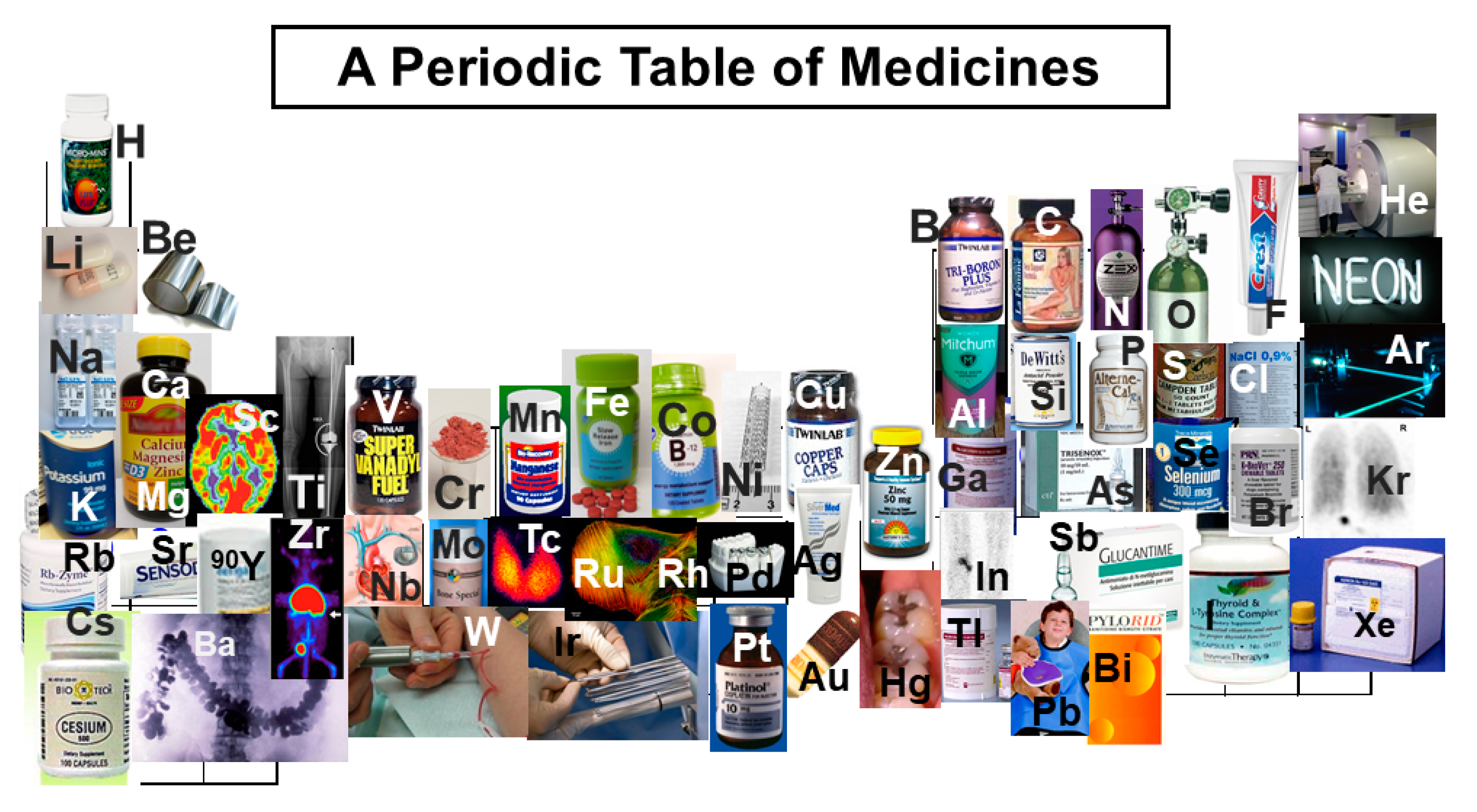
The First-Row Transition Metals in the Periodic Table of Medicine



Abstract
:1. Introduction
2. Properties of First-Row Transition Metals
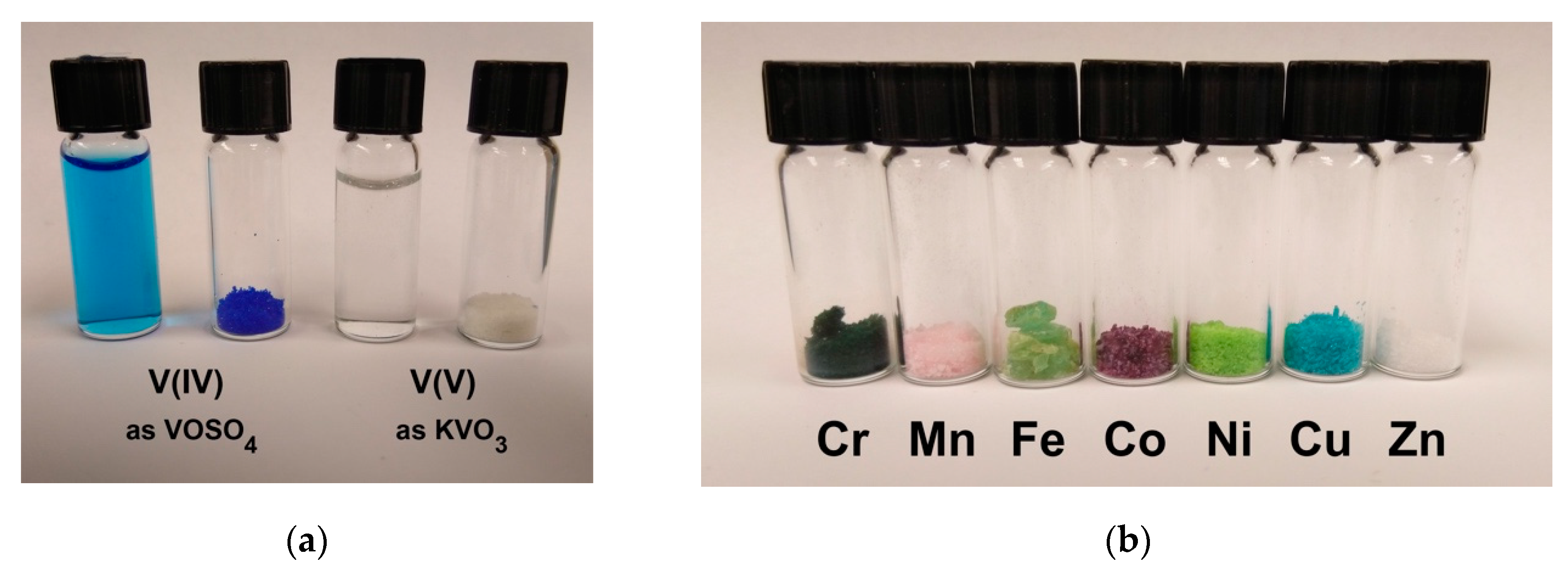
3. Speciation of First-Row Transition Metal Ions in Aqueous Solutions
4. Medicinal Uses of First-Row Transition Metals
4.1. Scandium (Sc)
4.2. Titanium (Ti)
4.3. Vanadium (V)
4.4. Chromium (Cr)
4.5. Manganese (Mn)
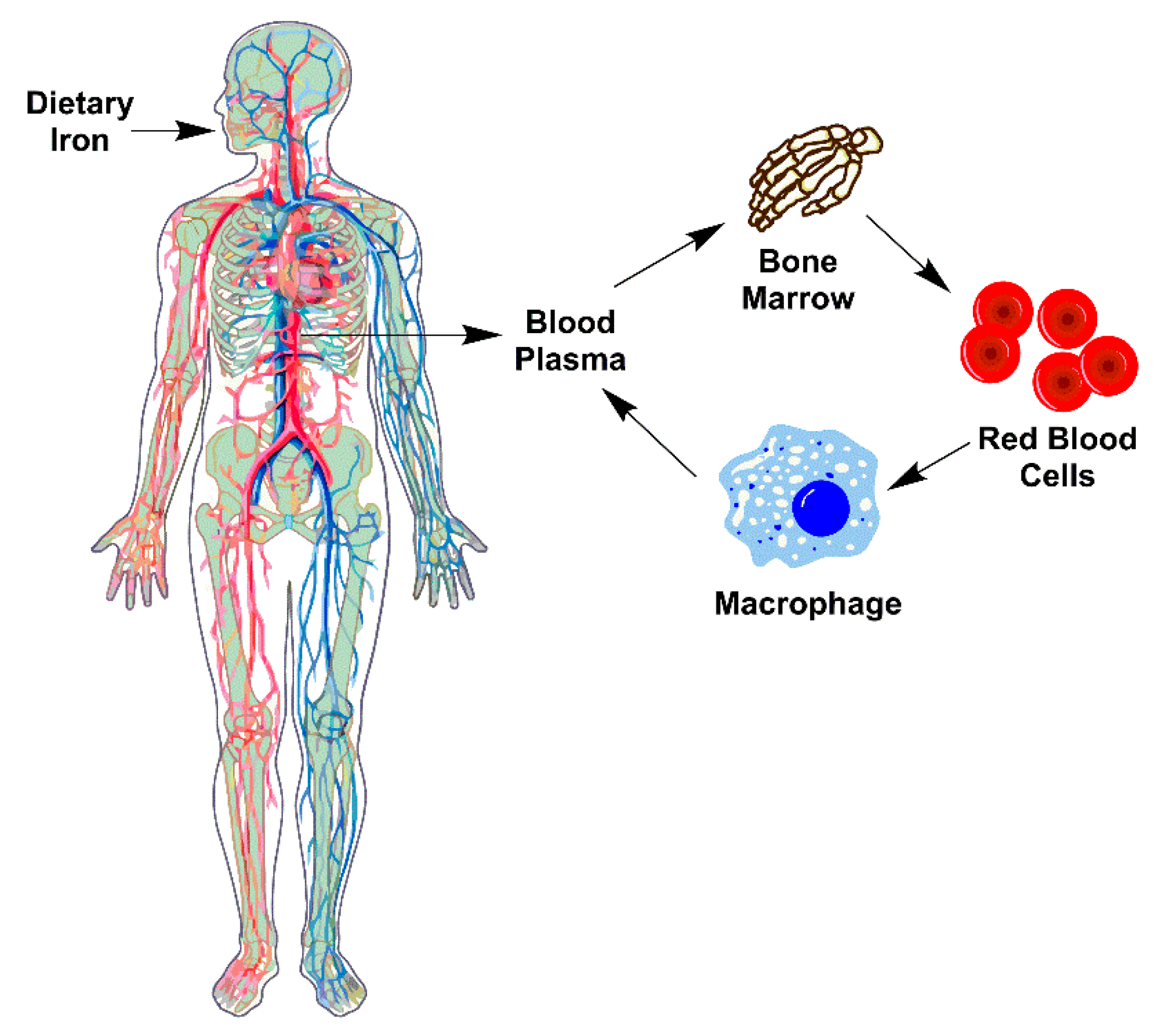
4.6. Iron (Fe)
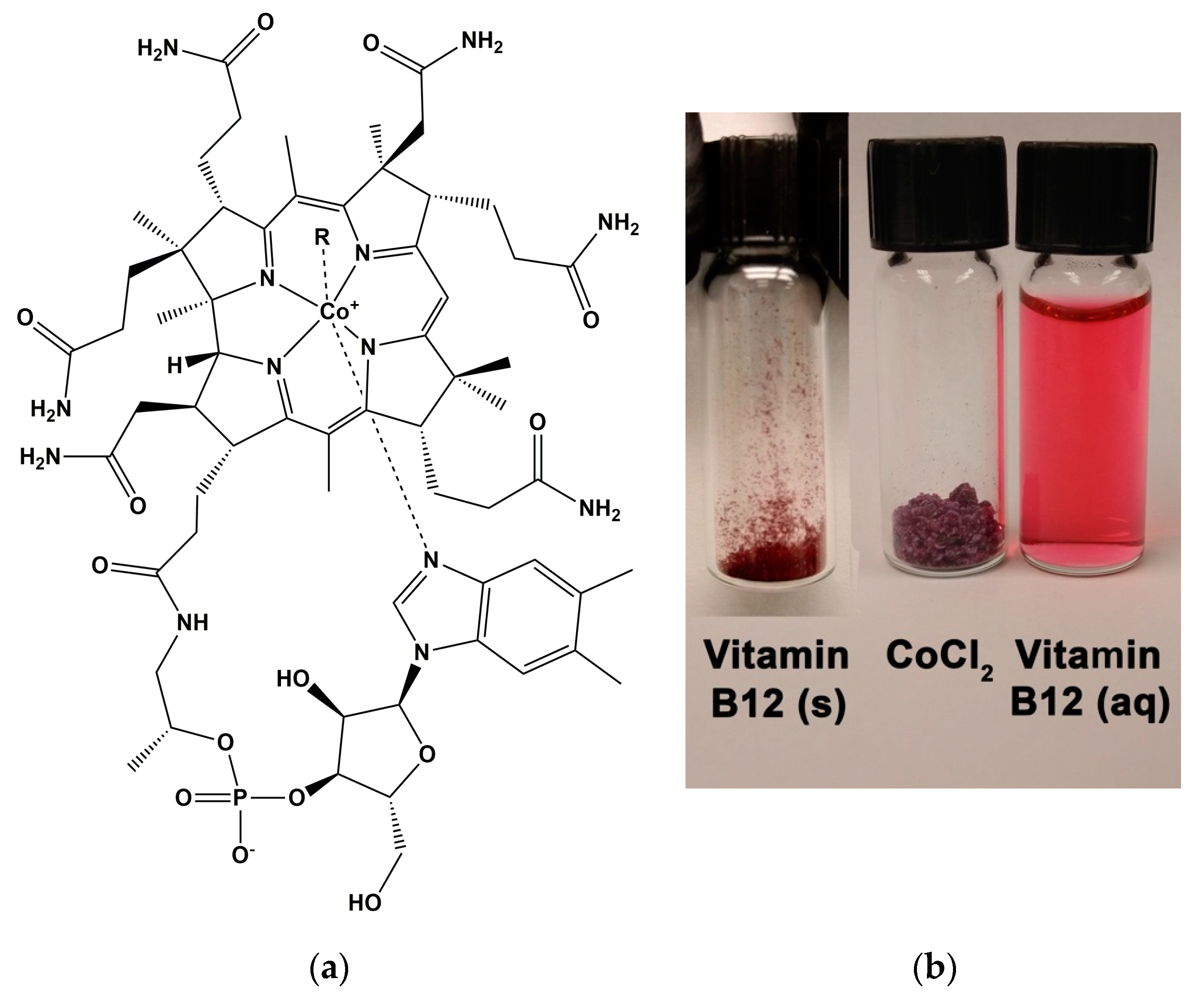
4.7. Cobalt (Co)
4.8. Nickel (Ni)
4.9. Copper (Cu)
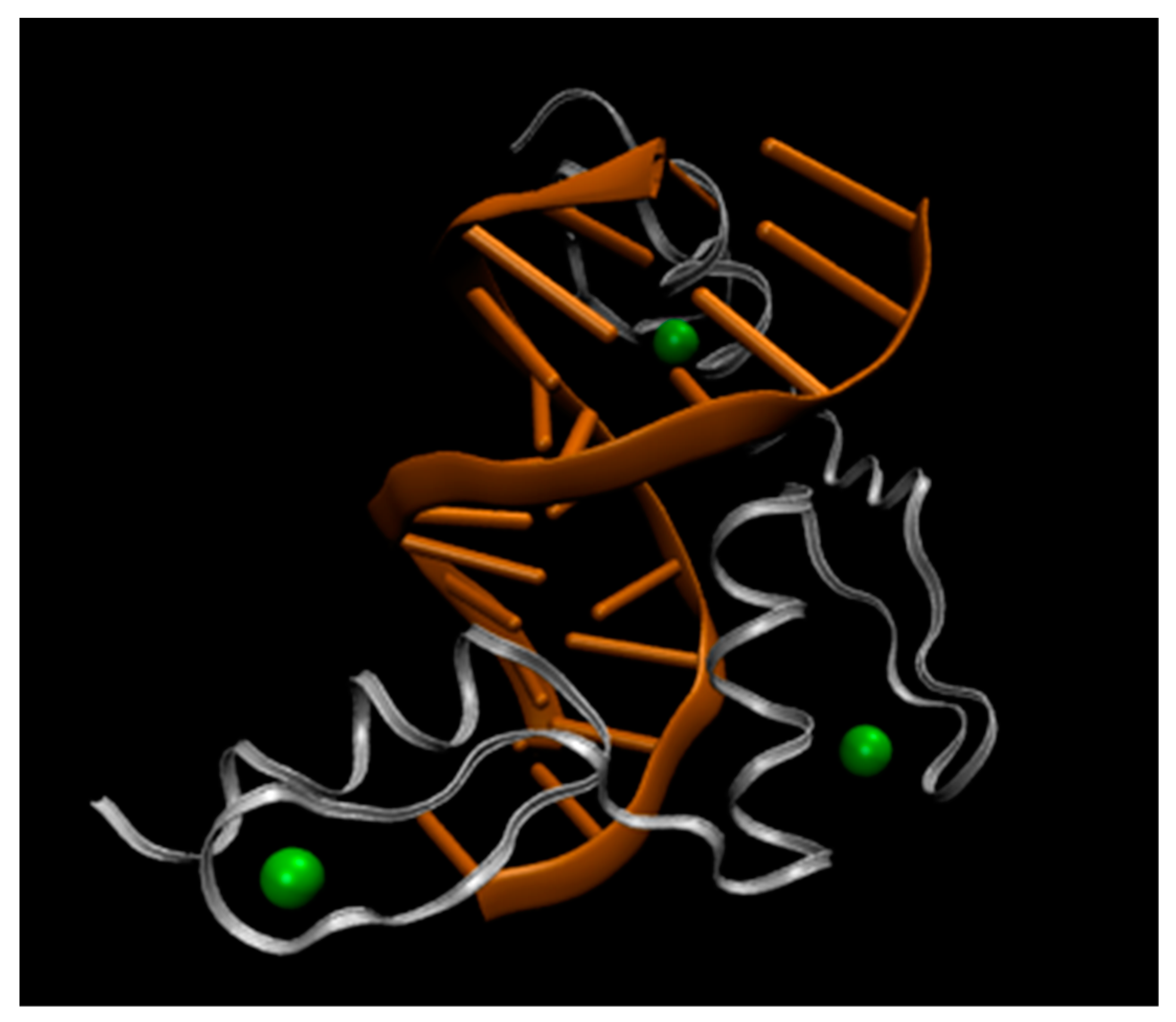
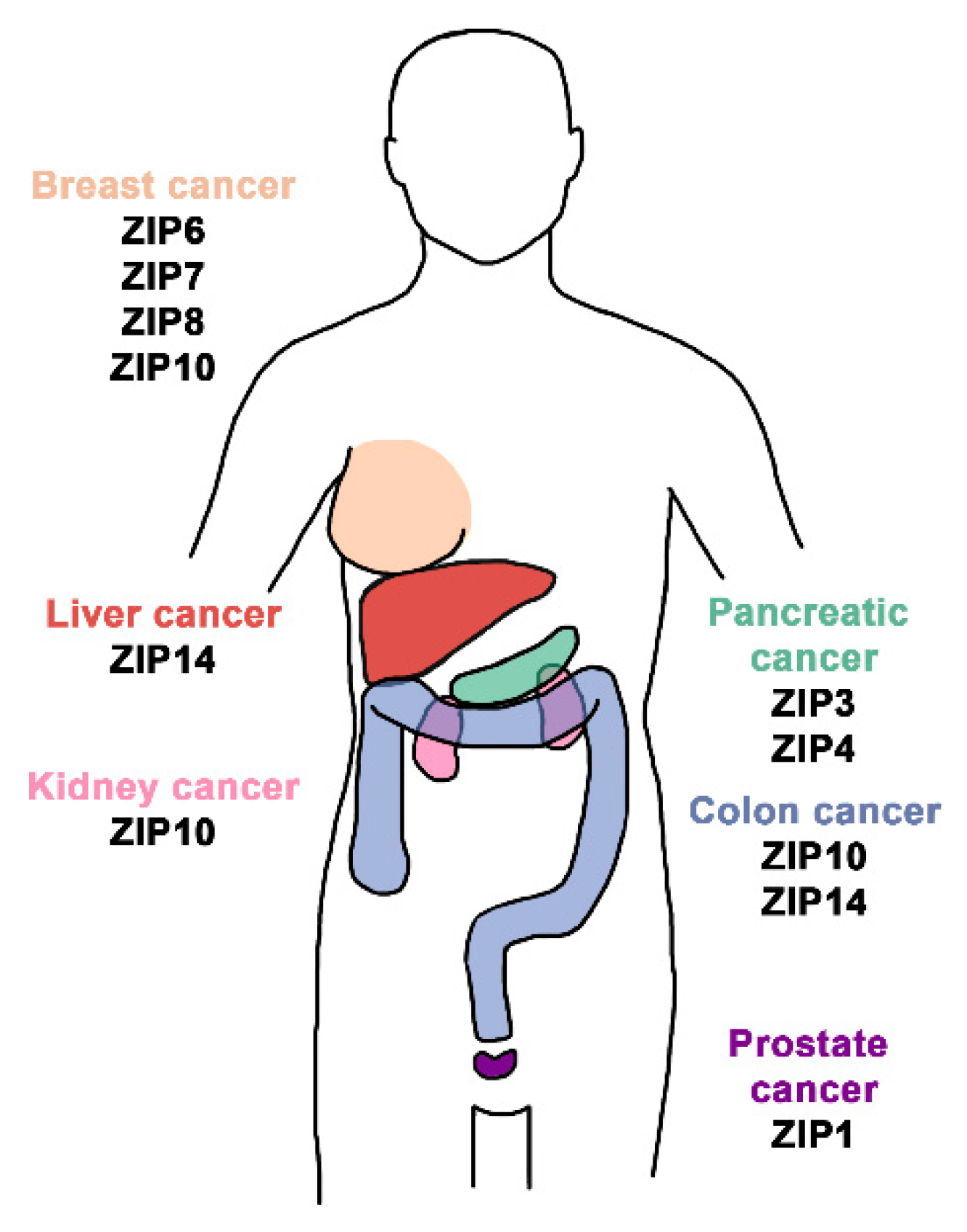
4.10. Zinc (Zn)
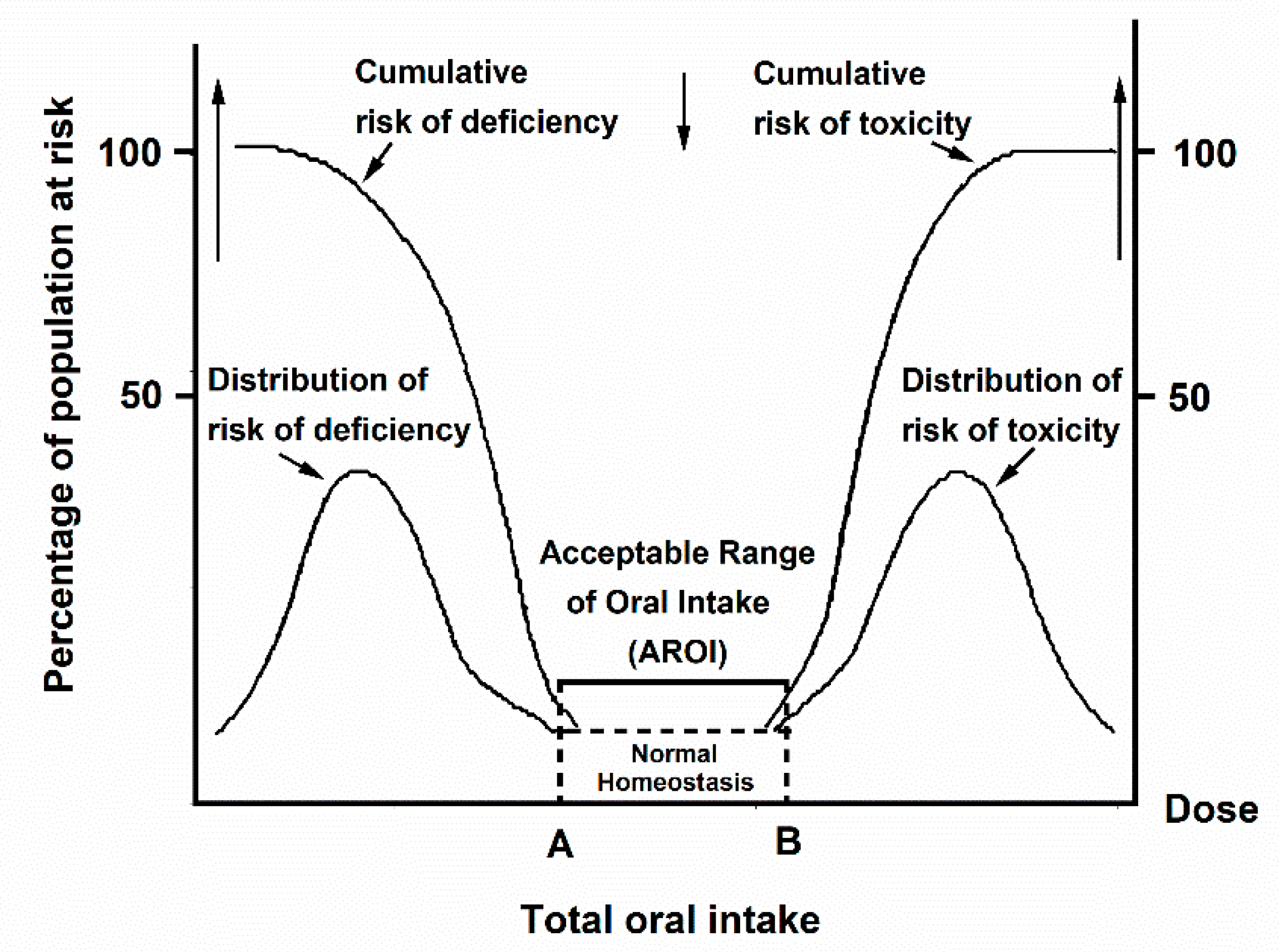
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lippard, S.L.; Berg, J.M. Principles of Bioinorganic Chemistry; University Science Books: Sausalito, CA, USA, 1994. [Google Scholar]
- Song, W.J.; Sontz, P.A.; Ambroggia, X.I.; Tezcan, F.A. Metals in Protein–Protein Interfaces. Annu. Rev. Biophys. 2014, 43, 409–431. [Google Scholar] [CrossRef]
- Weeks, M.E. The discovery of the elements. Chronology. J. Chem. Educ. 1933, 10, 223–227. [Google Scholar] [CrossRef]
- Sigel, H.; Sigel, A. The bio-relevant metals of the periodic table of the elements. Z. Für Nat. 2019, 74. [Google Scholar] [CrossRef]
- Scerri, E.R. The Periodic Table: Its Story and Its Significance; Oxford University Press: New York, NY, USA, 2007. [Google Scholar]
- Hsia, C.C.W. Respiratory Function of Hemoglobin. N. Engl. J. Med. 1998, 338, 239–247. [Google Scholar] [CrossRef]
- Frey, P.A.; Reed, G.H. The Ubiquity of Iron. ACS Chem. Biol. 2012, 7, 1477–1481. [Google Scholar] [CrossRef]
- Frieden, E. New Perspectives on the Essential Trace Elements. J. Chem Educ. 1985, 62, 917–923. [Google Scholar] [CrossRef]
- Chellan, P.; Sadler, P.J. The elements of life and medicines. Philos. Trans. A Math. Phys. Eng. Sci. 2015, 373, 56. [Google Scholar] [CrossRef]
- Rubino, J.T.; Franz, K.J. Coordination chemistry of copper proteins: How nature handles a toxic cargo for essential function. J. Inorg. Biochem. 2012, 107, 129–143. [Google Scholar] [CrossRef]
- Cotton, F.A.; Wilkinson, G.; Murillo, C.A.; Bochman, M. Advanced Inorganic Chemistry: A Comprehensive Text, 6th ed.; John Wiley and Sons: New York, NY, USA, 1999. [Google Scholar]
- Housecroft, C.E.; Sharpe, A.G. Inorganic Chemistry, 4th ed.; Pearson: Harlow, UK, 2012. [Google Scholar]
- Greenwood, N.N. Chemistry of the Elements, 2nd ed.; Oxford: Oxford, UK, 1997. [Google Scholar]
- Wang, W.; Pranolo, Y.; Cheng, C.Y. Metallurgical processes for scandium recovery from various resources: A review. Hydrometallurgy 2011, 108, 100–108. [Google Scholar] [CrossRef]
- Roberts, W.L.; Rapp, G.R.; Weber, J. Encyclopedia of Minerals; Van Nostrand Reinhold Company: New York, NY, USA, 1974. [Google Scholar]
- Williams-Jones, A.E.; Vasyukova, O.V. The Economic Geology of Scandium, the Runt of the Rare Earth Element Litter. Econ. Geol. 2018, 113, 973–988. [Google Scholar] [CrossRef]
- Barnebey, O.L.; Bishop, G.M. Differential Iodimetry IV.—The Analysis of Pyrolusite and Other Oxidized Manganese Ores. J. Am. Chem. Soc. 1917, 39, 1235–1238. [Google Scholar] [CrossRef]
- IUPAC. Compendium of Chemical Terminology (Gold Book); IUPAC: Research Triangle Park, NC, USA, 2014; p. 1622. [Google Scholar]
- Parkin, G. Valence, oxidation number, and formal charge: Three related but fundamentally different concepts. J. Chem. Educ. 2006, 83, 791–800. [Google Scholar] [CrossRef]
- Levina, A.; Lay, P.A. Mechanistic studies of relevance to the biological activities of chromium. Coord. Chem. Rev. 2005, 249, 281–298. [Google Scholar] [CrossRef]
- Scepaniak, J.J.; Vogel, C.S.; Khusniyarov, M.M.; Heinemann, F.W.; Meyer, K.; Smith, J.M. Synthesis, Structure, and Reactivity of an Iron(V) Nitride. Science 2011, 331, 1049–1052. [Google Scholar] [CrossRef] [Green Version]
- Baes, C.F.; Mesmer, R.E. The Hydrolysis of Cations; Wiley: New York, NY, USA, 1976. [Google Scholar]
- Horton, D.C.; VanDerveer, D.; Krysztek, J.; Telser, J.; Pittman, T.; Crans, D.C.; Holder, A. Spectroscopic Characterization of L-ascorbic Acid-induced Reduction of Vanadium(V) Dipicolinates: Formation of Vanadium(III) and Vanadium(IV) Complexes from Vanadium(V) Dipicolinate Derivatives. Inorg. Chim. Acta 2014, 420, 112–119. [Google Scholar] [CrossRef]
- Pyrzyńska, K.; Kilian, K.; Pęgier, M. Separation and purification of scandium: From industry to medicine. Sep. Purif. Rev. 2018, 48, 65–77. [Google Scholar] [CrossRef]
- Røyset, J.; Ryum, N. Scandium in aluminum alloys. Int. Mater. Rev. 2005, 50, 19–44. [Google Scholar] [CrossRef]
- Hirano, S.; Suzuki, K.T. Exposure, Metabolism, and Toxicity of Rare Earths and Related Compounds. Environ. Health Perspect. 1996, 104, 85–95. [Google Scholar] [CrossRef]
- Xu, T.; Zhang, M.; Hu, J.; Li, Z.; Wu, T.; Bao, J.; Wu, S.; Lei, L.; He, D. Behavioral deficits and neural damage of Caenorhabditis elegans induced by three rare earth elements. Chemosphere 2017, 181, 55–62. [Google Scholar] [CrossRef]
- Tai, P.; Zhao, Q.; Su, D.; Li, P.; Stagnitti, F. Biological toxicity of lanthanide elements on algae. Chemosphere 2010, 80, 1031–1035. [Google Scholar] [CrossRef]
- Majkowska-Pilip, A.; Bilewicz, A. Macrocyclic complexes of scandium radionulides as precursors for diagnostic and therapeutic radiopharmeceuticals. J. Inorg. Biochem. 2011, 105, 313–320. [Google Scholar] [CrossRef]
- Chaple, I.F.; Lapi, S.E. Production and Use of the First-Row Transition Metal PET Radionuclides 43,44Sc, 52Mn, 45Ti. J. Nucl. Med. 2018, 59, 1655–1659. [Google Scholar] [CrossRef]
- Huclier-Markai, S.; Sabatie, A.; Ribet, S.; Kubíček, V.; Paris, M.; Vidaud, C.; Hermann, P.; Cutler, C.S. Chemical and biological evaluation of scandium(III)-polyaminopolycarboxylate complexes as potential PET agents and radiopharmaceuticals. Radiochim. Acta 2011, 99, 653–662. [Google Scholar] [CrossRef]
- Müller, C. Folate-Based Radiotracers for PET Imaging Update and Perspectives. Molecules 2013, 18, 5005–5031. [Google Scholar] [CrossRef]
- Huclier-Markai, S.; Alliot, C.; Kerdjoudj, R.; Mougin-Degraef, M.; Chouin, N.; Haddad, F. Promising Scandium Radionuclides for Nuclear Medicine: A Review on the Production and Chemistry up to In Vivo Proofs of Concept. Cancer Biother. Radiopharm. 2018, 33, 316–329. [Google Scholar] [CrossRef]
- Chakravarty, R.; Goel, S.; Valdovinos, H.F.; Hernandez, R.; Hong, H.; Nickles, R.J.; Cai, W. Matching the Decay Half-Life with the Biological Half-Life: ImmunoPET Imaging with 44Sc-Labeled Cetuximab Fab Fragment. Bioconjugate Chem. 2014, 25, 2197–2204. [Google Scholar] [CrossRef]
- Van Dongen, G.A.; Visser, G.W.; Lub-de Hooge, M.N.; de Vries, E.G.; Perk, L.R. Immuno-PET: A Navigator in Monoclonal Antibody Development and Applications. Oncologist 2007, 12, 1379–1389. [Google Scholar] [CrossRef] [Green Version]
- Verel, I.; Visser, G.W.M.; Boellaard, R.; Stigter-van Walsum, M.; Snow, G.B.; van Dongen, G.A.M.S. 89Zr Immuno-PET: Comprehensive Procedures for the Production of 89Zr-Labeled Monoclonal Antibodies. J. Nucl. Med. 2003, 44, 1271–1281. [Google Scholar]
- Ozcelik, O.; Seydaoglu, G.; Haytac, C.M. Diode lasers for harvesting de-epithelialized palatal graft in the treatment of gingival recession defects: A randomized clinic trial. J. Clin. Periodontol. 2016, 43, 63–71. [Google Scholar] [CrossRef]
- Hakki, S.S.; Korkusuz, P.; Berk, G.; Dundar, N.; Saglam, M.; Bozkurt, B. Comparison of Er,Cr:YSGG Laser and Hand Instrumentation on the Attachment of Periodontal Ligament Fibroblasts to Periodontally Diseased Root Surfaces: An In Vitro Study. J. Periodontol. 2010, 81, 1216–1225. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Utsunomiya, A.; Akamatsu, H.; Neishi, K.; Furukawa, M.; Horita, Z.; Langdon, T.G. Influence of scandium and zirconium on grain stability and superplastic ductiles in ultrafine-grained Al–Mg alloys. Acta Mater. 2002, 50, 553–564. [Google Scholar] [CrossRef]
- Buettner, K.M.; Valentine, A.M. Bioinorganic Chemistry of Titanium. Chem. Rev. 2012, 112, 1863–1881. [Google Scholar] [CrossRef]
- Sharma, S.; Sharma, R.K.; Haur, K.; Cátala Torres, J.F.; Loza-Rosas, S.A.; Torres, A.; Saxena, M.; Julin, M.; Tinoco, A.D. Fueling a Hot Debate on the Application of TiO2 Nanoparticles in Sunscreen. Materials 2019, 12, 2317. [Google Scholar] [CrossRef]
- Davis, J.M.; Long, T.C.; Shatkin, J.A.; Wang, A.; Graham, J.A.; Gwinn, M.; Ranalli, B. Nanomaterial Case Studies: Nanoscale Titanium Dioxide in Water Treatment and in Topical Sunscreen (Final); US Environmental Protection Agency: Washington, DC, USA, 2010; p. 204. [Google Scholar]
- Tinoco, A.D.; Eames, E.V.; Valentine, A.M. Reconsideration of Serum Ti(IV) Transport: Albumin and Transferrin Trafficking of Ti(IV) and Its Complexes. J. Am. Chem. Soc. 2007, 130, 2262–2270. [Google Scholar] [CrossRef]
- Oosthuizen, S.J. Titanium: The innovators’ metal-Historical case studies tracing titanium process and product innovation. J. South. Afr. Inst. Min. Metall. 2011, 111, 781–786. [Google Scholar]
- Sansone, V.; Pagani, D.; Melato, M. The effects on bone cells of metal ions released from orthopaedic implants. A review. Clin. Cases Miner. Bone Metab. 2013, 10, 34–40. [Google Scholar] [CrossRef]
- Jung, C. About Oxygen, Cytochrome P450 and Titanium: Learning from Ron Estabrook. Drug Metab. Rev. 2007, 39, 501–513. [Google Scholar] [CrossRef]
- Tshuva, E.Y.; Miller, M. Coordination Complexes of Titanium(IV) for Anticancer Therapy. In Metallo-Drugs: Development and Action of Anticancer Agents; Sigel, A., Sigel, H., Freisinger, E., Sigel, R.K.O., Eds.; de Gruyter: Berlin, Germany, 2018; Volume 18, pp. 219–250. [Google Scholar]
- Kubacka, A.; Suárez Diez, M.; Rojo, D.; Bargiela, R.; Ciordia, S.; Zapico, I.; Albar, J.P.; Barbas, C.; Martins dos Santos, V.A.P.; Fernádez-Garcia, M.; et al. Understanding the microbial mechanism if TiO2-based nanocomposite films in a pathogenic bacterium. Sci. Rep. 2014, 4, 4134. [Google Scholar] [CrossRef]
- Chen, Q.; Thouas, G.A. Metallic implant biomaterials. Mater. Sci. Eng. R 2015, 87, 1–57. [Google Scholar] [CrossRef]
- Golaski, M.; Herman, M.; Piekoszewski, W. Toxicological aspects of soluble titanium—A review of in vitro and in vivo studies. Metallomics 2016, 8, 1227–1242. [Google Scholar] [CrossRef]
- Lechner, J.; Noumbissi, S.; von Baehr, V. Titanium implants and silent inflammation in jawbone—A critical interplay of dissolved titanium particles and cytokines TNF-α and RANTES/CCL5 on overall health? EPMA J. 2018, 9, 331–343. [Google Scholar] [CrossRef]
- Makihira, S.; Mine, Y.; Nikawa, H.; Shuto, T.; Iwata, S.; Hosokawa, R.; Kamoi, K.; Okazaki, S.; Yamaguchi, Y. Titanium ion induces necrosis and sensitivity to lipopolysaccharide in gingival spithelial-like cells. Toxicol. In Vitro 2010, 24, 1905–1910. [Google Scholar] [CrossRef]
- Soto-Alvaredo, J.; Blanco, E.; Bettmer, J.; Hevia, D.; Sainz, R.M.; López Cháves, C.; Sánchez, C.; Llopis, J.; Sanz-Medel, A.; Montes-Bayón, M. Evaluation of the biological effect of Ti generated debris from metal implants: Ions and nanoparticles. Metallomics 2014, 6, 1702–1708. [Google Scholar] [CrossRef]
- Huang, J.-H.; Huang, F.; Evans, L.; Glasauer, S. Vanadium: Global (bio)geochemistry. Chem. Geol. 2015, 417, 68–89. [Google Scholar] [CrossRef]
- Crans, D.C.; Amin, S.S.; Keramidas, A.D. Chemistry of relevance to vanadium in the environment. In Vanadium in the Environment Part 1: Chemistry and Biochemistry; Nriagu, J.O., Ed.; Wiley and Sons: New York, NY, USA, 1998. [Google Scholar]
- Fish, R.H.; Komlenic, J.J. Molecular characterization and profile identifications of vanadyl compounds in heavy crude petroleums by liquid chromatography/graphite furnace atomic absorption spectrometry. Anal. Chem. 1984, 56, 510–517. [Google Scholar] [CrossRef]
- Nriagu, J.O.; Pirrone, N. Vanadium in the atmosphere. In Vanadium in the Environment Part 1: Chemistry and Biochemistry; Nriagu, J.O., Ed.; Wiley and Sons: New York, NY, USA, 1998. [Google Scholar]
- Fraústo da Silva, J.J.R. Vanadium in biology the case of the Amanita toadstools. Chem. Speciat. Bioavailab. 1989, 1, 139–150. [Google Scholar] [CrossRef]
- Bayer, E. Amavadin: The vanadium compound in amanitae. In Metal Ions in Biological Systems; Sigel, H., Sigel, A., Eds.; Marcel Dekker, Inc.: New York, NY, USA, 1995; Volume 31, pp. 407–422. [Google Scholar]
- Nielsen, F.H. The Nutritional Essentiality and Physiological Metabolism of Vanadium in Higher Animals. In Vanadium Compounds: Chemistry, Biochemistry, and Therapeutic Applications; Tracey, A.S., Crans, D.C., Eds.; American Chemical Society: Washington, DC, USA, 1998; Volume 711, pp. 297–307. [Google Scholar]
- Leblanc, C.; Vilter, H.; Fournier, J.-B.; Delage, L.; Potin, P.; Rebuffet, E.; Michel, G.; Solari, P.L.; Feiters, M.C.; Czjzek, M. Vanadium haloperoxidases: From the discovery 30 years ago to X-ray crystallographic and V K-edge absorption spectroscopic studies. Coord. Chem. Rev. 2015, 301, 134–146. [Google Scholar] [CrossRef]
- Michibata, H.; Ueki, T. Advances in research on the accumulation, redox behavior, and function of vanadium in ascidians. Biomol. Concepts 2010, 1, 97–107. [Google Scholar] [CrossRef]
- Crans, D.C.; Smee, J.J.; Gaidamauskas, E.; Yang, L. The Chemistry and Biochemistry of Vanadium and the Biological Activities Exerted by Vanadium Compounds. Chem. Rev. 2004, 104, 849–902. [Google Scholar] [CrossRef]
- Pessoa, J.C.; Etcheverry, S.; Gambino, D. Vanadium compounds in medicine. Coord. Chem. Rev. 2015, 301, 24–48. [Google Scholar] [CrossRef]
- Rehder, D. The Bioinorganic Chemistry of Vanadium. Angew. Chem. Int. Ed. Engl. 1991, 30, 148–167. [Google Scholar] [CrossRef]
- Harvey, I.; Arber, J.M.; Eady, R.R.; Smith, B.E.; Garner, C.D.; Hasnain, S.S. Iron K-edge X-ray-absorption spectroscopy of the iron vanadium cofactor of the vanadium nitrogenase from Azobacter chroococcum. Biochem. J. 1990, 266, 929–931. [Google Scholar]
- Lee, C.C.; Hu, Y.; Ribbe, M.W. Vanadium Nitrogenase Reduces CO. Science 2010, 329, 642. [Google Scholar] [CrossRef]
- Sipper, D.; Einsle, O. The structure of vanadium nitrogenase reveals an unusual bridging ligand. Nat. Chem. Biol. 2017, 13, 956–961. [Google Scholar] [CrossRef]
- Crans, D.C.; Henry, L.; Cardiff, G.M.; Posner, B.I. Developing Vanadium as an Antidiabetic or Anticancer Drug: A Clinical and Historical Perspective. In Essential Metals in Medicine: Therputic Use and Toxicity of Metal Ions in the Clinic; Carver, P.L., Ed.; de Gruyter: Berlin, Germany, 2019; pp. 203–230. [Google Scholar]
- Crans, D.C. Antidiabetic, Chemical, and Physical Properties of Organic Vanadates as Presumed Transition-State Inhibitors for Phosphatases. J. Org. Chem. 2015, 80, 11899–11915. [Google Scholar] [CrossRef] [Green Version]
- McLauchlan, C.C.; Peters, B.J.; Willsky, G.R.; Crans, D.C. Vanadium-phosphatase complexes: Phosphatase inhibitors favor the trigonal bipyramidal transition state geometries. Coord. Chem. Rev. 2015, 301, 163–199. [Google Scholar] [CrossRef]
- Cantley, L.C.; Josephson, L.; Warner, R.; Yanagisawa, M.; Lechene, C.; Guidotti, G. Vanadate is a potent (Na,K)-ATPase inhibitor found in ATP from muscle. J. Biol. Chem. 1977, 251, 7421–7423. [Google Scholar]
- Borah, B.; Chen, C.-W.; Egan, W.; Miller, M.; Wlodawer, A.; Cohen, J.S. Nuclear magnetic resonance and neutron diffraction studies of the complex of ribonuclease A with uridine vanadate, a transition-state analogue. Biochemistry 1985, 24, 2058–2067. [Google Scholar] [CrossRef]
- Thompson, K.H.; Lichter, J.; LeBel, C.; Scaife, M.C.; McNeill, J.H.; Orvig, C. Vanadium treatment of type 2 diabetes: A view to the future. J. Inorg. Biochem. 2009, 103, 554–558. [Google Scholar] [CrossRef]
- Thompson, K.H.; Orvig, C. Vanadium in diabetes: 100 years from Phase 0 to Phase I. J. Inorg. Biochem. 2006, 100, 1925–1935. [Google Scholar] [CrossRef]
- Bishayee, A.; Waghray, A.; Patel, M.A.; Chatterjee, M. Vanadium in the detection, prevention and treatment of cancer: The in vivo evidence. Cancer Lett. 2010, 294, 1–12. [Google Scholar] [CrossRef]
- Crans, D.C.; Yang, L.; Haase, A.; Yang, X. Health Benefits of Vanadium and its Potential as an Anticancer Agent. In Metallo-Drugs: Development and Action of Anticancer Agents; Sigel, A., Sigel, H., Freisinger, E., Sigel, R.K.O., Eds.; de Gruyter: Berlin, Germany, 2018; Volume 18, pp. 251–280. [Google Scholar]
- Selman, M.; Ruosso, C.; Bergeron, A.; Son, H.H.; Krishnan, R.; El-Sayes, N.A.; Varette, O.; Chen, A.; Le Boeuf, F.; Tzelepis, F.; et al. Multi-modal Potentiation of Oncolytic Virotherapy by Vanadium Compounds. Mol. Ther. 2018, 26, 56–69. [Google Scholar] [CrossRef] [Green Version]
- Bergeron, A.; Kostenkova, K.; Selman, M.; Murakami, H.A.; Owens, E.; Haribabu, N.; Arulanandam, R.; Diallo, J.-S.; Crans, D.C. Enhancement of oncolytic virotherapy by vanadium(V) dipicolinates. BioMetals 2019, 32, 545–561. [Google Scholar] [CrossRef]
- Di Bona, K.R.; Love, S.; Rhodes, N.R.; McAdory, D.; Sinha, S.H.; Kern, N.; Kent, J.; Strickland, J.; Wilson, A.; Beaird, J.; et al. CHromium is not an essential trace element for mammals: Effects of a “low-chromium” diet. J. Biol. Inorg. Chem. 2011, 16, 381–390. [Google Scholar] [CrossRef]
- Vincent, J.B. Chromium: Is It Essential, Pharmacologically Relevant, or Toxic? In Interrelations between Essential Metal. Ions and Human Diseases; Sigel, A., Sigel, H., Sigel, R.K.O., Eds.; Springer: Dordrecht, The Netherlands, 2013; Volume 13, pp. 171–198. [Google Scholar]
- Wu, L.E.; Levina, A.; Harris, H.H.; Cai, Z.; Lai, B.; Vogt, S.; James, D.E.; Lay, P.A. Carcinogenic Chromium(VI) Compounds Formed by Intracellular Oxidation of Chromium(III) Dietary Supplements by Adipocytes. Angew. Chem. Int. Ed. 2016, 55, 1742–1745. [Google Scholar] [CrossRef]
- Valko, M.; Rhodes, N.R.; Moncol, J.; Izakovic, M.; Mazur, M. Free radicals, metals and antioxidants in oxidative stress-induced cancer. Chem. Biol. Interact. 2006, 160, 1–40. [Google Scholar] [CrossRef]
- Jomova, K.; Valko, M. Advances in metal-induced oxidative stress and human disease. Toxicology 2011, 283, 65–87. [Google Scholar] [CrossRef]
- Levina, A.; Pham, T.H.N.; Lay, P.A. Binding of Chromium(III) to Transferrin Could Be Involved in Detoxification of Dietary CHromium(III) Rather than Transport of an Essential Trace Element. Angew. Chem. Int. Ed. 2016, 55, 8104–8107. [Google Scholar] [CrossRef]
- Anderson, R.A. Chromium, glucose intolerance and diabetes. J. Am. Coll. Nutr. 1998, 17, 548–555. [Google Scholar] [CrossRef]
- Schwarz, K.; Mertz, W. Chromium(III) and the Glucose Tolerance Factor. Arch. Biochem. 1959, 85, 292–295. [Google Scholar] [CrossRef]
- Suh, M.; Wikoff, D.; Lipworth, L.; Goodman, M.; Fitch, S.; Mittal, L.; Ring, C.; Proctor, D. Hexavalent chromium and stomach cancer: A systematic review and meta-analysis. Crit. Rev. Toxicol. 2019, 1–20. [Google Scholar] [CrossRef]
- Proctor, D.M.; Suh, M.; Campleman, S.L.; Thompson, C.M. Assessment of the mode of action for hexavalent chromium-induced lung cancer following inhalation exposures. Toxicology 2014, 325, 160–179. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. Chromium(VI) Compounds. Available online: https://monographs.iarc.fr/wp-content/uploads/2018/06/mono100C-9.pdf (accessed on 25 July 2019).
- Levina, A.; Codd, R.; Dillon, C.T.; Lay, P.A. Chromium in Biology: Toxicology and Nutritional Aspects. In Progress in Inorganic Chemistry; Meyer, G.J., Karlin, K.D., Eds.; Wiley and Sons: New York, NY, USA, 2003. [Google Scholar]
- Institute of Medicine. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academic Press: Washington, DC, USA, 2001. [Google Scholar]
- Hasan, H. Manganese; Rosen Publishing Group: New York, NY, USA, 2008. [Google Scholar]
- Chambers, A.; Krewski, D.; Birkett, N.; Plunkett, L.; Hertzberg, R.; Danzeisen, R.; Aggett, P.J.; Starr, T.B.; Baker, S.; Dourson, M.; et al. An exposure-response curve for copper excess and deficiency. J. Toxicol. Environ. Health Part B 2010, 13, 546–578. [Google Scholar] [CrossRef]
- Takeda, A. Manganese action in brain function. Brain Res. Rev. 2003, 41, 79–87. [Google Scholar] [CrossRef]
- Suárez, I.; Bodega, G.; Fernández, B. Glutamine synthetase in brain: Effects of ammonia. Neurochem. Int. 2002, 41, 123–142. [Google Scholar] [CrossRef]
- Umena, Y.; Kawakami, K.; Shen, J.-R.; Kamiya, N. Crystal structure of oxygen-evolving photosystem II at a resolution of 1.9 Å. Nature 2011, 473, 55–60. [Google Scholar] [CrossRef]
- Matés, J.M.; Pérez-Gómez, C.; de Castro, I.N. Antioxidant Enzymes and Human Diseases. Clin. Biochem. 1999, 32, 595–603. [Google Scholar] [CrossRef]
- Li, G.J.; Zhang, L.-L.; Lu, L.; Wu, P.; Zheng, W. Occupational Exposure to Welding Fume among Welders: Alterations of Manganese, Iron, Zinc, Copper, and Lead in Body Fluids and the Oxidative Stress. J. Occup. Environ. Med. 2004, 46, 241–248. [Google Scholar] [CrossRef]
- Jungwirth, U.; Kowol, C.R.; Keppler, B.K.; Hartinger, C.G.; Berger, W.; Heffeter, P. Anticancer Activity of Metal Complexes: Involvement of Redox Processes. Antioxid. Redox Signal. 2011, 15, 1085–1127. [Google Scholar] [CrossRef] [Green Version]
- Batinić-Haberle, I.; Rebouças, J.S.; Spasojević, I. Superoxide Dismutase Mimics: Chemistry, Pharmacology, and Therapeutic Potential. Antioxid. Redox Signal. 2010, 13, 877–918. [Google Scholar] [CrossRef] [Green Version]
- Triller, M.U.; Hsieh, W.-Y.; Pecoraro, V.L.; Rompel, A.; Krebs, B. Preparation of Highly Efficient Manganese Catalase Mimics. Inorg. Chem. 2002, 41, 5544–5554. [Google Scholar] [CrossRef]
- Aschner, M.; Erikson, K.M.; Dorman, D.C. Manganese Dosimetry: Species Differences and Implications for Neurotoxicity. Crit. Rev. Toxicol. 2005, 35, 1–32. [Google Scholar] [CrossRef]
- Martinez-Finley, E.J.; Gavin, C.E.; Aschner, M.; Gunter, T.E. Manganese neurotoxicity and the role of reactive oxygen species. Free Radic. Biol. Med. 2013, 62, 65–75. [Google Scholar] [CrossRef] [Green Version]
- Kwakye, G.F.; Paoliello, M.M.B.; Mukhopadhyay, S.; Bowman, A.B.; Aschner, M. Manganese-Induced Parkinsomism and Parkinson’s Disease: Shared and Distinguishable Features. Int. J. Environ. Res. Public Health 2015, 12, 7519–7540. [Google Scholar] [CrossRef]
- Caline, D.B.; Chu, N.S.; Huang, C.C.; Lu, C.S.; Olanow, W. Manganism and idiopathic parkinsonism: Similarities and differences. Neurology 1994, 44, 1583–1586. [Google Scholar] [CrossRef]
- Thévenod, F. Iron and Its Role in Cancer Defense: A Double-Edged Sword. In Metallo-Drugs: Development and Action of Anticancer Agents; Sigel, A., Sigel, H., Freisinger, E., Sigel, R.K.O., Eds.; de Gruyter: Berlin, Germany, 2018; pp. 437–467. [Google Scholar]
- Nelson, D.L.; Cox, M.M. Lehinger Principles of Biochemistry, 5th ed.; W.H. Freeman: New York, NY, USA, 2008. [Google Scholar]
- Blumenthal, I. Carbon monoxide poisoning. J. R. Soc. Med. 2001, 94, 270–272. [Google Scholar] [CrossRef]
- Crichton, R. Iron Metabolism: From Molecular Mechanisms to Clinical Consequences, 4th ed.; Wiley and Sons: Chichester, UK, 2016. [Google Scholar]
- Sangkhae, V.; Nemeth, E. Regulation of the Iron Homeostatic Hormone Hepcidin. Adv. Nutr. 2017, 8, 126–136. [Google Scholar] [CrossRef]
- Vessières, A. Iron Compounds as Anticancer Agenta. In Metal-based Anticancer Agents; Casini, A., Vessières, A., Meier-Menches, S.M., Eds.; The Royal Society of Chemistry: Croyden, UK, 2019; pp. 62–90. [Google Scholar]
- Valko, M.; Morris, H.; Cronin, M.T.D. Metals, Toxicity, and Oxidative Stress. Curr. Med. Chem. 2005, 12, 1161–1208. [Google Scholar] [CrossRef]
- Braga, S.S.; Silva, A.M.S. A New Age for Iron: Antitumoral Ferrocenes. Organometallics 2013, 32, 5626–5639. [Google Scholar] [CrossRef]
- Kowalski, K. Recent developments in the chemistry of ferrocenyl secondary natural product conjugates. Coord. Chem. Rev. 2018, 366, 91–108. [Google Scholar] [CrossRef]
- Kondratskyi, A.; Kondratskyi, K.; Abeele, F.V.; Gordienko, D.; Duboid, C.; Toillon, R.-A.; Slomianny, C.; Lemière, S.; Delcourt, P.; Dewailly, E.; et al. Ferroquine, the next generation antimalarial drug, has antitumor activity. Sci. Rep. 2017, 7, 15896. [Google Scholar] [CrossRef]
- Whitnall, M.; Howard, J.; Ponka, P.; Richardson, D.R. A class of iron chelators with a wide spectrum of potent antitumor activity that overcome resistance to chemotherapeutics. Proc. Natl. Acad. Sci. USA 2006, 103, 14901–14906. [Google Scholar] [CrossRef]
- Rosa, L.; Cutone, A.; Lepanto, M.S.; Paesano, R.; Valenti, P. Lactoferrin: A Natural Glycoprotein Involved in Iron and Inflammatory Homeostasis. Int. J. Mol. Sci. 2017, 18, 1985. [Google Scholar] [CrossRef]
- Dorazio, S.J.; Olatunde, A.O.; Tsitovich, P.B.; Morrow, J.R. Comparison of divalent transition metal ion paraCEST MRI contrast agents. J. Biol. Inorg. Chem. 2014, 19, 191–205. [Google Scholar] [CrossRef]
- Kuźnik, N.; Wyskocka, M. Iron(III) Contrast Agent Candidates for MRI: A Survey of the Structure-Effect Relationship in the Last 15 Years of Study. Eur. J. Inorg. Chem. 2016, 2016, 445–458. [Google Scholar] [CrossRef]
- Tsitovich, P.B.; Gendron, F.; Nazarenko, A.Y.; Livesay, B.N.; Lopez, A.P.; Shores, M.P.; Autschbach, J.; Morrow, J. Low-Spin Fe(III) Macrocyclic Complexes of Imidazole-Appended 1,4,7-Triazacyclononane as Paramagnetic Probes. Inorg. Chem. 2018, 57, 8364–8374. [Google Scholar] [CrossRef]
- Viljoen, J.J.; Weir, I.; Fietz, S.; Cloete, R.; Loock, J.; Philibert, R.; Roychoudhury, A.N. Links Between the Phytoplankton Community Composition and Trace Metal Distribution in Summer Surface Waters of the Atlantic Southern Ocean. Front. Mar. Sci. 2019, 6, 295. [Google Scholar] [CrossRef]
- Hodgkin, D.C.; Kamper, J.; MacKay, M.; Pickworth, J.; Trueblood, K.N.; White, J.G. Structure of vitamin B12. Nature 1956, 178, 64–66. [Google Scholar] [CrossRef]
- Hunt, A.; Harrington, D.; Robinson, S. Vitamin B12 deficiency. Br. Med. J. 2014, 349, g5226. [Google Scholar] [CrossRef]
- Fortin, J.-L.; Waroux, S.; Giocanti, J.P.; Capellier, G.; Ruttimann, M.; Kowalski, J.-J. Hydroxocobalamin for poisoning caused by ingestion of potassium cyanide: A case study. J. Emerg. Med. 2008, 39, 320–324. [Google Scholar] [CrossRef]
- Jelkmann, W. Erythropoietin after a century of research: Younger than ever. Eur. J. Haematol. 2007, 78, 183–205. [Google Scholar] [CrossRef]
- Munteanu, C.R.; Suntharalingam, K. Advances in cobalt complexes as anticancer agents. Dalton Trans. 2015, 44, 13796–13808. [Google Scholar] [CrossRef]
- Mjos, K.D.; Orvig, C. Metallodrugs in Medicinal Inorganic Chemistry. Chem. Rev. 2014, 114, 4540–4563. [Google Scholar] [CrossRef]
- Martinez-Bulit, P.; Garza-Ortíz, A.; Mijangos, E.; Barrón-Sosa, L.; Sánchez-Bartéz, F.; Garcia-Mora, I.; Flores-Parra, A.; Contreras, R.; Reedijk, J.; Barba-Behrens, N. 2,6-Bis(2,6-diethylphenyliminomethyl)pyridine coordination compounds with cobalt(II), nickel(II), copper(II), and zinc(II): Synthesis, spectroscopic characterization, X-ray study and in vitro cytotoxicity. J. Inorg. Biochem. 2015, 142, 1–7. [Google Scholar] [CrossRef]
- Casini, A.; Vessières, A.; Meier-Menches, S.M. Heterometallic Complexes as Anticancer Agents. In Metal-Based Anticancer Agents; Casini, A.; Vessières, A.; Meier-Menches, S.M. The Royal Society of Chemistry: Croyden, UK, 2019; pp. 143–168. [Google Scholar]
- Singh, N.; Jang, S.; Jo, J.-H.; Kim, D.H.; Park, D.W.; Kin, I.; Kim, H.; Kang, S.C.; Chi, K.-W. Coordination-Driven Self-Assembly and Anticancer Potency Studies of Ruthenium-Cobalt-Based Heterometallic Rectangles. Chem. Eur. J. 2016, 22, 16157–16164. [Google Scholar] [CrossRef]
- EPA. Radionuclide Basics: Cobalt-60. Available online: https://www.epa.gov/radiation/radionuclide-basics-cobalt-60 (accessed on 18 June 2019).
- Yoshiya, K.; Sato, T.; Omori, S.; Maruyama, S. The Birthplace of Proto-Life: Role of Secondary Minerals in Forming Metallo-Proteins through Water-Rock Interaction of Hadean Rocks. Orig. Life Evol. Biosph. 2018, 48, 373–393. [Google Scholar] [CrossRef]
- Boer, J.L.; Mulrooney, S.B.; Hausinger, R.P. Nickel-dependent metalloenzymes. Arch. Biochem. Biophys. 2013, 544, 142–152. [Google Scholar] [CrossRef] [Green Version]
- Nim, Y.S.; Wong, K.-B. The Maturation Pathway of Nickel Urease. Inorganics 2019, 7, 85. [Google Scholar] [CrossRef]
- Zambelli, B.; Ciurli, S. Nickel and Human Health. In Interrelations between Essential Metal Ions and Human Diseases; Sigel, A., Sigel, H., Sigel, R.K.O., Eds.; Springer: New York, NY, USA, 2013; Volume 13, pp. 321–357. [Google Scholar]
- Kusters, J.G.; van Vliet, A.H.M.; Kuipers, E.J. Pathogenesis of Helicobacter pylori Infection. Clin. Microbiol. Rev. 2006, 19, 449–490. [Google Scholar] [CrossRef]
- Duerig, T.; Pelton, A.; Stöckel, D. An overview of nitinol medical applications. Mater. Sci. Eng. A 1999, 273, 149–160. [Google Scholar] [CrossRef]
- Martin, S.F.; Esser, P.R.; Weber, F.C.; Jakob, T.; Freudenberg, M.A.; Schmidt, M.; Goebler, M. Mechanisms of chemical-induced innate immunity in allergic contact dermatitis. Allergy 2011, 66, 1152–1163. [Google Scholar] [CrossRef]
- Vilar, R. Nucleic Acid Quadruplexes and Metallo-Drugs. In Metallo-Drugs: Development and Action of Anticancer Agents; Sigel, A., Sigel, H., Freisinger, E., Sigel, R.K.O., Eds.; De Gruyter: Berlin, Germany, 2018; pp. 325–350. [Google Scholar]
- Sauvage, J.-P. Transition Metal-Containing Rotaxanes and Catenanes in Motion: Toward Molecular Machines and Motors. Acc. Chem. Res. 1998, 31, 611–619. [Google Scholar] [CrossRef]
- Beuning, C.N.; Mestre-Voegtlé, B.; Faller, P.; Hureau, C.; Crans, D.C. Measurement of Interpeptidic Cu(II) Exchange Rate Constants by Static Fluorescence Quenching of Tryptophan. Inorg. Chem. 2018, 57, 4791–4794. [Google Scholar] [CrossRef]
- Alberts, B.; Bray, D.; Hopkin, K.; Johnson, A.; Lewis, J.; Raff, M.; Roberts, K.; Walter, P. Essential Cell Biology, 4th ed.; Garland Science: New York, NY, USA, 2014. [Google Scholar]
- Iwata, S.; Ostermeier, C.; Ludwig, B.; Michel, H. Structure at 2.8Å resolution of cytochrome c oxidase from Paracoccus denitrificans. Nature 1995, 376, 660–669. [Google Scholar] [CrossRef]
- Tsukihara, T.; Aoyama, H.; Yamashita, E.; Tomizaki, T.; Yamaguchi, H.; Shinzawa-Itoh, K.; Nakashima, R.; Yaono, R.; Yoshikawa, S. The Whole Structure of the 13-Subunit Oxidized Cytochrome c Oxidase at 2.8Å. Science 1996, 272, 1136–1144. [Google Scholar] [CrossRef]
- Brewer, G.J. Copper in medicine. Curr. Opin. Chem. Biol. 2003, 7, 207–212. [Google Scholar] [CrossRef]
- Cobbett, C.; Goldsbrough, P. Phytochelatins and Metallothioneins: Roles in Heavy Metal Detoxification and Homeostasis. Annu. Rev. Plant Biol. 2002, 53, 159–182. [Google Scholar] [CrossRef]
- Cruces-Sande, A.; Rodríguez-Pérez, A.; Herbello-Hermelo, P.; Bermejo-Barrera, P.; Méndez-Álvarez, E.; Labandeira-García, J.L.; Soto-Otero, R. Copper Increases Brain Oxidative Stess and Enhances the Ability of 6-Hydroxydopamine to Cause Dopaminergic Degeneration in a Rat Model of Parkinson’s Disease. Mol. Neurobiol. 2019, 56, 2845–2854. [Google Scholar] [CrossRef]
- Atrián-Blasco, E.; Gonzalez, P.; Santoro, A.; Alies, B.; Faller, P.; Hureau, C. Cu and Zn coordination to amyloid peptides: From fascinating chemistry to debated pathological relevance. Coord. Chem. Rev. 2018, 371, 38–55. [Google Scholar] [CrossRef]
- Schleper, B.; Stuerenburg, H.J. Copper deficiency-associated myelopathy in a 46-year-old woman. J. Neurol. 2001, 248, 705–706. [Google Scholar] [CrossRef]
- Kumar, N. Copper Deficiency Myelopathy (Human Swayback). Mayo Clin. Proc. 2006, 81, 1371–1384. [Google Scholar] [CrossRef] [Green Version]
- Marzano, C.; Pelleri, M.; Tisato, F.; Santini, C. Copper Complexes as Anticancer Agents. Anti-Cancer Agents Med. Chem. 2009, 9, 185–211. [Google Scholar] [CrossRef]
- Denoyer, D.; Clatworthy, S.A.S.; Cater, M.A. Copper Complexes in Cancer Therapy. In Metallo-Drugs: Development and Action of Anticancer Agents; Sigel, A., Sigel, H., Freisinger, E., Sigel, R.K.O., Eds.; De Gruyter: Berlin, Germany, 2018; pp. 469–506. [Google Scholar]
- Santini, C.; Pellei, M.; Gandin, V.; Porchia, M.; Tisato, F.; Marzano, C. Advances in Copper Complexes as Anticancer Agents. Chem. Rev. 2014, 114, 815–862. [Google Scholar] [CrossRef]
- Kellett, A.; Molphy, Z.; McKee, V.; Slator, C. Recent Advances in Anticancer Copper Compounds. In Metal-based Anticancer Agents; Casini, A., Vessières, A., Meier-Menches, S.M., Eds.; The Royal Society of Chemistry: Croyden, UK, 2019; pp. 91–119. [Google Scholar]
- Ala, A.; Walker, A.P.; Ashkan, K.; Dooley, J.S.; Schlisky, M.L. Wilson’s disease. Lancet 2007, 369, 397–408. [Google Scholar] [CrossRef]
- Kaneshiro, B.; Aeby, T. Long-term safety, efficacy, and patient acceptability of the intrauterine Copper T-308A contraceptive device. Int. J. Womens Health 2010, 2, 211–220. [Google Scholar] [CrossRef]
- Stanford, J.B.; Mikolajczyk, R.T. Mechanisms of action of intrauterine devices: Update and estimation of postfertilization effects. Am. J. Obstet. Gynecol. 2002, 187, 1699–1708. [Google Scholar] [CrossRef]
- Sifri, C.D.; Burke, G.H.; Enfield, K.B. Reduced health care-associated infections in an acture care community hospital using a combination of self-disinfecting copper-impregnated composite hard surfaces and linens. Am. J. Infect. Control 2016, 44, 1565–1571. [Google Scholar] [CrossRef]
- Perelshtein, I.; Ruderman, Y.; Perkas, N.; Beddow, J.; Singh, G.; Vinatoru, M.; Joyce, E.; Mason, T.J.; Blanes, M.; Mollá, K.; et al. The sonochemical coating of cotton withstands 65 washing cycles at hospital washing standards and retains its antibacterial properties. Cellulose 2013, 20, 1215–1221. [Google Scholar] [CrossRef]
- Ataie, N.J.; Hoang, Q.Q.; Zahniser, M.P.D.; Tu, Y.; Milne, A.; Petsko, G.A.; Ringe, D. Zinc Coordination Geometry and Ligand Binding Affinity: The Structural and Kinetic Analysis of the Second-Shell Serine 228 Residue and the Methionine 180 Residue of the Aminopeptidase from Vibrio proteolyticus. Biochemistry 2008, 47, 7673–7683. [Google Scholar] [CrossRef]
- Bauer, B.A. Zinc for Colds: The Final Word? Available online: https://www.mayoclinic.org/diseases-conditions/common-cold/expert-answers/zinc-for-colds/faq-20057769 (accessed on 26 June 2019).
- Maret, W.; Li, Y. Coordination Dynamics of Zinc in Proteins. Chem. Rev. 2009, 109, 4682–4707. [Google Scholar] [CrossRef]
- Berg, J.M.; Shi, Y. The Galvanization of Biology: A Growing Appreciation for the Roles of Zinc. Science 1996, 271, 1081–1085. [Google Scholar] [CrossRef]
- Humphrey, W.; Dalke, A.; Schulten, K. VMD: Visual Molecular Dynamics. J. Mol. Graph. 1996, 14, 33–38. [Google Scholar] [CrossRef]
- Elrod-Erickson, M.; Benson, T.E.; Pabo, C.O. High-resolution structures of variant Zif268–DNA complexes: Implications for understanding zinc finger–DNA recognition. Structure 1998, 6, 451–464. [Google Scholar] [CrossRef]
- Lichten, L.A.; Cousins, R.J. Mammalian Zinc Transporters: Nutritional and Physiologic Regulation. Annu. Rev. Nutr. 2009, 29, 153–176. [Google Scholar] [CrossRef]
- Ziliotto, S.; Ogle, O.; Taylor, K.M. Targeting Zn(II) Signalling to Prevent Cancer. In Metallo-Drugs: Development and Action of Anticancer Agents; Sigel, A., Sigel, H., Freisinger, E., Sigel, R.K.O., Eds.; De Gruyter: Berlin, Germany, 2018; Volume 18, pp. 507–530. [Google Scholar]
- Giachi, G.; Pallecchi, P.; Romualdi, A.; Ribechini, E.; Lucejko, J.J.; Colombini, M.P.; Lippi, M.M. Ingredients of a 2,000-y-old medicine revealed by chemical, mineralogical, and botanical investigations. Proc. Natl. Acad. Sci. USA 2012, 110, 1193–1196. [Google Scholar] [CrossRef]
- Xie, Y.; He, Y.; Irwin, P.L.; Jin, T.; Shi, X. Antibacterial Activity and Mechanism of Action of Zinc Oxide Nanoparticles against Campylobacter jejuni. Appl. Environ. Microbiol. 2011, 77, 2325–2331. [Google Scholar] [CrossRef]
- Sakurai, H.; Kojima, Y.; Yoshikawa, Y.; Kawabe, K.; Yasui, H. Antidiabetic vanadium(IV) and zinc(II) complexes. Coord. Chem. Rev. 2002, 226, 187–198. [Google Scholar] [CrossRef]
- Bellomo, E.; Singh, K.B.; Massarotti, A.; Hogstrand, C.; Maret, W. The metal face of protein tyrosine phosphatase 1B. Coord. Chem. Rev. 2016, 327–328, 70–83. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Element | Common Minerals | Mineral Crystal System | Mineral Color | References |
|---|---|---|---|---|
| Scandium (Sc) | Thortveitite (Sc2Si2O7) | Monoclinic | Grayish green | [13,14,15,16] |
| Titanium (Ti) | Ilmenite (FeTiO3) rutile (TiO2) | Hexagonal; tetragonal | Iron black; reddish brown | [11,12,15] |
| Vanadium (V) | Vanadinite [Pb5(VO4)3Cl] carnotite [K(UO2)VO4∙1.5 H2O] | Hexagonal; monoclinic | Red to brownish yellow; bright yellow to dark yellow | [11,12,15] |
| Chromium (Cr) | Chromite (FeCr2O4) | Cubic | Black | [11,12,15] |
| Manganese (Mn) | Pyrolusite (MnO2) | Tetragonal | Black or dark grey | [12,15,17] |
| Iron (Fe) | Hematite, (Fe2O3) magnetite (Fe3O4) | Hexagonal; cubic | Red or black; iron black | [11,12,15] |
| Cobalt (Co) | Smaltite (CoAs2) cobaltite (CoAsS) linnaetite (Co3S4) | All cubic | Grey to white; white to grey with purple tint; light gray to dark grey | [11,12,15] |
| Nickel (Ni) | Garnierite [(Ni,Mg)6Si4O10(OH)8] pentladite [(Ni,Fe)9S8] | N/A; cubic | N/A; bronze yellow | [11,12,15] |
| Copper (Cu) | Native metal, chalcopyrite (CuFeS2) chalcocite (Cu2S) | Cubic; tetragonal; orthorhombic | Pale rose to copper red; brass yellow; blackish grey to black | [12,15] |
| Zinc (Zn) | Sphalerite (ZnS) smithsonite (ZnCO3) | Cubic; hexagonal | Various colors possible | [11,12,15] |
| Element | Possible Oxididation States | Oxidation States at pH 7.4 in Blood | Other Possible Oxidation States in the Biosphere | Reference(s) |
|---|---|---|---|---|
| Scandium (Sc) | III | III | III | [11,12,16] |
| Titanium (Ti) | 0, II, III, IV | IV | 0, III, IV | [11,12] |
| Vanadium (V) | −II, −I, I, II, III, IV, V | IV, V as metal oxides | III, IV, V | [11,12] |
| Chromium (Cr) | −IV, −II, 0, I, II, III, V, VI | III | III, (IV), V, VI | [11,12,20] |
| Manganese (Mn) | −III, −II, −I, 0, I, II, III, V, VI, VII | II, IV, VII | II, III, IV, VII | [11,12] |
| Iron (Fe) | −II, 0, I, II, III, IV, V, VI | II, III | II, III, (IV) | [11,12,21] |
| Cobalt (Co) | −I, 0, I, II, III, IV | II, III | II, III | [11,12] |
| Nickel (Ni) | 0, I, II, III, IV | I, II, III | 0, II | [11,12] |
| Copper (Cu) | (0), I, II, III, (IV) | Mainly II | I, II | [11,12] |
| Zinc (Zn) | (I), II | II | II | [11,12] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Cleave, C.; Crans, D.C. The First-Row Transition Metals in the Periodic Table of Medicine. Inorganics 2019, 7, 111. https://doi.org/10.3390/inorganics7090111
Van Cleave C, Crans DC. The First-Row Transition Metals in the Periodic Table of Medicine. Inorganics. 2019; 7(9):111. https://doi.org/10.3390/inorganics7090111
Chicago/Turabian StyleVan Cleave, Cameron, and Debbie C. Crans. 2019. "The First-Row Transition Metals in the Periodic Table of Medicine" Inorganics 7, no. 9: 111. https://doi.org/10.3390/inorganics7090111