


Solid Phase Microextraction—A Promising Tool for Graft Quality Monitoring in Solid Organ Transplantation

Department of Pharmacodynamics and Molecular Pharmacology, Faculty of Pharmacy, Collegium Medicum in Bydgoszcz, Nicolaus Copernicus University in Torun, 85-089 Bydgoszcz, Poland
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Separations 2023, 10(3), 153; https://doi.org/10.3390/separations10030153
Submission received: 29 December 2022
/
Revised: 20 February 2023
/
Accepted: 21 February 2023
/
Published: 23 February 2023
(This article belongs to the Special Issue Women in Separations)
Abstract
:Solid organ transplantation is a life-saving intervention for patients suffering from end-stage organ failure. Although improvements in surgical techniques, standards of care, and immunosuppression have been observed over the last few decades, transplant centers have to face the problem of an insufficient number of organs for transplantation concerning the growing demand. An opportunity to increase the pool of organs intended for transplantation is the more frequent use of organs from extended criteria and the development of analytical methods allowing for a better assessment of the quality of organs to minimize the risk of post-transplant organ injury and rejection. Therefore, solid-phase microextraction (SPME) has been proposed in various studies as an effective tool for determining compounds of significance during graft function assessment or for the chemical profiling of grafts undergoing various preservation protocols. This review summarizes how SPME addresses the analytical challenges associated with different matrices utilized in the peri-transplant period and discusses its potential as a diagnostic tool in future work.
1. Introduction
Solid organ transplantation is a life-saving intervention for patients suffering from end-stage organ failure. The transplantation of livers, kidneys, hearts, and lungs has become a routine part of clinical care worldwide, and has contributed to higher survival rates and greater quality of life among patients [1]. Over the last few decades, advancements in surgical techniques, standards of care, and immunosuppression have significantly improved transplantation outcomes. However, the number of patients on waiting lists for all solid organs has rapidly increased, resulting in an ever-growing disparity between organ availability and demand [2]. Furthermore, this shortage of donor organs is exacerbated by the fact that many organs are ultimately deemed unsuitable for transplantation due to strict criteria and are discarded as a result [3]. Indeed, it is estimated that only 20% of lungs and less than 40% of hearts are considered suitable for transplantation [4,5].
Given this scarcity of viable organs, strategies aimed at increasing the donor pool, reducing patient wait times, and decreasing the number of unnecessarily discarded organs are crucial. Among such strategies, one of the most notable is the use of organs from expanded criteria donors (ECD) and donors after circulatory death (DCD) [6,7]. However, it is well known that compared with standard criteria donors (SCD), marginal grafts tend to have worse outcomes, including an increased risk of delayed graft function (DGF) and primary nonfunction incidence (PNF) [8,9]. Hence, there is a great need for accurate methods of assessing graft quality and estimating donor risk, especially in relation to marginal grafts. Currently, an organ’s suitability for transplantation is determined based on detailed parameters, including the donor’s medical history and examination results. Depending on the organ, different parameters will be considered. The factors taken into account when assessing organ quality include, among others: smoking history, chest X-rays, oxygenation, active infections, hemodynamic stability, electrocardiograms, echocardiograms, serum bilirubin, AST, ALT, creatinine concentration, visual assessment of the organ, and biopsy [7,10,11,12,13]. Unfortunately, the decision-making process for accepting an organ for transplantation is always subjective to some extent and often lacks sufficient overall predictive power. Furthermore, many of the evaluated parameters cannot be used as independent predictors due to their low specificity.
The transplant team’s visual assessment of donor organs is often fundamental in decision-making. Although a general inspection can help to identify tumors and anatomical changes, this method is subjective and depends on the transplant team’s experience level [12]. In the case of heart transplants, several studies have indicated that elevated troponin levels in donor serum may be related to primary graft dysfunction (PGD). However, higher troponin levels in serum from donors who have experienced brain death may be a result of the brain’s degradation rather than an indication of myocardial damage [7,14]. Similarly, left ventricular dysfunction is another common reason for discarding potential transplant organs, but this condition may be caused by a potentially reversible sequela of brain death, rather than a defective heart [14]. For lung transplants, non-smokers are ideal donors, as a donor history of smoking has been related to PGD. Nonetheless, findings have shown that recipients who received a graft from an actively smoking donor have significantly lower mortality compared to patients who remained on the waiting list [15]. In the case of kidney and liver transplantation, pre-transplant biopsies remain the gold standard for diagnosing organ injury. However, histological assessments are usually applied selectively, predominantly in ECD and DCD grafts, and the frequency of performed biopsies varies between medical facilities and countries. Although biopsies can provide comprehensive information relating to organ status, the role of a pre-transplant biopsy in graft evaluation is intensely debated. The use of biopsies to evaluate graft quality is hampered by two major limitations: the low reproducibility of results between on-call pathologists, and their time-consuming nature. Previous studies have analyzed the consistency of scores assigned to kidney donor biopsies by different on-call pathologists and the retrospective evaluation of the same sections performed by the renal pathologist. Interestingly, a correlation between donor histology and graft outcome was observed in the evaluations performed by the renal pathologists, but not in the evaluations performed by the on-call pathologists [16]. Thus, histological evaluation remains only one component of graft assessment and should not be the sole determinant in deciding whether to accept an organ for transplantation or to discard it. All of the above examples illustrate the comprehensiveness and complexity of organ-quality assessment and the decision-making processes. In an attempt to improve and standardize the evaluation process, researchers have developed several scoring systems aimed at providing an objective estimate of post-transplant survival based on donors’ and/or recipients’ characteristics. Two of these systems, the Kidney Donor Risk Index (KDRI) and the Liver Donor Risk Index (LDRI), are among the most established metrics for estimating graft survival; however, new solutions are still being proposed [17]. Although risk indices can facilitate and improve the decision-making process, they are not intended to serve as the only metric for determining donor suitability; rather, they should be utilized as part of a comprehensive evaluation along with other factors. Furthermore, while donor age is one of the most influential factors in calculating most risk indexes, it is not well-established whether these indexes can be applied to elderly and pediatric donors [18,19].
Another way to increase the donor pool is the implementation of new organ preservation methods. At present, static cold storage (SCS) is the standard technique for organ preservation in clinical practice due to its readily available logistics and low cost. The hypothermic conditions of SCS reduce the organ’s metabolic activity and oxygen demand, thereby reducing ischemic injury. However, ECD grafts appear to be more prone to prolonged ischemia, resulting in increased morbidity and mortality in recipients. Thus, the technique of preserving these types of organs is crucial [20,21]. In recent years, numerous preclinical and clinical studies have sought to develop and optimize alternative organ-preservation methods in an attempt to improve the outcomes of ECD graft transplantation. Currently, the proposed machine perfusion methods can be divided into three categories based on the pumping temperature of the preservation solution and the oxygen supply (i.e., with or without oxygen): normothermic (35–37 °C), sub-normothermic (20–25 °C), and hypothermic (4–10 °C) [22]. These methods are advantageous because they minimize the risk of organ damage and early allograft dysfunction (EAD), in addition to allowing the administration of additional pharmacological agents for protective ischemic postconditioning and for assessing organ function immediately before transplantation [4,5]. Unfortunately, although machine perfusion enables the monitoring of perfusion parameters that can predict organ viability after transplantation, there is still a lack of representative methods for assessing graft quality.
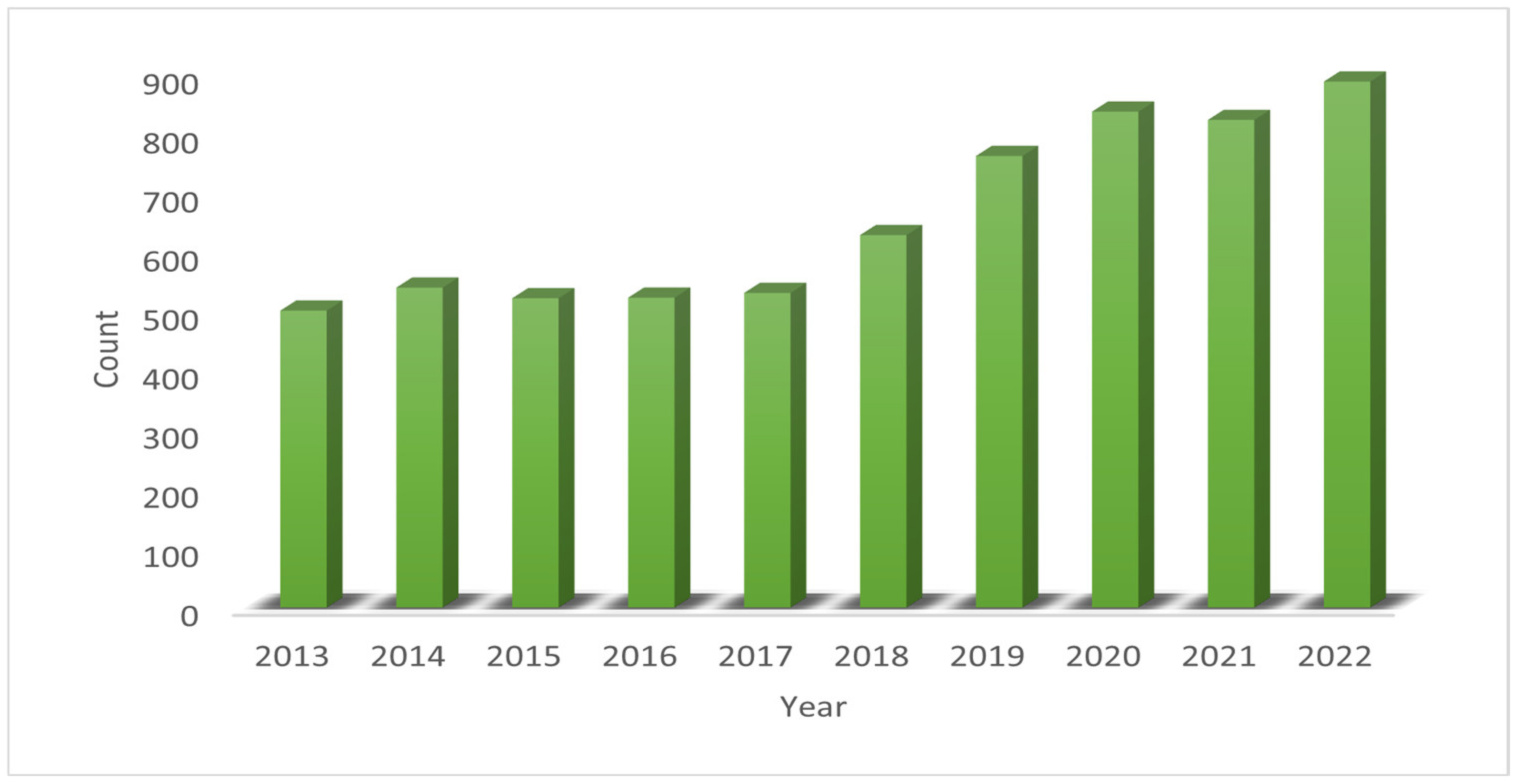
Solid-phase microextraction (SPME) is a widely accepted analytical method in bioanalysis. Undoubtedly, the analysis of volatile compounds in the headspace of a given sample is both the original and most studied application of SPME. However, in recent years, the direct extraction of non-volatile compounds from complex matrices has emerged as a very attractive alternative to conventional sample preparation methods in bioanalysis. While SPME fibers—which are probes with a small diameter (ca. 250 nm)—are the most well-known geometry, thin-film devices are also frequently used, as their larger coating area and use of higher sorbent volumes enables greater sensitivity. The literature contains numerous reviews detailing developments in and applications of SPME [23,24,25,26,27,28,29,30]. In addition, there is an ever-growing trend showing that the SPME technique is increasingly used for sample preparation prior to analysis in recent years (Figure 1).
In brief, SPME is an equilibrium-based technique that extracts via free concentration. In complex matrices containing macromolecules (e.g., proteins), small species equilibrate with the macromolecules so that they are partially bound and partially free. In general, the more hydrophobic the compound, the higher the binding and the lower the free concentration; therefore, one would expect SPME to perform poorly in recovering these species. However, the coatings most commonly used in bioanalysis, such as C18 or mixed-mode coatings, have a high affinity toward hydrophobic compounds, thus compensating for the aforementioned phenomenon. The opposite situation is observed for hydrophilic metabolites, thereby allowing SPME to provide balanced coverage of the compounds. Another feature of SPME that should be emphasized is its capacity for capturing unstable species, which is made possible by its ability to extract small compounds while excluding large molecules. The chemistry and porosity of commonly used SPME coatings restrict the penetration of macromolecules into the sorbent, which protects the absorbed metabolites from enzymatic degradation. Moreover, due to the small size of probes (e.g., fibers), SPME affords minimal invasiveness and allows the same organ to be sampled several times without damaging the tissue. Conventional sample preparation methods demand the collection and homogenization of tissue, followed by the extraction of analytes with aqueous and organic solvents. Such techniques are widely used; however, their complex protocols make them unsuitable for on-site extraction. Additionally, tissue collection usually restricts analysis to a single sampling because repeated biopsy carries the risk of tissue damage and other side effects [31]. Because of SPME’s unique features—which include, but are not limited to, balanced analyte coverage, minimal invasiveness [32], lack of physical sample consumption [33], the ability to extract labile metabolites and determine free (i.e., active) concentrations of metabolites [34], and the biocompatibility of SPME probes—new applications are continually being tested and proposed. As mentioned above, one of the major challenges in transplant surgery is assessing graft quality and function in order to minimize the risk of post-transplant organ injury and rejection. Given the above-discussed possibilities, SPME has been proposed in various studies as an effective tool for determining compounds of significance during graft function assessment, or for the chemical profiling of grafts undergoing various preservation protocols. The recent literature contains numerous papers detailing the use of SPME and omics approaches to assess the quality of organs intended for transplantation. As such, this review summarizes how solid-phase microextraction addresses the analytical challenges associated with different matrices utilized in the peri-transplant period (Figure 2) and discusses its potential as diagnostic tool in future work. The main assumptions of the cited studies are summarized in Table 1.
2. Monitoring Graft Function in Donor Specimens
One of the first protocols involving both thin-film and solid-phase microextraction explored the diagnostic value of bronchoalveolar lavage fluid (BALF) in lung transplant patients [35]. The presence of bile acids (BAs) and pepsin in BALF is a marker of the aspiration of gastric components, which carries a risk of obliterative bronchiolitis and allograft dysfunction. In routine clinical practice, the total concentration of bile acids is measured using an enzymatic assay; however, this method is not specific and might be associated to cross-reactions. Mass spectrometry coupled to liquid chromatography is capable of successfully measuring individual bile acids. As such, Bessonneau et al. combined this approach with PAN-C18-coated thin-film microextraction (TFME) blades for the determination of cholic acid (CA) and deoxycholic acid (DCA), which served as representatives of di- and trihydroxy bile acids, respectively. Their method-validation results showed good figures of merit, with an RSD < 4% and an LOQ of 0.02 μmol/L. In addition, the results obtained for the clinical samples revealed that the proposed method was able to detect the investigated bile acids at concentrations below the LOQ. The summary concentration of the two acids ranged from 0.02 to 0.06 μmol/L and was correlated with the results of the enzymatic assay (TBA 0.01 to 0.24 μmol/L). While no correlation was found (R2 = 0.11) when all of the studied samples were included in the comparison, the removal of one patient’s data resulted in a correlation coefficient of 0.92. BALF samples were also extracted using fibers with a mix-mode coating, followed by untargeted profiling on a high-resolution orbitrap mass spectrometer. Here, the results revealed that of the few thousand detected features, three belonged to bile acids, with 7-ketolithocholic acid as the predominant type (ca. 94% of all BAs). The summary peak area of the identified bile acids correlated with the TBA enzymatic assay data (R2 = 0.86). Interestingly, the principal component analysis plot showed clear separation between two groups of patients, which was characterized by the TBA value < and > 0.05 μmol/L. This separation was driven by the 13 metabolites in the “TBA > 0.05 μmol/L” group but was absent in the other. Among these compounds were three bile acids, one steroid, three fatty aldehydes, one fatty alcohol, two prenol lipids, one fatty amide, and two fatty acids (p-value <0.01 and fold change ≥5). These results highlighted the importance of re-considering the TBA cut-off value for “healthy/sick” BALF samples, which is currently set for 0.2 μmol/L. Furthermore, Bessonneau et al.’s work also demonstrated the potential diagnostic value of metabolites apart from BAs in assessing the risk of obliterative bronchiolitis and lung allograft dysfunction. Elsewhere, Stefanuto et al. proposed a different SPME-based approach for identifying PGD after lung transplantation in BALF and blind bronchial aspirate (BBA) samples [36]. To this end, the authors employed 2 cm divinylbenzene/carboxen/polydimethylsiloxane (DVB/CAR/PDMS) fibers to extract volatile compounds from the headspace of 20 mL headspace vial that contained 500 µL of lung fluid samples and was sealed with a PTFE/silicone cap. The extracted analytes were then analyzed via two-dimensional gas chromatography coupled to a time-of-flight mass spectrometer (HS-SPME-GC × GC-TOFMS). In the first step, samples obtained at the end of transplant surgery were profiled and the VOC patterns of patients who later developed severe PGD and those who either did not develop PGD, or who only developed low-grade PGD (0-2), were compared. In the next step, a support vector machine (SVM) with a linear kernel on the training set model was built to select features discriminating the studied groups at the first 6 h after transplantation. For 20 selected compounds, the SVM model provided sensitivity of 0.63, specificity of 0.94, and positive and negative predictive value of 0.87 and 0.80, respectively. The majority of the detected compounds were up-regulated in grade 3 PGD (Figure 3).
Given the complexity of the factors influencing the VOC profiles, the authors employed a multivariate analysis of variance (MANOVA) to assess how clinical risk factors influenced the VOC patterns. The results showed no statistically significant relationships between the VOC profile and the type of donation, cause of death, or time of ischemia. Instead, the donor’s body mass index (BMI) was found to be most strongly correlate with the VOC pattern (p < 0.05). From a biochemical point of view, the results indicated the potential importance of lipid peroxidation in the development of PGD; from a diagnostic point of view, the findings demonstrated that the analysis of volatile compounds in lung fluids may be applicable in clinical practice.
Yang et al. tested a completely different hypothesis in liver transplant patients [37]. In this work, they sought to determine the concentrations of two drugs (i.e., rocuronium bromide (ROC) and tranexamic acid (TXA)) routinely used during transplant surgery in order to evaluate liver and kidney performance in patients receiving grafts from living donors (LD) or heart beating brain dead donors (HBD). Although the transplanted grafts in living donors were smaller (<50%) compared to those from the HBDs (full size), the latter group of grafts may result in worse outcomes due to the longer ischemia times required for graft preservation. Rocuronium bromide is primarily eliminated through hepatobiliary excretion (up to 90%), with the kidneys excreting only about 10%. In contrast, the kidneys are the main route through which TXA is eliminated (>95%). Therefore, the simultaneous monitoring of these two drugs can potentially provide insight into the development of multiorgan dysfunction in the neohepatic phase. The extractions were performed using high-throughput TFME with stainless steel blades coated with polyacrylonitrile (PAN) and weak cation exchange (WCX) particles according to a previously published method [46]. The WCX particles were selected to compensate for the characteristics of ROC; specifically, as a quaternary ammonium compound, sample preparation for ROC can be challenging due to its propensity to interact with glass surfaces. Moreover, prior studies have reported that due to its instability in collected blood samples, ROC analysis requires sample acidification, which may affect the analysis of other metabolites and drugs from the same sample. The method proposed by Gorynski et al. [46] enabled the effective extraction of both analytes of interest without the need for matrix modification. The obtained data was further used to build pharmacokinetic profiles of the targeted drugs using a two-compartment model. In the case of ROC, liver clearance was lower in the HBD group, while the LD group showed similar clearance to that observed in people with normal liver function. While the comparison of TXA renal clearance did not reveal any significant differences between the HBD and LD cohorts, it was found to be slightly lower than normal in both cases. In addition to targeted drug analysis, TFME coated with hydrophilic-lipophilic balance (HLB) particles was applied for the metabolomic profiling of plasma. The HBD and LD groups formed separate clusters, with oxidized lipids and bile acids being identified as the main discriminating metabolites. The SPME-LC-MS measurements were supplemented by determining the relative expression of miR-122, miR-148a, and γ-glutamyltranspeptidase (GGT), a known biomarker of liver injury. Indeed, GGT levels were significantly higher in HBD patients, suggesting that this increase may have been the result of cold ischemia time (CIT) and may result in injury to the sinusoidal epithelial cells. The study’s findings demonstrated that ROC analysis may be a good indicator of early liver function, while TXA clearance may be a promising marker of the granular filtration rate and, consequently, chronic or acute renal injury, which may lead to early graft dysfunction. On the other hand, metabolomic profiling may help to develop a more detailed understanding of the mechanisms underlying the development of graft injury, in addition to identifying potential diagnostic biomarkers.
Łuczykowski et al. developed a high-throughput sample-analysis protocol based on TFME to evaluate the metabolomic profiles of bile samples from porcine model donors with mild (HBD) and moderate warm ischemia (DCD) grafts that had been subjected to SCS or normothermic ex vivo liver perfusion (NEVLP) prior to transplantation [38]. Extraction was performed using steel blades coated with an HLB sorbent, and each sample consisted of 10 µL of bile diluted in phosphate-buffered saline (1:99). The extraction and desorption times were 120 min, and an ACN:H2O (80:20, v:v) mixture was selected as the desorption solution. The findings showed that the bile produced in the SCS-preserved livers was characterized by increased levels of chenodeoxycholic acid, arachidonic acid, and 5S-hydroxyeicosatetraeonic acid, as well as saturated and monounsaturated LPCs, which may be due to changes in the bile acid synthesis pathways and organ inflammation. In addition, the metabolomic profile of bile produced by the SCS-preserved livers changed after a short-term (30 min) ischemia (22 and 7 statistically significant differentiating compounds for reperfusion and POD, respectively), while significant changes only appeared in the NEVLP group after 90 min. These metabolites primarily consisted of amino acids and lipids, including bile acids and steroid compounds, along with their derivatives. Moreover, a linear relationship was observed between levels of lipids from the LPC group and the organ ischemia time. Ultimately, Łuczykowski et al. identified a number of metabolites worth considering in future targeted and fully validated analyses as potential markers of changes occurring in preserved grafts. Based on the above experiment, Łuczykowski et al. conducted a subsequent pilot study to assess whether BA concentrations in bile are correlated with changes in the transplanted organ [39]. Here, sample preparation was performed via TFME using C18 sorbent as the extraction phase and methanol as the desorption solvent. Due to the high concentration of BA in this biological matrix, dilution factors of 100x and 20,000x were used to cover a wide range of primary and secondary BA concentrations. Conjugated forms of bile acids (with taurine or glycine) were significantly predominant in the bile samples compared to unconjugated forms. High concentrations of taurocholic acid characterized the perfusion period and they remained high during reperfusion in the 90′DCD group. Furthermore, prolonged ischemia caused an increase in taurodeoxycholic (15,87 ± 8,22 vs. 2,83 ± 0,57 ug/mL) and glycodeoxycholic acid (135,82 ± 78,5 vs. 18,56 ± 4,57 ug/mL) levels in the first days after transplantation compared to the HBD group.
3. Monitoring Graft Function by Direct Analysis of Graft
As noted above, the wide range of SPME applications is largely attributable to the tremendous variability of the devices. One unique feature making SPME ideal for in vivo and in situ analyses of intact tissues and organs is its low invasiveness when using the fiber geometry. There are other restrictions and requirements related to in vivo sampling, particularly when human subjects are involved in the studies, such as biocompatibility, single use of the devices, and sterilizability in the conditions established in the given hospital (in most cases, via autoclaving or ethylene oxide sterilization). As previously detailed, SPME is a safe and minimally invasive tissue sampling technique capable of providing coverage for a broad spectrum of metabolites. Moreover, the miniaturized nature of the device enables simultaneous analysis in different areas of the organ and more importantly, multiple analyses of the same organ over time.
The very first trials to use SPME for the direct extraction of metabolites from organ grafts focused on evaluating not only the method’s efficiency, but also the utilized storage and transportation conditions [40]. For the latter objective, the authors used pig liver grafts undergoing NEVLP. Six 7 mm mix-mode fibers were used to perform extractions on-site during graft perfusion, while three identical fibers were used to perform extractions from liver fragments, which had been collected at the beginning of the medical procedure and stored at −80 °C after being transported to the laboratory in dry ice. Immediately after sampling, the six fibers were divided into two groups. The first group was subjected to desorption on-site, with the resultant extracts being transported to the laboratory and stored using the same conditions described for the tissue, while the second group of fibers was secured in the empty vials for transportation and storage. As expected, the results revealed marked differences between the three approaches. The authors suggested that the discrepancies between on-fiber storage and in vivo sampling followed by extract storage may have been due to the partial evaporation of the desorption solvent, and thus, the preconcentration of the metabolites. To address this issue, complete evaporation and reconstitution in lab would be advisable. On the other hand, the in vivo vs. ex vivo sampling was characterized by differences in the presence of metabolites. For instance, in the extracts from ex vivo sampling, the authors observed the absence of some labile metabolites (e.g., itaconic acid, hypoxanthine, lactaldehyde or hydroxyacetone), but the presence of metabolites recognized as the products of the primary metabolite degradation (e.g., diacylglycerol). Although the untargeted nature of these studies precluded the strict monitoring of the extracted metabolites’ stability, the results indicated that in vivo sampling followed by on-fiber storage was the most convenient strategy. With regards to method performance, the authors tested three fiber coating lengths (i.e., 4, 7, and 15 mm) for 30 min extractions from liver tissue. The best sensitivity was observed for the 15 mm coating, while reproducibility was better for the two shorter coatings, which was likely due to the heterogeneity of the liver. When selecting the optimum sorbent length, it is very important to carefully consider all aspects of the experiment, including: the main goal of the experiment (spatial resolution studies e.g., characterization of the specific region such as malignant lesion vs. obtaining average information about the studied area); characteristics of the sampled tissue (homo- vs. heterogenous); size of the studied area; and the properties and concentrations of the compounds of interest. Furthermore, in clinical environments, particularly during surgical procedures, restrictions related to sampling time are very challenging from an analytical perspective. Specifically, while the method’s overall sensitivity largely depends on the coating length and extraction time, both parameters must be as small as possible to ensure that the method is minimally invasive and disturbs the subject as little as possible. For that reason, the authors of the above study selected probes with a 7 mm coating for use in subsequent experiments. Another practical aspect discussed in [40] was the option of using needle-assembled fibers, which enable penetration through harder tissues such as muscles or barriers (e.g., pleura). Although this approach is slightly more invasive, it is still less so than a regular biopsy, while continuing to allow for sampling with no physical tissue consumption. The extraction coverage results showed that the proposed method provided coverage ranging from 239 molecular features in negative ionization mode for lung sampling to 1580 in positive ionization mode for liver samples, thus confirming the excellent efficiency reported previously for SPME. As emphasized in previous metabolomics studies using SPME, the number and range of the metabolites extracted via SPME is lower compared to conventional sample preparation methods based on tissue collection, homogenization, and multi-solvent extraction, because SPME is an equilibrium technique that extracts via free fraction of metabolites. Thus, only metabolites present in their free form are available for extraction. This feature can be either an advantage or a disadvantage depending on the biological information the researcher wants to obtain from their study. If the main goal is to identify the active molecules involved in a given mechanism, then SPME is a good choice; however, if the objective is to characterize all molecules in the studied system independently based on their biological activity, then more conventional strategies should be considered. The optimized protocol described in [40] was subsequently used in pilot studies conducted on liver and lungs, wherein sampling times of 20 and 30 min were used, respectively [41]. Similar to the previously described studies on ROC and TXA [37], these studies showed that monitoring drugs routinely used during the transplantation procedure may shed light on changes in liver function. The authors found that methylprednisolone was only present in non-ischemic organs, while no drug metabolites were detected in livers subjected to 38 and 78 min of warm ischemia time (WIT), thus suggesting impaired organ function. This hypothesis was supported by observed alterations in endogenous compounds from the Krebs, pentose cycles, and TCA pathway. The metabolic profiling of lungs at different stages of their transplantation procedure (i.e., CIT, ex vivo perfusion (EVLP) and after revascularization) revealed clear differences between the subsequent groups of samples and enabled the tentative identification of metabolites that have been up- and down-regulated under different conditions and factors. In addition to organ sampling, the authors proposed monitoring metabolites in perfusate circulating throughout the graft in a closed circuit as a non-invasive approach for monitoring graft function during perfusion. In addition, this experiment bypassed the need for sample withdrawal, as extraction was performed by exposing the SPME needle-assembled fibers to the perfusate by inserting them into the three-way stopcock—which was equipped with a Luer-lock connected to the perfusate line—for 2 min. In this study, all sampling was conducted in triplicate. Unsupervised analysis of the data showed clustering of the samples at different perfusion time points, indicating the occurrence of alterations in the studied organs, mainly involving amino acids, fatty acids, and their derivatives.
Stryjak et al. conducted a proof-of-concept study to demonstrate this technology’s suitability for characterizing changes during the cold preservation of kidneys [42]. Specifically, Stryjak et al. assessed how prolonged ischemia and the accompanying oxidative stress affected the condition of kidneys subjected to static cold storage using a rabbit model. Extraction was performed by inserting duplicate SPME probes (4 mm length mixed-mode extraction phase) into each kidney cortex for 30 min at 5 different time points: immediately following the removal of kidneys, and after 2, 4, 6, and 21 h of cold preservation. The results revealed a significant change in the metabolic profile of the kidney over the first 4 h of storage. The most pronounced alterations were observed in the levels of essential amino acids, which changed depending on exposure to the ischemic milieu, and purine nucleosides, which are associated with various metabolic pathways involved in the production of reactive oxygen species (ROS). Among the identified metabolites, the presence of adenosine and adenosine monophosphate was notable, as this indicated the adenosine-dependent nature of the mechanisms underlying preconditioning and protection against renal ischemia. Other notable identified metabolites also included inosine, hypoxanthine, and xanthine. Furthermore, the short half-life of some of the identified metabolites highlights this analytical approach’s usefulness for capturing unstable and short-lived compounds. Moreover, Stryjak et al. extended the existing protocol for use in lipidomic studies and optimized it for in vivo studies on a porcine model and in human subjects [43]. Since biological applications necessitate a compromise between the method’s sensitivity and repeatability and the restrictions inherent to medical procedures, it is necessary to determine the optimal extraction phase length and extraction time. Although equilibrium extraction provides the highest sensitivity, the authors decided to use pre-equilibrium conditions for safety reasons, as this would avoid affecting the operation’s total duration. The findings confirmed that a 10-min extraction using probes coated with 7 mm of mix-mode (MM) sorbent provided sufficient sensitivity for a broad spectrum of metabolites, enabling the effective profiling of the renal cortex during ex vivo kidney perfusion, in vivo prior to organ harvest, and in vivo after revascularization. The developed protocol used 100 µL of desorption solutions consisting of ACN:H2O (80:20, v:v) and IPA:MeOH (50:50) for the metabolomic and lipidomic analyses, respectively. The SPME method’s potential for evaluating kidney quality during the transplantation procedure was demonstrated in a pig autotransplantation model, with particular emphasis on HBD and DCD donors [44]. For both donor types, extractions were performed in vivo prior to retrieval; after 1 h, 3 h, 5 h, and 7 h of perfusion; and again in vivo immediately after revascularization. Additionally, the DCD kidneys were also sampled after 45 min and 2 h of warm ischemia. Direct tissue sampling was carried out for 30 min using probes coated with 7 mm of MM extraction phase. The utilized metabolomic and lipidomic platforms enabled the identification of a set of metabolites that may have diagnostic value in monitoring organ function before transplantation. The metabolomic data revealed changes in purine levels between the HBD and DCD groups. The accumulation of adenosine observed during perfusion in the HBD group may be associated with its protective effects against ischemia-reperfusion injury IRI, while the reduced levels of inosine observed during reperfusion in the DCD group may be associated with a worse prognosis after transplantation. In addition, changes in the levels of certain amino acids were found to be correlated with the organ’s warm ischemia duration. For instance, increased levels of alanine and valine are associated with impaired organ function, can be a sensitive discriminator of ischemia, and may lead to less favourable outcomes. On the other hand, the decrease in histidine concentrations during WIT may have resulted from ongoing inflammatory processes and the development of oxidative stress. The lipidomic portion of the work revealed differences in LPC levels between the HBD and DCD organs and an upward trend in the level of these metabolites during WIT. Although the exact mechanisms governing the effects of LPC on the graft remain unclear, this group of lipids may be associated with increased oxidative stress, increased inflammatory responses, and the remodelling of cell membranes. Furthermore, the decreased PC/PE ratio in the DCD organs during reperfusion may be associated with impaired liver regeneration, alterations in energy metabolism, increased cell leakage, and endoplasmic reticulum stress. This research was continued by Warmuzińska et al., who used an SPME chemical biopsy to compare the effects of SCS, normothermic ex vivo kidney perfusion (NEVKP), and hypothermic machine perfusion (HMP) on the lipidomic profile of a graft in a renal DCD autotransplantation porcine model [45]. Similar to Stryjak et al.’s study, 7 mm length MM fibre probes were employed to perform 30 min direct extractions from the kidney cortex. The samples were harvested in vivo before retrieval; after 1 h and 2 h of warm ischemia; after 1 h, 3 h, 5 h, and 7 h of perfusion; in vivo immediately after reperfusion; and in vivo under deep anesthesia at the time of sacrifice on postoperative day 3. The findings indicated that the preservation temperature had a more significant impact on the lipidomic profile than the mechanical character of perfusion. Higher levels of CARs, PCs and PEs (including ether-linked), PIs, TGs, most LPCs, and LPEs were observed in the hypothermic preservation group, which may be related to IRI, mitochondrial dysfunction, and oxidative stress. The obtained results also revealed that the NEKVP method may have a beneficial effect on graft function. Specifically, NEKVP-perfused kidneys showed lower accumulation of pro-inflammatory lipids, which contributes to improved graft function after perfusion compared to hypothermic preservation methods.
In one of the most recent studies on this topic, SPME was applied to sample myocardium during prolonged ex situ heart perfusion (ESHP) [5]. In this work, a porcine model was used for protocol development and exploratory analysis, while two explanted human hearts that had been declined for transplantation and used for scientific purposes were treated as validatory grafts. In the porcine model, sampling was conducted at various in vivo and ex vivo stages (i.e., heart beating before harvesting the organ and during perfusion, respectively). The human hearts were only monitored during the ESHP procedure. The untargeted screening covered both the polar metabolome and the lipidome, thereby offering a comprehensive insight into the molecular changes taking place within the examined organs. From a biological perspective, increased metabolite dysregulation in response to prolonged organ preservation indicated the presence of inflammatory processes, the progression of mitochondrial oxidative stress, the disturbance of mitochondrial bioenergetics, and the dysregulation of many lipids, with increases in the level of species negatively impacting the tissue. An especially interesting component of the study was the authors’ comparison of the results obtained with SPME and those obtained via solid-liquid extraction (SLE) performed on biopsies collected from the same hearts that had been sampled with SPME probes. The results confirmed that SLE enables more comprehensive analyte coverage, particularly with respect to lipid species that are integrated components of cell membranes, and that are not present in free form or are present at concentrations that are too low to be detected by SPME. In contrast to SLE, SPME proved to be more effective in detecting unstable and intermediate compounds and in offering better sample clean-up, which enabled the detection of low abundance species and a greater variety of lipid subclasses. In SLE, sample homogenization followed by solvent extraction releases and dissolves compounds bound to macromolecules located in different organelles and fractions of the cells and tissues, thus providing higher sensitivity; however, this improved sensitivity comes at the cost of compromised extract clean-up and the production of matrix effects.
4. Conclusions
This review’s up-to-date survey of SPME-based studies focusing on graft monitoring in the peri-transplant period demonstrates this technology’s profound potential for use in the diagnostic process. The ability to process different biofluid samples regardless of their complexity can be effectively exploited to monitor the state of the graft after surgery when access to the organ is very limited or impossible. On the other hand, the minimally invasive nature of SPME fibres creates the unique opportunity to directly monitor biochemical changes occurring in the graft over the entire period of transplantation (i.e., “from donor to recipient”). Furthermore, untargeted studies, particularly on well-controlled animal models, can lead to a better understanding of the mechanisms underlying organ injury and rejection, in addition to identifying metabolites with potential diagnostic value. Considering the fact that SPME devices have been directly coupled with stand-alone instruments (e.g., mass spectrometers) in numerous studies, it can be envisioned that such strategies can be used for determination of discovered biomarkers. Given SPME’s short sample preparation time and ability to perform on-site extractions without the need for sample consumption, combined with its ability to provide the rapid, quantitative, and sensitive determination of target analytes, the use of this technology to obtain results in close to real time appears to be an attainable goal.
Author Contributions
Writing—original draft preparation, K.Ł., N.W. and B.B.; writing—review and editing, K.Ł., N.W. and B.B.; funding acquisition, B.B. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by National Science Center 2017/27/B/NZ5/01013.
Data Availability Statement
Not appliable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kvietkauskas, M.; Zitkute, V.; Leber, B.; Strupas, K.; Stiegler, P.; Schemmer, P. The Role of Metabolomics in Current Concepts of Organ Preservation. Int. J. Mol. Sci. 2020, 21, 6607. [Google Scholar] [CrossRef] [PubMed]
- Warmuzińska, N.; Łuczykowski, K.; Bojko, B. A Review of Current and Emerging Trends in Donor Graft-Quality Assessment Techniques. J. Clin. Med. 2022, 11, 487. [Google Scholar] [CrossRef] [PubMed]
- Bruinsma, B.G.; Sridharan, G.V.; Weeder, P.D.; Avruch, J.H.; Saeidi, N.; Özer, S.; Geerts, S.; Porte, R.J.; Heger, M.; Van Gulik, T.M.; et al. Metabolic Profiling during Ex Vivo Machine Perfusion of the Human Liver. Sci. Rep. 2016, 6, 22415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Looby, N.; Roszkowska, A.; Ali, A.; Bojko, B.; Cypel, M.; Pawliszyn, J. Metabolomic Fingerprinting of Porcine Lung Tissue during Pre-Clinical Prolonged Ex Vivo Lung Perfusion Using in Vivo SPME Coupled with LC-HRMS. J. Pharm. Anal. 2022, 12, 590–600. [Google Scholar] [CrossRef] [PubMed]
- Olkowicz, M.; Ribeiro, R.V.P.; Yu, F.; Alvarez, J.S.; Xin, L.; Yu, M.; Rosales, R.; Adamson, M.B.; Bissoondath, V.; Smolenski, R.T.; et al. Dynamic Metabolic Changes During Prolonged Ex Situ Heart Perfusion Are Associated With Myocardial Functional Decline. Front. Immunol. 2022, 13, 859506. [Google Scholar] [CrossRef]
- Mihaylov, P.; Mangus, R.; Ekser, B.; Cabrales, A.; Timsina, L.; Fridell, J.; Lacerda, M.; Ghabril, M.; Nephew, L.; Chalasani, N.; et al. Expanding the Donor Pool With the Use of Extended Criteria Donation After Circulatory Death Livers. Liver Transplant. 2019, 25, 1198–1208. [Google Scholar] [CrossRef]
- Beuth, J.; Falter, F.; Pinto Ribeiro, R.V.; Badiwala, M.; Meineri, M. New Strategies to Expand and Optimize Heart Donor Pool: Ex Vivo Heart Perfusion and Donation after Circulatory Death: A Review of Current Research and Future Trends. Anesth. Analg. 2019, 128, 406–413. [Google Scholar] [CrossRef]
- Ravaioli, M.; Maroni, L.; Angeletti, A.; Fallani, G.; De Pace, V.; Germinario, G.; Odaldi, F.; Corradetti, V.; Caraceni, P.; Baldassarre, M.; et al. Hypothermic Oxygenated Perfusion versus Static Cold Storage for Expanded Criteria Donors in Liver and Kidney Transplantation: Protocol for a Single-Center Randomized Controlled Trial. JMIR Res. Protoc. 2020, 9, e13922. [Google Scholar] [CrossRef] [Green Version]
- McGuinness, D.; Mohammed, S.; Monaghan, L.; Wilson, P.A.; Kingsmore, D.B.; Shapter, O.; Stevenson, K.S.; Coley, S.M.; Devey, L.; Kirkpatrick, R.B.; et al. A Molecular Signature for Delayed Graft Function. Aging Cell 2018, 17, e12825. [Google Scholar] [CrossRef]
- Kurosaki, T.; Miyoshi, K.; Otani, S.; Imanishi, K.; Sugimoto, S.; Yamane, M.; Kobayashi, M.; Toyooka, S.; Oto, T. Low-Risk Donor Lungs Optimize the Post-Lung Transplant Outcome for High Lung Allocation Score Patients. Surg. Today 2018, 48, 928–935. [Google Scholar] [CrossRef] [Green Version]
- D’Errico, A.; Riefolo, M.; Serenari, M.; De Pace, V.; Santandrea, G.; Monica, M.; de Cillia, C.; Ravaioli, M.; Cescon, M.; Vasuri, F. The Histological Assessment of Liver Fibrosis in Grafts from Extended Criteria Donors Predicts the Outcome after Liver Transplantation: A Retrospective Study. Dig. Liver Dis. 2020, 52, 185–189. [Google Scholar] [CrossRef]
- Dare, A.J.; Pettigrew, G.J.; Saeb-Parsy, K. Preoperative Assessment of the Deceased-Donor Kidney: From Macroscopic Appearance to Molecular Biomarkers. Transplantation 2014, 97, 797–807. [Google Scholar] [CrossRef]
- Moeckli, B.; Sun, P.; Lazeyras, F.; Morel, P.; Moll, S.; Pascual, M.; Bühler, L.H. Evaluation of Donor Kidneys Prior to Transplantation: An Update of Current and Emerging Methods. Transpl. Int. 2019, 32, 459–469. [Google Scholar] [CrossRef]
- Kransdorf, E.P.; Stehlik, J. Donor Evaluation in Heart Transplantation: The End of the Beginning. J. Heart Lung Transplant. 2014, 33, 1105–1113. [Google Scholar] [CrossRef]
- Courtwright, A.; Cantu, E. Evaluation and Management of the Potential Lung Donor. Clin. Chest Med. 2017, 38, 751–759. [Google Scholar] [CrossRef]
- Azancot, M.A.; Moreso, F.; Salcedo, M.; Cantarell, C.; Perello, M.; Torres, I.B.; Montero, A.; Trilla, E.; Sellarés, J.; Morote, J.; et al. The Reproducibility and Predictive Value on Outcome of Renal Biopsies from Expanded Criteria Donors. Kidney Int. 2014, 85, 1161–1168. [Google Scholar] [CrossRef] [Green Version]
- Scheuermann, U.; Truong, T.; Seyferth, E.R.; Freischlag, K.; Gao, Q.; Yerxa, J.; Ezekian, B.; Davis, R.P.; Schroder, P.M.; Peskoe, S.B.; et al. Kidney Donor Profile Index Is a Reliable Alternative to Liver Donor Risk Index in Quantifying Graft Quality in Liver Transplantation. Transplant. Direct 2019, 5, e511. [Google Scholar] [CrossRef]
- Jun, H.; Yoon, H.E.; Lee, K.W.; Lee, D.R.; Yang, J.; Ahn, C.; Han, S.Y. Kidney Donor Risk Index Score Is More Reliable Than Kidney Donor Profile Index in Kidney Transplantation From Elderly Deceased Donors. Transplant. Proc. 2020, 52, 1744–1748. [Google Scholar] [CrossRef]
- Parker, W.F.; Thistlethwaite Jr, J.R.; Ross, L.F. Kidney Donor Profile Index (KDPI) Does Not Accurately Predict the Graft Survival of Pediatric Deceased Donor Kidneys. Transplantation 2016, 100, 2471–2478. [Google Scholar] [CrossRef] [Green Version]
- Verhoeven, C.J.; Farid, W.R.R.; De Jonge, J.; Metselaar, H.J.; Kazemier, G.; Van Der Laan, L.J.W. Biomarkers to Assess Graft Quality during Conventional and Machine Preservation in Liver Transplantation. J. Hepatol. 2014, 61, 672–684. [Google Scholar] [CrossRef] [Green Version]
- Cypel, M.; Keshavjee, S. Extending the Donor Pool: Rehabilitation of Poor Organs. Thorac. Surg. Clin. 2015, 25, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Ravaioli, M.; De Pace, V.; Angeletti, A.; Comai, G.; Vasuri, F.; Baldassarre, M.; Maroni, L.; Odaldi, F.; Fallani, G.; Caraceni, P.; et al. Hypothermic Oxygenated New Machine Perfusion System in Liver and Kidney Transplantation of Extended Criteria Donors:First Italian Clinical Trial. Sci. Rep. 2020, 10, 6063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Queiroz, M.E.C.; Souza, I.D.d.; Oliveira, I.G.d.; Grecco, C.F. In Vivo Solid Phase Microextraction for Bioanalysis. TrAC-Trends Anal. Chem. 2022, 153, 116656. [Google Scholar] [CrossRef]
- Ji, X. Applications of Headspace Solid-Phase Microextraction in Human Biological Matrix Analysis. Rev. Anal. Chem. 2022, 41, 180–188. [Google Scholar] [CrossRef]
- Hemmati, M.; Nix, C.; Crommen, J.; Servais, A.C.; Fillet, M. Benefits of Microsampling and Microextraction for Metabolomics Studies. TrAC-Trends Anal. Chem. 2020, 127, 115899. [Google Scholar] [CrossRef]
- Riboni, N.; Fornari, F.; Bianchi, F.; Careri, M. Recent Advances in in Vivo Spme Sampling. Separations 2020, 7, 6. [Google Scholar] [CrossRef] [Green Version]
- Filipiak, W.; Bojko, B. SPME in Clinical, Pharmaceutical, and Biotechnological Research–How Far Are We from Daily Practice? Trends Anal. Chem. 2019, 115, 203–213. [Google Scholar] [CrossRef]
- Reyes-Garcés, N.; Gionfriddo, E. Recent Developments and Applications of Solid Phase Microextraction as a Sample Preparation Approach for Mass-Spectrometry-Based Metabolomics and Lipidomics. TrAC-Trends Anal. Chem. 2019, 113, 172–181. [Google Scholar] [CrossRef]
- Godage, N.H.; Gionfriddo, E. A Critical Outlook on Recent Developments and Applications of Matrix Compatible Coatings for Solid Phase Microextraction. TrAC-Trends Anal. Chem. 2019, 111, 220–228. [Google Scholar] [CrossRef]
- Roszkowska, A.; Miękus, N.; Bączek, T. Application of Solid-Phase Microextraction in Current Biomedical Research. J. Sep. Sci. 2019, 42, 285–302. [Google Scholar] [CrossRef] [Green Version]
- Bojko, B. Solid-Phase Microextraction: A Fit-for-Purpose Technique in Biomedical Analysis. Anal. Bioanal. Chem. 2022, 414, 7005–7013. [Google Scholar] [CrossRef]
- Bojko, B.; Looby, N.; Olkowicz, M.; Roszkowska, A.; Kupcewicz, B.; Reck dos Santos, P.; Ramadan, K.; Keshavjee, S.; Waddell, T.K.; Gómez-Ríos, G.; et al. Solid Phase Microextraction Chemical Biopsy Tool for Monitoring of Doxorubicin Residue during in Vivo Lung Chemo-Perfusion. J. Pharm. Anal. 2021, 11, 37–47. [Google Scholar] [CrossRef]
- Thirukumaran, M.; Singh, V.; Arao, Y.; Fujito, Y.; Nishimura, M.; Ogura, T.; Pawliszyn, J. Solid-Phase Microextraction- Probe Electrospray Ionization Devices for Screening and Quantitating Drugs of Abuse in Small Amounts of Biofluids. Talanta 2021, 231, 122317. [Google Scholar] [CrossRef]
- Lendor, S.; Olkowicz, M.; Boyaci, E.; Yu, M.; Diwan, M.; Hamani, C.; Palmer, M.; Reyes-Garcés, N.; Gómez-Ríos, G.A.; Pawliszyn, J. Investigation of Early Death-Induced Changes in Rat Brain by Solid Phase Microextraction via Untargeted High Resolution Mass Spectrometry: In Vivo versus Postmortem Comparative Study. ACS Chem. Neurosci. 2020, 11, 1827–1840. [Google Scholar] [CrossRef]
- Bessonneau, V.; Bojko, B.; Azad, A.; Keshavjee, S.; Azad, S.; Pawliszyn, J. Determination of Bronchoalveolar Lavage Bile Acids by Solid Phase Microextraction Liquid Chromatography-Tandem Mass Spectrometry in Combination with Metabolite Profiling: Comparison with Enzymatic Assay. J. Chromatogr. A 2014, 1367, 33–38. [Google Scholar] [CrossRef]
- Stefanuto, P.H.; Romano, R.; Rees, C.A.; Nasir, M.; Thakuria, L.; Simon, A.; Reed, A.K.; Marczin, N.; Hill, J.E. Volatile Organic Compound Profiling to Explore Primary Graft Dysfunction after Lung Transplantation. Sci. Rep. 2022, 12, 2053. [Google Scholar] [CrossRef]
- Yang, Q.J.; Kluger, M.; Goryński, K.; Pawliszyn, J.; Bojko, B.; Yu, A.-M.; Noh, K.; Selzner, M.; Jerath, A.; McCluskey, S.; et al. Comparing Early Liver Graft Function from Heart Beating and Living-Donors: A Pilot Study Aiming to Identify New Biomarkers of Liver Injury. Biopharm. Drug Dis. 2017, 38, 326–339. [Google Scholar] [CrossRef]
- Łuczykowski, K.; Warmuzińska, N.; Kollmann, D.; Selzner, M.; Bojko, B. Biliary Metabolome Profiling for Evaluation of Liver Metabolism and Biliary Tract Function Related to Organ Preservation Method and Degree of Ischemia in a Porcine Model. Int. J. Mol. Sci. 2023, 24, 2127. [Google Scholar] [CrossRef]
- Łuczykowski, K.; Warmuzińska, N.; Stryjak, I.; Kollmann, D.; Selzner, M.; Bojko, B. Analysis of Changes in Bile Acids Concentration in Bile in Response to the Degree of Liver Ischemia and the Method of Organ Preservation. Mass Spectrom. Advences Clin. Lab. 2019. Available online: https://www.msacl.org/program/view_abstract_selection.php?id=1146&event=2019%20EU (accessed on 28 December 2022).
- Bojko, B.; Gorynski, K.; Gomez-Rios, G.A.; Knaak, J.M.; Machuca, T.; Spetzler, V.N.; Cudjoe, E.; Hsin, M.; Cypel, M.; Selzner, M.; et al. Solid Phase Microextraction Fills the Gap in Tissue Sampling Protocols. Anal. Chim. Acta 2013, 803, 75–81. [Google Scholar] [CrossRef]
- Bojko, B.; Gorynski, K.; Gomez-Rios, G.A.; Knaak, J.M.; Machuca, T.; Cudjoe, E.; Spetzler, V.N.; Hsin, M.; Cypel, M.; Selzner, M.; et al. Low Invasive in Vivo Tissue Sampling for Monitoring Biomarkers and Drugs during Surgery. Lab. Investig. 2014, 94, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Stryjak, I.; Warmuzińska, N.; Bogusiewicz, J.; Łuczykowski, K.; Bojko, B. Monitoring of the Influence of Long-Term Oxidative Stress and Ischemia on the Condition of Kidneys Using Solid-Phase Microextraction Chemical Biopsy Coupled with Liquid Chromatography–High-Resolution Mass Spectrometry. J. Sep. Sci. 2020, 43, 1867–1878. [Google Scholar] [CrossRef] [PubMed]
- Stryjak, I.; Warmuzińska, N.; Łuczykowski, K.; Hamar, M.; Urbanellis, P.; Wojtal, E.; Masztalerz, M.; Selzner, M.; Włodarczyk, Z.; Bojko, B. Using a Chemical Biopsy for Graft Quality Assessment. J. Vis. Exp. 2020, 2020, 1–12. [Google Scholar] [CrossRef]
- Stryjak, I.; Warmuzińska, N.; Łuczykowski, K.; Urbanellis, P.; Selzner, M.; Bojko, B. Metabolomic and Lipidomic Landscape of Porcine Kidney Associated with Kidney Perfusion in Heart Beating Donors and Donors after Cardiac Death. Sci. Rep. 2022. [Google Scholar] [CrossRef]
- Warmuzińska, N.; Stryjak, I.; Łuczykowski, K.; Hamar, M.; Urbanellis, P.; Selzner, M.; Bojko, B. Low Invasive SPME Tissue Sampling As A New Tool For Graft Quality Assessment. Eur. Soc. Organ Transplant. Congr. 2021, 316, F1714–F1719. [Google Scholar] [CrossRef]
- Gorynski, K.; Bojko, B.; Kluger, M.; Jerath, A.; Wasowicz, M.; Pawliszyn, J. Development of SPME Method for Concomitant Sample Preparation of Rocuronium Bromide and Tranexamic Acid in Plasma. J. Pharm. Biomed. Anal. 2014, 92, 183–192. [Google Scholar] [CrossRef]
Figure 1.
The number of articles that include SPME as a sample preparation method. Numbers are based on PubMed searching for “SPME” or “solid-phase microextraction” in titles and/or abstracts.
Figure 1.
The number of articles that include SPME as a sample preparation method. Numbers are based on PubMed searching for “SPME” or “solid-phase microextraction” in titles and/or abstracts.

Figure 2.
Exemplary application of solid-phase microextraction in solid organ transplantation. Details are discussed in the text.
Figure 2.
Exemplary application of solid-phase microextraction in solid organ transplantation. Details are discussed in the text.

Figure 3.
Ratio of the normalized areas of the 20 selected features. Reprinted from [36] with permission under a Creative Commons Attribution 4.0 International License.
Figure 3.
Ratio of the normalized areas of the 20 selected features. Reprinted from [36] with permission under a Creative Commons Attribution 4.0 International License.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Applications of solid-phase microextraction in solid organ transplantation.
| Monitored Organ | Biological Specimen | Sampling Mode (Ex Vivo/In Vivo; Head-Space/Direct Immersion HS/DI) | Device Geometry and Coating Chemistry | Target Analyte | Comments | Reference |
|---|---|---|---|---|---|---|
| lung | bronchoalveolar lavage fluid (BALF) (human) | ex vivo; DI | TFME, PAN-C18 | cholic acid (CA), deoxycholic acid (DCA) |
| [35] |
| lung | bronchoalveolar lavage fluid (BALF) (human) | ex vivo; DI | fiber, mix-mode | untargeted profiling |
| [35] |
| lung | bronchoalveolar lavage fluid BALF and blind bronchial aspirate (BBA) (human) | ex vivo; HS | fiber, DVB/CAR/PDMS | untargeted profiling |
| [36] |
| liver | plasma (human) | ex vivo; DI | TFME, PAN-WCX | rocuronium bromide (ROC), tranexamic acid (TXA) |
| [37] |
| liver | plasma (human) | ex vivo; DI | TFME, HLB | untargeted profiling |
| [37] |
| liver | bile (pig) | ex vivo; DI | TFME, HLB | untargeted profiling |
| [38] |
| liver | bile (pig) | ex vivo; DI | TFME, C18 | glycocholic acid (GCA), taurocholic acid (TCA), glycochenodeoxycholic acid (GCDCA), taurolithocholic acid (TLCA), glycoursodeoxycolic acid (GUDCA), tauroursodeoxycholic acid (TDCA), glycodeoxycholic acid (GDCA), cholic acid (CA), chenodeoxycholic acid (CDCA), deoxycholic acid (DCA), hyocholic acid (HCA), taurochenodeoxycholic acid (TCDCA), ursodeoxycholic acid (UDCA) |
| [39] |
| lung; liver | tissue (pig) | ex vivo, in vivo; DI | fiber, mix-mode | untargeted profiling |
| [40] |
| lung; liver | tissue (pig) | ex vivo, in vivo; DI | fiber, mix-mode | methylprednisolone (MP) |
| [41] |
| lung; liver | tissue (pig), perfusate | ex vivo, in vivo; DI | fiber, mix-mode | untargeted profiling |
| [41] |
| kidney | tissue (rabbit) | ex vivo; DI | fiber, mix-mode | untargeted profiling |
| [42] |
| kidney | tissue (pig, human) | ex vivo, in vivo; DI | fiber, mix-mode | untargeted profiling |
| [43] |
| kidney | tissue (pig) | ex vivo, in vivo; DI | fiber, mix-mode | untargeted profiling |
| [44] |
| kidney | tissue (pig) | ex vivo, in vivo; DI | fiber, mix-mode | untargeted profiling |
| [45] |
| heart | tissue (pig), perfusate | ex vivo, in vivo; DI | fiber, mix-mode, C18, HLB | untargeted profiling |
| [5] |
| heart | tissue (human), perfusate | ex vivo; DI | fiber, mix-mode, C18 | untargeted profiling |
| [5] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Łuczykowski, K.; Warmuzińska, N.; Bojko, B. Solid Phase Microextraction—A Promising Tool for Graft Quality Monitoring in Solid Organ Transplantation. Separations 2023, 10, 153. https://doi.org/10.3390/separations10030153
AMA Style
Łuczykowski K, Warmuzińska N, Bojko B. Solid Phase Microextraction—A Promising Tool for Graft Quality Monitoring in Solid Organ Transplantation. Separations. 2023; 10(3):153. https://doi.org/10.3390/separations10030153
Chicago/Turabian StyleŁuczykowski, Kamil, Natalia Warmuzińska, and Barbara Bojko. 2023. "Solid Phase Microextraction—A Promising Tool for Graft Quality Monitoring in Solid Organ Transplantation" Separations 10, no. 3: 153. https://doi.org/10.3390/separations10030153
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.