application in critically ill patients, as well as some of the challenges associated with PM in intensive care from the perspective of economic, approval, and ethical issues. This review can help in understanding the complexity of, P.M.; the complex processes needed for its application in critically ill patients, the benefits that make the effort of implementation worthwhile, and the current challenges of PM.
1. What Is Personalized Medicine?
Personalized medicine (PM) is a concept that is increasingly referred to in medicine. This concept is seen as a solution through which the progress of ongoing research can be integrated into everyday medical practice. Medical research is a few steps ahead, owing to technological advancement. New clinical hypotheses can be constructed on the basis of an increase in data quantity and diversity. PM represents the integration of molecular data (systems biology) with clinical data from individual patients in order to develop a more accurate molecular taxonomy of diseases that enhances diagnosis and treatment and tailors disease management to the individual characteristics of each patient [1].
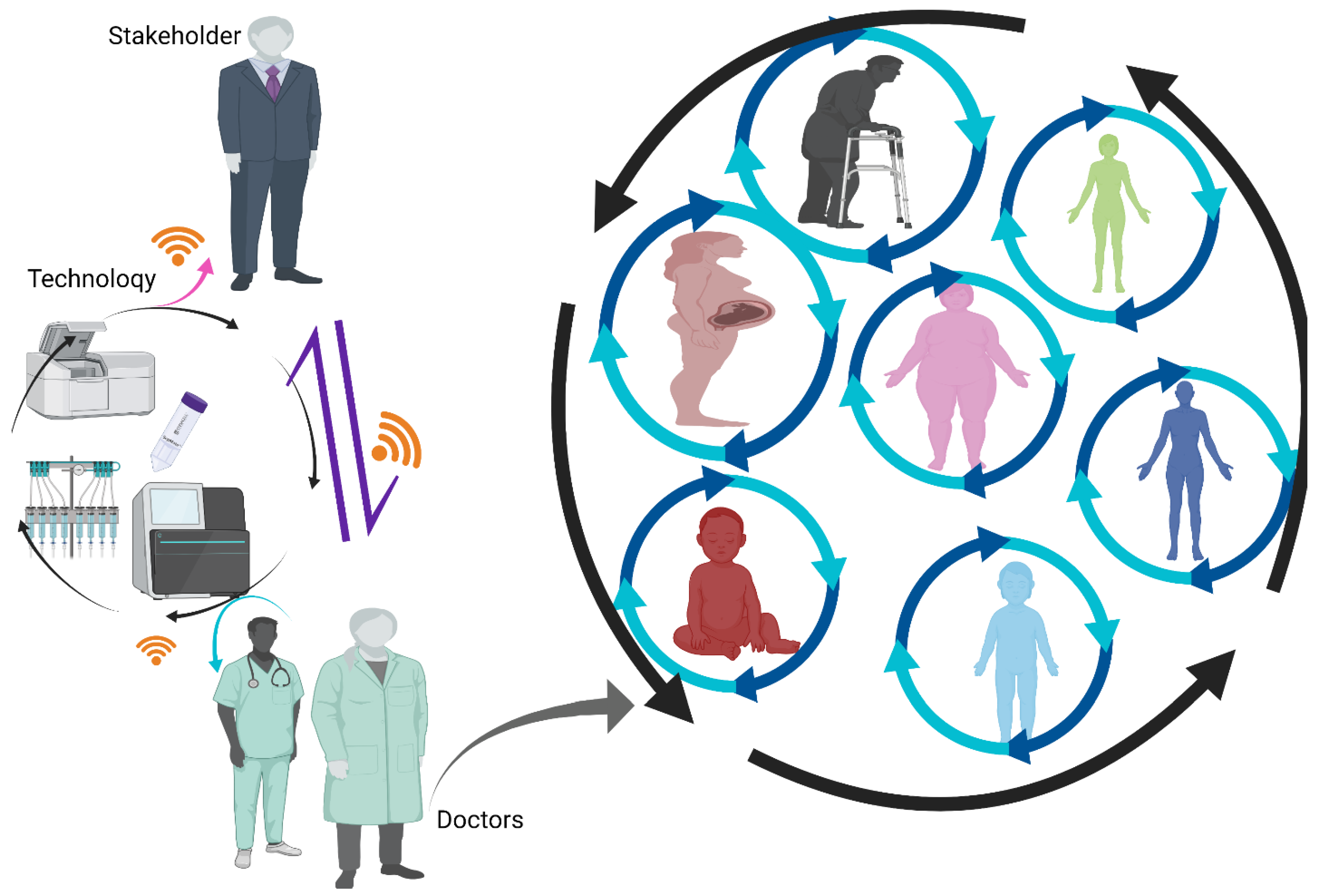
Precision medicine is defined as “an innovative approach that considers individual differences in people’s genes, environments, and lifestyles” to create unique sets of treatments tailored to the individual [2]. (Figure 1).
Conceptually, precision medicine and personalized medicine are identical. Both concepts focus on the individual and the disease or on a larger group of individuals with the same pathological/physiological features. An editorial about a personalized approach to cancer and diabetes triggered the inclusion of this concept in a governmental plan advanced by President Obama [3]. The President’s 2016 budget included investments in an emerging field of medicine that considers individual differences in people’s genes, microbiomes, environments, and lifestyles, making possible more effective, targeted treatments for diseases such as cancer and diabetes [4].
The first utilization of personalized medicine was in oncology and genetics, particularly in genomics, a branch of genetics that studies the response to certain treatments dependent upon genetic variability. Although nowadays, technologies allow for biomarker analysis and identification and it is estimated that a quarter of treatments have genetic variability, this information is not used in daily practice [5].
Personalized medicine can be seen as the integration of information from multiple sources to recreate the whole individual based solely on the gathered information, i.e., the big data. This information requires special processing and storage so that it can be accurately accessed and combined in such ways that the results of the analysis can be transposed into clinical practice. Therefore, specific technologies and processing methods are required so that personalized treatments, prognoses, or preventive measures can be applied in daily practice.
2. Big Data
In 2013, Goldman et al. established that 0 and 1 can be assigned to the well-known components of human DNA [6]. Based on this information, computers with living cells as their primary memory can be built, an advance which was incredibly well captured by Steve Jobs: “I think the biggest innovations of the 21st century will be at the intersection of biology and technology. A new era is beginning” [7].
With the data obtained from genome sequencing and the help of currently available omics technologies, we can digitize a human being in a similar manner to how maps are created in the Google application. We can unfold a human being as we would open a book and separately read each of its pages; however, in this situation, the pages would represent the results on the basis of different evaluations: biosensors, omics, imaging, scanners, social media, etc. All these results can be stored at different levels of storage, and when needed, the information can be corroborated to obtain a specific result with respect to a given problem that the individual may present with.
All the information we can obtain about one patient, including from all levels of genomics and clinical records, should be stored in one place so it is accessible at any time. This aspect is one of the main problems when it comes to personalized medicine because for so-called “big data”, which encompasses all possible information about an individual, software with the capacity to store, analyze, and process it is still being developed.
The obstacles that need to be overcome to store such a large amount of information consist of the “four Vs” [8].
Volume: the quantity and dimensionality of data.
Velocity: the speed at which data change in a short amount of time.
Variety: the multitude of categories of data sets.
Veracity: the quality and reliability of data.
2.1. Topological Data Analysis
Managing big data is demanding, even for high-end super computers. Nowadays, methods used to process biodata include known statistical methods, data ordination and/or clustering, and machine learning. These methods are used to analyze data in the established database Datasaurus, which offers the possibility to visualize data before committing to trusting the descriptive statistics [9]. The above-mentioned biodata processing methods can individually answer a given set of specific questions; however, they are far from mastering analysis of all the available biodata [10].
A possibility for analysis of such large, continuous biodata is a topological data analysis (TDA) mathematical model. TDA comprises schemes that pertain to “topology”, a field of mathematics that addresses abstract notions of shape and connectivity [11].
Two algorithms constitute the foundation of TDA:
- -
- Mapper, an algorithm used for data visualization and exploration; and
- -
- Persistent homology, which implies that similar data can be analyzed given the context that these data are found nearby or next to each other to create an individualized diagram with those data [12].
TDA can be applied to systems that generate a large amount of data, data with continuous character, and multiple scaling systems. TDA can summarize these data, preserving their essential topological relationships. The system can be integrated to work with other computer intelligence or machine learning tools to increase its computational capacity [13,14,15].
2.2. Machine Learning
Studies have shown that the applicability of machine learning (ML) in biomedicine is respectable when it comes to performing tasks such as diagnostics and prediction [14,16,17,18,19].
However, ML alone has serious limitations when interpreting big data due to data complexity and volume. If ML technologies could be interconnected with TDA technologies, the interpretability of biodata could become, to a point, faultless [20].
One example in this respect is represented by critically ill patients. These patients have complex diseases, many of them in advanced stages, as well as many organ failures. Each of these comorbidities represents a source of continuous variables, which could be explored in two ways:
- -
- From low risk to high risk, with the intent of evaluating the pathophysiology; or
- -
- From high risk to low risk in order to evaluate potential treatment options [11].
2.3. Digital Twins
- -
- Digital twins could be regarded as the ultimate technology for PM. This concept relies on a mathematical model that can summarize an individual’s unique physiology and further create personalized treatments [11]. The resulting biodata achieved by digital twinning could also be used to perform “in silico” tests with the intent of creating different computer-simulated disease models, along with possible treatments, which could further be transposed into reality [11]. As with other biodata used in the management of computational intelligence, the main limitation consists of managing large volumes and real-time data changes. To increase accuracy and facilitate biodata management, these mathematical models could be linked together with the goal of delivering correct solutions to patients [21].
2.4. Human Geographic Information System
Human characteristics can be mapped similarly to terrain. Geographic information systems (GIS) are mostly used to create maps for different environmental structures. Based on the same premises, one could also map a human being, from basic features to specific details, creating a Human GIS with which medical specialists could navigate with the goal of diagnostics, prognosis, or treatment. Human digitization is possible if all the information available from one individual— i.e., data from biosensors, medical imagistic, medical documents, monitoring, blood tests, social environments, and omics—can be stored and the proper information or combination of information specific to a given situation can be extracted at any given moment [22].
One of the first individuals who mapped himself using these technologies was Michael Snyder, on whom the whole genome was sequenced, with data extracted from the metabolome, proteome, certain antibodies, and biosensors. Based on these results, he was able regulate his lifestyle and manage his glucose levels [23].
2.5. “Omics” Technologies
These technologies imply a wide range of assessments of a set of molecular data. Each data category can provide a list of alterations consistent with the studied disease, which provides an insight into biological pathways and processes.
If more than one such list can be provided, every detail about a given disease can be unraveled, and proper medical conduct is a certainty. Many type of omics data currently exist, and specialists in biodata analysis are still working on methods to integrate them all.
Examples of omics data include:
Genomics considers genetic variability in terms of response to treatment and susceptibility to some illnesses [24].
Proteomics considers as its main activity, peptide content, and their interactions/modifications and proteomic analysis of cellular systems [25].
Epigenomics involves definition of genome-wide DNA-reversible modifications [26].
Transcriptomics explores RNA from both quantitative and qualitative perspectives [27].
Metabolomic analyses consider various products of body metabolism, including lipids, carbohydrates, and other byproducts of cell metabolism [28].
Microbiomics involves the study of microorganisms of a given group [29].
Physiome and exposome analyses involve collection of data from biosensors available in the environment, including data with respect to variables concerning an individual’s physiology [22] (Figure 2).
The diploid genome (diplomics) was elucidated more than decade ago due to the need for improved understanding of the complex pathways of diseases. The physiopathology of different illnesses often involves mutations, allele-specific effects, and variant combinations; therefore, the “diplomics” genomic microsequencing approach is suitable for analyzing, characterizing, and determining the appropriate conduit of a given disease [22,30].
With the advent of sequencing with a two-year timeframe, the database of rare Mendelian conditions improved from four fully characterized rare diseases in 2010 to 68 in 2012, with the number anticipated to increase to 7000 in the coming years [31].
Such methods of gathering and accurately analyzing biodata for the development of treatment or prognosis strategies constitute the core of personalized medicine, a medical practice of the future. The enormous volume of data gathered from an individual can be used to create a digitized human and, when required, a precise fragment of this human map can be studied. Specialists will happily embrace this approach and contribute to its extension.
2.6. Microfluidics
Microfluidics is a technology that involving fluids up to a femtoliter scale. This technology is incredibly useful in handling small probes with high specificity. Microfluidics function in the same way as electronics, the difference being that in fluidics, chemical mixtures or cells are moved onto a chip created using soft photolithography [32] (Figure 3).
Microfluidics technology can benefit PM by determining exact combinations of drugs using less biomaterial. Furthermore, it reduces costs by using fewer reagents, and phenotyping and biomarkers can be obtained from the same cell sample, with physiological conditions obtained with microfluidics for cell growth [33].
Organ cells can also be created using microfluidics. Such organs on a chip (OOACs) can be created for either physiologic organs or different pathologies. In this regard, different models that can replace experiments on animal models can be used for further research on personalized treatments for different pathologies [34]. To date, several OOACs have been created and used for studies, lung on a chip, liver on a chip, kidney on a chip, heart on a chip, intestine on a chip, and multi-organ on a chip [35,36,37,38,39,40].
These complex and precise technologies have a long way to go before they can be implemented in bedside clinical practice, but progress to date is promising, with good prospects for translation from in vitro to in vivo.
3. Precision Medicine in Intensive Care Units
The abovementioned mathematical models and sophisticated informatics technologies are applicable to modern medicine and the critically ill. In these patients, the data needed for processing have a continuous and intricate character due to ongoing and complex monitoring. Below, we present some specific conditions that must be met in critically ill patients.
3.1. Discriminative Models for Prediction of Perioperative and Long-Term Outcomes
- Perioperative organ dysfunction.
3.1.1. Coronary Disease
Coronary artery disease (CAD) is known to be a serious health problem worldwide. This disease is produced by a complex of factors, one of the most important of which is the hereditary factor [41].
Among these, a few mendelian contributions have been described in CAD:
- -
- Familial forms of hypercholesterolemia, are often caused by mutations in the low-density lipoprotein (LDL) receptor gene or the apolipoprotein (apo) B gene, which encodes the major protein in the LDL particle [42];
- -
- Familial hyperhomocystinuria associated with mutations in the 5,10-methylenetetrahydrofolate reductase gene [43];
- -
- Hutchinson–Gilford progeria syndrome is caused by mutations in the lamin A/C gene [44];
- -
- Tangier disease related to mutations in the ATP-binding cassette, subfamily, A.; member 1 gene (ABCA1) [45]; and
- -
- A type of coronary artery disease related to the MADS box transcription enhancer factor 2, polypeptide A gene (MEF2A), as well as some forms of inherited primary electrical diseases (“channelopathies”) caused by variants of the sodium channel, voltage-gated, type, V.; α-subunit gene (SCN5A); the potassium channel, voltage-gated, KQT-like subfamily, member 1 gene (KCNQ1); and other genes [46].
Postoperative atrial fibrillation (PAF) also presents with a multifactorial etiology. It is known to be the most encountered pathology after coronary artery bypass graft (CABG), occurring in as many as 40% of patients [47,48].
Genetic variations are thought to play a key role in PAF, and several studies have been conducted in this direction. The genes believed to be the most involved in PAF are those that modulate the heart’s electric activity (sinoatrial node, signal transmission/modulation genes). Genetic alterations of any of the involved genes can be identified by genome wide association studies (GWAS) or by single-nucleotide polymorphisms (SNP) [49].
Based on personalized approaches to biodata analysis, GWAS and SNP, researchers were able to identify an SNP in the LY96 gene and a supplementary gene–gene interaction with NFkB1, on the signaling pathway of PAF. These findings are important, as the identified genes participate in the innate immune system, and they are modified when this system is challenged. Findings such as those mentioned above prove that personalized biodata approaches provide new targets for PAF prevention [50,51].
3.1.2. Acute Kidney Injury
Another well-acknowledged hospital pathology related to cardiac surgery is acute kidney injury (AKI). This disorder is confirmed to have a strong link in terms of its appearance in patients who have undergone a coronary artery bypass graft [52]. AKI is triggered by a range of factors, i.e., age, obesity, chronic kidney disease, pre-existent heart pathologies, and systemic inflammation; however, genetic predisposition and familial inheritance play an important but understudied role [53].
AKI constitutes a perfect candidate for PM due to its vast heterogeneity and the multiple potential causes that may lead to this disorder, which increases the number of possible connections made among biodata points. A GWAS analysis performed on AKI found identified new loci associated with post CABG-AKI; hence, a new approach to AKI pathophysiology was described [54].
3.1.3. Sepsis
Sepsis is one of the most complex pathologies, in addition to being the most expensive pathology to treat, with estimated costs in the US totaling approximately USD 20 billion per year [55]. The physiopathology of sepsis can be understood as a complex maze, with multiple pathways indicated, including inflammatory and anti-inflammatory pathways, coagulopathies, the systemic action of microorganisms, and multiple organ failure. Since its first mention and definition as a life-threatening condition caused by an abnormal response of a host to infection, sepsis has been studied continuously; however, the literature does not offer a clear plan for management or diagnosis [56]. Although extensive research has been conducted on sepsis, results are limited with respect to the prevention and management of this syndrome [57,58].
The extreme complexity and discrepancy presented by this pathology makes it a perfect candidate for the implementation of personalized medicine with the hope of finding proper treatments or prognostic means. Metabolomic and proteomic studies of severely septic patients and septic shock patients revealed the possibility of personalizing a set of biomarkers to be used to determine the mortality prognosis of such critically ill patients and to improve survival [59].
A personalized medicine approach that could be applied in sepsis is the enrichment approach. This concept is divided into two categories: prognostic and predictive enrichment [60]. Both categories are required for the application of personalized medicine in septic patients in intensive care. With the help of this approach, septic patients were clustered based on the probability of experiencing a given sepsis-related outcome, such as multiple organ failure or mortality rate [61]. Prognostic enrichment strategies allow researchers to conclude their studies by enrolling a smaller number of individuals, as in the CONSENSUS trial, which required hundreds of patients to prove that the studied treatment significantly reduced mortality among critically ill patients. The study would have required thousands of patients to prove its point with classic approaches and simple statistics [62]. The predictive component of the enrichment approach aids in selecting patients with a higher probability of response to given therapeutic conduct, with biological mechanisms as the foundation (Figure 4) [63].
Extensive research has been conducted in the field of sepsis and its genetic pathways, and a tremendous amount of biodata has been gathered and deposited in specific databases, such as the National Institutes of Health Gene Expression Omnibus (GEO), Array Express, and the Host Response to Injury Program (Glue Grant) [64,65,66]. The Glue Grant program is of particular interest with respect to personalized approaches to sepsis due to some notable findings. The program showed that a real genetic storm happens in sepsis, that more than 80% of the expressed genes present with differential expression, and that different groups of genes recover at significantly different rates in the context of sepsis [64,65].
3.1.4. Pain
Critically ill patients, like any other patient, suffer from chronic or acute pain. The difference between most ICU patients and other patients consists of the impossibility of verbalizing pain. Nonetheless, the need to identify appropriate pain-management strategies is equally necessary for any patient.
Genome-wide association studies (GWAS) on pain-specific mechanisms and approaches revealed that a three-SNP haplotype of catecholamine O-methyltransferase (COMT) is correlated with a 30-fold difference in enzymatic activity and important modifications in sensitivity to pain in humans. However, it is not yet known the exact mechanism by which this enzyme modulates pain [67]. The GWAS approach is not the ideal system for genetic pain decryption due to challenges including the impossibility of differentiating between different ethnicities and the need to include many subjects in studies [68].
Another method that can be applied with the aim of decoding the underlying mechanisms of pain is constituted of whole genome sequencing. With this approach, rare gene variants were identified in the angiotensin pathway alone, an enzyme linked with pain in animal models [69].
The targeted gene approach proved a strong link between the voltage-gated sodium channels Nav1.7 and human pain. The targeted gene approach was used to identify the genomic variants of Nav1.7 that have a connection to four pain syndromes, and the Nav 1.7 polymorphism was found to be related to pain perception. The Nav 1.7 sodium channel constitutes a target for both inherited and non-inherited pain management [70]. The trajectory from the targeted gene to the treatment of pain is paved by some small molecules targeted specifically toward the variants of sodium channel voltage-gated Nav 1.7 [71].
Although these small molecules are not yet widely used in clinical practice, the premises for this targeted pain therapy by a genetic approach have been proposed, and pain management practice will likely benefit from these discoveries.
3.1.5. Blood Loss
Perhaps one of the best examples of demand for personalized medicine is a study on the effectiveness of the use of drotrecogin alfa (recombinant human activated protein C) in severely septic patients. This drug was introduced in 2011 for the treatment of sepsis and a renowned trial, Recombinant Human Activated Protein C Worldwide Evaluation in Severe Sepsis (PROWESS), concluded that in addition to reducing mortality amongst critically ill septic patients, it also had a very low rate of side effects, namely bleeding [72]. A meta-analysis published a few years after the release of the PROWESS study results proved that side effects such as bleeding are significantly more likely to appear than initially reported. After the publication of the meta-analysis results, the drug was withdrawn from clinical use [73].
3.2. Selection/Stratification for Perioperative Interventions
3.2.1. Prevention of Organ Failure
Critically ill patients are defined as patients with complex intricated pathologies; multiple organ failure is often encountered in this subset of patients. Tailoring a specific personalized treatment for such patients represents a considerable challenge. A combined approach involving prediction, prevention, and personalized medicine should be considered. To reach the point where the appropriate drug is administered in a precise therapeutic window to the patient who will benefit the most from it, a strong link needs to be created between research results and bedside application. Translational medicine is defined the branch of medicine that can construct such a link between research and bedside practice [74].
With the main objective of taking advantage of the therapeutic window and preventing reaching the organ failure stage, numerous animal experimental studies have been conducted on different treatment means, diagnoses, and preventive measures. Animal studies now constitute the primary method for development of new therapies [75].
The main downside of animal studies is that no animal model can recreate the complexity of a human patient, let alone an ICU patient. Hence, the applicability of their results to humans often fails due to the toxicity of severe side effects that did not appear in animal experiments [76,77,78]. Animal models are mainly focused and mimic the researched pathology without considering many other factors that could interfere with the disease in humans. Among the factors ignored in animal studies are environmental factors, sex, age, emotional factors, interactions with other drugs, and social behaviors [70,71,72,73,74,75,76,77,78,79,80,81,82].
The medicine of the future should prioritize the individual over the disease, and the way to succeed in this quest is by using predictive, preventive, and personalized medicine (PPPM). The PPPM approach aims to develop appropriate knowledge and technological skills to promote affordable strategies in the emerging fields of environmental risk factors, epidemiology, healthy lifestyle, individualized nutrition, food technology, and culture within a framework of cost-effective healthcare [83].
3.2.2. Hemodynamic Optimization
The homeostasis of ICU patients is a considerable risk, and shock states are often observed in critically ill patients. Optimization of hemodynamics in this category of patients is an outcome that has been sought for a long time but has not yet been achieved due to the massive heterogeneity of ICU patients. Currently, the success of goal-directed therapy, in terms of hemodynamics, is defined as a mean arterial pressure of at least 65 mmHg [84]. However, this “one size doesn’t fit all” hemodynamically unstable ICU patients.
A possible solution to this problem is cardiac modeling based on a set of mathematical relations, with the goal of creating a myocardium with the same characteristics as those presented by the patient. This model includes and processes anthropometric data, data regarding the disease/diseases the patient may have, and the results from different imagistic other tests. The result incorporates all this specific data on the studied individual, resulting in a heart model that matches their unique patient features [85]. Such models acquired were validated to an extent by comparison with experimental studies and imaging results [86].
Limitations of cardiac modeling are associated with the immense volume and complexity of data that need to be processed; the lack of a standard for data acquisition, such as standard imaging results; material laws; and multidomain physics that need to be applied [87,88]. Additional research is needed to facilitate the development and clinical implementation of such cardiac modeling in terms of minimum data requirements, the ideal timeframe to acquire images of the heart, and the type of statistics that should be used according to the patient [89].
Even with these uncertainties in mind, this approach to achieving personalized hemodynamic stability is a promising means by which intensivists can better understand and help hemodynamically unstable patients.
3.2.3. Fluid Resuscitation
Fluid resuscitation constitutes one of the most used treatments in ICUs. Many large studies have proposed different strategies for fluid administration in critically ill patients, from a more liberal to restrictive fluid therapy and from balanced solutions to crystalloids alone; furthermore, some studies have suggested alternative routes of administration, such as bolus or continuous infusion [90,91,92,93,94]. Special adaptive platforms have been created to help intensivists administer personalized fluid therapy, whereby patient data can be introduced; then, using complex mathematical and statistical methods, the results can be tailored to the individual instead of being protocolized for a given disease presented in the patient [95].
Critical illness is vastly different from the areas in which precision medicine has made a substantial impact, particularly oncology. Intensive care, as a medical specialty, is newer than the other medical specialties, such as surgery or internal medicine. However, intensive care has found itself on an ascending slope in recent decades due to improved understanding of disease pathways and the development of novel technologies with the aim of sustaining and monitoring patients’ vitals. An improved understanding of physiopathology has allowed intensivists to characterize and more clearly comprehend the complex pathologies encountered in ICUs. Examples in this respect include the ongoing development sepsis definitions and treatment or those for acute respiratory distress syndrome. Although advances in intensive care are in progress, treatment and prognosis of critically ill patients have not yet reached a satisfactory level. This may be attributed to the burden of properly grouping critically ill patients into homogenous groups for development of improved treatment protocols and prognostics. Intergroup variability among ICU patients is greater than in other specialties, and the severity of the pathologies of critically ill patients is high [96,97]. When critically ill patients were grouped based on their diagnosis, the results were mostly negative; however, scientists observed that in some individuals, the proposed interventions were successful. Biomarkers were subsequently identified based on these subgroups, and a more precise diagnosis/treatment was drafted for critically ill patients [98].
Such discoveries were achieved by changing the lens through which critically ill patients are viewed, from a conglomerate of diagnostics and diseases to individuals with specific diagnostic and disease characteristics. Using this personalized perspective and the multiple technological possibilities—sophisticated mathematical and statistical methods, as well as exploration of proteomics, metabolomics, and genomics—the treatment and diagnosis of ICU patients can be tailored accordingly, with the focus shifted from treating a pathology to treating the individual.
One of the most difficult obstacles when it comes to the critically ill is that such patients have more complex, heterogeneous diseases with multiple comorbidities and conditions that can impact outcomes and response to treatment, making it difficult to identify a single target. In this respect, panels of biomarkers have been proposed for ICU patients to diagnose, treat, or prognosticate the course of their pathologies [99,100].
4. Approval of the FDA
All these new targeted therapies and technological methods of determining exact doses or biomarkers need to be approved by quality control structures.
Because most newer PM therapies involve pharmacogenomics (PGx), the Food and Drug Administration (FDA) built drug labeling databases. The first label of this kind was approved by the FDA 20 years ago: Herceptin, a genetically targeted therapy [101].
The FDA endorses PGx drug labeling, since the first labeled drug was approved, additional public databases have been created in this direction, such as the Pharmacologic Knowledgebase (PharmGKB), and the Clinical Pharmacogenetics Implementation Consortium (CPIC) database. In addition to drug labeling information, these databases include information related to clinical observation, specific scientific literature, disease pathways, dosing, specific warnings, and administration guidelines based on genotype [102,103]. The existing PGx public table, FDALabel, contains 75 biomarkers that can be used for research on different processes and treatment conduct. Basic training in drug labeling is required to correctly extract data from these databases [104]. Results of PGx labeling have already been reported in oncologic patients treated based on the genetic population to which they belong [105].
Once the information from these specific databases is made accessible and basic principles of their utilization are understood, specialists can facilitate personalized treatments for any type of patient based on the patient’s genetics, with the aim of treating the individual rather than the pathologies presented by the individual. Personalized medicine deals with a multitude of complex concepts, from “omics” and genetic characterization of the individual to high-end equipment and advanced mathematical and statistical models for data processing. A multidisciplinary approach is required to achieve the desired results.
When it comes to critically ill patients, the situation is complicated because such patients have multiple comorbidities that require the supervision of specialists representing different branches of the medical field, in addition to technicians, statisticians, geneticists, and access to proper equipment to sustain the patient’s vitals and to store, extract, and process biodata. Collaboration among researchers and industry aims to ensure standardization of measurements and reporting. Studies have been conducted to determine the best ways to create multidisciplinary teams that can work together and achieve the expected results [106]. Tigers BB et al., after a comprehensive review of studies on research team collaboration and formation, formulated recommendations for best practices, which included the development of psychometric testing of measures of research collaboration quality that can be applied by each researcher and validated by other participants, such as stakeholders, researchers, academics, and government officials. Both quality and quantity should be considered to achieve the highest standards [107].
5. Ethics of Personalized Medicine
Personalized medicine raises some ethical issues that need to be addressed. According to PM desire to “treat the individual and not the disease” in some cases, different patients might receive a different course of treatment for the same disease on the basis of the patient’s genetic characteristics. Even for the same phenotype, medical conduct might differ due to the integration of all available biodata pertaining to an individual, exposome, metabolome, proteome, microbiome, etc. In this context, a patient might not benefit from a certain treatment because in his exposome or other factors that interfere with the desired results.
Personalized medicine shifts the balance of responsibility from the doctor to the patient by implementing proactive as opposed to medicine, as is currently the standard. In this initiative-taking approach to medicine, the patient has the responsibility of having “good genetic references” to benefit from personalized treatment [108].
Another ethical problem specific to PM is the genetic material donated and stored in biobanks issues related to donor consent when it comes to the use of stored biodata. At the time of donation, it is impossible to know exactly to what extent genetic material can be analyzed and exactly how much information can be extracted from the material. Some solutions have been identified, and distinct types of consent are available, such as the “broad consent” or multilayered or “tiered” consent, which allow donors to choose whether their genetic material can be used for one or multiple research projects [109,110].
6. Economic Challenge
Personalized medicine has the capacity to improve the quality and longevity of human lives and reduce costs by administering “the right treatment to the right patient at the right time”. However, PM involves costs associated with data acquisition, storage, and processing, as well as education of medical personnel and out-of-hospital personnel who deal with biodata.
In a review of studies on the cost-effectiveness of drug pharmacogenetics wherein FDA databases were searched, of 137 studies on pharmacokinetically engineered drugs, only 44 complete economic studies were found on 9 PGx drugs [111] Table 1.
The economic aspect of PM constitutes one of the perspectives through which the International Consortium for Personalized Medicine advocates for a balance between investment, profit, benefit, telemedicine, mobile resources, and creation new jobs in the healthcare system [112].
7. Concluding Notes
Future medicine relies on personalized treatments, as well as personalized diagnosis and prognosis. Technological advancements allow researchers and medical specialists to offer medical care based on individualism. Clinical trials should be developed in such a manner that patients are grouped according to genotypes and clustered based on their genetic characteristics. “Omics” technologies make a more precise differentiation when it comes to prognostication and assigning individuals a certain group or treatment.
Newer data processing technologies and methods allow for improved prognostication in both acute and chronic phases of pathologies.
Critically ill patients, although complex due to their severe and combined pathologies, can benefit from personalized treatments in spite of difficulties in implementation. These patients should be treated as individuals because even if they may have the same diagnosis, their responses to treatments can be different. Treatment personalization could be the key to successfully managing critically ill patients, as well as a response to the inconclusive results obtained in studies performed of the critically ill.
The multitude of identified biomarkers can help in candidate selection for different therapeutic methods and offer the possibility of therapeutic efficacy tracking.
The advanced technology involved in precision medicine can be used to create predictive models to enhance discrimination of recovery probabilities in patients.
We have a long road ahead before personalized medicine can be applied daily in intensive care, although the steps that have been taken to date are significant and promising.
Author Contributions
A.E.L., manuscript writing—original draft, data acquisition, writing—review and editing; L.A., conceptualization, methodology, writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- National Research Council (US) Committee on A Framework for Developing a New Taxonomy of Disease. Toward Precision Medicine: Building A Knowledge Network for Biomedical Research and A New Taxonomy of Disease; National Academies Press (US): Washington, DC, USA, 2011.
- The Precision Medicine Initiative. Available online: https://obamawhitehouse.archives.gov/precision-medicine (accessed on 30 January 2015).
- Collins, F.S.; Varmus, H. A new initiative on precision medicine. N. Engl. J. Med. 2015, 372, 793–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holst, L. The Precision Medicine Initiative: Data-Driven Treatments as Unique as Your Own Body; The White House: Washington, DC, USA, 2015.
- Johnson, J.A. Pharmacogenetics: Potential for individualized drug therapy through genetics. Trends Genet. 2003, 19, 660–666. [Google Scholar] [CrossRef] [PubMed]
- Goldman, N.; Bertone, P.; Chen, S.; Dessimoz, C.; LeProust, E.M.; Sipos, B.; Birney, E. Towards practical, high-capacity, low-maintenance information storage in synthesized DNA. Nature 2013, 494, 77–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Issacson Simon, W.; Steve Jobs, S. New York; Simon & Schuster: New York, NY, USA, 2011. [Google Scholar]
- L’Heureux, A.; Grolinger, K.; Elyamany, H.F.; Capretz, M.A. Machine Learning With Big Data: Challenges and Approaches. IEEE Access 2017, 5, 7776–7797. [Google Scholar] [CrossRef]
- Mirza, B.; Wang, W.; Wang, J.; Choi, H.; Chung, N.C.; Ping, P. Machine Learning and Integrative Analysis of Biomedical Big Data. Genes 2019, 10, 87. [Google Scholar] [CrossRef] [Green Version]
- Matejka, J.; Fitzmaurice, G. Same Stats, Different Graphs: Generating Datasets with Varied Appearance and Identical Statistics through Simulated Annealing. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems, Denver, CO, USA, 6–11 May 2017; pp. 1290–1294. [Google Scholar]
- Skaf, Y.; Laubenbacher, R. Topological data analysis in biomedicine: A review. J. Biomed. Inform. 2022, 130, 104082. [Google Scholar] [CrossRef]
- Adams, H.; Moy, M. Topology Applied to Machine Learning: From Global to Local. Front. Artif. Intell. 2021, 4, 668302. [Google Scholar] [CrossRef]
- Chazal, F.; Michel, B. An Introduction to Topological Data Analysis: Fundamental and Practical Aspects for Data Scientists. Front. Artif. Intell. 2021, 4, 667963. [Google Scholar] [CrossRef]
- Giannini, H.M.; Chivers, C.; Draugelis, M. Development and implementation of a machine-learning algorithm for early identification of sepsis in a multi-hospital academic healthcare system. Am. J. Respir. Crit. Care Med. 2017, 195, A7015. [Google Scholar]
- Chung, Y.M.; Hu, C.S.; Lo, Y.L.; Wu, H.T. A Persistent Homology Approach to Heart Rate Variability Analysis With an Application to Sleep-Wake Classification. Front. Physiol. 2021, 12, 637684. [Google Scholar] [CrossRef]
- Huysmans, J.; Dejaeger, K.; Mues, C.; Vanthienen, J.; Baesens, B. An empirical evaluation of the comprehensibility of decision table, tree and rule based predictive models. Decis. Support Syst. 2011, 51, 141–154. [Google Scholar] [CrossRef]
- Rudin, C. Stop explaining black box machine learning models for high stakes decisions and use interpretable models instead. Nat. Mach. Intell. 2019, 1, 206–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, P.H. Signal processing and machine learning for biomedical big data. IEEE Pulse 2019, 10, 34–35. [Google Scholar] [CrossRef]
- Chicco, D. Ten quick tips for machine learning in computational biology. BioData Min. 2017, 10, 35. [Google Scholar] [CrossRef] [PubMed]
- Moraleda, R.R.; Xiong, W.; Valous, N.A.; Halama, N. Segmentation of biomedical images based on a computational topology framework. Semin. Immunol. 2020, 48, 101432. [Google Scholar] [CrossRef]
- Kamel Boulos, M.N.; Zhang, P. Digital Twins: From Personalised Medicine to Precision Public Health. J. Pers. Med. 2021, 11, 745. [Google Scholar] [CrossRef]
- Topol, E.J. Individualized medicine from prewomb to tomb. Cell 2014, 157, 241–253. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.; Mias, G.I.; Li-Pook-Than, J.; Jiang, L.; Lam, H.Y.; Chen, R.; Miriami, E.; Karczewski, K.J.; Hariharan, M.; Dewey, F.; et al. Personal omics profiling reveals dynamic molecular and medical phenotypes. Cell 2012, 148, 1293–1307. [Google Scholar] [CrossRef] [Green Version]
- Voight, B.F.; Kang, H.M.; Ding, J.; Palmer, C.D.; Sidore, C.; Chines, P.S.; Burtt, N.P.; Fuchsberger, C.; Li, Y.; Erdmann, J.; et al. The metabochip, a custom genotyping array for genetic studies of metabolic, cardiovascular, and anthropometric traits. PLoS Genet. 2013, 9, e1002793. [Google Scholar] [CrossRef]
- Hein, M.Y.; Sharma, K.; Cox, J.; Mann, M. Proteomic Analysis of Cellular Systems. In Handbook of Systems Biology: Concepts and Insights; Walhout, M., Vidal, M., Dekker, J., Eds.; Academic Press: New York, NY, USA, 2013; pp. 3–25. [Google Scholar]
- Piunti, A.; Shilatifard, A. Epigenetic balance of gene expression by Polycomb and, C.O.MPASS families. Science 2016, 352, aad9780. [Google Scholar] [CrossRef] [Green Version]
- ENCODE Project Consortium. An integrated encyclopedia of DNA elements in the human genome. Nature 2012, 489, 57–74. [Google Scholar] [CrossRef] [PubMed]
- Kettunen, J.; Tukiainen, T.; Sarin, A.P.; Ortega-Alonso, A.; Tikkanen, E.; Lyytikäinen, L.P.; Kangas, A.J.; Soininen, P.; Würtz, P.; Silander, K.; et al. Genome-wide association study identifies multiple loci influencing human serum metabolite levels. Nat. Genet. 2012, 44, 269–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Org, E.; Parks, B.W.; Joo, J.W.; Emert, B.; Schwartzman, W.; Kang, E.Y.; Mehrabian, M.; Pan, C.; Knight, R.; Gunsalus, R.; et al. Genetic and environmental control of host-gut microbiota interactions. Genome Res. 2015, 25, 1558–1569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tewhey, R.; Bansal, V.; Torkamani, A.; Topol, E.J.; Schork, N.J. The importance of phase information for human genomics. Nat. Rev. Genet. 2011, 12, 215–223. [Google Scholar] [CrossRef] [Green Version]
- Boycott, K.M.; Vanstone, M.R.; Bulman, D.E.; MacKenzie, A.E. Rare-disease genetics in the era of next-generation sequencing: Discovery to translation. Nat. Rev. Genet. 2013, 14, 681–691. [Google Scholar] [CrossRef]
- Shembekar, N.; Chaipan, C.; Utharala, R.; Merten, C.A. Droplet-based microfluidics in drug discovery, transcriptomics and high-throughput molecular genetics. Lab Chip. 2016, 16, 1314–1331. [Google Scholar] [CrossRef] [Green Version]
- Mathur, L.; Ballinger, M.; Utharala, R.; Merten, C.A. Microfluidics as an Enabling Technology for Personalized Cancer Therapy. Small 2020, 16, e1904321. [Google Scholar] [CrossRef]
- Wu, Q.; Liu, J.; Wang, X.; Feng, L.; Wu, J.; Zhu, X.; Wen, W.; Gong, X. Organ-on-a-chip: Recent breakthroughs and future prospects. Biomed. Eng. Online 2020, 19, 9. [Google Scholar] [CrossRef] [Green Version]
- Ma, L.D.; Wang, Y.T.; Wang, J.R.; Wu, J.L.; Meng, X.S.; Hu, P.; Mu, X.; Liang, Q.L.; Luo, G.A. Design and fabrication of a liver-on-a-chip platform for convenient, highly efficient, and safe in situ perfusion culture of 3D hepatic spheroids. Lab Chip. 2018, 18, 2547–2562. [Google Scholar] [CrossRef]
- Humayun, M.; Chow, C.-W.; Young, E.W.K. Microfluidic lung airway-on-a-chip with arrayable suspended gels for studying epithelial and smooth muscle cell interactions. Lab Chip. 2018, 18, 1298–1309. [Google Scholar] [CrossRef]
- Schutgens, F.; Rookmaaker, M.B.; Margaritis, T.; Rios, A.; Ammerlaan, C.; Jansen, J.; Gijzen, L.; Vormann, M.; Vonk, A.; Viveen, M.; et al. Tubuloids derived from human adult kidney and urine for personalized disease modeling. Nat. Biotechnol. 2019, 37, 303–313. [Google Scholar] [CrossRef] [PubMed]
- Schneider, O.; Zeifang, L.; Fuchs, S.; Sailer, C.; Loskill, P. User-friendly and parallelized generation of human induced pluripotent stem cell-derived microtissues in a centrifugal heart-on-a-chip. Tissue Eng. Part A 2019, 25, 786–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasendra, M.; Tovaglieri, A.; Sontheimer-Phelps, A.; Jalili-Firoozinezhad, S.; Bein, A.; Chalkiadaki, A.; Scholl, W.; Zhang, C.; Rickner, H.; Richmond, C.A.; et al. Development of a primary human small intestine-on-a-chip using biopsy-derived organoids. Sci. Rep. 2018, 8, 2871. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Kankala, R.K.; Wang, S.-B.; Chen, A.-Z. Multi-organs-on-chips: Towards long-term biomedical investigations. Molecules 2019, 24, 675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thom, T.; Haase, N.; Rosamond, W.; Howard, V.J.; Rumsfeld, J.; Manolio, T.; Zheng, Z.J.; Flegal, K.; O’Donnell, C.; Kittner, S.; et al. Heart disease and stroke statistics—2006 update: A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2006, 113, e85–e151. [Google Scholar]
- Brown, M.S.; Goldstein, J.L. A receptor-mediated pathway for cholesterol homeostasis. Science 1986, 232, 34–47. [Google Scholar] [CrossRef] [Green Version]
- Cho, S.E.; Sook Hong, K.; Shin, G.J.; Chung, W.S. The methylenetetrahydrofolate reductase C677T gene mutation is associated with hyperhomocysteinemia, cardiovascular disease, and plasma B-type natriuretic peptide levels in Korea. Clin. Chem. Lab. Med. 2006, 44, 1070–1075. [Google Scholar] [CrossRef]
- DeBusk, F.L. The Hutchinson-Gilford progeria syndrome: Report of 4 cases and review of the literature. J. Pediatr. 1972, 80, 697–724. [Google Scholar] [CrossRef]
- Brooks-Wilson, A.; Marcil, M.; Clee, S.M.; Zhang, L.H.; Roomp, K.; van Dam, M.; Yu, L.; Brewer, C.; Collins, J.A.; Molhuizen, H.O.; et al. Mutations in ABC1 in Tangier disease and familial high-density lipoprotein deficiency. Nat. Genet. 1999, 22, 336–345. [Google Scholar] [CrossRef]
- Wang, L.; Fan, C.; Topol, S.E.; Topol, E.J.; Wang, Q. Mutation of, M.E.F2A in an inherited disorder with features of coronary artery disease. Science 2003, 302, 1578–1581. [Google Scholar] [CrossRef] [Green Version]
- Mathew, J.P.; Fontes, M.L.; Tudor, I.C.; Ramsay, J.; Duke, P.; Mazer, C.D.; Barash, P.G.; Hsu, P.H.; Mangano, D.T. A multicenter risk index for atrial fibrillation after cardiac surgery. JAMA 2004, 291, 1720–1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waldron, N.H.; Cooter, M.; Piccini, J.P.; Anstrom, K.J.; Klinger, R.Y.; Kertai, M.D.; Podgoreanu, M.V.; Stafford-Smith, M.; Newman, M.F.; Mathew, J.P. Predictive ability of perioperative atrial fibrillation risk indices in cardiac surgery patients: A retrospective cohort study. Capacité de prédiction des indices de risque de fibrillation auriculaire périopératoire chez les patients de chirurgie cardiaque: Une étude de cohorte rétrospective. Can. J. Anaesth. 2018, 65, 786–796. [Google Scholar] [PubMed] [Green Version]
- Ellinor, P.T.; Lunetta, K.L.; Albert, C.M.; Glazer, N.L.; Ritchie, M.D.; Smith, A.V.; Arking, D.E.; Müller-Nurasyid, M.; Krijthe, B.P.; Lubitz, S.A.; et al. Meta-analysis identifies six new susceptibility loci for atrial fibrillation. Nat. Genet. 2012, 44, 670–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darbar, D.; Roden, D.M. Genetic mechanisms of atrial fibrillation: Impact on response to treatment. Nat. Rev. Cardiol. 2013, 10, 317–329. [Google Scholar] [CrossRef] [Green Version]
- Kertai, M.D.; Li, Y.J.; Ji, Y.; Qi, W.; Lombard, F.W.; Shah, S.H.; Kraus, W.E.; Stafford-Smith, M.; Newman, M.F.; Milano, C.A.; et al. Genome-wide association study of new-onset atrial fibrillation after coronary artery bypass grafting surgery. Am. Heart J. 2015, 170, 580–590.e28. [Google Scholar] [CrossRef] [Green Version]
- Swaminathan, M.; Hudson, C.C.; Phillips-Bute, B.G.; Patel, U.D.; Mathew, J.P.; Newman, M.F.; Milano, C.A.; Shaw, A.D.; Stafford-Smith, M. Impact of early renal recovery on survival after cardiac surgery-associated acute kidney injury. Ann. Thorac. Surg. 2010, 89, 1098–1104. [Google Scholar] [CrossRef]
- Lu, J.C.; Coca, S.G.; Patel, U.D.; Cantley, L.; Parikh, C.R. Translational Research Investigating Biomarkers and Endpoints for Acute Kidney Injury (TRIBE-AKI) Consortium.. Searching for genes that matter in acute kidney injury: A systematic review. Clin. J. Am. Soc. Nephrol. 2009, 4, 1020–1031. [Google Scholar] [CrossRef] [Green Version]
- Stafford-Smith, M.; Li, Y.J.; Mathew, J.P.; Li, Y.W.; Ji, Y.; Phillips-Bute, B.G.; Milano, C.A.; Newman, M.F.; Kraus, W.E.; Kertai, M.D.; et al. Genome-wide association study of acute kidney injury after coronary bypass graft surgery identifies susceptibility loci. Kidney Int. 2015, 88, 823–832. [Google Scholar] [CrossRef] [Green Version]
- Torio, C.M.; Andrews, R.M. National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2011. Healthcare Cost and Utilization Project Statistical Brief #160. Rockville; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2013. Available online: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb160.pdf (accessed on 17 June 2015).
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Marshall, J.C. Why have clinical trials in sepsis failed? Trends Mol. Med. 2014, 20, 195–203. [Google Scholar] [CrossRef]
- Lazăr, A.; Georgescu, A.; Vitin, A.; Azamfirei, L. Precision Medicine and its Role in the Treatment of Sepsis: A Personalised View. J. Crit. Care Med. 2019, 5, 90–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalil, A.C.; LaRosa, S.P. Effectiveness and safety of drotrecogin alfa (activated) for severe sepsis: A meta-analysis and meta regression. Lancet Infect. Dis. 2012, 12, 678–686. [Google Scholar] [CrossRef]
- Wong, H.R. Intensive care medicine in 2050, precision medicine. Intensive Care Med. 2017, 43, 1507–1509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prescott, H.C.; Calfee, C.S.; Thompson, B.T.; Angus, D.C.; Liu, V.X. Toward smarter lumping and smarter splitting: Rethinking strategies for sepsis and acute respiratory distress syndrome clinical trial design. Am. J. Respir. Crit. Care Med. 2016, 194, 147–155. [Google Scholar] [CrossRef] [Green Version]
- Swedberg, K.; Kjekshus, J.; CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. results of the cooperative north Scandinavian enalapril survival study (CONSENSUS). N. Engl. J. Med. 1987, 316, 1429–1435. [Google Scholar] [CrossRef]
- Center for Drug Evaluation and Research. Enrichment Strategies for Clinical Trials to Support Approval of Human Drugs and Biological Products FDA 2019. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/enrichment-strategies-clinical-trials-support-approval-human-drugs-and-biological-products (accessed on 11 March 2019).
- Xiao, W.; Mindrinos, M.N.; Seok, J.; Cuschieri, J.; Cuenca, A.G.; Gao, H.; Hayden, D.L.; Hennessy, L.; Moore, E.E.; Minei, J.P.; et al. Response to Injury Large-Scale Collaborative Research Program, A genomic storm in critically injured humans. J. Exp. Med. 2011, 208, 2581–2590. [Google Scholar] [CrossRef]
- Seok, J.; Warren, H.S.; Cuenca, A.G.; Mindrinos, M.N.; Baker, H.V.; Xu, W.; Richards, D.R.; McDonald-Smith, G.P.; Gao, H.; Hennessy, L.; et al. Genomic responses in mouse models poorly mimic human inflammatory diseases. Proc. Natl. Acad. Sci. USA 2013, 110, 3507–3512. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, T.E.; Shidham, A.; Wong, H.R.; Khatri, P. A comprehensive time-course-based multicohort analysis of sepsis and sterile inflammation reveals a robust diagnostic gene set. Sci. Transl. Med. 2015, 7, 287ra71. [Google Scholar] [CrossRef] [Green Version]
- Young, E.E.; Lariviere, W.R.; Belfer, I. Genetic basis of pain variability: Recent advances. J. Med. Genet. 2012, 49, 1–9. [Google Scholar] [CrossRef]
- Dib-Hajj, S.D.; Waxman, S.G. Translational pain research: Lessons from genetics and genomics. Sci. Transl. Med. 2014, 6, 249sr4. [Google Scholar] [CrossRef]
- Anand, U.; Facer, P.; Yiangou, Y.; Sinisi, M.; Fox, M.; McCarthy, T.; Bountra, C.; Korchev, Y.E.; Anand, P. Angiotensin II type 2 receptor (AT2 R) localization and antagonist-mediated inhibition of capsaicin responses and neurite outgrowth in human and rat sensory neurons. Eur. J. Pain. 2013, 17, 1012–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dib-Hajj, S.D.; Yang, Y.; Black, J.A.; Waxman, S.G. The Na(V)1.7 sodium channel: From molecule to man. Nat. Rev. Neurosci. 2013, 14, 49–62. [Google Scholar] [CrossRef] [PubMed]
- Bregman, H.; Berry, L.; Buchanan, J.L.; Chen, A.; Du, B.; Feric, E.; Hierl, M.; Huang, L.; Immke, D.; Janosky, B.; et al. Identification of a potent, state-dependent inhibitor of Nav1.7 with oral efficacy in the formalin model of persistent pain. J. Med. Chem. 2011, 54, 4427–4445. [Google Scholar] [CrossRef] [PubMed]
- Ely, E.W.; Laterre, P.F.; Angus, D.C.; Ely, E.W.; Laterre, P.F.; Angus, D.C.; Helterbrand, J.D.; Levy, H.; Dhainaut, J.F.; Vincent, J.L.; et al. Drotrecogin alfa (activated) administration across clinically important subgroups of patients with severe sepsis. Crit. Care Med. 2003, 31, 12–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angus, D.C. Drotrecogin alfa (activated)...a sad final fizzle to a roller-coaster party. Crit Care 2012, 16, 107. [Google Scholar] [CrossRef] [Green Version]
- Seifirad, S.; Haghpanah, V. Inappropriate modeling of chronic and complex disorders: How to reconsider the approach in the context of predictive, preventive and personalized medicine, and translational medicine. EPMA J. 2019, 10, 195–209. [Google Scholar] [CrossRef] [Green Version]
- Seifirad, S. An emerging need for developing new models for myocardial infarction as a chronic complex disease: Lessons learnt from animal vs. human studies on cardioprotective effects of Erythropoietin in reperfused myocardium. Front. Physiol. 2014, 5, 44. [Google Scholar] [CrossRef] [Green Version]
- Greek, J.; Shanks, N. Thoughts on animal models for human disease and treatment. J. Am. Vet. Med. Assoc. 2009, 235, 363–364. [Google Scholar]
- Hackam, D.G. Translating animal research into clinical benefit. BMJ 2007, 334, 163–164. [Google Scholar] [CrossRef] [Green Version]
- Mak, I.W.; Evaniew, N.; Ghert, M. Lost in translation: Animal models and clinical trials in cancer treatment. Am. J. Transl. Res. 2014, 6, 114–118. [Google Scholar]
- McGonigle, P.; Ruggeri, B. Animal models of human disease: Challenges in enabling translation. Biochem. Pharmacol. 2014, 87, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Bruno, R.; Vivier, N.; Montay, G.; Liboux, A.É.; Powe, L.K.; Delumeau, J.C.; Rhodes, G.R. Population pharmacokinetics of riluzole in patients with amyotrophic lateral sclerosis. Clin. Pharmacol. Ther. 1997, 62, 518–526. [Google Scholar] [CrossRef]
- Lidegaard, O. Smoking and use of oral contraceptives: Impact on thrombotic diseases. Am. J. Obstet. Gynecol. 1999, 180, S357–S363. [Google Scholar] [CrossRef]
- Jerie, P. New catastrophe in pharmacological treatment—The crisis of clinical studies? Acute organ failure after administration of TGN1412. Cas. Lek. Ceskych 2006, 145, 426. [Google Scholar]
- Golubnitschaja, O.; Baban, B.; Boniolo, G.; Wang, W.; Bubnov, R.; Kapalla, M.; Krapfenbauer, K.; Mozaffari, M.S.; Costigliola, V. Medicine in the early twenty-first century: Paradigm and anticipation—EPMA position paper 2016. EPMA J. 2016, 7, 23. [Google Scholar] [CrossRef] [Green Version]
- Beloncle, F.; Radermacher, P.; Guerin, C.; Asfar, P. Mean arterial pressure target in patients with septic shock. Minerva Anestesiol. 2016, 82, 777–784. [Google Scholar]
- Holzapfel, G.A. Nonlinear Solid Mechanics: A Continuum Approach for Engineering; John Wiley & Sons: Hoboken, NJ, USA, 2001; pp. 388–390. [Google Scholar]
- Zhu, Y.; Hardy, C.J.; Sodickson, D.K.; Giaquinto, R.O.; Dumoulin, C.L.; Kenwood, G.; Niendorf, T.; Lejay, H.; McKenzie, C.A.; Ohliger, M.A.; et al. Highly parallel volumetric imaging with a 32-element RF coil array. Magn. Reson. Med. 2004, 52, 869–877. [Google Scholar] [CrossRef] [Green Version]
- Pathmanathan, P.; Shotwell, M.S.; Gavaghan, D.J.; Cordeiro, J.M.; Gray, R.A. Uncertainty quantification of fast sodium current steady-state inactivation for multi-scale models of cardiac electrophysiology. Prog. Biophys. Mol. Biol. 2015, 117, 4–18. [Google Scholar] [CrossRef] [Green Version]
- Johnstone, R.H.; Chang, E.T.Y.; Bardenet, R.; de Boer, T.P.; Gavaghan, D.J.; Pathmanathan, P.; Clayton, R.H.; Mirams, G.R. Uncertainty and variability in models of the cardiac action potential: Can we build trustworthy models? J. Mol. Cell Cardiol. 2016, 96, 49–62. [Google Scholar] [CrossRef] [Green Version]
- Mangion, K.; Gao, H.; Husmeier, D.; Luo, X.; Berry, C. Advances in computational modeling for personalised medicine after myocardial infarction. Heart 2018, 104, 550–557. [Google Scholar] [CrossRef] [Green Version]
- Malbrain, M.L.; Marik, P.E.; Witters, I.; Cordemans, C.; Kirkpatrick, A.W.; Roberts, D.J.; Van Regenmortel, N. Fluid overload, de-resuscitation, and outcomes in critically ill or injured patients: A systematic review with suggestions for clinical practice. Anaesthesiol. Intensive Ther. 2014, 46, 361–380. [Google Scholar] [CrossRef] [PubMed]
- Byrne, L.; Van Haren, F. Fluid resuscitation in human sepsis: Time to rewrite history? Ann. Intensive Care 2017, 7, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caironi, P.; Tognoni, G.; Masson, S.; Fumagalli, R.; Pesenti, A.; Romero, M.; Fanizza, C.; Caspani, L.; Faenza, S.; Grasselli, G.; et al. Albumin replacement in patients with severe sepsis or septic shock. N. Engl. J. Med. 2014, 370, 1412–1421. [Google Scholar] [CrossRef] [Green Version]
- Finfer, S.; Bellomo, R.; Boyce, N.; French, J.; Myburgh, J.; Norton, R.; Investigators, S.S. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N. Engl. J. Med. 2004, 350, 2247–2256. [Google Scholar] [PubMed] [Green Version]
- Myburgh, J.A.; Finfer, S.; Bellomo, R.; Billot, L.; Cass, A.; Gattas, D.; Glass, P.; Lipman, J.; Liu, B.; McArthur, C.; et al. Hydroxyethyl starch or saline for fluid resuscitation in intensive care. N. Engl. J. Med. 2012, 367, 1901–1911. [Google Scholar] [CrossRef] [Green Version]
- Saville, B.R.; Berry, S.M. Efficiencies of platform clinical trials: A vision of the future. Clin. Trials 2016, 13, 358–366. [Google Scholar] [CrossRef]
- Vincent, J.L. Improved survival in critically ill patients: Are large, R.C.Ts more useful than personalized medicine? Intensive Care Med. 2016, 42, 1778–1780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J.; Vincent, J.L.; Adhikari, N.K.; Machado, F.R.; Angus, D.C.; Calandra, T.; Jaton, K.; Giulieri, S.; Delaloye, J.; Opal, S.; et al. Sepsis: A roadmap for future research. Lancet Infect. Dis. 2015, 15, 581–614. [Google Scholar] [CrossRef]
- Shakoory, B.; Carcillo, J.A.; Chatham, W.W.; Amdur, R.L.; Zhao, H.; Dinarello, C.A.; Cron, R.Q.; Opal, S.M. Interleukin-1 receptor blockade is associated with reduced mortality in sepsis patients with features of macrophage activation syndrome: Reanalysis of a prior phase III trial. Crit. Care Med. 2016, 44, 275–281. [Google Scholar] [CrossRef] [Green Version]
- Langley, R.J.; Tipper, J.L.; Bruse, S.; Baron, R.M.; Tsalik, E.L.; Huntley, J.; Rogers, A.J.; Jaramillo, R.J.; O’Donnell, D.; Mega, W.M.; et al. Integrative“omic” analysis of experimental bacteremia identifies a metabolic signature that distinguishes human sepsis from systemic inflammatory response syndromes. Am. J. Respir. Crit. Care Med. 2014, 190, 445–455. [Google Scholar] [CrossRef] [Green Version]
- McHugh, L.; Seldon, T.A.; Brandon, R.A.; Kirk, J.T.; Rapisarda, A.; Sutherland, A.J.; Presneill, J.J.; Venter, D.J.; Lipman, J.; Thomas, M.R.; et al. A Molecular Host Response Assay to Discriminate Between Sepsis and Infection-Negative Systemic Inflammation in Critically Ill Patients: Discovery and Validation in Independent Cohorts. PLoS Med. 2015, 12, e1001916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hudis, C.A. Trastuzumab—Mechanism of action and use in clinical practice. N. Engl. J. Med. 2007, 357, 39–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whirl-Carrillo, M.; McDonagh, E.M.; Hebert, J.M.; Gong, L.; Sangkuhl, K.; Thorn, C.F.; Altman, R.B.; Klein, T.E. Pharmacogenomics knowledge for personalized medicine. Clin. Pharmacol. Ther. 2012, 92, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Relling, M.V.; Klein, T.E. CPIC: Clinical Pharmacogenetics Implementation Consortium of the Pharmacogenomics Research Network. Clin. Pharmacol. Ther. 2011, 89, 464–467. [Google Scholar] [CrossRef] [PubMed]
- Fang, H.; Harris, S.C.; Liu, Z.; Zhou, G.; Zhang, G.; Xu, J.; Rosario, L.; Howard, P.C.; Tong, W. FDA drug labeling: Rich resources to facilitate precision medicine, drug safety, and regulatory science. Drug Discov. Today 2016, 21, 1566–1570. [Google Scholar] [CrossRef] [Green Version]
- Friedman, A.A.; Letai, A.; Fisher, D.E.; Flaherty, K.T. Precision medicine for cancer with next-generation functional diagnostics. Nat. Rev. Cancer 2015, 15, 747–756. [Google Scholar] [CrossRef]
- Sandoval, J.A.; Lucero, J.; Oetzel, J.; Avila, M.; Belone, L.; Mau, M.; Pearson, C.; Tafoya, G.; Duran, B.; Iglesias Rios, L.; et al. Process and outcome constructs for evaluating community-based participatory research projects: A matrix of existing measures. Health Educ. Res. 2012, 27, 680–690. [Google Scholar] [CrossRef]
- Tigges, B.B.; Miller, D.; Dudding, K.M.; Balls-Berry, J.E.; Borawski, E.A.; Dave, G.; Hafer, N.S.; Kimminau, K.S.; Kost, R.G.; Littlefield, K.; et al. Measuring quality and outcomes of research collaborations: An integrative review. J. Clin. Transl. Sci. 2019, 3, 261–289. [Google Scholar] [CrossRef] [Green Version]
- Gefenas, E.; Cekanauskaite, A.; Tuzaite, E.; Dranseika, V.; Characiejus, D. Does the “new philosophy” in predictive, preventive and personalised medicine require new ethics? EPMA J. 2011, 2, 141–147. [Google Scholar] [CrossRef] [Green Version]
- Froud, R.; Meza, T.J.; Ernes, K.O.; Slowther, A.M. Research ethics oversight in Norway: Structure, function, and challenges. BMC Health Serv. Res. 2019, 19, 24. [Google Scholar] [CrossRef]
- Maschke, K.J. Wanted: Human biospecimens. Hastings Cent. Rep. 2010, 40, 21–23. [Google Scholar] [CrossRef] [PubMed]
- Verbelen, M.; Weale, M.E.; Lewis, C.M. Cost-effectiveness of pharmacogenetic-guided treatment: Are we there yet? Pharm. J. 2017, 17, 395–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vicente, A.M.; Ballensiefen, W.; Jönsson, J.I. How personalised medicine will transform healthcare by 2030, the ICPerMed vision. J. Transl. Med. 2020, 18, 180–187. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Precision Medicine considers the individual, not the disease. A given illness can be present in all age groups, genders, and physiological/pathological conditions; however, a particular patient presents with different symptoms and responds differently to the same treatment recommendations due to their uniqueness. Bioclinical discoveries need to be implemented specifically according to subject and in order to meet personal needs.
Figure 1.
Precision Medicine considers the individual, not the disease. A given illness can be present in all age groups, genders, and physiological/pathological conditions; however, a particular patient presents with different symptoms and responds differently to the same treatment recommendations due to their uniqueness. Bioclinical discoveries need to be implemented specifically according to subject and in order to meet personal needs.

Figure 2.
Types of biosensors and their applications.

Figure 3.
From human cells to a chip: schematic workflow of microfluidics technology for human cells.
Figure 3.
From human cells to a chip: schematic workflow of microfluidics technology for human cells.

Figure 4.
Enrichment approach method for personalized medicine in septic patients.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Examples of PGx drugs and their economic evaluation.
| Drug | Therapy | Gene | Economic Evaluation |
|---|---|---|---|
| Abacavir | HIV | HLA-B | Cost-saving |
| Carbamazepine | Neurology | HLA-A, HLA-B | Cost-effective |
| Azathioprine | Rheumatology | TPMT | Cost-saving |
| Warfarine | CYP2C9 VKORC1 | Cost-saving | |
| Clopidogrel | Cardiology | CYP2C19 | Cost-effective |
| Irinotecan | Oncology | UGT1A1 | Cost-saving |
| Citalopram | Psychiatry | CYP2C19 5HTTLPR HTR2A | Cost-saving |
| Clozapine | Psychiatry | CYP2D6 H2 5-HTT 5-HT2A 5-HT2C | Cost-effective |
| Mercaptopurine | Oncology | TPMT | Cost-saving |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lazar, A.E.; Azamfirei, L. Personalized Medicine for the Critically Ill Patient: A Narrative Review. Processes 2022, 10, 1200. https://doi.org/10.3390/pr10061200
AMA Style
Lazar AE, Azamfirei L. Personalized Medicine for the Critically Ill Patient: A Narrative Review. Processes. 2022; 10(6):1200. https://doi.org/10.3390/pr10061200
Chicago/Turabian StyleLazar, Alexandra Elena, and Leonard Azamfirei. 2022. "Personalized Medicine for the Critically Ill Patient: A Narrative Review" Processes 10, no. 6: 1200. https://doi.org/10.3390/pr10061200
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.