

Temporal Fluctuations of Suicide Mortality in Japan from 2009 to 2023 Using Government Databases


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Statistical Analyses
2.3. Ethics
3. Results
3.1. Fluctuation in SMRs from 2009 to 2023
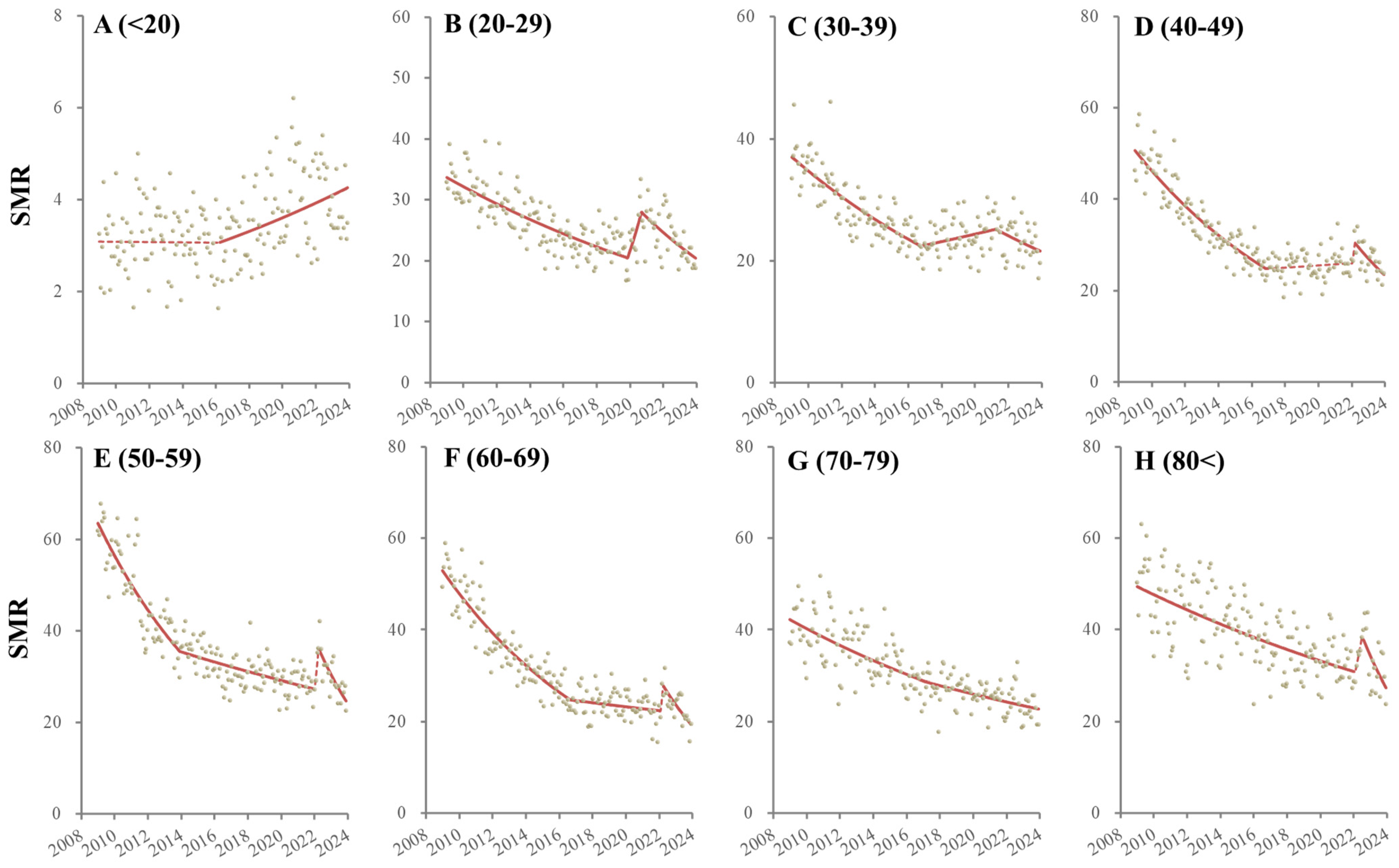
3.2. Fluctuations in Male SMRs Disaggregated by Age from 2009 to 2023
3.3. Fluctuations in Female SMRs Disaggregated by Age from 2009 to 2023
4. Discussion
4.1. Suicides among Adolescents and the Elderly
4.2. Suicide in Working-Age Females
4.3. Suicide in Working-Age Males
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hasegawa, T.; Fukuyama, K.; Okada, M. Relationships between expenditure of regional governments and suicide mortalities caused by six major motives in japan. Int. J. Environ. Res. Public Health 2022, 19, 84. [Google Scholar] [CrossRef] [PubMed]
- Shiroyama, T.; Fukuyama, K.; Okada, M. Effects of financial expenditure of prefectures/municipalities on regional suicide mortality in japan. Int. J. Environ. Res. Public Health 2021, 18, 8639. [Google Scholar] [CrossRef] [PubMed]
- Nakano, T.; Hasegawa, T.; Okada, M. Analysing the impacts of financial support for regional suicide prevention programmes on suicide mortality caused by major suicide motives in japan using statistical government data. Int. J. Environ. Res. Public Health 2021, 18, 3414. [Google Scholar] [CrossRef] [PubMed]
- Nakamoto, M.; Nakagawa, T.; Murata, M.; Okada, M. Impacts of dual-income household rate on suicide mortalities in japan. Int. J. Environ. Res. Public Health 2021, 18, 5670. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Matsumoto, R.; Yamamoto, Y.; Okada, M. Analysing effects of financial support for regional suicide prevention programmes on methods of suicide completion in japan between 2009 and 2018 using governmental statistical data. BMJ Open 2021, 11, e049538. [Google Scholar] [CrossRef] [PubMed]
- Okada, M.; Hasegawa, T.; Kato, R.; Shiroyama, T. Analysing regional unemployment rates, gdp per capita and financial support for regional suicide prevention programme on suicide mortality in japan using governmental statistical data. BMJ Open 2020, 10, e037537. [Google Scholar] [CrossRef] [PubMed]
- Kato, R.; Okada, M. Can financial support reduce suicide mortality rates? Int. J. Environ. Res. Public Health 2019, 16, 4797. [Google Scholar] [CrossRef] [PubMed]
- Saxena, S.; Setoya, Y. World health organization’s comprehensive mental health action plan 2013–2020. Psychiatry Clin. Neurosci. 2014, 68, 585–586. [Google Scholar] [CrossRef] [PubMed]
- Dhungel, B.; Sugai, M.K.; Gilmour, S. Trends in suicide mortality by method from 1979 to 2016 in japan. Int. J. Environ. Res. Public Health 2019, 16, 1794. [Google Scholar] [CrossRef]
- Wada, K.; Gilmour, S. Inequality in mortality by occupation related to economic crisis from 1980 to 2010 among working-age japanese males. Sci. Rep. 2016, 6, 22255. [Google Scholar] [CrossRef]
- Wada, K.; Kondo, N.; Gilmour, S.; Ichida, Y.; Fujino, Y.; Satoh, T.; Shibuya, K. Trends in cause specific mortality across occupations in japanese men of working age during period of economic stagnation, 1980–2005: Retrospective cohort study. BMJ 2012, 344, e1191. [Google Scholar] [CrossRef]
- Yoshioka, E.; Hanley, S.J.; Kawanishi, Y.; Saijo, Y. Time trends in method-specific suicide rates in japan, 1990–2011. Epidemiol. Psychiatr. Sci. 2016, 25, 58–68. [Google Scholar] [CrossRef]
- Yoshioka, E.; Hanley, S.J.B.; Sato, Y.; Saijo, Y. Impact of the COVID-19 pandemic on suicide rates in japan through december 2021: An interrupted time series analysis. Lancet Reg. Health–West. Pac. 2022, 24, 100480. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, R.; Motomura, E.; Onitsuka, T.; Okada, M. Trends in suicidal mortality and motives among working-ages individuals in japan during 2007–2022. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 2795–2810. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, R.; Motomura, E.; Okada, M. Impacts of complete unemployment rates disaggregated by reason and duration on suicide mortality from 2009–2022 in japan. Healthcare 2023, 11, 2806. [Google Scholar] [CrossRef]
- Matsumoto, R.; Motomura, E.; Okada, M. Fluctuation of suicide mortality and temporal causality from unemployment duration to suicide mortality in japan during 2009–2022. Asian J. Psychiatr. 2023, 84, 103574. [Google Scholar] [CrossRef]
- Okada, M. Is an increase in japan’s suicides caused by COVID-19 alone? Asian J. Psychiatr. 2022, 78, 103320. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, R.; Motomura, E.; Fukuyama, K.; Shiroyama, T.; Okada, M. Determining what changed japanese suicide mortality in 2020 using governmental database. J. Clin. Med. 2021, 10, 5199. [Google Scholar] [CrossRef]
- Sakamoto, H.; Ishikane, M.; Ghaznavi, C.; Ueda, P. Assessment of suicide in japan during the COVID-19 pandemic vs previous years. JAMA Netw. Open 2021, 4, e2037378. [Google Scholar] [CrossRef]
- Seposo, X.T. COVID-19 threatens decade-long suicide initiatives in japan. Asian J. Psychiatr. 2021, 60, 102660. [Google Scholar] [CrossRef]
- Tanaka, T.; Okamoto, S. Increase in suicide following an initial decline during the COVID-19 pandemic in japan. Nat. Hum. Behav. 2021, 5, 229–238. [Google Scholar] [CrossRef]
- Koda, M.; Harada, N.; Eguchi, A.; Nomura, S.; Ishida, Y. Reasons for suicide during the COVID-19 pandemic in japan. JAMA Netw. Open 2022, 5, e2145870. [Google Scholar] [CrossRef]
- Okada, M.; Matsumoto, R.; Motomura, E.; Shiroyama, T.; Murata, M. Exploring characteristics of increased suicide during the COVID-19 pandemic in japan using provisional governmental data. Lancet Reg. Health–West. Pac. 2022, 24, 100481. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Begum, N.; Saini, A.; Wang, S.; McGuire, P.; Fusar-Poli, P.; Lewis, G.; David, A.S. Suicide, self-harm and thoughts of suicide or self-harm in infectious disease epidemics: A systematic review and meta-analysis. Epidemiol. Psychiatr. Sci. 2021, 30, e32. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, R.; Kawano, Y.; Motomura, E.; Shiroyama, T.; Okada, M. Analyzing the changing relationship between personal consumption and suicide mortality during COVID-19 pandemic in japan, using governmental and personal consumption transaction databases. Front. Public Health 2022, 10, 982341. [Google Scholar] [CrossRef]
- Gunnell, D.; Appleby, L.; Arensman, E.; Hawton, K.; John, A.; Kapur, N.; Khan, M.; O’Connor, R.C.; Pirkis, J.; Collaboration, C.-S.P.R. Suicide risk and prevention during the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 468–471. [Google Scholar] [CrossRef]
- Kawohl, W.; Nordt, C. COVID-19, unemployment, and suicide. Lancet Psychiatry 2020, 7, 389–390. [Google Scholar] [CrossRef] [PubMed]
- Reger, M.A.; Stanley, I.H.; Joiner, T.E. Suicide mortality and coronavirus disease 2019-a perfect storm? JAMA Psychiatry 2020, 77, 1093–1094. [Google Scholar] [CrossRef]
- Tandon, R. COVID-19 and suicide: Just the facts. Key learnings and guidance for action. Asian J. Psychiatr. 2021, 60, 102695. [Google Scholar] [CrossRef]
- Menon, V.; Cherian, A.V.; Vijayakumar, L. Rising incidence and changing demographics of suicide in india: Time to recalibrate prevention policies? Asian J. Psychiatr. 2021, 69, 102983. [Google Scholar] [CrossRef]
- Arya, V.; Page, A.; Spittal, M.J.; Dandona, R.; Vijayakumar, L.; Munasinghe, S.; John, A.; Gunnell, D.; Pirkis, J.; Armstrong, G. Suicide in india during the first year of the COVID-19 pandemic. J. Affect. Disord. 2022, 307, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Pirkis, J.; John, A.; Shin, S.; DelPozo-Banos, M.; Arya, V.; Analuisa-Aguilar, P.; Appleby, L.; Arensman, E.; Bantjes, J.; Baran, A.; et al. Suicide trends in the early months of the COVID-19 pandemic: An interrupted time-series analysis of preliminary data from 21 countries. Lancet Psychiatry 2021, 8, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Ramalle-Gómara, E.; Palacios-Castaño, M.-I.; Martínez-Ochoa, E.; Quiñones-Rubio, C. Trends in suicide mortality in spain from 1998 to 2021 and its relationship with the COVID-19 pandemic: A joinpoint regression analysis. Psychiatry Res. 2023, 329, 115520. [Google Scholar] [CrossRef] [PubMed]
- de la Torre-Luque, A.; Perez-Diez, I.; Pemau, A.; Martinez-Ales, G.; Borges, G.; Perez-Sola, V.; Ayuso-Mateos, J.L. Suicide mortality in spain during the COVID-19 pandemic: Longitudinal analysis of sociodemographic factors. Eur. Neuropsychopharmacol. 2024, 82, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.; Lee, S.; Park, S.; Kang, B.; Choi, H. Analysis of suicide statistics and trends between 2011 and 2021 among korean women. Korean J. Women Health Nurs. 2023, 29, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Li, Y.; Xu, X. Suicidal ideation and suicide attempts in psychiatric patients during the COVID-19: A systematic review and meta-analysis. Psychiatry Res. 2022, 317, 114837. [Google Scholar] [CrossRef] [PubMed]
- Zohn, J.H.; Hovis, S. The impact of the global COVID-19 pandemic on risk factors for suicide in healthcare workers: A narrative review. J. Clin. Nurs. 2023, 33, 224–241. [Google Scholar] [CrossRef] [PubMed]
- Giannouli, V. Ethnicity, mortality, and severe mental illness. Lancet Psychiatry 2017, 4, 517. [Google Scholar] [CrossRef] [PubMed]
- Okada, M. Suicide mortality rates in japan before and beyond the COVID-19 pandemic era. Psychiatry Clin. Neurosci. Rep. 2024, 3, e188. [Google Scholar] [CrossRef]
- Okada, M.; Matsumoto, R.; Shiroyama, T.; Motomura, E. Suicidal mortality and motives among middle-school, high-school and university students. JAMA Netw. Open 2023, 6, e2328144. [Google Scholar] [CrossRef]
- Matsumoto, R.; Motomura, E.; Shiroyama, T.; Okada, M. Impact of the japanese government’s “general policies for comprehensive measures against suicide” on youth suicide from 2007–2022. BJPsy Open 2023, 10, e16. [Google Scholar] [CrossRef] [PubMed]
- Anzai, T.; Fukui, K.; Ito, T.; Ito, Y.; Takahashi, K. Excess mortality from suicide during the early COVID-19 pandemic period in japan: A time-series modeling before the pandemic. J. Epidemiol. 2021, 31, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, M.; Yamasaki, S.; Endo, K.; Ando, S.; Sakai, M.; Yoshii, H.; Nishida, A. Suicide rates during the COVID-19 pandemic in japan from april 2020 to december 2021. Psychiatry Res. 2022, 316, 114774. [Google Scholar] [CrossRef] [PubMed]
- Ueda, M.; Nordstrom, R.; Matsubayashi, T. Suicide and mental health during the COVID-19 pandemic in japan. J. Public Health 2022, 44, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Tanaka, H. Increased suicide mortality in japan during the COVID-19 pandemic in 2020. Psychiatry Res. 2022, 309, 114422. [Google Scholar] [CrossRef] [PubMed]
- WHO. Statement on the Fifteenth Meeting of the Ihr (2005) Emergency Committee on the COVID-19 Pandemic. Available online: https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic?gclid=CjwKCAiAgeeqBhBAEiwAoDDhn4qy9aIN3Tr9m_ryxsWPehcEORmQ6MfWenqKJYy6bfQS54DPQZALlxoC7gkQAvD_BwE (accessed on 1 April 2023).
- MHLW. Novel Coronavirus (COVID-19). Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000164708_00079.html (accessed on 1 November 2023).
- Dhungel, B.; Thapa, A.; Martinez-Rives, N.L.; Takagi, K.; Martin, P.; Wada, K.; Gilmour, S. Method-specific suicide trends from 1979 to 2016 among japanese adolescents. J. Affect. Disord. 2022, 310, 129–134. [Google Scholar] [CrossRef] [PubMed]
- MHLW. Vital Statistics Registration. Available online: https://www.e-stat.go.jp/en/statistics/00450011 (accessed on 1 January 2024).
- NPA. Suicide Statistics (Ssnpa). Available online: https://www.npa.go.jp/publications/statistics/safetylife/jisatsu.html (accessed on 30 March 2023).
- MHLW. Basic Data on Suicide in the Region. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000140901.html (accessed on 31 January 2024).
- MIAC. Surveys of Population, Population Change and the Number of Households Based on the Basic Resident Registration. Available online: https://www.e-stat.go.jp/en/statistics/00200241 (accessed on 28 December 2023).
- Pirkis, J.; Gunnell, D.; Shin, S.; Del Pozo-Banos, M.; Arya, V.; Aguilar, P.A.; Appleby, L.; Arafat, S.M.Y.; Arensman, E.; Ayuso-Mateos, J.L.; et al. Suicide numbers during the first 9–15 months of the COVID-19 pandemic compared with pre-existing trends: An interrupted time series analysis in 33 countries. EClinicalMedicine 2022, 51, 101573. [Google Scholar] [CrossRef] [PubMed]
- Linden, A. A comprehensive set of postestimation measures to enrich interrupted time-series analysis. Stata J. Promot. Commun. Stat. Stata 2017, 17, 73–88. [Google Scholar] [CrossRef]
- Linden, A. Conducting interrupted time-series analysis for single-and multiple-group comparisons. Stata J. 2015, 15, 480–500. [Google Scholar] [CrossRef]
- Bernal, J.L.; Cummins, S.; Gasparrini, A. Interrupted time series regression for the evaluation of public health interventions: A tutorial. Int. J. Epidemiol. 2017, 46, 348–355. [Google Scholar] [CrossRef]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- NCI. Joinpoint Regression Program ver4.9.1.0. Available online: https://surveillance.cancer.gov/joinpoint/ (accessed on 1 August 2022).
- WHO. Mental Health of Adolescents. Available online: https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health (accessed on 1 April 2023).
- MHLW. 2022 White Paper on Suicide Prevention. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/jisatsuhakusyo2022.html (accessed on 1 April 2023).
- Lu, C.Y.; Penfold, R.B.; Wallace, J.; Lupton, C.; Libby, A.M.; Soumerai, S.B. Increases in suicide deaths among adolescents and young adults following us food and drug administration antidepressant boxed warnings and declines in depression care. Psychiatr. Res. Clin. Pract. 2020, 2, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Bahk, J.; Jung-Choi, K. Cause-specific mortality in korea during the first year of the COVID-19 pandemic. Epidemiol. Health 2022, 44, e2022110. [Google Scholar] [CrossRef] [PubMed]
- Ji, Z.; Wu, H.; Zhu, R.; Wang, L.; Wang, Y.; Zhang, L. Trends in cause-specific injury mortality in china in 2005–2019: Longitudinal observational study. JMIR Public Health Surveill. 2023, 9, e47902. [Google Scholar] [CrossRef]
- Stefanac, N.; Hetrick, S.; Hulbert, C.; Spittal, M.J.; Witt, K.; Robinson, J. Are young female suicides increasing? A comparison of sex-specific rates and characteristics of youth suicides in australia over 2004–2014. BMC Public Health 2019, 19, 1389. [Google Scholar] [CrossRef] [PubMed]
- Bersia, M.; Koumantakis, E.; Berchialla, P.; Charrier, L.; Ricotti, A.; Grimaldi, P.; Dalmasso, P.; Comoretto, R.I. Suicide spectrum among young people during the COVID-19 pandemic: A systematic review and meta-analysis. EClinicalMedicine 2022, 54, 101705. [Google Scholar] [CrossRef] [PubMed]
- Horita, N.; Moriguchi, S. COVID-19, young people, and suicidal behaviour. Lancet Psychiatry 2023, 10, 484–485. [Google Scholar] [CrossRef] [PubMed]
- Goto, R.; Okubo, Y.; Skokauskas, N. Reasons and trends in youth’s suicide rates during the COVID-19 pandemic. Lancet Reg. Health West. Pac. 2022, 27, 100567. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef]
- Petersen, A.C.; Sarigiani, P.A.; Kennedy, R.E. Adolescent depression: Why more girls? J. Youth Adolesc. 1991, 20, 247–271. [Google Scholar] [CrossRef]
- Serio, B.; Kohler, R.; Ye, F.; Lichenstein, S.D.; Yip, S.W. A multidimensional approach to understanding the emergence of sex differences in internalizing symptoms in adolescence. Dev. Cogn. Neurosci. 2022, 58, 101182. [Google Scholar] [CrossRef]
- MHLW. Patient Survey. Available online: https://www.e-stat.go.jp/en/statistics/00450022 (accessed on 31 January 2023).
- MHLW. Annual Population and Social Security Surveys. 2021. Available online: https://www.e-stat.go.jp/en/statistics/00450431 (accessed on 1 February 2022).
- CAO. Annual Report on the Declining Birthrate. 2022. Available online: https://www8.cao.go.jp/shoushi/shoushika/whitepaper/measures/w-2022/r04webhonpen/index.html (accessed on 1 April 2023).
- Adler, A. The progress of mankind. J. Individ. Psychol. 1957, 13, 9–13. [Google Scholar]
- Winnicott, D. The Child, the Family, and the Outside World; Penguin: London, UK, 2021. [Google Scholar]
- Eisenberg, N.; Valiente, C.; Spinrad, T.L.; Liew, J.; Zhou, Q.; Losoya, S.H.; Reiser, M.; Cumberland, A. Longitudinal relations of children’s effortful control, impulsivity, and negative emotionality to their externalizing, internalizing, and co-occurring behavior problems. Dev. Psychol. 2009, 45, 988–1008. [Google Scholar] [CrossRef]
- Sheng, L.; Yang, B.; Story, M.; Wu, W.; Xi, X.; Zhou, Y.; Wen, Y.; Wang, H.; Liu, Q. Emotional and behavioral changes and related factors of firstborn school-aged compared to same age only children. Front. Public Health 2022, 10, 822761. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, L.; Baillies, J. Firstborns’ Behaviors during a mother’s second pregnancy. Nurs. Res. 1995, 44, 356–363. [Google Scholar] [CrossRef]
- Kuo, P.X.; Volling, B.L.; Gonzalez, R.; Oh, W.; Yu, T. Chapter VII. Developmental trajectories of children’s emotional reactivity after the birth of a sibling. Monogr. Soc. Res. Child Dev. 2017, 82, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Volling, B.L. Chapter XI. General discussion: Children’s adjustment and adaptation following the birth of a sibling. Monogr. Soc. Res. Child Dev. 2017, 82, 142–158. [Google Scholar] [CrossRef]
- Volling, B.L.; Oh, W.; Gonzalez, R. Chapter III. Stability and change in children’s emotional and behavioral adjustment after the birth of a sibling. Monogr. Soc. Res. Child Dev. 2017, 82, 46–52. [Google Scholar] [CrossRef]
- Volling, B.L. Family transitions following the birth of a sibling: An empirical review of changes in the firstborn’s adjustment. Psychol. Bull. 2012, 138, 497–528. [Google Scholar] [CrossRef]
- Goschin, S.; Briggs, J.; Blanco-Lutzen, S.; Cohen, L.J.; Galynker, I. Parental affectionless control and suicidality. J. Affect. Disord. 2013, 151, 1–6. [Google Scholar] [CrossRef]
- Parker, G. Parental characteristics in relation to depressive disorders. Br. J. Psychiatry 2018, 134, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Heider, D.; Matschinger, H.; Bernert, S.; Alonso, J.; Angermeyer, M.C. Relationship between parental bonding and mood disorder in six european countries. Psychiatry Res. 2006, 143, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Heider, D.; Matschinger, H.; Bernert, S.; Alonso, J.; Brugha, T.S.; Bruffaerts, R.; de Girolamo, G.; Dietrich, S.; Angermeyer, M.C. Adverse parenting as a risk factor in the occurrence of anxiety disorders. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Silove, D.; Parker, G.; Hadzi-Pavlovic, D.; Manicavasagar, V.; Blaszczynski, A. Parental representations of patients with panic disorder and generalised anxiety disorder. Br. J. Psychiatry 2018, 159, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Lennertz, L.; Grabe, H.J.; Ruhrmann, S.; Rampacher, F.; Vogeley, A.; Schulze-Rauschenbach, S.; Ettelt, S.; Meyer, K.; Kraft, S.; Reck, C.; et al. Perceived parental rearing in subjects with obsessive–compulsive disorder and their siblings. Acta Psychiatr. Scand. 2010, 121, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Bienvenu, O.J.; Krasnow, J.; Wang, Y.; Grados, M.A.; Cullen, B.; Goes, F.S.; Maher, B.; Greenberg, B.D.; McLaughlin, N.C.; et al. Parental bonding and hoarding in obsessive–compulsive disorder. Compr. Psychiatry 2017, 73, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Siqueira-Campos, V.M.; De Deus, M.S.C.; Carneiro, L.A.; Naghettini, A.V.; Pereira, M.A.D.; De Deus, J.M.; Conde, D.M.; Harrison, P. Dysfunctional parenting styles are associated with mental disorders and low self-efficacy beliefs in brazilian undergraduate medical students. BioMed Res. Int. 2021, 2021, 6372922. [Google Scholar] [CrossRef] [PubMed]
- Parker, G.; Tupling, H.; Brown, L.B. A parental bonding instrument. Br. J. Med. Psychol. 2011, 52, 1–10. [Google Scholar] [CrossRef]
- Otani, K.; Suzuki, A.; Matsumoto, Y.; Enokido, M.; Shirata, T. Effects of perceived affectionless control parenting on working models of the self and other. Psychiatry Res. 2016, 242, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Tugnoli, S.; Casetta, I.; Caracciolo, S.; Salviato, J. Parental bonding, depression, and suicidal ideation in medical students. Front. Psychol. 2022, 13, 877306. [Google Scholar] [CrossRef]
- Karasawa, M.; Curhan, K.B.; Markus, H.R.; Kitayama, S.S.; Love, G.D.; Radler, B.T.; Ryff, C.D. Cultural perspectives on aging and well-being: A comparison of japan and the united states. Int. J. Aging Hum. Dev. 2011, 73, 73–98. [Google Scholar] [CrossRef] [PubMed]
- Maree, J.G. The psychosocial development theory of erik erikson: Critical overview. Early Child Dev. Care 2021, 191, 1107–1121. [Google Scholar] [CrossRef]
- Sachs-Ericsson, N.; Van Orden, K.; Zarit, S. Suicide and aging: Special issue ofaging & mental health. Aging Ment. Health 2015, 20, 110–112. [Google Scholar] [PubMed]
- Campos, B.; Kim, H.S. Incorporating the cultural diversity of family and close relationships into the study of health. Am. Psychol. 2017, 72, 543–554. [Google Scholar] [CrossRef] [PubMed]
- Meda, N.; Miola, A.; Slongo, I.; Zordan, M.A.; Sambataro, F. The impact of macroeconomic factors on suicide in 175 countries over 27 years. Suicide Life Threat. Behav. 2022, 52, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Ying, Y.H.; Chang, K. A study of suicide and socioeconomic factors. Suicide Life Threat. Behav. 2009, 39, 214–226. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.S.; Stuckler, D.; Yip, P.; Gunnell, D. Impact of 2008 global economic crisis on suicide: Time trend study in 54 countries. BMJ 2013, 347, f5239. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Wu, K.C.; Yousuf, S.; Yip, P.S. Suicide in asia: Opportunities and challenges. Epidemiol. Rev. 2012, 34, 129–144. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Yip, P.S.; Lee, C.; Fan, H.F.; Fu, K.W. Economic fluctuations and suicide: A comparison of taiwan and hong kong. Soc. Sci. Med. 2010, 71, 2083–2090. [Google Scholar] [CrossRef]
- WHO. Suicide in the World in 2019. Available online: https://apps.who.int/iris/handle/10665/326948 (accessed on 18 November 2020).
- MHLW. Labour Force Survey. Available online: https://www.e-stat.go.jp/statistics/00200531 (accessed on 1 December 2023).
- Cabinet-Office. COVID-19 Information and Resources. Available online: https://corona.go.jp/en/ (accessed on 1 August 2023).
- METI. 2023 White Paper on Small and Medium Enterprises in Japan. Available online: https://www.chusho.meti.go.jp/pamflet/hakusyo/index.html (accessed on 1 January 2024).
- Hoffman, M.; Bearman, P. Bringing anomie back in: Exceptional events and excess suicide. Sociol. Sci. 2015, 2, 186–210. [Google Scholar] [CrossRef]
- Marra, R.; Orru, M. Social images of suicide. Br. J. Sociol. 1991, 42, 273–288. [Google Scholar] [CrossRef] [PubMed]
- Phillips, J.A.; Nugent, C.N. Suicide and the great recession of 2007–2009: The role of economic factors in the 50 u.S. States. Soc. Sci. Med. 2014, 116, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Lutter, M.; Roex, K.L.A.; Tisch, D. Anomie or imitation? The werther effect of celebrity suicides on suicide rates in 34 oecd countries, 1960–2014. Soc. Sci. Med. 2020, 246, 112755. [Google Scholar] [CrossRef]
- Foulkes, L.; Blakemore, S.J. Individual differences in adolescent mental health during COVID-19: The importance of peer relationship quality. Neuron 2021, 109, 3203–3205. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Lower Endpoint | Upper Endpoint | MPC | p | ||
|---|---|---|---|---|---|
| Male + Female | 2009/1 | 2017/1 | −0.57 | <0.01 | ** |
| 2017/2 | 2022/9 | 0.14 | 0.01 | * | |
| 2022/10 | 2023/12 | −1.19 | 0.02 | * | |
| Male | 2009/1 | 2016/12 | −0.60 | <0.01 | ** |
| 2017/1 | 2022/9 | −0.01 | 0.07 | ||
| 2022/10 | 2023/12 | −1.15 | 0.02 | * | |
| female | 2009/1 | 2019/12 | −0.43 | <0.01 | ** |
| 2020/1 | 2020/10 | 3.24 | <0.01 | ** | |
| 2020/11 | 2023/12 | −0.62 | <0.01 | ** |
| Age | (Males) | Lower Endpoint | Upper Endpoint | MPC | p | (Females) | Lower Endpoint | Upper Endpoint | MPC | p | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| <20 | 2009/1 | 2016/3 | −0.01 | 0.93 | 2009/1 | 2014/12 | −0.45 | 0.01 | * | |||
| 2016/4 | 2023/12 | 0.35 | <0.01 | ** | 2015/1 | 2023/12 | 0.07 | <0.01 | ** | |||
| (2020/4) | 0.27 (jump) | <0.01 | ** | |||||||||
| 20–29 | 2009/1 | 2019/11 | −0.38 | <0.01 | ** | 2009/1 | 2016/8 | −0.65 | <0.01 | ** | ||
| 2019/12 | 2020/9 | 3.16 | 0.04 | * | 2016/9 | 2019/12 | 0.41 | 009 | ||||
| 2020/10 | 2023/12 | −0.80 | <0.01 | ** | 2020/1 | 2020/11 | 4.38 | 0.04 | * | |||
| 2020/12 | 2023/12 | −0.66 | <0.01 | ** | ||||||||
| 30–39 | 2009/1 | 2016/10 | −0.54 | <0.01 | ** | 2009/1 | 2019/12 | −0.55 | <0.01 | ** | ||
| 2016/11 | 2021/4 | 0.22 | 0.04 | * | 2020/1 | 2020/10 | 4.72 | 0.02 | * | |||
| 2021/5 | 2023/12 | −0.48 | 0.03 | * | 2020/11 | 2023/12 | −0.83 | <0.01 | ** | |||
| 40–49 | 2009/1 | 2016/11 | −0.76 | <0.01 | ** | 2009/1 | 2019/12 | −0.47 | <0.01 | ** | ||
| 2016/12 | 2021/12 | 0.08 | 0.29 | 2020/1 | 2020/10 | 4.00 | 0.03 | * | ||||
| 2022/1 | 2022/3 | 8.17 | 0.48 | 2020/11 | 2023/12 | −0.88 | <0.01 | ** | ||||
| 2022/4 | 2023/12 | −1.23 | <0.01 | ** | ||||||||
| 50–59 | 2009/1 | 2013/11 | −0.98 | <0.01 | ** | 2009/1 | 2020/4 | −0.32 | <0.01 | ** | ||
| 2013/12 | 2022/1 | −0.27 | <0.01 | ** | 2020/5 | 2020/8 | 16.59 | <0.01 | ** | |||
| 2022/1 | 2022/4 | 9.81 | 0.56 | 2020/9 | 2023/12 | −0.47 | 0.01 | * | ||||
| 2022/5 | 2023/12 | −1.90 | <0.01 | ** | ||||||||
| 60–69 | 2009/1 | 2016/9 | −0.82 | <0.01 | ** | 2009/1 | 2020/2 | −0.59 | <0.01 | ** | ||
| 2016/10 | 2022/1 | −0.16 | 0.05 | * | 2020/2 | 2020/9 | 3.02 | 0.14 | ||||
| 2022/2 | 2022/4 | 11.44 | 0.44 | 2020/9 | 2023/12 | −0.64 | <0.01 | ** | ||||
| 2022/5 | 2023/12 | −1.78 | <0.01 | ** | ||||||||
| 70–79 | 2009/1 | 2017/2 | −0.39 | <0.01 | ** | 2009/1 | 2020/5 | −0.43 | <0.01 | ** | ||
| 2017/3 | 2023/12 | −0.28 | <0.01 | ** | 2020/7 | 2020/7 | 9.47 | 0.79 | ||||
| 2020/7 | 2023/12 | −0.91 | <0.01 | ** | ||||||||
| >80 | 2009/1 | 2022/1 | −0.30 | <0.01 | ** | 2009/1 | 2020/4 | −0.55 | <0.01 | ** | ||
| 2022/2 | 2022/7 | 4.56 | 0.55 | 2020/4 | 2020/7 | 5.08 | 0.83 | |||||
| 2022/8 | 2023/12 | −1.98 | 0.01 | * | 2020/7 | 2023/12 | −0.60 | <0.01 | ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumoto, R.; Motomura, E.; Okada, M. Temporal Fluctuations of Suicide Mortality in Japan from 2009 to 2023 Using Government Databases. Eur. J. Investig. Health Psychol. Educ. 2024, 14, 1086-1100. https://doi.org/10.3390/ejihpe14040071
Matsumoto R, Motomura E, Okada M. Temporal Fluctuations of Suicide Mortality in Japan from 2009 to 2023 Using Government Databases. European Journal of Investigation in Health, Psychology and Education. 2024; 14(4):1086-1100. https://doi.org/10.3390/ejihpe14040071
Chicago/Turabian StyleMatsumoto, Ryusuke, Eishi Motomura, and Motohiro Okada. 2024. "Temporal Fluctuations of Suicide Mortality in Japan from 2009 to 2023 Using Government Databases" European Journal of Investigation in Health, Psychology and Education 14, no. 4: 1086-1100. https://doi.org/10.3390/ejihpe14040071