
Biosynthesis of Salbutamol-4′-O-sulfate as Reference for Identification of Intake Routes and Enantiopure Salbutamol Administration by Achiral UHPLC-MS/MS


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
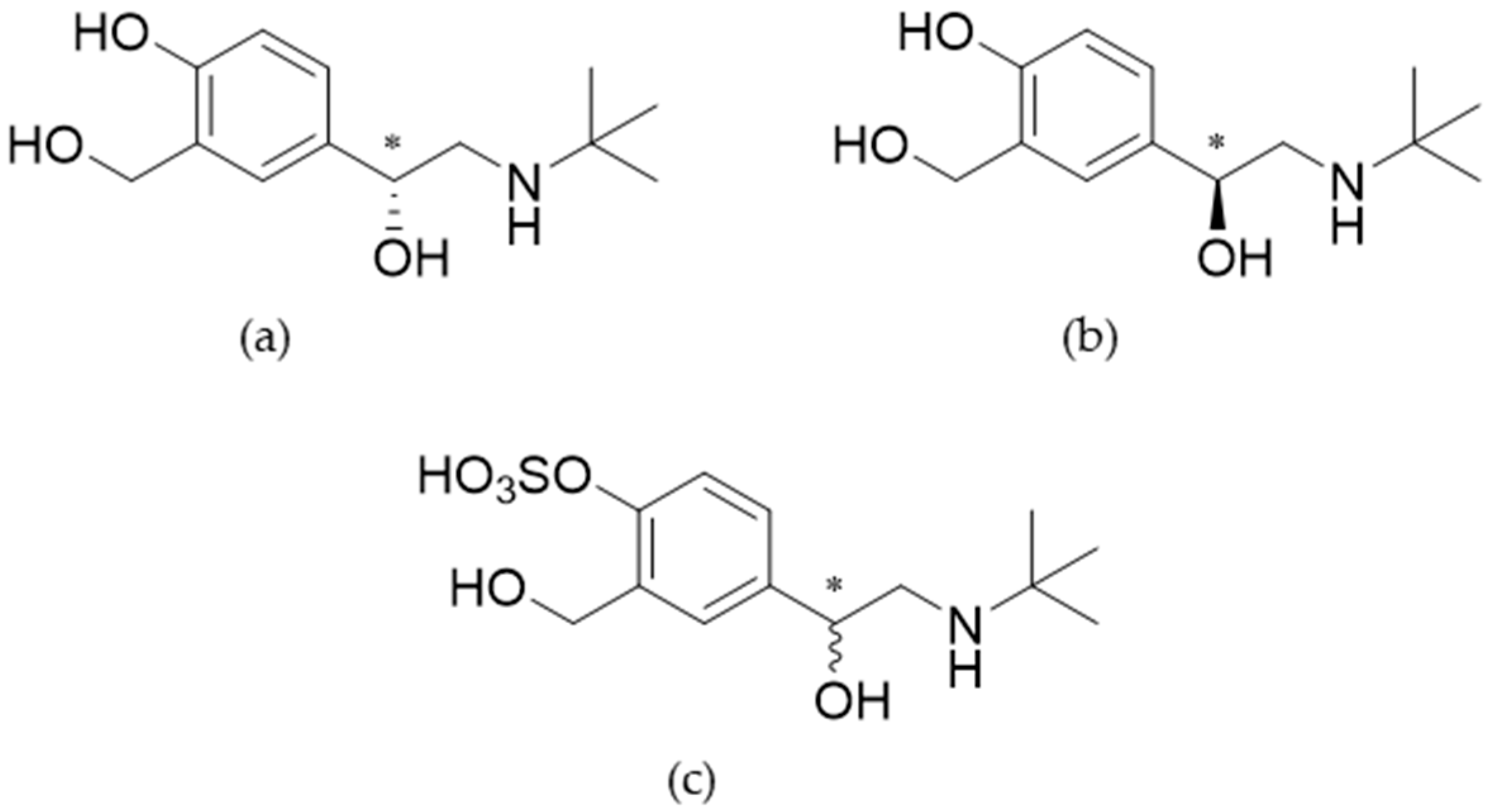
2.2. Synthesis of Salbutamol-4′-O-sulfate as Reference
2.3. Characterization of Salbutamol-4′-O-sulfate
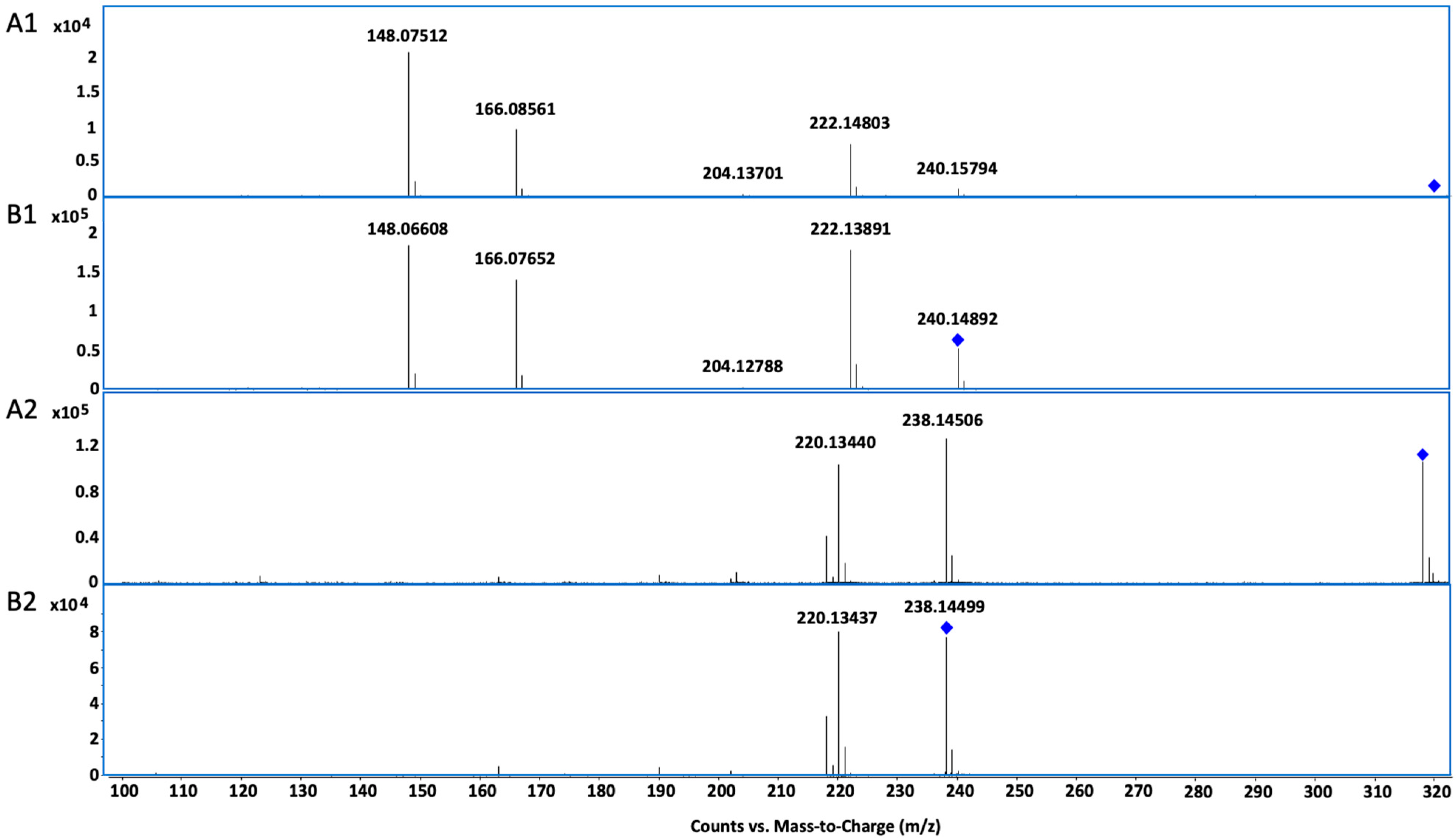
2.3.1. UHPLC-QTOF-MS
2.3.2. Nuclear Magnetic Resonance
2.4. Proof of Concept: Longitudinal Case Study and Urine Analysis
2.4.1. Study Design
2.4.2. Matrix Assisted Calibration
2.4.3. Sample Preparation
2.4.4. Specific Gravity of Urine Samples
2.4.5. Instruments and Chromatographic Conditions for Urine Analysis
2.4.6. Method Characterization
2.5. Data Analysis
3. Results
3.1. Biosynthesis and Characterization of Reference by UHPLC-QTOF-MS and NMR
3.2. Metabolite Identification in Urine Samples
3.3. UHPLC-QQQ-MS/MS Method Characterization
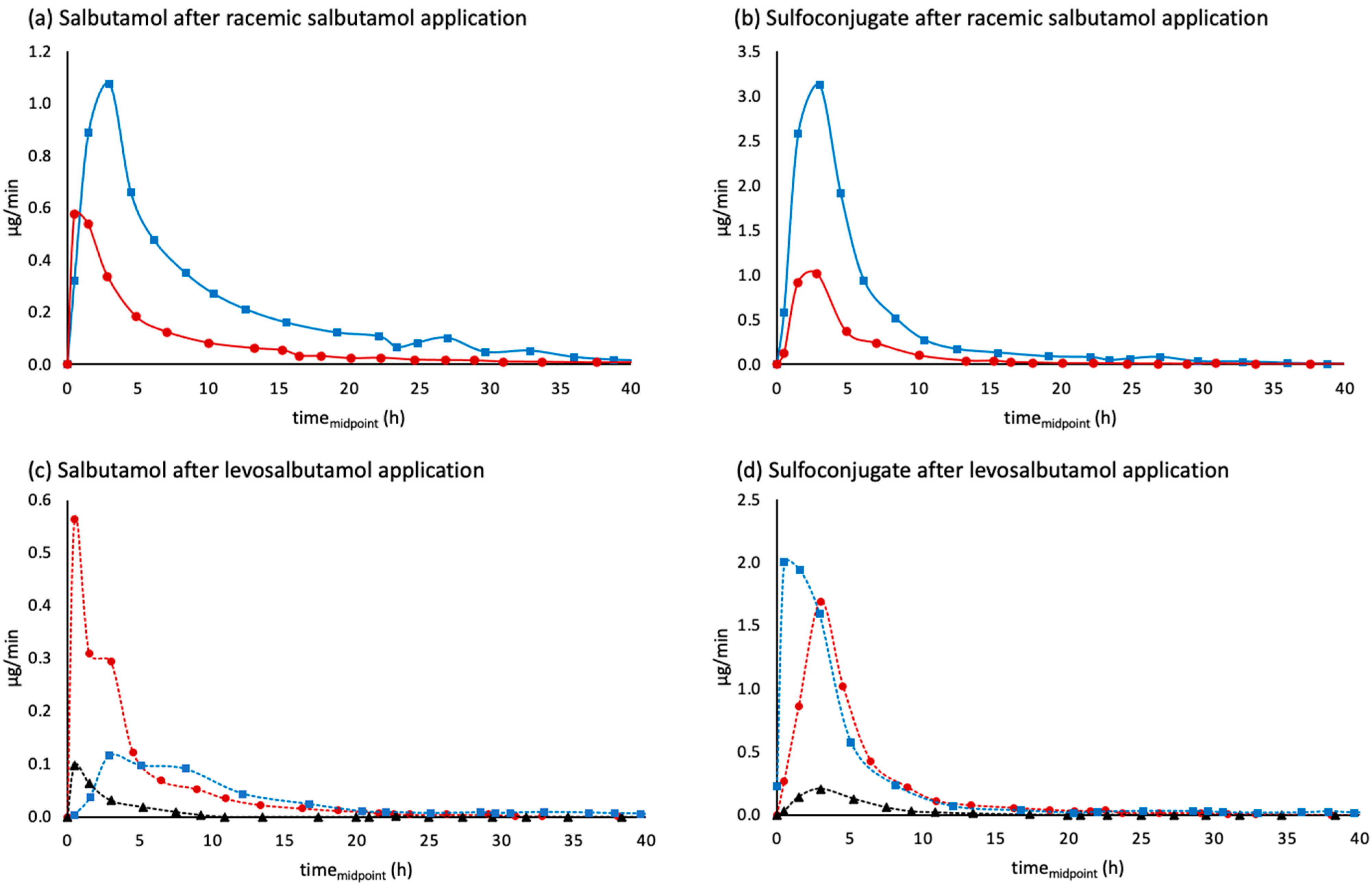
3.4. Evaluation of Urinary Excretion Profiles
3.4.1. Inhalation of Salbutamol through Dry Powder Inhaler vs. Metered Dose Inhaler
3.4.2. Urinary Excretion Rates
3.4.3. Proportions of Salbutamol and Salbutamol-4′-O-sulfate
3.4.4. Salbutamol-4′-O-sulfate in Relation to Unchanged Salbutamol
3.4.5. Adjustment by the Specific Gravity of the Urine and by Urinary Flow Rate
4. Discussion
4.1. Biosynthesis and Characterization of Salbutamol-4′-O-sulfate
4.2. Basic Method Validation
4.3. Proof of Concept: Achiral Analysis of Urinary Excreted Salbutamol and Salbutamol-4′-O-sulfate for Discrimination of Application Routes and Enantiomeric Composition of the Administered Drug
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Purification of Biosynthesized Salbutamol-4′-O-sulfate

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gravity Column Purification | HPLC Purification | |
|---|---|---|
| Sample preparation | Dissolving dried remains in methanol, filtration | Evaporation of fractions containing product to reduce sample volume Filtration of silica remains |
| Stationary phase | Silica | C18 |
| Column length | 40 cm | 25 cm |
| Column diameter | 3.5 cm | 1 cm |
| Particle size | n.a. | 5 µm |
| Flow rate | n.a. | 2.5 mL/min |
| Mobile phase | Isopropanol:ethyl acetate:ammonia (17.5%) 40:50:10 (V:V:V) | A: water B: acetonitrile 0–5 min: 3% B to 15% B 5–6.5 min: 15% B 6.5–16 min: 15% B to 27% B 16–20 min: 27% B to 45% B 20–22 min: 45% B to 95% B 25–27 min: 95% B to 3% B |
| Detection of product | Fraction analysis with LC-MS | UV detection 265 nm |
Appendix A.2. Inhalation of Salbutamol through Dry Powder Inhaler vs. Metered Dose Inhaler
| DPI 1 | MDI 2 | MDI 2_2 | |
|---|---|---|---|
| Percentage of dose recovered in urine 3 | 80% | 115% | 83% |
| Proportion of parent compound 4 | 42% | 46% | 41% |
| Proportion of salbutamol-4′-O-sulfate 4 | 58% | 54% | 59% |
Appendix A.3. Appendix Figures


References
- Boulton, D.W.; Fawcett, J.P. The pharmacokinetics of levosalbutamol: What are the clinical implications? Clin. Pharmacokinet. 2001, 40, 23–40. [Google Scholar] [CrossRef]
- World Anti-Doping Agency. WADA Prohibited List 2022. Available online: https://www.wada-ama.org/sites/default/files/resources/files/2022list_final_en.pdf (accessed on 5 July 2023).
- World Anti-Doping Agency. WADA Technical Document TD2022DL. Available online: https://www.wada-ama.org/sites/default/files/2022-01/td2022dl_v1.0_final_eng_0.pdf (accessed on 5 July 2023).
- Mackay, L.G.; Kazlauskas, R. The importance of reference materials in doping-control analysis. Anal. Bioanal. Chem. 2011, 401, 483–492. [Google Scholar] [CrossRef]
- Harps, L.C.; Bizjak, D.A.; Girreser, U.; Zügel, M.; Steinacker, J.M.; Diel, P.; Parr, M.K. Quantitation of Formoterol, Salbutamol, and Salbutamol-4′-O-Sulfate in Human Urine and Serum via UHPLC-MS/MS. Separations 2023, 10, 368. [Google Scholar] [CrossRef]
- Winkler, M.; Geier, M.; Hanlon, S.P.; Nidetzky, B.; Glieder, A. Human Enzymes for Organic Synthesis. Angew. Chem. Int. Ed. 2018, 57, 13406–13423. [Google Scholar] [CrossRef] [Green Version]
- Drăgan, C.-A.; Peters, F.T.; Bour, P.; Schwaninger, A.E.; Schaan, S.M.; Neunzig, I.; Widjaja, M.; Zapp, J.; Kraemer, T.; Maurer, H.H.; et al. Convenient Gram-Scale Metabolite Synthesis by Engineered Fission Yeast Strains Expressing Functional Human P450 Systems. Appl. Biochem. Biotechnol. 2011, 163, 965–980. [Google Scholar] [CrossRef]
- Ko, K.; Kurogi, K.; Davidson, G.; Liu, M.Y.; Sakakibara, Y.; Suiko, M.; Liu, M.C. Sulfation of ractopamine and salbutamol by the human cytosolic sulfotransferases. J. Biochem. 2012, 152, 275–283. [Google Scholar] [CrossRef]
- Jacobson, G.A.; Raidal, S.; Robson, K.; Narkowicz, C.K.; Nichols, D.S.; Haydn Walters, E. Bronchopulmonary pharmacokinetics of (R)-salbutamol and (S)-salbutamol enantiomers in pulmonary epithelial lining fluid and lung tissue of horses. Br. J. Clin. Pharmacol. 2017, 83, 1436–1445. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Harps, L.C.; Bureik, M.; Parr, M.K. Human Sulfotransferase Assays With PAPS Production in situ. Front. Mol. Biosci. 2022, 9, 827638. [Google Scholar] [CrossRef]
- Teubner, W. Charakterisierung von Sulfotransferasen im Gastrointestinaltrakt von Mensch und Ratte und Aktivierung von Promutagenen in V79-Zellen, die Eine Intestinale Form (1B1) des Menschen und der Ratte Exprimieren; Universität Potsdam: Potsdam, Germany, 2001. [Google Scholar]
- Gamage, N.; Barnett, A.; Hempel, N.; Duggleby, R.G.; Windmill, K.F.; Martin, J.L.; McManus, M.E. Human sulfotransferases and their role in chemical metabolism. Toxicol. Sci. 2006, 90, 5–22. [Google Scholar] [CrossRef] [Green Version]
- Riches, Z.; Stanley, E.L.; Bloomer, J.C.; Coughtrie, M.W.H. Quantitative Evaluation of the Expression and Activity of Five Major Sulfotransferases (SULTs) in Human Tissues: The SULT “Pie”. Drug Metab. Dispos. 2009, 37, 2255. [Google Scholar] [CrossRef] [Green Version]
- Walle, T.; Eaton, E.A.; Walle, U.K.; Pesola, G.R. Stereoselective metabolism ofRS-albuterol in humans. Clin. Rev. Allergy Immunol. 1996, 14, 101–113. [Google Scholar] [CrossRef]
- Boulton, D.W.; Fawcett, J.P. Pharmacokinetics and pharmacodynamics of single oral doses of albuterol and its enantiomers in humans. Clin. Pharmacol. Ther. 1997, 62, 138–144. [Google Scholar] [CrossRef]
- Mareck, U.; Guddat, S.; Schwenke, A.; Beuck, S.; Geyer, H.; Flenker, U.; Elers, J.; Backer, V.; Thevis, M.; Schänzer, W. Determination of salbutamol and salbutamol glucuronide in human urine by means of liquid chromatography-tandem mass spectrometry. Drug Test. Anal. 2011, 3, 820–827. [Google Scholar] [CrossRef]
- Boulton, D.W.; Fawcett, J.P. Enantioselective disposition of salbutamol in man following oral and intravenous administration. Br. J. Clin. Pharmacol. 1996, 41, 35–40. [Google Scholar] [CrossRef]
- Ward, J.K.; Dow, J.; Dallow, N.; Eynott, P.; Milleri, S.; Ventresca, G.P. Enantiomeric disposition of inhaled, intravenous and oral racemic-salbutamol in man--no evidence of enantioselective lung metabolism. Br. J. Clin. Pharmacol. 2000, 49, 15–22. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Machalz, D.; Wolber, G.; Parr, M.K.; Bureik, M. Functional Expression of All Human Sulfotransferases in Fission Yeast, Assay Development, and Structural Models for Isoforms SULT4A1 and SULT6B1. Biomolecules 2020, 10, 1517. [Google Scholar] [CrossRef]
- Matuszewski, B.K.; Constanzer, M.L.; Chavez-Eng, C.M. Strategies for the assessment of matrix effect in quantitative bioanalytical methods based on HPLC-MS/MS. Anal. Chem. 2003, 75, 3019–3030. [Google Scholar] [CrossRef]
- World Anti-Doping Agency. WADA Technical Document TD2021IDCR. Available online: https://www.wada-ama.org/sites/default/files/resources/files/td2021idcr_final_eng_0.pdf (accessed on 21 July 2021).
- Orlovius, A.-K.L. Sulfokonjugierte Sympathomimetika in der Dopinganalytik: Synthese, Charakterisierung und Analyse; Rheinische Friedrich-Wilhelms-Universität Bonn: Bonn, Germany, 2014; Available online: https://hdl.handle.net/20.500.11811/6086 (accessed on 9 July 2023).
- Kharissova, O.V.; Kharisov, B.I.; Oliva González, C.M.; Méndez, Y.P.; López, I. Greener synthesis of chemical compounds and materials. R. Soc. Open Sci. 2019, 6, 191378. [Google Scholar] [CrossRef] [Green Version]
- Purchartová, K.; Valentová, K.; Pelantová, H.; Marhol, P.; Cvačka, J.; Havlíček, L.; Křenková, A.; Vavříková, E.; Biedermann, D.; Chambers, C.S.; et al. Prokaryotic and Eukaryotic Aryl Sulfotransferases: Sulfation of Quercetin and Its Derivatives. ChemCatChem 2015, 7, 3152–3162. [Google Scholar] [CrossRef]
- Horst, M.; Hartog, A.; Morabet, R.; Marais, A.; Kircz, M.; Wever, R. Enzymatic Sulfation of Phenolic Hydroxy Groups of Various Plant Metabolites by an Arylsulfotransferase. Eur. J. Org. Chem. 2015, 2015, 534–541. [Google Scholar] [CrossRef]
- Ragan, M.A. Phenol sulfate esters: Ultraviolet, infrared, 1H and 13C nuclear magnetic resonance spectroscopic investigation. Can. J. Chem. 1978, 56, 2681–2685. [Google Scholar] [CrossRef]
- Melchor, R.; Biddiscombe, M.F.; Mak, V.H.; Short, M.D.; Spiro, S.G. Lung deposition patterns of directly labelled salbutamol in normal subjects and in patients with reversible airflow obstruction. Thorax 1993, 48, 506–511. [Google Scholar] [CrossRef] [Green Version]
- Nishikawa, M.; Masuyama, Y.; Nunome, M.; Yasuda, K.; Sakaki, T.; Ikushiro, S. Whole-cell-dependent biosynthesis of sulfo-conjugate using human sulfotransferase expressing budding yeast. Appl. Microbiol. Biotechnol. 2018, 102, 723–732. [Google Scholar] [CrossRef]
- Nakpheng, T.; Songkarak, S.; Suwandecha, T.; Sritharadol, R.; Chunhachaichana, C.; Srichana, T. Evidences for salbutamol metabolism by respiratory and liver cell lines. Drug Metab. Pharmacokinet. 2017, 32, 127–134. [Google Scholar] [CrossRef]









| Electrospray Ionization | ||||
|---|---|---|---|---|
| Gas temperature | 170 °C | |||
| Gas flow | 17 L/min | |||
| Nebulizer | 10 psi | |||
| Sheath gas temperature | 400 °C | |||
| Sheath gas flow | 12 L/min | |||
| Capillary voltage | 4000 V | |||
| Nozzle voltage | 500 V | |||
| MRM | ||||
| Precursor Ion [m/z] | Product Ion [m/z] | Collision Energy [eV] | ||
| Salbutamol | [M+H]+ = 240.0 | 222.1 | 8 | |
| 166.1 | 12 | |||
| 148.1 * | 16 | |||
| 121.1 | 25 | |||
| 91.0 | 48 | |||
| 77.1 | 56 | |||
| Salbutamol-4′-O-sulfate | [M+H]+ = 320.0 | 240.0 * | 4 | |
| 222.0 | 16 | |||
| 166.0 | 16 | |||
| 148.0 | 32 | |||
| 77.0 | 80 | |||
| [M−H]− = 318.0 1 | 238.0 | 25 | ||
| d9-Salbutamol | [M+H]+ = 249.2 | 231.1 | 8 | |
| 166.1 | 12 | |||
| 148.1 | 16 | |||
| 121.1 | 25 | |||
| Salbutamol glucuronide | [M+H]+ = 416.0 1 | 298.0 | 12 | |
| 240.0 | 18 | |||
| 224.0 | 29 | |||
| 222.0 | 20 | |||
| 148.0 | 20 | |||
| [M−H]− = 414.0 1 | 396.0 | 18 | ||
| 220.0 | 25 | |||
| 146.0 | 25 | |||
| Salbutamol (a) | Salbutamol-4′-O-sulfate (a) | Chemical Shift Differences ∆δ= δOsulfate − δOH | ||||
|---|---|---|---|---|---|---|
| Position | 1H | 13C | 1H | 13C | 1H | 13C |
| 1 | 4.72, dd (b), 10.0, 2.8 Hz | 69.71 | 4.77, dd (b), 10.2, 2.6 Hz | 69.69 | +0.05 | –0.02 |
| 2 | 2.74/2.83, AB d (b) 11.8, 10.0, 2.8 Hz | 49.14 | 2.69/2.81 (c) | 49.67 | –0.05/–0.02 | +0.53 |
| 4 | 53.89 | 54.68 (d) | +0.79 | |||
| 5 | 1.20, s | 26.12 | 1.23, s | 25.91 | +0.03 | –0.21 |
| 1′ | 132.93 | 137.46 | +4.53 | |||
| 2′ | 7.31, d, 2.3 Hz | 125.88 | 7.43, d, 2.1 Hz | 124.86 | +0.12 | –1.02 |
| 3′ | 128.10 | 134.57 | +6.47 | |||
| 3′-CH2 | 4.47, s | 58.24 | 4.55, s | 58.30 | +0.08 | +0.06 |
| 4′ | 153.43 | 149.59 | –3.84 | |||
| 5′ | 6.73, d, 8.3 Hz | 114.16 | 7.27. d, 8.3 Hz | 121.46 | +0.54 | +7.30 |
| 6′ | 7.07, dd, 8.3, 2.3 Hz | 124.96 | 7.20, dd 8.3, 2.1 Hz | 121.50 | +0.13 | –3.46 |
| Product Ion (m/z) | 77.1 | 91.0 | 121.1 | 166.1 | 222.1 |
|---|---|---|---|---|---|
| salbutamol | 12.1–22.1 | 4.0–14.0 | 5.1–15.1 | 26.4–39.6 | 59.8–79.8 |
| Product Ion (m/z) | 148.0 | 166.0 | 222.0 | ||
| salbutamol-4′-O-sulfate | 44.8–64.8 | 15.2–25.2 | 29.9–44.9 |
| Salbutamol | Salbutamol-4′-O-sulfate | |
|---|---|---|
| tmax (urine) | ||
| Oral racemate 2 mg (SAP) | 3 h | 3 h |
| Inhaled aerosol racemate 600 µg (SA_MDI_2) | 1.5 h | 1.5 h |
| Oral levosalbutamol 1 mg (LSAP) | 3 h | 0.5 h |
| Inhaled levosalbutamol 630 µg (LSA_MDI) | 0.5 h | 3 h |
| Inhaled levosalbutamol 90 µg (LSA_MDI_TD) | 0.5 h | 3 h |
| Total urinary excretion 1 | ||
| Oral racemate 2 mg (SAP) 1 | 449 µg (22.5%) | 1030 µg (51.5%) |
| Inhaled aerosol racemate 600 µg (SA_MDI_2) 1 | 203 µg (33.8%) | 298 µg (49.6%) |
| Oral levosalbutamol 1 mg (LSAP) 1 | 65 µg (6.5%) | 847 µg (84.7%) |
| Inhaled levosalbutamol 630 µg (LSA_MDI) 1 | 129 µg (20.5%) | 371 µg (58.9%) |
| Inhaled levosalbutamol 90 µg (LSA_MDI_TD) 1 | 19 µg (21.1%) | 55 µg (61.1%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jendretzki, A.L.; Harps, L.C.; Sun, Y.; Bredendiek, F.; Bureik, M.; Girreser, U.; de la Torre, X.; Botrè, F.M.; Parr, M.K. Biosynthesis of Salbutamol-4′-O-sulfate as Reference for Identification of Intake Routes and Enantiopure Salbutamol Administration by Achiral UHPLC-MS/MS. Separations 2023, 10, 427. https://doi.org/10.3390/separations10080427
Jendretzki AL, Harps LC, Sun Y, Bredendiek F, Bureik M, Girreser U, de la Torre X, Botrè FM, Parr MK. Biosynthesis of Salbutamol-4′-O-sulfate as Reference for Identification of Intake Routes and Enantiopure Salbutamol Administration by Achiral UHPLC-MS/MS. Separations. 2023; 10(8):427. https://doi.org/10.3390/separations10080427
Chicago/Turabian StyleJendretzki, Annika Lisa, Lukas Corbinian Harps, Yanan Sun, Felix Bredendiek, Matthias Bureik, Ulrich Girreser, Xavier de la Torre, Francesco M. Botrè, and Maria Kristina Parr. 2023. "Biosynthesis of Salbutamol-4′-O-sulfate as Reference for Identification of Intake Routes and Enantiopure Salbutamol Administration by Achiral UHPLC-MS/MS" Separations 10, no. 8: 427. https://doi.org/10.3390/separations10080427